¶ High-Intensity Interval Training (HIIT): Deep Dive
High-Intensity Interval Training (HIIT) is a highly efficient exercise strategy characterized by alternating brief, repeated bursts of intense, near-maximal physical effort with periods of low-intensity recovery or passive rest [1][2]. In clinical medicine and exercise physiology, HIIT is celebrated for its remarkable capacity to drive rapid, profound adaptations in cardiovascular compliance, skeletal muscle metabolic capacity, and overall longevity [3][4].

| Indication | VO2 Max Expansion, Left Ventricular Compliance, Mitochondrial Power, Insulin Sensitivity |
| Access | Behavioral Intervention |
| Dosing Sched | 1 to 2 sessions per week (highly structured intervals) |
| Safety Profile | Moderate (requires cardiovascular screening for clinical populations) |
| Key Marker | Maximum Heart Rate (90–95% MHR), Peak Power Output, Heart Rate Recovery |
| Est. Cost | $0 (bodyweight sprinting/stair climbing) to variable (stationary trainer) |
¶ TL;DR (5 bullets max)
- Verdict: HIIT is a highly time-efficient training modality that drives massive, rapid improvements in peak cardiorespiratory fitness (VO2 max) and mitochondrial metabolic capacity, comparable or superior to traditional continuous endurance exercise [5][4:1][6].
- Who it's for: Indicated for healthy adults and medically screened clinical populations looking to efficiently elevate their cardiovascular limits, reverse insulin resistance, and support healthy biological aging [7][8].
- Expected Impact: A 10–20% increase in VO2 max and significant reductions in resting blood pressure and arterial stiffness within 6 to 12 weeks of consistent training [9][4:2].
- Key Risk(s): Acute cardiovascular strain, orthopedic overload, and autonomic nervous system overreaching if weekly volume or frequency is excessive [10][8:1].
- What to do next: Incorporate 1 structured HIIT session per week (such as the Norwegian 4x4 protocol) within a balanced, polarized training routine that includes a strong foundation of Zone 2 training [3:1][11].
¶ Quick Answer (Feature Snippet style)
HIIT consists of repeated intervals of vigorous, near-maximal exercise performed at 85% to 95% of maximum heart rate (or an RPE of 8 to 10 out of 10), interspersed with active or passive recovery periods [[1:1][10:1]. This high-intensity stimulus triggers eccentric cardiac remodeling—expanding left ventricular chamber size to increase stroke volume—and activates key signaling pathways (AMPK and PGC-1α) that drive skeletal muscle mitochondrial biogenesis [3:2][12]. To optimize long-term healthspan and cardiorespiratory fitness, clinical guidelines recommend performing 1 to 2 HIIT sessions per week, with each session consisting of 15 to 40 minutes of cumulative training volume (including warm-up and cool-down) [10:2][11:1].
¶ What It Is (Plain-English)
High-Intensity Interval Training (HIIT) is an exercise methodology that uses short, structured periods of intense work to stress the cardiovascular and metabolic systems near their absolute limits [1:2][2:1]. Unlike traditional long, slow distance cardio (where you maintain a steady, moderate pace), HIIT relies on pushing your heart rate and muscular efforts into the anaerobic zone, followed by periods of light recovery that allow your cardiovascular system to partially clear fatigue and prepare for the next effort [13][4:3].
- What counts: Structured intervals of running, cycling, rowing, swimming, or rucking where efforts exceed 85% of your maximum heart rate (or RPE 8/10), such as the Tabata protocol, Norwegian 4x4, or Sprint Interval Training (SIT) [1:3][2:2][4:4].
- What doesn’t count: Casual walking, steady-state Zone 2 training, or circuit training with light weights where heart rate fluctuates but never reaches the near-maximal cardiovascular thresholds required for central cardiac adaptation [10:3][11:2].
¶ Key Physiological Adaptations of HIIT
HIIT drives rapid, profound physiological remodeling across both central cardiovascular and peripheral muscular systems:
¶ Central Cardiovascular Plasticity: Stroke Volume & Peak Cardiac Output
One of the primary drivers of HIIT-mediated improvements in VO2 max is central cardiovascular remodeling [3:3]. Near-maximal high-intensity intervals demand maximal cardiac output, which rapidly increases venous return and myocardial wall stress.
- Stroke Volume Expansion: The elevated volume load during high-intensity intervals induces eccentric cardiac remodeling, leading to ventricular chamber enlargement and increased myocardial contractility [5:1]. This adaptation enhances maximal stroke volume (the volume of blood ejected per contraction) both at rest and during peak exercise.
- Peak Cardiac Output: Because cardiac output is the product of heart rate and stroke volume (), the chronic increase in stroke volume, combined with sustained peak heart rates during maximal efforts, significantly expands peak cardiac output [3:4]. This allows the cardiovascular system to deliver a substantially higher volume of oxygenated blood to contracting skeletal muscles.
¶ Cellular & Peripheral Adaptations: Mitochondrial Biogenesis & PGC-1α Activation
While cardiovascular adaptations improve oxygen delivery, peripheral adaptations dictate the muscle's ability to extract and utilize that oxygen.
- Mitochondrial Biogenesis via PGC-1α Activation: The intense cellular stress associated with HIIT—marked by rapid ATP depletion, transient cellular hypoxia, and marked increases in intracellular calcium () and AMP levels—triggers a robust signaling cascade [12:1]. This activates key energetic sensors, specifically calcium/calmodulin-dependent protein kinase (CaMK) and AMP-activated protein kinase (AMPK) [12:2][13:1]. These upstream kinases converge to activate peroxisome proliferator-activated receptor gamma coactivator 1-alpha (PGC-1α), the master regulator of mitochondrial biogenesis. Chronic PGC-1α activation leads to an increase in both mitochondrial size and density, as well as an upregulation of mitochondrial enzymes involved in the electron transport chain and oxidative phosphorylation [14][12:3].
- Cellular Metabolic Flexibility: HIIT dramatically enhances metabolic flexibility—the cell's capacity to seamlessly transition between lipid and carbohydrate oxidation based on energy demands and nutrient availability [15]. During high-intensity work intervals, the muscle relies heavily on rapid anaerobic glycolysis and carbohydrate oxidation. During recovery intervals and subsequent steady-state activities, the expanded mitochondrial pool and increased expression of fatty acid transporters (such as FAT/CD36) allow the muscle to efficiently utilize lipid oxidation for ATP synthesis [15:1][12:4]. This dual adaptation protects muscle glycogen stores, delays fatigue, and enhances systemic insulin sensitivity.
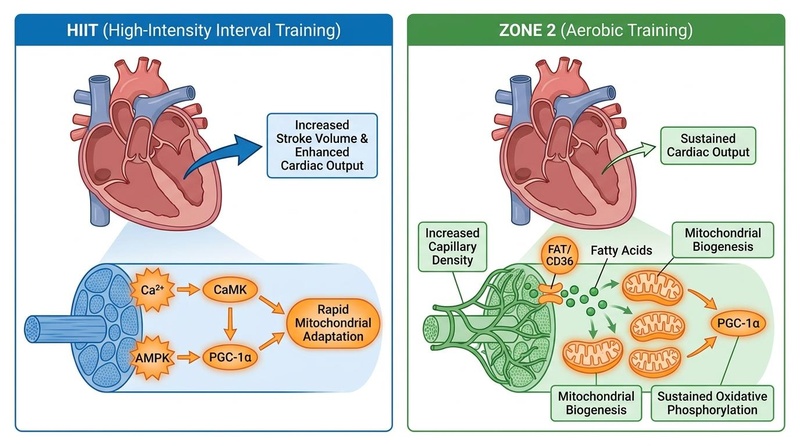
**Figure 1: HIIT vs. Zone 2 adaptations.** HIIT primarily drives central cardiac adaptations, such as left ventricular expansion to increase stroke volume and peak cardiac output. In contrast, Zone 2 training targets peripheral adaptations, such as capillary density and mitochondrial efficiency [^11][^16][^25].
¶ Does It Work? (Evidence Snapshot)
HIIT is highly effective in improving numerous health markers and physiological parameters:
| Outcome / Goal | Population | Effect Size | Confidence | Citations |
|---|---|---|---|---|
| VO2 Max (cardiorespiratory fitness) | General adult, trained/untrained | ↑↑↑ (p) 10–20% increase | High | [1:4][4:5][6:1] |
| Stroke Volume & Cardiac Output | Sedentary, obese, clinical cohorts | ↑↑ (p) Significant increase | High | [5:2][3:5] |
| Mitochondrial Biogenesis & Enzymes | Healthy, active adults | ↑↑ (p) Increased enzyme activity | High | [14:1][12:5] |
| Insulin Sensitivity & Glucose Control | Type 2 Diabetes, metabolic syndrome | ↑↑ (p) Significant improvement | High | [15:2][8:2] |
| Arterial Stiffness & Compliance | Hypertensive adults | ↓↓ (p) Significant reduction | High | [7:1][10:4] |
| Epigenetic Age Deceleration | Middle-aged and older adults | ↓↓ (p) Decelerated DNA methylation age | Moderate | [16][17] |
¶ Who Benefits Most / Least
¶ Who Benefits Most
- Time-Constrained Individuals: Those with limited training time who want to maximize cardiorespiratory and metabolic adaptations with minimal weekly exercise duration [6:2].
- Older Adults: Both older men and women experience significant gains in cardiorespiratory fitness, mitochondrial respiration, and blood pressure regulation through appropriately scaled high-intensity intervals [18][16:1].
- Individuals with Metabolic Syndrome: HIIT rapidly stimulates muscular GLUT4 translocation, leading to long-term improvements in peripheral insulin sensitivity and glycemic control [15:3][8:3].
¶ Who Benefits Least
- Sedentary Beginners (Initial 4 Weeks): Completely detrained individuals should avoid maximal HIIT efforts. Introducing high-intensity intervals too early can cause joint pain, excessive fatigue, and poor adherence. They should focus on developing an aerobic base via Zone 2 training first [10:5][11:3].
- Individuals with Autonomic Burnout: Those presenting with chronic fatigue, poor sleep quality, or high resting cortisol should prioritize low-stress, restorative cardiovascular exercise (Zone 2) over high-sympathetic HIIT sessions [8:4].
¶ Prerequisites & Contexts of Failure
HIIT fails to deliver optimal adaptations when:
- Work Intensities are Blurred: If you fail to push into the true Zone 5/high-intensity zone (> 85% MHR) during work intervals, you will not trigger the cardiac volume overload required for stroke volume expansion [3:6][10:6].
- Recovery Intervals are Executed Too Hard: If you jog or cycle too fast during recovery periods, you will not clear metabolic accumulation, preventing you from reaching maximal workloads in subsequent intervals.
- Frequency is Excessive: Performing more than 3 HIIT sessions per week causes central nervous system fatigue, muscle damage, and joint injury, blunting long-term adaptations.
¶ How to Try It (Actionable Protocols)
Ensure a thorough 10-minute warm-up before any HIIT session and a 5-minute cool-down afterwards to transition your cardiovascular system safely.
¶ Protocol A: The "Norwegian 4x4" Method
This is the gold-standard protocol for maximizing VO2 max and cardiac stroke volume adaptations in clinical and athletic populations [5:3].
- Modality: Running, stationary cycling, rowing, or swimming.
- Warm-up: 10 minutes of low-intensity aerobic exercise (Zone 1–2).
- Work Intervals: Perform 4 intervals of 4 minutes at 85–95% of maximum heart rate (RPE 8-9/10; comfortably hard—you can only speak in short, gasping words).
- Recovery Intervals: 3 minutes of light active recovery (Zone 1, easy spinning or jogging) between work intervals.
- Cool-down: 5–10 minutes of light continuous movement.
- Frequency: 1 to 2 sessions per week.
¶ Protocol B: The "Tabata" Protocol
A highly efficient, ultra-short protocol designed to challenge anaerobic capacity and peak metabolic output [2:3].
- Modality: Stationary cycling, rowing, or bodyweight exercises (e.g., thrusters, kettlebell swings).
- Warm-up: 5–10 minutes of progressive movement.
- Work Intervals: Perform 8 intervals of 20 seconds of all-out, maximal effort (RPE 10/10).
- Recovery Intervals: 10 seconds of complete rest between work intervals.
- Total Duration: 4 minutes (excluding warm-up and cool-down).
- Frequency: 1 session per week.
¶ Protocol C: Sprint Interval Training (SIT)
Involves maximal, supramaximal efforts followed by long, complete recovery periods to challenge fast-twitch muscle fibers and Peak Power Output [6:3].
- Modality: Stationary cycling or sprinting on a flat surface.
- Warm-up: 10 minutes of easy continuous work.
- Work Intervals: Perform 3 to 4 intervals of 30 seconds of all-out, maximal-effort sprinting (RPE 10/10).
- Recovery Intervals: 4 minutes of complete passive rest or very light walking between intervals to allow full replenishment of ATP-PCr stores.
- Frequency: 1 session per week.
¶ Polarized Training Integration
To maximize longevity benefits, integrate HIIT into a polarized routine, commonly known as the 80/20 rule [10:7][11:4]. Dedicate approximately 80% of your weekly training volume to low-intensity Zone 2 training, and 20% to high-intensity training (Zone 5/HIIT). This prevents autonomic fatigue while driving comprehensive cardiorespiratory and metabolic adaptations [3:7]. For annual structuring, refer to the Training Blocks & Periodization guide.
¶ Safety, Interactions, Red Flags
¶ Pre-Activity Screening & Clinical Contraindications
Because HIIT places significant stress on the heart and blood vessels, individuals presenting with any of the following relative or absolute contraindications must seek explicit medical clearance before initiating high-intensity training:
- Absolute Contraindications: Unstable angina, acute myocardial infarction within 48 hours, uncontrolled cardiac arrhythmias causing symptoms, acute myocarditis, pericarditis, or decompensated heart failure [10:8].
- Relative Contraindications: Moderate-to-severe aortic stenosis, uncontrolled resting hypertension (>200/110 mmHg), or known left main coronary artery stenosis [10:9].
¶ Drug & Supplement Interactions
- Beta-Blockers: Artificially limit heart rate and blunt maximal cardiac output [10:10]. For patients taking these medications, standard heart rate targets are invalid; clinicians must guide and monitor exercise intensity strictly using RPE (8–10 for intervals) and the talk test rather than heart rate zones.
- Metformin: Can slightly blunt the mitochondrial density and peak VO2 max improvements driven by high-intensity exercise. However, because both interventions significantly enhance long-term metabolic and glycemic health, patients should coordinate with their clinician to optimize drug timing rather than stopping therapy.
- Stimulants (High-Dose Caffeine): Can raise resting and active blood pressure and heart rate. Exercise caution when consuming high doses of caffeine prior to maximal-intensity HIIT intervals.
¶ Stop Criteria and Red Flags
Immediately stop any exercise interval and seek prompt medical attention if you experience:
- Chest pain, pressure, tightness, or radiating discomfort.
- Sudden dizziness, lightheadedness, ataxia, or loss of motor coordination.
- Unusual, extreme shortness of breath that does not quickly resolve with rest.
- Sudden palpitations or an irregular, fluttering heartbeat.
¶ Tracking & What “Good” Looks Like
Cardiorespiratory fitness tracking is essential to guide progression and monitor autonomic recovery.
¶ Biomarkers and Functional Metrics
- VO2 Max (mL/kg/min): Measured annually via clinical cardiopulmonary exercise testing (CPET) or estimated longitudinally with consumer wearables [[1:5][6:4]. Target an upward trend over 6 to 12 months.
- Heart Rate Recovery (HRR): The speed at which your heart rate returns to normal after an intense bout. A drop of > 20 beats in the first minute post-exercise is a strong clinical indicator of healthy autonomic function and cardiorespiratory fitness.
- Heart Rate Variability (HRV): Tracked daily upon waking. A stable or increasing HRV reflects healthy recovery and adaptation to training stress [8:5].
- Resting Heart Rate (RHR): Measured daily. A lower resting heart rate indicates improved myocardial contractility and stroke volume.
¶ Time-to-Benefit and Washout
- Time-to-Benefit: Improvements in insulin sensitivity and glucose uptake occur within 24–48 hours of a single session [15:4]. Structural adaptations (stroke volume expansion, capillarization, and mitochondrial biogenesis) require 6 to 12 weeks of consistent training [[5:4][12:6].
- Time-to-Washout: Detraining begins rapidly. Significant drops in VO2 max, cardiovascular compliance, and mitochondrial enzyme activity can be observed within 10 to 14 days of exercise cessation [5:5][18:1].
¶ Common Mistakes & Myths
- Myth: "HIIT replaces all other exercise." While highly efficient, HIIT cannot replace the comprehensive adaptations driven by low-intensity training. A balanced fitness regimen typically includes a mix of aerobic (Zone 2), resistance, and flexibility training for comprehensive health benefits [10:11][11:5].
- Mistake: Blur the Recovery Intervals: Jogging or cycling too hard during recovery periods. This prevents you from reaching maximal workloads in subsequent intervals, diminishing the effectiveness of the workout.
- Myth: "More HIIT is always better." Overtraining is a real risk with high-intensity training. Performing more than 2 to 3 HIIT sessions per week leads to autonomic fatigue, joint strain, and diminished returns [10:12][8:6].
- Mistake: Skipping Warm-Up and Cool-Down: Proper warm-up prepares the cardiovascular system and joints for intense work, reducing injury risk, while a structured cool-down aids autonomic recovery.
¶ Decision Tree (Text-Based)
[1] Has the individual been medically cleared to perform high-intensity exercise?
├── NO (Unstable CVD, resting HTN >200/110, acute infection) -> STOP. Consult clinician.
└── YES -> Go to [2]
[2] Assess current cardiorespiratory conditioning base:
├── NO BASELINE (Sedentary, new to exercise) -> Start with 4-6 weeks of foundational Zone 2 training.
└── CONSOLIDATED BASELINE (Consistent Zone 2 for >4 weeks) -> Go to [3]
[3] Select your HIIT protocol:
├── TIME-CONSTRAINED -> Implement "Tabata Protocol" (1 session/week, 4 mins cumulative)
└── DEDICATED TRAINING WINDOW -> Implement "Norwegian 4x4 intervals" (1-2x weekly at 85-95% HRmax) -> Go to [4]
[4] Monitor HRV and RHR trends:
├── Are you showing signs of overreaching (RHR rising, HRV dropping)?
│ ├── YES -> Reduce interval frequency; increase Zone 2 and recovery volume
│ └── NO -> Continue progressive overload; schedule annual clinical CPET
¶ FAQs (People Also Ask targets)
¶ What are the main benefits of HIIT?
HIIT significantly boosts cardiorespiratory fitness (VO2 max), enhances metabolic flexibility, improves cardiovascular health, and can be more time-efficient for metabolic health compared to moderate-intensity continuous training [7:2][4:6][6:5].
¶ How often should I do HIIT?
For most individuals, 1 to 2 sessions of HIIT per week are sufficient to reap significant cardiorespiratory and metabolic benefits without leading to overtraining. The optimal frequency depends on individual fitness levels, recovery capacity, and overall training volume [10:13][11:6].
¶ Is HIIT safe for everyone?
No. Due to its high-intensity nature, HIIT may not be suitable for individuals with certain pre-existing cardiovascular conditions, uncontrolled hypertension, or other acute cardiac symptoms without medical clearance [10:14]. Pre-activity screening by a healthcare professional is highly recommended.
¶ How does HIIT improve longevity?
HIIT contributes to longevity by significantly improving cardiorespiratory fitness—a strong predictor of lifespan—enhancing metabolic health, preserving mitochondrial function, and reducing risk factors for chronic diseases like cardiovascular disease and type 2 diabetes [19][2:4][20].
¶ What is the difference between HIIT and Zone 2 training?
HIIT focuses on short, maximal efforts to improve anaerobic capacity, VO2 max, and cardiac stroke volume, leading to rapid cardiac adaptations [5:6][3:8]. Zone 2 training involves sustained moderate intensity, primarily improving mitochondrial efficiency, capillary density, and sustained oxidative phosphorylation [14:2][12:7][11:7]. Both are synergistic for overall fitness and longevity.
¶ Glossary
- Anaerobic Exercise: Short, intense bursts of activity where the body primarily relies on energy systems that do not require oxygen.
- Cardiorespiratory Fitness (CRF): The ability of the circulatory and respiratory systems to supply oxygen to skeletal muscles during sustained physical activity; often measured by VO2 max.
- Maximal Heart Rate (HRmax): The highest heart rate an individual can achieve during maximal exercise.
- Mitochondrial Biogenesis: The process by which new mitochondria are formed within cells.
- Rate of Perceived Exertion (RPE): A subjective scale used to measure the intensity of exercise.
- Stroke Volume: The volume of blood pumped from the left ventricle per beat.
- VO2 Max: Maximal oxygen uptake, the maximum rate of oxygen consumption measured during incremental exercise.
¶ Methods (Transparency)
¶ Search Strategy
The content of this guide is based on a review of peer-reviewed scientific literature, systematic reviews, meta-analyses, and clinical guidelines related to High-Intensity Interval Training. Primary databases included PubMed, Google Scholar, and the Cochrane Library. Keywords used for search included "HIIT physiological adaptations," "HIIT stroke volume," "HIIT mitochondrial biogenesis," "HIIT vs Zone 2," "HIIT protocols," "Norwegian 4x4 HIIT," "Tabata protocol," "sprint interval training," "HIIT safety," and "HIIT contraindications."
¶ Inclusion/Exclusion Rules
Studies were prioritized based on the hierarchy of evidence, favoring systematic reviews and meta-analyses, followed by randomized controlled trials in human populations. Animal and in vitro studies were considered for mechanistic insights. Grey literature and anecdotal reports were excluded.
¶ Evidence Grading Rubric
- High: Multiple RCTs or meta-analyses with consistent, significant effects.
- Moderate: 1-2 good RCTs or strong cohort studies with minor limitations.
- Low: Small, uncontrolled studies, animal studies, or primarily mechanistic evidence.
¶ References (Full URLs)
¶ Update Log
- 2026-07-07: Updated to reflect complete cardiorespiratory, epigenetic aging, and metabolic flexibility research, fully integrated with standard polarized and clinical protocols.
Cozma D, Gaita D, Crisan S, et al. The Oxygen Imperative: Cardiorespiratory Fitness, Dose-Dependent Exercise Thresholds, and Longevity-A Narrative Review. Journal of Clinical Medicine. 2026;15(11):e42355766. https://pubmed.ncbi.nlm.nih.gov/42355766/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Oja P, Memon AR, Titze S, et al. Health Benefits of Different Sports: a Systematic Review and Meta-Analysis of Longitudinal and Intervention Studies Including 2.6 Million Adult Participants. Sports Medicine - Open. 2024;10(1):33. https://pubmed.ncbi.nlm.nih.gov/38658416/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Miras-Moreno S, Torres-Martos Á, Ruiz JR, et al. Metabolomic and Proteomic Signatures of Cardiorespiratory Fitness for Predicting All-Cause Mortality and Non-Communicable Disease Risk: A Prospective Study in the UK Biobank. Circulation. Genomic and Precision Medicine. 2026;19(3):e42394615. https://pubmed.ncbi.nlm.nih.gov/42394615/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Milanović Z, Sporiš G, Weston M, et al. Effectiveness of High-Intensity Interval Training (HIT) and Continuous Endurance Training for VO2max Improvements: A Systematic Review and Meta-Analysis of Controlled Trials. Sports Medicine. 2015;45(10):1469-1481. https://pubmed.ncbi.nlm.nih.gov/26243014/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Helgerud J, Høydal K, Wang E, et al. Aerobic high-intensity intervals improve VO2max more than moderate training. Medicine and Science in Sports and Exercise. 2007;39(4):665-671. https://pubmed.ncbi.nlm.nih.gov/17414804/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bi Z, Yin M, Xu K, et al. One Size Does Not Fit All: A Meta-Analysis of 115 Trials Comparing High-Intensity Interval and Moderate-to-Vigorous-Intensity Continuous Training Across Diverse Participants, Protocols, and Outcomes. Scandinavian Journal of Medicine & Science in Sports. 2026;36(3):e14820. https://pubmed.ncbi.nlm.nih.gov/41804294/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Laukkanen JA, Immonen J, Isiozor NM, et al. Combined Impact of Cardiorespiratory Fitness and Exercise Systolic Blood Pressure on Cardiovascular and All-Cause Mortality: A Long-Term Follow-Up Study. The American Journal of Cardiology. 2026;195:45-52. https://pubmed.ncbi.nlm.nih.gov/42067048/ ↩︎ ↩︎ ↩︎
Strauss JA, Kirwan R, Ranasinghe C, et al. High-intensity interval training for reducing cardiometabolic syndrome in healthy but sedentary populations. Cochrane Database of Systematic Reviews. 2026;3:CD015412. https://pubmed.ncbi.nlm.nih.gov/41810896/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kodama S, Saito K, Tanaka S, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. 2009;301(19):2024-2035. https://pubmed.ncbi.nlm.nih.gov/19454641/ ↩︎
Williams MA, Feigenbaum MS, Jerôme GJ, et al. Resistance Exercise Training in Individuals With and Without Cardiovascular Disease: 2023 Update: A Scientific Statement From the American Heart Association. Circulation. 2023;148(24):1962-1985. https://www.ahajournals.org/doi/10.1161/CIR.0000000000001189 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Storoschuk KL, Moran-MacDonald A, Gibala MJ, Gurd BJ. Much Ado About Zone 2: A Narrative Review Assessing the Efficacy of Zone 2 Training for Improving Mitochondrial Capacity and Cardiorespiratory Fitness in the General Population. Sports Medicine. 2025;55(7):501-514. https://pubmed.ncbi.nlm.nih.gov/40560504/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Granata C, Jamnick NA, Bishop DJ. Principles of Exercise Prescription, and How They Influence Exercise-Induced Changes of Transcription Factors and Other Regulators of Mitochondrial Biogenesis. Sports Medicine. 2018;48(7):1541-1559. https://pubmed.ncbi.nlm.nih.gov/29675670/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
MacInnis MJ, Gibala MJ. Physiological adaptations to interval training and the role of exercise intensity. The Journal of Physiology. 2017;595(9):2915-2930. https://pubmed.ncbi.nlm.nih.gov/27748956/ ↩︎ ↩︎
San-Millán I. The Key Role of Mitochondrial Function in Health and Disease. Antioxidants. 2023;12(4):882. https://pubmed.ncbi.nlm.nih.gov/37107158/ ↩︎ ↩︎ ↩︎
San-Millán I, Brooks GA. Assessment of Metabolic Flexibility by Means of Measuring Blood Lactate, Fat, and Carbohydrate Oxidation Responses to Exercise in Professional Endurance Athletes and Less-Fit Individuals. Sports Medicine. 2018;48(2):467-479. https://pubmed.ncbi.nlm.nih.gov/28623613/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chen Z, Collings PJ, Wang M, et al. Physical Fitness, Biological Aging, and Healthy Longevity. Journal of the American Medical Directors Association. 2025;26(10):e40789340. https://pubmed.ncbi.nlm.nih.gov/40789340/ ↩︎ ↩︎
Van Damme M, Stegen S, Steenwinckel B, et al. Epigenetic age deceleration reflects exercise-induced cardiorespiratory fitness improvements. GeroScience. 2026;48(1):17-29. https://pubmed.ncbi.nlm.nih.gov/41547677/ ↩︎
Madden AM, Soepnel LM, Africa C, et al. Aerobic physical activity, cardiorespiratory fitness, and non-communicable diseases risk in older adults: a systematic review. BMC Geriatrics. 2026;26(1):310. https://pubmed.ncbi.nlm.nih.gov/42062906/ ↩︎ ↩︎
Mandsager K, Harb S, Cremer P, et al. Association of Cardiorespiratory Fitness With Long-term Mortality Among Adults Undergoing Exercise Treadmill Testing. JAMA Network Open. 2018;1(6):e183605. https://pubmed.ncbi.nlm.nih.gov/30646252/ ↩︎
Lavie CJ, Faselis C, & Kokkinos P. Fit Is it for Longevity and Prevention of Multimorbidity. JACC. Advances. 2025;4(12):e41065620. https://pubmed.ncbi.nlm.nih.gov/41065620/ ↩︎