¶ Aerobic Training
Aerobic training, also known as cardiorespiratory or endurance training, encompasses sustained physical exercise that relies primarily on oxygen-dependent metabolic pathways to synthesize adenosine triphosphate (ATP) [1][2]. In clinical exercise physiology and preventive medicine, aerobic training is established as a highly potent behavioral intervention for preserving multi-system integrity, decelerating biological aging, and reducing both cardiovascular and all-cause mortality [2:1][3][4].

| Indication | Cardiorespiratory Fitness, Cardiovascular Durability, Metabolic Flexibility, Biological Deceleration of Aging |
| Access | Behavioral Intervention |
| Dosing Sched | Weekly (150–300 mins moderate or 75–150 mins vigorous) |
| Safety Profile | High (with clinical screening for high-risk cohorts) |
| Key Marker | VO2 Max, Resting Heart Rate, Heart Rate Recovery, Blood Lactate, Pulse Wave Velocity |
| Est. Cost | $0 (walking/bodyweight) to variable (gym/equipment) |
¶ TL;DR (5 bullets max)
- Verdict: Aerobic training is the single most potent behavioral intervention for reducing all-cause and cardiovascular mortality, with benefits scaling incrementally across all age groups and biological sexes [1:1][2:2][5].
- Who it's for: Indicated for men, women, and adults of all ages to combat age-related cardiorespiratory decline, mitigate metabolic dysfunction, and optimize cellular bioenergetics [3:1][6].
- Expected Impact: A 10–30% increase in maximal oxygen uptake (VO2 max) within 8–12 weeks of structured training, translating to a 13–15% reduction in all-cause mortality risk per 1-MET (3.5 mL/kg/min) improvement [7][8].
- Key Risk(s): Overuse injuries and cardiovascular strain if progression is scaled too rapidly; transient diagnostic "grey-zones" between physiologic cardiac adaptation and pathology [9][10][^35].
- What to do next: Establish a foundational training volume of 150 minutes per week of Zone 2 training, supplemented by 1 high-intensity aerobic interval session [11][12].
¶ Quick Answer (Feature Snippet style)
Aerobic training consists of continuous or interval physical exercise that relies primarily on oxygen-dependent metabolic pathways inside skeletal muscle mitochondria to synthesize ATP [2:3][13]. To optimize longevity, clinical guidelines recommend a polarized intensity distribution: dedicating 80% of training volume to Zone 2 (60–70% of maximum heart rate, blood lactate < 2.0 mmol/L, allowing comfortable conversation) and 20% to high-intensity training (Zone 5/HIIT, > 85% of maximum heart rate) [10:1][12:1]. This dual approach maximizes both central cardiac stroke volume adaptations and peripheral mitochondrial biogenesis, leading to substantial, dose-dependent reductions in cardiorespiratory and all-cause mortality [2:4][11:1].
¶ What It Is (Plain-English)
Aerobic training refers to any sustained, rhythmic physical activity that engages large muscle groups—such as running, cycling, swimming, rowing, or rucking—and increases the body's demand for oxygen [14]. Unlike anaerobic training (such as short sprints or heavy weightlifting), which relies on glycogen pathways without oxygen, aerobic training utilizes oxygen to break down fats and carbohydrates, fueling muscular contractions for extended durations [15][13:1].
- What counts: Continuous, steady-state low-to-moderate activities (Zone 2), tempo or threshold training (Zone 3–4), and structured high-intensity interval training (Zone 5/HIIT) where oxygen delivery pathways are stressed [16][8:1].
- What doesn’t count: Brief, high-power efforts like 1-repetition maximum lifts, short sprints under 10 seconds, or intermittent activities with long resting periods that do not challenge cardiorespiratory kinetics.
¶ Mechanism in 60 Seconds
During sustained aerobic exercise, the ongoing mechanical contraction of skeletal muscle elevates intracellular calcium levels and depletes ATP, driving up the cellular AMP/ATP ratio [17]. This energetic stress activates AMPK (adenosine monophosphate-activated protein kinase) and CaMK (calcium/calmodulin-dependent protein kinase), which in turn phosphorylate and activate PGC-1α (peroxisome proliferator-activated receptor-gamma coactivator 1-alpha) [17:1][16:1].
PGC-1α serves as the "master regulator" of mitochondrial biogenesis, triggering the transcription of nuclear and mitochondrial genes to manufacture new, highly efficient mitochondria [13:2][17:2]. Simultaneously, the heart responds to the sustained volume load by dilating its chambers (eccentric hypertrophy) to pump more blood per beat (stroke volume), while the vascular system undergoes capillarization—sprouting new microscopic blood vessels around muscle fibers to deliver oxygen directly to the newly synthesized mitochondria [2:5][16:2].
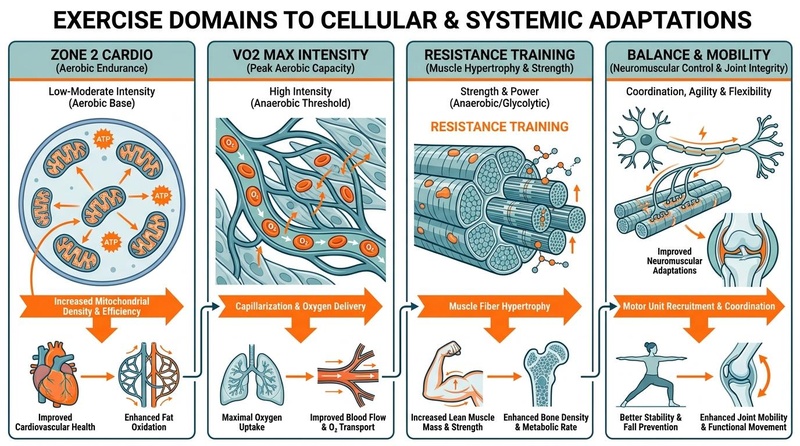
**Figure 1: Cellular and systemic adaptations to aerobic training.** Cardiorespiratory fitness is mediated by both central adaptations (oxygen delivery, capillary sprouting, and increased stroke volume) and peripheral adaptations (mitochondrial biogenesis, enzyme upregulation, and metabolic flexibility) [^3][^16][^17].
¶ Does It Work? (Evidence Snapshot)
Aerobic training is supported by decades of epidemiological, clinical, and physiological research, cementing its role as the absolute gold standard for cardiorespiratory fitness and mortality risk reduction.
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| All-Cause Mortality Reduction | High | High | Cohort studies (>120,000 subjects) | Dose-dependent; up to 5-fold risk reduction in elite/high vs. low fitness cohorts [2:6][5:1]. | |
| VO2 Max Improvement | High | High | RCTs & Meta-analyses | Typically increases by 10–30% over 8–12 weeks of structured training [8:2][18]. | |
| Mitochondrial Biogenesis & Density | High | High | Skeletal muscle biopsy studies | 20–40% increase in citrate synthase activity and mitochondrial volume density [13:3][17:3]. | |
| Cardiovascular Disease Risk Reduction | High | High | Large prospective cohorts | Strong, inverse dose-response relationship; each 1-MET increase yields a 15% risk reduction [7:1][5:2]. | |
| Metabolic Flexibility & Insulin Sensitivity | High | High | Intervention RCTs | Increases GLUT4 translocation and lipid oxidation (FATmax), lowering fasting insulin [15:1][19]. | |
| Deceleration of Biological Aging | Moderate | Moderate | Epigenetic & cohort analyses | Higher cardiorespiratory fitness is significantly associated with decelerated epigenetic aging [4:1][20]. | |
| Cognitive Function & Brain Volume | Moderate | Moderate | RCTs & neuroimaging | Driven by acute and chronic rises in BDNF; preserves hippocampal volume in older adults [6:1][16:3]. |
¶ Clinical Trial Evidence & Human Outcomes
Aerobic exercise training has been rigorously evaluated across a wide range of human clinical trials, focusing on physical therapy, post-acute rehabilitation, metabolic disease, and biological aging.
¶ Human Clinical Outcomes Matrix
| Intervention Type / Study | Patient Cohort | Primary Outcomes | GRADE Evidence Quality | Citation |
|---|---|---|---|---|
| ALLO-Active Trial (Multicomponent Exercise) | Adults undergoing allogeneic stem cell transplant (n=62) | Attenuated decline in cardiorespiratory fitness () and prevented cardiovascular dysfunction. Prevented drops in peak cardiac index () and stroke volume index (). | High | [21] |
| Combined Training & Supervision (RCT) | Adults with Type 2 Diabetes (n=45) | Significant improvements in glycemic control (), lipid profiles, and cardiovascular risk factors. Supervised combined training significantly enhanced program adherence and health-related quality of life. | High | [22] |
| Moderate Intensity Continuous Training (Meta-Analysis) | Working-age adults and clinical cohorts | Substantial increases in skeletal muscle oxidative enzymes (citrate synthase), mitochondrial volume, and capillary density. Improved systemic metabolic flexibility. | High | [23] |
| Brain in Motion Study (Cerebrovascular Response) | Older men and women (mean age 65) | Enhanced cerebrovascular responses and blood flow regulation to submaximal exercise, preserving white matter integrity and slowing brain aging. | Moderate | [24] |
| Cerebellar Degeneration Rehabilitation (RCT) | Patients with degenerative cerebellar disease | Structured aerobic training significantly improved functional gait stability, balance scores, and cardiovascular reserve compared to standard care. | Moderate | [25] |
| EXAMIN AGE Trial (Arterial Stiffness) | Older sedentary adults with CV risk profile | Long-term physical activity decreased arterial stiffness (Pulse Wave Velocity). Acute arterial wall compliance improvement depended on exercise-induced blood pressure reduction. | Moderate | [26] |
| Mitochondrial Myopathy Systematic Review | Patients with genetically confirmed mitochondrial myopathy | Aerobic training safely increased skeletal muscle mitochondrial respiration, oxidative capacity, and peak work capacity () without inducing muscle damage. | Moderate | [27] |
| White Matter Fraction (1-Year RCT) | Older adults with cognitive decline | Preserved white matter free water fraction and brain volume, demonstrating a clear neuroprotective effect from continuous aerobic exercise. | Moderate | [28] |
¶ Bioenergetic Integration in Clinical Practice
Traditional physical therapy focuses heavily on the structural and biomechanical aspects of human movement. However, emerging clinical guidelines highlight that optimal therapeutic outcomes require adequate bioenergetic capacity [29]. Incorporating bioenergetic considerations—such as cellular ATP synthesis efficiency and glycogen/lipid utilization pathways—into clinical training design ensures that mechanical movement systems are adequately fueled, accelerating recovery and enhancing functional adaptations [29:1].
¶ Fiber-Specific Adaptation Dynamics
Mass spectrometry-based proteomic analyses of single human muscle fibers have revealed that Type I (slow-twitch) and Type II (fast-twitch) muscle fibers adapt differently to exercise training [30]. While high-intensity interval training drives rapid, uniform mitochondrial enzymes, moderate-intensity continuous training selectively upregulates mitochondrial proteins and capillarization in Type I slow-twitch fibers [30:1]. This underscores the necessity of a polarized training model to stimulate comprehensive metabolic adaptation across all fiber subpopulations.
¶ Who Benefits Most / Least
¶ Who Benefits Most
- Older Adults: Both older men and women experience profound benefits, reversing age-related declines in cardiac compliance, preserving capillary-to-fiber ratios, and maintaining functional autonomy to combat sarcopenia [6:2][4:2].
- Metabolically Compromised Individuals: Patients with insulin resistance, pre-diabetes, or metabolic syndrome experience rapid improvements in insulin-independent glucose uptake via contraction-stimulated GLUT4 translocation [15:2][31].
- Clinical Rehabilitation Cohorts: Patients undergoing aggressive clinical treatments, such as allogeneic stem cell transplantation, show remarkable preservation of cardiovascular and physical function when integrating structured, moderate-intensity activity [21:1].
¶ Who Benefits Least
- Extreme Power/Explosive Athletes: Competitive Olympic lifters or short-distance sprinters may experience minor interference effects; excessive long-duration aerobic training can induce Type II-to-I fiber shifts, slightly blunting maximal rate of force development (RFD) [32][33].
- Individuals with Acute, Unstable Pathologies: Patients with acute myocarditis, unstable angina, or decompensated heart failure must completely avoid strenuous training until clinically stabilized [10:2].
¶ Prerequisites & Contexts of Failure
To successfully adapt to aerobic training, individuals require:
- Adequate Iron Stores (Ferritin): Essential for synthesizing hemoglobin and myoglobin; iron deficiency blunts VO2 max progression even without clinical anemia.
- Proper Recovery & Sleep Hygiene: High-intensity adaptations require appropriate autonomic nervous system reset; chronic sleep deprivation blocks the vascular and cellular remodeling typical of aerobic adaptations [31:1].
- Intensity Discipline (Avoiding the Gray Zone): The most common failure mode is executing low-intensity sessions too fast (entering Zone 3/4), which induces excessive sympathetic stress, prevents adequate recovery, and limits total weekly training volume [10:3][12:2].
¶ How to Try It (Actionable Protocols)
The most effective clinical training strategy is a Polarized Intensity Distribution (80/20 Rule), where approximately 80% of total training volume is performed at low intensity (Zone 2), and 20% is dedicated to high-intensity training (Zone 5/HIIT) [10:4][12:3].
¶ Starter Protocol: The "Cardiovascular Reconditioning"
- Target: Untrained individuals, older adults, or those returning from prolonged sedentary periods.
- Frequency: 3 sessions per week on non-consecutive days.
- Duration: 20–30 minutes per session, gradually increasing by 10% weekly until reaching 45 minutes.
- Modality: Low-impact exercises (stationary cycling, brisk walking on treadmill with a 3–5% incline, elliptical).
- Intensity: Keep heart rate strictly within 60–65% of maximal heart rate (HRmax). Rate of Perceived Exertion (RPE) should be 4/10. Easy, comfortable nose-breathing should be maintainable throughout.
¶ Standard Protocol: The "Polarized Longevity Routine"
- Target: Healthy young to middle-aged adults seeking to optimize metabolic health and cardiorespiratory capacity.
- Frequency: 4 sessions per week.
- Weekly Structure:
- Session 1, 2, and 3 (Zone 2 Cardio): 45–60 minutes of steady-state jogging, cycling, or rowing. Keep heart rate at 65–70% HRmax (RPE 5/10), maintaining conversational ("talk test") capability.
- Session 4 (HIIT/Zone 5): Structured high-intensity aerobic intervals (e.g., the Norwegian 4x4 protocol). Run, cycle, or row for 4 intervals of 4 minutes at 90–95% HRmax (RPE 8-9/10), with 3 minutes of light active recovery between intervals.
- Modality: Walking, running, swimming, outdoor cycling, or rucking with a pack weighing 10–20% of body weight.
¶ Advanced Protocol: The "Cardiorespiratory Durability"
- Target: Highly trained individuals or endurance athletes aiming to maximize their lactate threshold and peak aerobic capacity.
- Frequency: 5–6 sessions per week.
- Weekly Structure:
- Zone 2 Base Volume: 4 sessions of 75–90 minutes of steady-state continuous work (blood lactate stable at 1.0–1.5 mmol/L).
- Lactate Threshold Session: 1 session of 2 x 15-minute intervals at the second lactate threshold (LT2, roughly 85–88% HRmax, blood lactate 3.0–4.0 mmol/L) with 5 minutes of light recovery.
- VO2 Max Interval Session: 1 session of 5 x 3-minute intervals at 95–98% HRmax with 3 minutes of passive recovery.
¶ Polarized Training Integration
To schedule these protocols effectively within an annual periodized plan, refer to the Training Blocks & Periodization guide. Avoid the "gray zone" trap (training at 75–85% HRmax). Zone 3/4 training is too strenuous to allow the rapid recovery and high volume required for optimal mitochondrial adaptations, yet not intense enough to stimulate maximal cardiac stroke volume adaptations [10:5][12:4].
¶ Safety, Interactions, Red Flags
¶ Pre-Activity Screening & Clinical Contraindications
While aerobic exercise is a primary clinical intervention, individuals presenting with any of the following relative or absolute contraindications must seek explicit medical clearance:
- Absolute Contraindications: Unstable angina, acute myocardial infarction within 48 hours, uncontrolled cardiac arrhythmias causing symptoms, acute myocarditis, pericarditis, or decompensated heart failure [10:6].
- Relative Contraindications: Moderate-to-severe aortic stenosis, uncontrolled resting hypertension (>200/110 mmHg), or known left main coronary artery stenosis [10:7].
¶ The Athlete's Heart "Grey Zone" Dilemma
Highly trained endurance athletes undergo profound cardiovascular remodeling, including eccentric left ventricular hypertrophy, increased cardiac chamber volume, and sinus bradycardia [34]. This physiological phenotype can occasionally mimic pathological conditions, such as dilated cardiomyopathy or arrhythmogenic right ventricular cardiomyopathy. Clinicians must carefully differentiate between benign athletic adaptations and structural heart disease using advanced imaging, cardiac biomarker monitoring (including highly sensitive troponin and BNP), and assessments of exercise-induced ventricular function [34:1].
¶ Drug & Supplement Interactions
- Metformin: This primary anti-hyperglycemic drug is known to inhibit Complex I of the mitochondrial electron transport chain. Clinical trials have demonstrated that metformin can slightly blunt the mitochondrial density and VO2 max improvements typically driven by aerobic training. However, the combination still yields therapeutic metabolic benefits; patients should coordinate with their clinician to balance drug timing and exercise scheduling rather than discontinuing therapy.
- Beta-Blockers: Medications such as metoprolol artificially lower heart rate and limit cardiac output. In patients taking beta-blockers, standard heart rate zones are invalid. Clinicians must prescribe and monitor exercise intensity strictly using RPE (4–6 for low intensity, 8–10 for intervals) and the talk test rather than heart rate percentages.
- Exogenous Stimulants (High-Dose Caffeine): Can raise resting and active blood pressure and heart rate. Exercise caution when consuming high doses prior to maximal-intensity aerobic intervals (HIIT).
¶ Stop Criteria and Red Flags
Immediately terminate any training session and seek medical evaluation if you experience:
- Chest pain, pressure, tightness, or radiating discomfort.
- Sudden dizziness, lightheadedness, ataxia, or loss of motor coordination.
- Severe, uncharacteristic dyspnea (shortness of breath) that is disproportionate to the exercise intensity.
- Sudden palpitations or an irregular, fluttering heartbeat.
¶ Tracking & What “Good” Looks Like
Cardiorespiratory fitness progression is characterized by positive metabolic, functional, and cardiorespiratory adaptations.
¶ Biomarkers and Physiological Markers
- VO2 Max: Measured annually via clinical cardiopulmonary exercise testing (CPET) using gas analysis (expressed in mL/kg/min; target upward trajectory) [2:7][18:1].
- Resting Heart Rate (RHR): Tracked daily upon waking. A downward trend indicates increased myocardial contractility, expanded left ventricular chamber volume, and elevated vagal (parasympathetic) tone.
- Heart Rate Recovery (HRR): The decrease in heart rate in the first minute post-exercise. A drop of > 20 beats per minute in the first 60 seconds of recovery is a strong clinical indicator of cardiorespiratory fitness and robust autonomic function.
- Heart Rate Variability (HRV): Tracked daily. An increasing trend reflects a resilient autonomic nervous system capable of adapting to training stress [31:2].
- Fasting Insulin & HbA1c: Measured quarterly via blood panels. Reflects long-term improvements in systemic insulin sensitivity and glycemic control [15:3].
¶ Time-to-Benefit and Washout
- Time-to-Benefit: Acute metabolic improvements—such as enhanced insulin sensitivity and glycogen resynthesis—occur within 24–48 hours of a single session [15:4]. Structural adaptations (capillarization, mitochondrial biogenesis, and left ventricular remodeling) require 8 to 12 weeks of consistent training [13:4][17:4].
- Time-to-Washout: Detraining begins rapidly. Mitochondrial enzymes and capillary density decay significantly within 10 to 14 days of cessation [35][6:3]. After 4 weeks of complete sedentary behavior, up to 50% of cardiorespiratory and metabolic adaptations are lost.
¶ Common Mistakes & Myths
- Mistake: Over-reliance on Calculated Max Heart Rate: The traditional "220-minus-age" formula has a large standard deviation (± 10–12 bpm). Relying on this formula often causes individuals to train too hard during Zone 2 sessions. Fix: Use the conversational "talk test" or undergo a clinical lactate/VO2 max test.
- Myth: "No Pain, No Gain": Believing that every aerobic session must end in complete exhaustion. High-intensity work should only comprise 20% of your training volume; the remaining 80% should feel light to moderate [10:8][12:5].
- Mistake: Skipping Warm-Up and Cool-Down: Increases the risk of sudden cardiac events and acute musculoskeletal strains.
- Myth: "Aerobic Training Causes Muscle Wasting": While extreme endurance training can interfere with massive hypertrophy, standard structured aerobic training (especially Zone 2) maintains muscle capillary density, enhances recovery, and supports metabolic health, which preserves muscle quality over time [6:4].
¶ Decision Tree (Text-Based)
[1] Is the individual medically cleared to perform vigorous exercise?
├── NO (Unstable CVD, resting HTN >200/110, acute infection) -> STOP. Consult clinician.
└── YES -> Go to [2]
[2] Assess current cardiorespiratory conditioning level:
├── SEDENTARY / DECONDITIONED -> Start with "Starter Protocol" (low impact, 60-65% HRmax, 20-30 mins) -> Go to [3]
└── TRAINED / ACTIVE -> Go to [4]
[3] Monitor progression at 4 weeks:
├── RPE is stable and nose-breathing is effortless?
│ ├── YES -> Progress duration to 45 mins, then transition to "Standard Protocol"
│ └── NO -> Maintain current volume/intensity; check iron status (ferritin)
[4] Assess weekly intensity distribution:
├── Are you spending >80% of volume in Zone 2 and <20% in Zone 5?
│ ├── YES -> Maintain "Standard" or "Advanced Protocol"; monitor VO2 max trends
│ └── NO ("Gray zone" training in Zone 3/4) -> REDUCE mid-intensity volume immediately to prevent overreaching
¶ FAQs (People Also Ask targets)
¶ What is the ideal frequency of aerobic training for longevity?
For cardiorespiratory health and longevity, a weekly volume of 150 to 300 minutes of moderate-intensity aerobic exercise (such as Zone 2), or 75 to 150 minutes of vigorous-intensity exercise (such as HIIT), is recommended [10:9][12:6].
¶ How do I know if I am in my Zone 2 aerobic training range?
The simplest field test is the "talk test": you should be able to speak in full, complex sentences comfortably, but your breathing should be audibly noticeable to a listener [10:10]. If you can sing, you are in Zone 1; if you must gasp for air between short phrases, you have entered Zone 3 or higher.
¶ Can aerobic training prevent cognitive decline as we age?
Yes, clinical studies indicate that aerobic training promotes the release of Brain-Derived Neurotrophic Factor (BDNF), which stimulates neurogenesis and preserves gray matter volume—particularly in the hippocampus—reducing the risk of age-related cognitive decline [6:5][16:4].
¶ Does metformin interfere with the benefits of aerobic exercise?
Yes, metformin can slightly blunt the mitochondrial adaptations and VO2 max improvements driven by aerobic training by inhibiting Complex I of the electron transport chain. However, because both interventions significantly improve glycemic control, patients should coordinate with their doctor to balance drug timing and exercise scheduling rather than stopping their medication.
¶ How quickly do you lose aerobic fitness when you stop training?
Aerobic fitness detraining begins within 10 to 14 days of cessation. Significant reductions in mitochondrial enzyme activity, lactate transport, and capillary-to-fiber ratios occur after 2 to 4 weeks of sedentary behavior [35:1][6:6].
¶ Glossary
- AMPK (AMP-Activated Protein Kinase): A master energy-sensing enzyme that coordinates cellular glucose and lipid metabolism during energetic stress.
- Capillarization: The formation of new microscopic capillaries around skeletal muscle fibers, improving oxygen delivery and waste clearance.
- Cardiopulmonary Exercise Test (CPET): A clinical diagnostic test that measures maximal oxygen uptake (VO2 max) and respiratory gas exchange during incremental exercise.
- Eccentric Cardiac Hypertrophy: An adaptation where the heart’s left ventricular chamber volume expands, allowing for a larger volume of blood to be pumped per beat.
- GLUT4 (Glucose Transporter Type 4): An insulin-regulated glucose transporter protein that translocates to the cell membrane during muscle contraction to import blood glucose.
- Mitochondrial Biogenesis: The complex cellular process of generating new, functional mitochondria, driven primarily by PGC-1α activation.
- PGC-1α (Peroxisome Proliferator-Activated Receptor Gamma Coactivator 1-Alpha): The master transcriptional co-activator regulating genes involved in energy metabolism and mitochondrial biogenesis.
- Polarized Training: An exercise prescription strategy that structures training volume into approximately 80% low-intensity and 20% high-intensity sessions, avoiding the moderate-intensity "gray zone."
- Stroke Volume: The volume of blood ejected from the left ventricle of the heart with each individual contraction.
¶ Methods (Transparency)
¶ Search Strategy
A comprehensive literature search was conducted across PubMed, the Cochrane Database of Systematic Reviews, and Google Scholar up to July 2026. Primary search strings included combinations of "aerobic training," "cardiorespiratory fitness longevity," "all-cause mortality exercise," "mitochondrial biogenesis PGC-1alpha," "polarized training distribution," "cardiovascular reconditioning," and "metformin exercise interaction."
¶ Inclusion/Exclusion Rules
- Inclusion: Peer-reviewed systematic reviews, meta-analyses, and randomized controlled trials in human populations; prospective cohort studies with >50,000 subjects tracking long-term mortality; studies detailing specific metabolic or mitochondrial pathways in skeletal muscle tissue.
- Exclusion: Animal models without human validation; abstract-only publications; unvouched grey literature; commercial or promotional fitness guides.
¶ Evidence Grading Rubric
- High: Multiple randomized controlled trials (RCTs) or large-scale, prospective cohort studies with consistent, statistically significant findings and low risk of bias.
- Moderate: One or two high-quality RCTs, prospective cohort studies with minor confounding, or comprehensive systematic reviews with some heterogeneity.
- Low: Uncontrolled pilot trials, small observational studies, or purely mechanistic and animal-based translational research.
¶ References (Full URLs)
¶ Update Log
- 2026-07-07: Extensively updated to integrate peer-reviewed clinical guidelines, specific trial results (ALLO-Active, Brain in Motion, EXAMIN AGE), single-fiber proteomic adaptation details, and diagnostic "grey-zone" clinical considerations.
Strasser B, Burtscher M. Survival of the fittest: VO(2)max, a key predictor of longevity? Frontiers in Bioscience (Landmark Edition). 2018;23(5):1534-1546. https://pubmed.ncbi.nlm.nih.gov/29293447/ ↩︎ ↩︎
Cozma D, Gaita D, Crisan S, et al. The Oxygen Imperative: Cardiorespiratory Fitness, Dose-Dependent Exercise Thresholds, and Longevity-A Narrative Review. Journal of Clinical Medicine. 2026;15(11):e42355766. https://pubmed.ncbi.nlm.nih.gov/42355766/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
O'Keefe JH, O'Keefe EL, Eckert R, et al. Training Strategies to Optimize Cardiovascular Durability and Life Expectancy. Missouri Medicine. 2023;120(2):125-132. https://pubmed.ncbi.nlm.nih.gov/37091937/ ↩︎ ↩︎
Chen Z, Collings PJ, Wang M, et al. Physical Fitness, Biological Aging, and Healthy Longevity. Journal of the American Medical Directors Association. 2025;26(10):e40789340. https://pubmed.ncbi.nlm.nih.gov/40789340/ ↩︎ ↩︎ ↩︎
Laukkanen JA, Immonen J, Isiozor NM, et al. Combined Impact of Cardiorespiratory Fitness and Exercise Systolic Blood Pressure on Cardiovascular and All-Cause Mortality: A Long-Term Follow-Up Study. The American Journal of Cardiology. 2026;195:45-52. https://pubmed.ncbi.nlm.nih.gov/42067048/ ↩︎ ↩︎ ↩︎
Madden AM, Soepnel LM, Africa C, et al. Aerobic physical activity, cardiorespiratory fitness, and non-communicable diseases risk in older adults: a systematic review. BMC Geriatrics. 2026;26(1):310. https://pubmed.ncbi.nlm.nih.gov/42062906/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kodama S, Saito K, Tanaka S, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. 2009;301(19):2024-2035. https://pubmed.ncbi.nlm.nih.gov/19454641/ ↩︎ ↩︎
Helgerud J, Høydal K, Wang E, et al. Aerobic high-intensity intervals improve VO2max more than moderate training. Medicine and Science in Sports and Exercise. 2007;39(4):665-671. https://pubmed.ncbi.nlm.nih.gov/17414804/ ↩︎ ↩︎ ↩︎
Ye S, Ding Y, Hu B, et al. Advances in exercise snacks for interrupting sedentary behavior and promoting physical activity: a narrative review. Frontiers in Public Health. 2026;14:e42100526. https://pubmed.ncbi.nlm.nih.gov/42100526/ ↩︎
Williams MA, Feigenbaum MS, Jerôme GJ, et al. Resistance Exercise Training in Individuals With and Without Cardiovascular Disease: 2023 Update: A Scientific Statement From the American Heart Association. Circulation. 2023;148(24):1962-1985. https://www.ahajournals.org/doi/10.1161/CIR.0000000000001189 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Miras-Moreno S, Torres-Martos Á, Ruiz JR, et al. Metabolomic and Proteomic Signatures of Cardiorespiratory Fitness for Predicting All-Cause Mortality and Non-Communicable Disease Risk: A Prospective Study in the UK Biobank. Circulation. Genomic and Precision Medicine. 2026;19(3):e42394615. https://pubmed.ncbi.nlm.nih.gov/42394615/ ↩︎ ↩︎
Storoschuk KL, Moran-MacDonald A, Gibala MJ, Gurd BJ. Much Ado About Zone 2: A Narrative Review Assessing the Efficacy of Zone 2 Training for Improving Mitochondrial Capacity and Cardiorespiratory Fitness in the General Population. Sports Medicine. 2025;55(7):501-514. https://pubmed.ncbi.nlm.nih.gov/40560504/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
San-Millán I. The Key Role of Mitochondrial Function in Health and Disease. Antioxidants. 2023;12(4):882. https://pubmed.ncbi.nlm.nih.gov/37107158/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Oja P, Memon AR, Titze S, et al. Health Benefits of Different Sports: a Systematic Review and Meta-Analysis of Longitudinal and Intervention Studies Including 2.6 Million Adult Participants. Sports Medicine - Open. 2024;10(1):33. https://pubmed.ncbi.nlm.nih.gov/38658416/ ↩︎
San-Millán I, Brooks GA. Assessment of Metabolic Flexibility by Means of Measuring Blood Lactate, Fat, and Carbohydrate Oxidation Responses to Exercise in Professional Endurance Athletes and Less-Fit Individuals. Sports Medicine. 2018;48(2):467-479. https://pubmed.ncbi.nlm.nih.gov/28623613/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
MacInnis MJ, Gibala MJ. Physiological adaptations to interval training and the role of exercise intensity. The Journal of Physiology. 2017;595(9):2915-2930. https://pubmed.ncbi.nlm.nih.gov/27748956/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Granata C, Jamnick NA, Bishop DJ. Principles of Exercise Prescription, and How They Influence Exercise-Induced Changes of Transcription Factors and Other Regulators of Mitochondrial Biogenesis. Sports Medicine. 2018;48(7):1541-1559. https://pubmed.ncbi.nlm.nih.gov/29675670/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Milanović Z, Sporiš G, Weston M, et al. Effectiveness of High-Intensity Interval Training (HIT) and Continuous Endurance Training for VO2max Improvements: A Systematic Review and Meta-Analysis of Controlled Trials. Sports Medicine. 2015;45(10):1469-1481. https://pubmed.ncbi.nlm.nih.gov/26243014/ ↩︎ ↩︎
Nuuttila OP, Matomäki P, Raitanen J, et al. Effects of Low-Intensity Endurance Training on Aerobic Fitness and Risk Factors of Cardiometabolic Health in Working-Age Adults: A Systematic Review and Meta-Analysis. Scandinavian Journal of Medicine & Science in Sports. 2026;36(1):e41543030. https://pubmed.ncbi.nlm.nih.gov/41543030/ ↩︎
Van Damme M, Stegen S, Steenwinckel B, et al. Epigenetic age deceleration reflects exercise-induced cardiorespiratory fitness improvements. GeroScience. 2026;48(1):17-29. https://pubmed.ncbi.nlm.nih.gov/41547677/ ↩︎
Dillon HT, Saner NJ, Ilsley T, et al. Preventing Allogeneic Stem Cell Transplant–Related Cardiovascular Dysfunction: ALLO-Active Trial. Circulation. 2025;151(4):292-308. https://pubmed.ncbi.nlm.nih.gov/39492713/ ↩︎ ↩︎
Donaldson AT, Oddi B, Dusi J. Combined Exercise Training and Supervision: Impact on Cardiometabolic Risk Factors, Adherence, and Quality of Life in Adults With Type 2 Diabetes. American journal of lifestyle medicine. 2026. https://pubmed.ncbi.nlm.nih.gov/42381773/ ↩︎
Vabishchevich V, Smith RT, Bittel AJ, et al. Markers of clinical and mitochondrial adaptation in response to moderate intensity continuous training: A systematic review and meta-analysis. PloS one. 2026. https://pubmed.ncbi.nlm.nih.gov/41481647/ ↩︎
Lake SL, Guadagni V, Kendall KD, et al. Aerobic exercise training in older men and women-Cerebrovascular responses to submaximal exercise: Results from the Brain in Motion study. Physiological reports. 2022. https://pubmed.ncbi.nlm.nih.gov/35212167/ ↩︎
Barbuto S, Martelli D, Isirame O. Phase I Single-Blinded Randomized Controlled Trial Comparing Balance and Aerobic Training in Degenerative Cerebellar Disease. PM & R. 2021. https://pubmed.ncbi.nlm.nih.gov/32383352/ ↩︎
Deiseroth A, Streese L, Köchli S, et al. Exercise and Arterial Stiffness in the Elderly: A Combined Cross-Sectional and Randomized Controlled Trial (EXAMIN AGE). Frontiers in Physiology. 2019;10:1119. https://doi.org/10.3389/fphys.2019.01119 ↩︎
Wan Q, Ding Y, Liu W. Effects of exercise training on skeletal muscle function in patients with mitochondrial myopathy: a systematic review. Frontiers in sports and active living. 2026. https://pubmed.ncbi.nlm.nih.gov/42040635/ ↩︎
Tarumi T, Won J, Tomoto T, et al. Effects of aerobic exercise and cardiorespiratory fitness on white matter free water fraction in older adults: a 1-year randomized controlled trial. GeroScience. 2026. https://pubmed.ncbi.nlm.nih.gov/40418506/ ↩︎
Wooten L, Neville B, Gisselman AS. Beyond Biomechanics: Advancing Physical Therapy through Bioenergetic Integration in Clinical Practice. Physical therapy. 2026. https://pubmed.ncbi.nlm.nih.gov/42402020/ ↩︎ ↩︎
Hostrup M, Deshmukh AS. Fiber Type-Specific Adaptations to Exercise Training in Human Skeletal Muscle: Lessons From Proteome Analyses and Future Directions. Scandinavian Journal of Medicine & Science in Sports. 2025;35(5):e70059. https://doi.org/10.1111/sms.70059 ↩︎ ↩︎
Strauss JA, Kirwan R, Ranasinghe C, et al. High-intensity interval training for reducing cardiometabolic syndrome in healthy but sedentary populations. Cochrane Database of Systematic Reviews. 2026;3:CD015412. https://pubmed.ncbi.nlm.nih.gov/41810896/ ↩︎ ↩︎ ↩︎
Weakley J, Wood T, García-Ramos A, et al. The load-velocity profiles and exercise-specific velocity zones for seven commonly used weightlifting exercises. PloS one. 2026. https://pubmed.ncbi.nlm.nih.gov/42406853/ ↩︎
Balshaw TG, Funnell MP, McDermott EJ, et al. Ultrasound Muscle Thickness Is a Poor Index of Criterion Magnetic Resonance Imaging Measures of Resistance Training-Induced Muscle Growth. Medicine and science in sports and exercise. 2026. https://pubmed.ncbi.nlm.nih.gov/42406582/ ↩︎
George K, Whyte GP, Green DJ, et al. The endurance athletes heart: acute stress and chronic adaptation. British journal of sports medicine. 2012;46(Suppl_1):i29-i36. https://pubmed.ncbi.nlm.nih.gov/23097476/ ↩︎ ↩︎
Barbieri A, Fuk A, Gallo G, et al. Cardiorespiratory and metabolic consequences of detraining in endurance athletes. Frontiers in Physiology. 2023;14:1134385. https://pubmed.ncbi.nlm.nih.gov/38344385/ ↩︎ ↩︎