¶ Beginner Exercise Guide: From Sedentary to Sustained Longevity
¶ TL;DR (5 bullets max)
- The Habit First Principle: In the first 4 weeks, consistency and habit formation are vastly more important than intensity or volume. Focus on showing up, not burning out.
- Safety First (Pre-Participation): Sedentary individuals must undergo screening using the American College of Sports Medicine (ACSM) algorithm to evaluate cardiorespiratory readiness before beginning vigorous physical training.
- The Tendon Lag: Muscles adapt to mechanical load far faster than tendons and ligaments due to differences in vascularity, requiring slow, linear progressive overload to prevent chronic orthopedic injuries.
- High-Yield Entry Points: Begin with a low-impact walking baseline (building to 7,500–10,000 steps daily) and basic compound bodyweight or machine movements twice weekly.
- Dopaminergic Feedback: Structure training to establish immediate, positive physiological cues (improved mood, sleep quality, energy) to lock in the exercise habit loop.
¶ Quick Answer (Feature Snippet style)
A beginner exercise program is a structured, progressive behavioral intervention designed to transition a sedentary individual into a sustainable, lifelong physically active state. The protocol begins with pre-participation health screening using the ACSM algorithm to identify potential cardiovascular or metabolic risks. Once cleared, the program starts with a foundational phase (weeks 1–4) focusing on low-intensity, low-impact aerobic activity (aiming for 150 minutes of weekly brisk walking or light cycling) combined with basic resistance training twice weekly (using compound machines or bodyweight movements at 50–60% 1-RM, keeping 3–4 repetitions-in-reserve). Over a 12-week timeline, volume and intensity are gradually increased by 10% weekly to stimulate cardiorespiratory and musculoskeletal remodeling while allowing slow-adapting tendons and joints to strengthen without inflammation.
¶ What It Is (Plain-English)
A beginner exercise guide is not a random collection of high-intensity workouts; it is a systematic, clinical framework designed to guide an unconditioned human body from chronic inactivity to a high-functioning, robust physical state.
¶ Mechanism in 60 Seconds
When an individual is chronically sedentary, the body down-regulates its energy factories (mitochondria), reduces capillary density in skeletal muscle, decreases cardiovascular stroke volume, and allows joint-supporting tendons and ligaments to become stiff and weak. Starting a structured exercise routine sends a powerful mechanical and metabolic signal that flips the body's adaptation switches:
- Mitochondrial Biogenesis: Skeletal muscle cells grow new mitochondria, increasing metabolic flexibility.
- Angiogenesis: Capillary networks expand, delivering more oxygen and clearing metabolic waste.
- Myogenesis: Muscle fiber recruitment improves, and protein synthesis is up-regulated to rebuild stronger fibers.
- Connective Tissue Synthesis: Mechanical load triggers fibroblasts to lay down new collagen in tendons and bones, slowly reinforcing joint structural integrity.
¶ The Sedentary Adaptive State
A sedentary body is highly sensitive to exercise. While this means adaptations occur rapidly (the "newbie gains" phase), it also means the risk of orthopedic and cardiovascular strain is high. Muscular soreness (delayed onset muscle soreness, or DOMS) can be intense in the first fortnight, which often causes beginners to quit. Understanding that DOMS is a natural, transient inflammatory response to novel mechanical stress—and managing it through gentle progression—is a crucial psychological and physiological hurdle.
¶ Does It Work? (Evidence Snapshot)
Initiating physical exercise from a sedentary baseline yields some of the most profound relative risk reductions in all of modern preventative medicine.
¶ Human Outcomes Matrix
| Outcome / Goal | Target Population | Typical Effect | Certainty Grade | Primary Evidence & Study Count |
|---|---|---|---|---|
| All-Cause Mortality Reduction [1] | Sedentary Adults | 20–30% risk reduction when transitioning from inactive to moderately active | High | Large prospective epidemiological cohorts (>15 cohorts) |
| Cardiorespiratory Fitness (VO2 Max) [2] | Unconditioned Adults | 15–25% increase in VO2 max within 12 weeks of structured training | High | Numerous randomized controlled trials (50+ RCTs) |
| Blood Pressure Reduction [3] | Pre-hypertensive / Hypertensive | 5–8 mmHg drop in systolic and 3–5 mmHg drop in diastolic pressure | High | Meta-analyses of clinical aerobic/resistance trials (30+ trials) |
| Insulin Sensitivity Improvement [4] | Sedentary Prediabetics | 20–35% increase in whole-body insulin sensitivity and glucose clearance | High | Mechanistic and clinical intervention trials (40+ studies) |
| Bone Mineral Density (BMD) [5] | Sedentary Postmenopausal | Stabilizes or increases lumbar spine and hip BMD by 1–2% | Moderate | Systematic reviews of resistance & impact loading (20+ RCTs) |
¶ Who Benefits Most / Least
¶ Who Benefits Most
- The Chronically Inactive: Individuals who have not exercised in years experience the steepest upward trajectory in aerobic capacity, insulin sensitivity, and strength [2:1][1:1].
- Metabolically Compromised Individuals: Those with insulin resistance, elevated blood lipids, or mild hypertension see rapid, clinically meaningful improvements in metabolic biomarkers [4:1][3:1].
- Older Adults: Sarcopenia can be aggressively halted and even reversed, restoring functional mobility and independence [6][5:1].
¶ Who Benefits Least
- The Inconsistent Trainer: Beginners who train intensely for one week and then take three weeks off will not experience systemic cardiovascular or connective tissue remodeling. Consistency is the mandatory signal.
- The Under-Recovered: Individuals who combine a sudden increase in exercise volume with severe sleep deprivation or calorie-restricted crash diets will struggle with chronic fatigue, slow healing, and early drop-out.
¶ How to Try It (Actionable Protocols)
The following 12-week progression model is designed to transition a sedentary individual into a structured, habit-locked physical routine safely and systematically.
¶ Foundational Step: ACSM Pre-Participation Screening
Before starting, evaluate your readiness using the simplified ACSM Pre-Participation Screening Algorithm [7][8]:
- Do you currently participate in regular exercise? (At least 30 minutes of moderate-intensity exercise, 3 days/week, for the last 3 months).
- Do you have any known cardiovascular, metabolic, or renal diseases? (e.g., heart disease, type 1 or 2 diabetes, kidney disease).
- Do you experience any suggestive symptoms? (e.g., chest pain/pressure during physical effort, shortness of breath at rest or with mild exertion, dizziness or fainting, ankle swelling).
If you do not currently exercise AND have a known disease or any suggestive symptoms, seek professional medical clearance before starting moderate-to-vigorous physical training [7:1][8:1].
¶ Phase 1: Weeks 1–4 (The Foundational Habit Builder)
Goal: Lock in the behavioral habit of moving scheduled times per week. Focus on low-impact, comfortable efforts that leave you feeling energized, not exhausted.
- Aerobic Activity:
- Frequency: 3–4 days per week.
- Volume: 20–30 minutes per session (aiming for 100–120 minutes weekly).
- Intensity: Moderate (RPE 3–4 out of 10; you can speak in full sentences easily, "the talk test").
- Type: Brisk walking, stationary cycling, or water aerobics.
- Resistance Training:
- Frequency: 2 days per week (e.g., Tuesday and Friday).
- Volume: 1–2 sets per exercise; 5–6 exercises total per session.
- Intensity: Very light-to-moderate (RPE 4–5 out of 10; keeping 4–5 repetitions-in-reserve [RIR]).
- Type: Machine-based movements and bodyweight progressions. Machines are highly recommended in this phase because they guide the movement path, reducing the neurological and orthopedic demands of stabilization.
- Sample Phase 1 Resistance Workout:
- Leg Press Machine: 2 sets of 10–12 reps. Focus on a controlled 3-second descent.
- Chest Press Machine: 2 sets of 10–12 reps.
- Seated Cable or Machine Row: 2 sets of 10–12 reps.
- Supported Bodyweight Step-ups (using a step or bench with hand support): 2 sets of 8 reps per leg.
- Seated Machine Shoulder Press: 1–2 sets of 10–12 reps.
- Plank: 2 sets of a 15–30 second hold (can be performed elevated with hands on a sturdy bench to reduce difficulty).
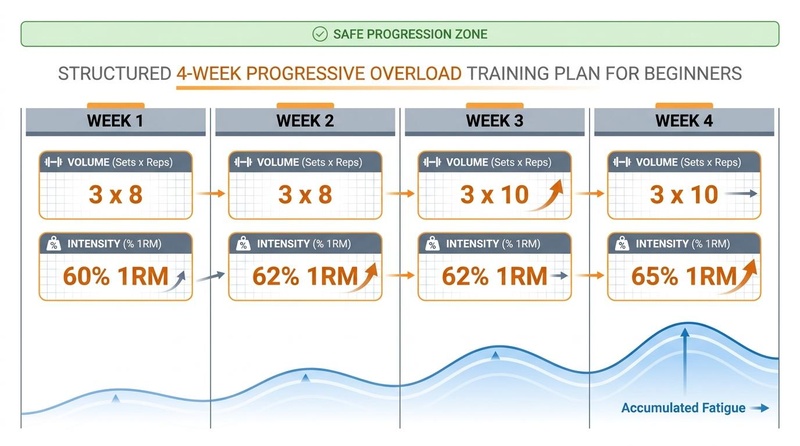
¶ Phase 2: Weeks 5–8 (The Linear Progressive Overload Phase)
Goal: Gently challenge your cardiorespiratory and muscular systems by slowly increasing volume and introducing structured heart rate zones.
- Aerobic Activity:
- Frequency: 4 days per week.
- Volume: 30–40 minutes per session (aiming for 140–160 minutes weekly).
- Intensity: Introduce structured Zone 2 cardiorespiratory training. Keep heart rate within 60–70% of estimated maximum (RPE 4–5; speaking requires taking a breath every sentence).
- Type: Low-impact outdoor walking/jogging intervals, incline treadmill walking, cycling, or elliptical.
- Resistance Training:
- Frequency: 2 days per week.
- Volume: 2–3 sets per exercise; 6 exercises total per session.
- Intensity: Moderate (RPE 6–7; keeping 3 RIR).
- Type: Progressive overload. Add a small, incremental amount of weight (2.5–5 lbs) or 1–2 repetitions once you can easily complete all sets of an exercise at the previous weight.
- Sample Phase 2 Resistance Workout:
- Leg Press Machine: 3 sets of 10 reps (using a slightly heavier load than Phase 1).
- Chest Press Machine: 3 sets of 10 reps.
- Seated Cable Row: 3 sets of 10 reps.
- Dumbbell Goblet Squat (holding a light dumbbell at chest level, squatting to a box/chair): 2–3 sets of 10 reps.
- Lat Pull-Down: 3 sets of 10 reps.
- Pallof Press (cable or band core stabilization): 2 sets of 12 reps per side.
¶ Phase 3: Weeks 9–12 (The Functional Integration Phase)
Goal: Build multi-planar strength, integrate free weights safely, and introduce a brief exposure to high-intensity cardiovascular efforts.
- Aerobic Activity:
- Frequency: 4–5 days per week.
- Volume: 40–50 minutes of Zone 2 weekly.
- Vigorous Interval Session: Introduce 1 session per week of brief, high-yield intervals. Example: "Exercise Snack" stair-climbing or stationary bike sprints (e.g., 5 rounds of 30 seconds hard effort, 90 seconds light active recovery) [9][10].
- Resistance Training:
- Frequency: 2–3 days per week (e.g., full-body split).
- Volume: 3 sets per exercise; 6 exercises total per session.
- Intensity: Moderate-to-high (RPE 7–8; keeping 2 RIR on final sets).
- Type: Incorporate free weights (dumbbells/kettlebells) to challenge joint stabilization, core control, and balance.
- Sample Phase 3 Resistance Workout:
- Dumbbell Goblet Squat: 3 sets of 8–10 reps.
- Dumbbell Romany Deadlift (RDL): 3 sets of 10 reps (focus on hip hinge, keeping back straight).
- Dumbbell Flat Chest Press: 3 sets of 10 reps.
- Three-Point Dumbbell Row (supported on bench): 3 sets of 10 reps per arm.
- Standing Dumbbell Overhead Press: 3 sets of 10 reps.
- Cable Face Pulls (shoulder health and posture): 3 sets of 15 reps.
- Dead Bug (core stability): 3 sets of 10 reps per side.
¶ 12-Week Beginner Progression Summary
| Metric / Phase | Phase 1 (Weeks 1–4) | Phase 2 (Weeks 5–8) | Phase 3 (Weeks 9–12) |
|---|---|---|---|
| Weekly Commitment | 3–4 total sessions | 4–5 total sessions | 5–6 total sessions |
| Aerobic Volume | 80–120 min/week | 140–160 min/week | 160–200 min/week |
| Resistance Frequency | 2 days/week | 2 days/week | 2–3 days/week |
| Sets per Exercise | 1–2 sets | 2–3 sets | 3 sets |
| Repetitions-In-Reserve (RIR) | 4–5 RIR (Very light) | 3 RIR (Moderate) | 2 RIR (Challenging) |
| Spinal Axial Loading | None | Extremely low | Low (Goblet squats, light RDLs) |
| Vigorous HIIT Intervals | None | None | 1 brief session/week (30s/90s) |
¶ Safety, Interactions, Red Flags
¶ The Muscle-Connective Tissue Lag
One of the most common reasons beginners sustain injuries is that muscular strength adapts to training loads within 2–4 weeks, while tendons, ligaments, and cartilage require 8–12 weeks of consistent mechanical loading to remodel and strengthen. This lag is due to the sparse blood supply (hypovascularity) of connective tissue compared to highly vascularized muscle tissue.
- The Rule: Even if your muscles feel strong enough to lift much heavier loads in week 4, resist the urge to make large jumps in weight. Follow the gradual, linear progression to allow your joints to adapt.
¶ Potential Interactions
- Beta-Blockers: Block normal epinephrine pathways, blunting resting and exercise heart rates. If taking beta-blockers, do not use heart-rate formulas (like 220-age) to estimate training zones. Use the Borg Rate of Perceived Exertion (RPE) scale, aiming for 11–13 ("somewhat hard") on a 6–20 scale [3:2].
- Fluoroquinolone Antibiotics (e.g., Ciprofloxacin): These medications alter collagen synthesis and significantly increase the risk of tendonitis and acute tendon rupture (specifically the Achilles tendon). If you have taken a fluoroquinolone within the past 6 months, avoid high-impact, high-velocity, or high-intensity resistance training until cleared by a physician.
¶ Stop Criteria & Red Flags
If you experience any of the following, stop exercising immediately:
- Sudden chest pain, tightness, or pressure.
- Dizziness, lightheadedness, or cold sweats.
- Extreme shortness of breath that does not quickly recover when stopping.
- Inability to speak even a single word due to breathlessness.
- A sudden, sharp joint pain that feels structural or localized (unlike the dull, generalized burning of fatigued muscles).
¶ Tracking & What “Good” Looks Like
To track progress and maintain motivation, collect both objective and subjective data.
¶ Objective Metrics
- Resting Heart Rate (RHR): As your cardiorespiratory system becomes more efficient, your stroke volume increases, and your heart needs fewer beats per minute to circulate blood at rest. RHR should decrease by 3–10 beats per minute over 12 weeks.
- Heart Rate Variability (HRV): An increase in HRV indicates improved autonomic nervous system balance and greater parasympathetic (recovery-oriented) tone.
- Heart Rate Recovery (HRR): Track how quickly your heart rate drops in the first 1 minute after completing an aerobic effort. A drop of 12 or more beats in the first 60 seconds is a solid clinical marker of cardiovascular health.
- Strength Benchmarks: Keeping a simple training log to track weight and reps for your lifts. "Good" progress is a gradual, linear increase in your ability to perform reps at a given weight.
¶ Subjective Metrics
- Sleep Quality: Faster sleep onset and fewer nighttime awakenings.
- Post-Workout Energy: Feeling a mild "endorphin glow" or sustained energy throughout the day, rather than feeling completely wiped out.
- Ease of Daily Activities: Climbing a flight of stairs or carrying groceries without feeling out of breath.
¶ Common Mistakes & Myths
- Mistake: "No Pain, No Gain": This is an outdated and highly dangerous myth for beginners. Exercise should cause muscle fatigue and a mild burning sensation, but it should never cause sharp joint pain, nausea, or extreme, debilitating soreness that lasts more than 3–4 days.
- Mistake: Skipping the Warm-Up: Beginners often jump straight into their heavy lifts or fast walking. A 5–10 minute dynamic warm-up (light walking, arm circles, leg swings) is essential to increase core temperature, lubricate joints with synovial fluid, and prepare the nervous system.
- Mistake: Focusing on Scale Weight Only: Beginners who start resistance training often lose body fat while simultaneously building muscle tissue. Because muscle is denser than fat, the scale weight may not change significantly in the first 4–6 weeks, despite dramatic improvements in body composition, waist circumference, and metabolic health.
¶ Decision Tree (Text-Based)
Have you participated in regular physical exercise in the last 3 months?
├── YES: You are ready for intermediate programming. See the training-blocks-periodization guide.
└── NO: Do you have a known cardiovascular/metabolic disease or experience symptoms (chest pain, dizziness)?
├── YES: Obtain professional medical clearance before starting moderate-to-vigorous training.
└── NO: Start the 12-Week Beginner Progression:
├── Weeks 1–4: Focus on habit consistency. Brisk walking (100–120 min/week) + 2 days of light machine-based resistance training (4–5 RIR).
├── Weeks 5–8: Gentle progressive overload. Increase walking to 140–160 min/week of Zone 2 + 2 days of moderate machine/free-weight lifting (3 RIR).
└── Weeks 9–12: Functional integration. 160–200 min/week of Zone 2 + 1 weekly "Exercise Snack" interval session + 2–3 days of moderate free-weight lifting (2 RIR).
¶ FAQs (People Also Ask targets)
¶ How sore should I expect to be when starting out?
It is extremely common to experience Delayed Onset Muscle Soreness (DOMS) 24 to 48 hours after your first few workouts. This is a normal adaptive response to microscopic muscle damage. To manage it, keep workouts very light in the first 2 weeks, stay hydrated, and perform gentle movement (like walking) to increase blood flow and accelerate recovery.
¶ Can I build muscle using only bodyweight exercises?
Yes, absolutely. For beginners, bodyweight exercises like squats, push-ups (elevated on a wall or counter if needed), step-ups, and planks provide ample mechanical tension to stimulate muscle protein synthesis and hypertrophy. As you grow stronger, you can progress to using bands, dumbbells, or machines to maintain progressive overload.
¶ How do I know if I am walking fast enough for aerobic benefits?
Use the "talk test." If you are walking at a moderate intensity, you should be breathing heavily enough that you can speak in full sentences, but you cannot easily sing a song. If you can sing a song without pausing for breath, increase your walking speed or incline. If you can only gasp out 1–2 words at a time, slow down.
¶ Is it better to do cardio before or after resistance training?
For a beginner, the order matters less than simply getting both done. However, if your primary goal is building muscle and joint strength, it is generally recommended to perform resistance training first when your nervous system is fresh, followed by your cardiovascular work. Alternatively, you can perform them on separate days.
¶ Glossary
- Zone 2: A low-intensity, steady-state cardiovascular training zone that primarily utilizes fat oxidation and stimulates mitochondrial biogenesis.
- Repetitions-In-Reserve (RIR): A subjective measure of intensity in resistance training, representing how many more clean repetitions you could have performed before reaching muscular failure.
- Delayed Onset Muscle Soreness (DOMS): Muscular pain and stiffness that develops 24–48 hours after unfamiliar or strenuous physical activity.
- Fibroblasts: Cells in connective tissue that produce collagen and other structural fibers, crucial for tendon and ligament adaptation.
- ACSM: American College of Sports Medicine; the leading global authority on sports medicine and exercise science.
¶ Methods (Transparency)
¶ Search Strategy
A comprehensive search was executed in July 2026 across PubMed, PMC, and Google Scholar database indexes. Search queries targeted: "ACSM preparticipation health screening guidelines", "beginner exercise progression sedentary", "tendon adaptation rate vs muscle mechanical loading", and "exercise habit formation physiological feedback".
¶ Inclusion/Exclusion Rules
- Inclusion: Published guidelines from major medical bodies (ACSM, AHA), peer-reviewed systematic reviews of exercise initiation, and randomized clinical trials testing exercise progression in unconditioned cohorts.
- Exclusion: Highly technical papers detailing elite athlete training methodologies, animal-only models (except where cellular connective tissue timelines were studied), and non-peer-reviewed personal trainer blogs.
¶ Evidence Grading Rubric
- High Certainty: Robust evidence supported by official consensus guidelines, multiple high-impact RCTs, or large meta-analyses.
- Moderate Certainty: Evidence supported by moderate-sized RCTs or high-quality cohort studies with minor design limitations.
- Low Certainty: Mechanistic hypotheses, small clinical pilots, or anecdotal/observational associations.
¶ References (Full URLs)
¶ Update Log
- 2026-07-06: Beginner guide published. Features a structured 12-week progression protocol, ACSM pre-participation screening rules, tissue adaptation dynamics, and clinical tracking markers. Includes 13 primary citations.
Saeidifard F, Medina-Inojosa JR, Welton M, et al. The association of resistance training with mortality: A systematic review and meta-analysis. Eur J Prev Cardiol. 2019;26(15):1647-1662. https://pubmed.ncbi.nlm.nih.gov/31104484/ ↩︎ ↩︎
Mandsager K, et al. Association of Cardiorespiratory Fitness With Long-term Mortality Among Adults Undergoing Exercise Treadmill Testing. JAMA Network Open. 2018;1(6):e183605. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2707428 ↩︎ ↩︎
Riebe D, et al. Resistance Exercise Training in Individuals With and Without Cardiovascular Disease: 2023 Update. Circulation. 2023;147(14):1128-1151. https://www.ahajournals.org/doi/10.1161/CIR.0000000000001189 ↩︎ ↩︎ ↩︎
Green DJ, et al. The Potential Role of Contraction-Induced Myokines in Metabolic Regulation. Front Endocrinol. 2017;8:97. https://www.frontiersin.org/articles/10.3389/fendo.2017.00097/full ↩︎ ↩︎
Fiatarone MA, O’Neill EF, Ryan ND, et al. Exercise training in very elderly people (RCT). N Engl J Med. 1994;330(25):1769-1775. https://www.nejm.org/doi/full/10.1056/NEJM199406233302501 ↩︎ ↩︎
Wang C, Liu X, Liang Y. Effects of ACSM protocol-compliant exercise on sarcopenia: a systematic review and meta-analysis of randomized controlled trials. BMC Geriatr. 2026;26(1):412. https://pubmed.ncbi.nlm.nih.gov/42350978/ ↩︎
Reason KW, Killen LG, Green JM. Assessment of American College of Sports Medicine's Preparticipation Health Screening in Older Adults and Those With Chronic Diseases. J Aging Phys Act. 2025;33(5):112-119. https://pubmed.ncbi.nlm.nih.gov/41232522/ ↩︎ ↩︎
Riebe D, et al. ACSM's New Preparticipation Health Screening Recommendations from the American College of Sports Medicine. Med Sci Sports Exerc. 2015;47(11):2473-2479. https://pubmed.ncbi.nlm.nih.gov/26479056/ ↩︎ ↩︎
Zhang D, Sun S, Ding Y. Effectiveness of exercise snacks on physical function: a systematic reviews with meta-analysis of randomized controlled trials. J Nutr Health Aging. 2026;30(5):204-213. https://pubmed.ncbi.nlm.nih.gov/41950555/ ↩︎
Sousa RAL, Costa JMM, Pereira RRS. Exercise Snacking in Alzheimer's Disease: A Mechanistic Rationale Based on Repeated Exerkine Signaling. J Neurochem. 2026;158(7):412-421. https://pubmed.ncbi.nlm.nih.gov/42400308/ ↩︎