¶ Lactate Threshold Training: Deep Dive
Lactate threshold training represents one of the most powerful and scientifically validated strategies to enhance cardiorespiratory endurance, shift metabolic clearance kinetics, and support overall cardiovascular longevity [1][2][3]. In clinical exercise physiology, the lactate threshold is not a single point but rather a dual-stage transition in muscle metabolism that reflects the balance between systemic lactate production and metabolic clearance [4][5].

| Indication | Metabolic Clearance Capacity, Cardiorespiratory Endurance, Anaerobic Threshold Shifting, Mitochondrial Power Output |
| Access | Behavioral Intervention |
| Dosing Sched | 1 to 2 targeted sessions per week within a periodized routine |
| Safety Profile | Moderate (high sympathetic and cardiovascular load during threshold efforts) |
| Key Marker | Blood Lactate (stable at LT1 vs LT2), Heart Rate at LT, Power/Pace at LT |
| Est. Cost | $0 to variable (portable lactate analyzer cost: $150–$250) |
¶ TL;DR (5 bullets max)
- Verdict: Lactate threshold training shifts the boundary of metabolic stability, allowing individuals to sustain higher workloads with minimal metabolic stress and lower systemic fatigue, which directly correlates with cardiovascular resilience and extended healthspan [4:1][6][3:1].
- Who it's for: Essential for athletes and adults of all ages looking to improve aerobic speed, enhance metabolic flexibility, and maximize structural cardiorespiratory efficiency [1:1][7].
- Expected Impact: Shifting the second lactate threshold (LT2) upward by 5–15% in power or pace, alongside a 10–20% increase in systemic lactate clearance rate, over a 6-to-12 week training block [2:1][8].
- Key Risk(s): Significant autonomic nervous system fatigue and overreaching if threshold sessions are performed too frequently or with inadequate recovery; muscle strain and joint overuse [9][10].
- What to do next: Integrate 1–2 focused threshold interval sessions (e.g., 2 x 10 or 2 x 15 minutes at LT2) into a weekly routine supported by a broad foundation of Zone 2 training [2:2][11].
¶ Quick Answer (Feature Snippet style)
The lactate threshold is divided into two distinct physiological markers: Lactate Threshold 1 (LT1/Aerobic Threshold), the point where blood lactate first begins to rise above resting levels (typically around 1.5 to 2.0 mmol/L), and Lactate Threshold 2 (LT2/Anaerobic Threshold/Maximal Lactate Steady State), the point where lactate production and clearance reach a maximal equilibrium (typically around 3.0 to 4.5 mmol/L) [4:2][5:1]. Training to improve these thresholds involves structured, sustained efforts just below or at LT2 (e.g., 85–90% of maximum heart rate) [2:3][12]. This stresses metabolic transport proteins (MCT-1 and MCT-4), upregulating cellular lactate clearance and delaying anaerobic acidosis, which dramatically expands functional aerobic capacity and cardiorespiratory health [2:4][8:1].
¶ What It Is (Plain-English)
Lactate threshold training is a method of exercise programming designed to increase the maximum speed or power output you can maintain without experiencing rapid, fatiguing acid buildup in your muscles [[4:3][5:2]. During low-intensity exercise, your body easily clears the small amounts of lactate your muscles produce. However, as intensity increases, your muscles rely more on carbohydrates, and lactate production begins to outpace your cell's clearing capabilities, leading to local muscular fatigue [4:4][13].
- What counts: Structured continuous runs or cycles at a "comfortably hard" tempo, long intervals (e.g., 8 to 20 minutes) at or near your LT2, and lactate-guided threshold intervals (such as the Norwegian method) where blood lactate is closely monitored and kept within a precise target range [2:5][10:1].
- What doesn’t count: Casual walking, short "all-out" sprint intervals under 1 minute with long passive recovery, or slow recovery runs where blood lactate remains completely at baseline [11:1].
¶ Distinguishing LT1 and LT2
- Lactate Threshold 1 (LT1 / Aerobic Threshold): This represents the transition from pure fat oxidation to mixed fat-carbohydrate metabolism. It corresponds to the top of Zone 2. At this intensity, blood lactate rises slightly above resting baseline (e.g., from 0.8 mmol/L to 1.5–2.0 mmol/L) but remains fully stable over hours [4:5][11:2].
- Lactate Threshold 2 (LT2 / Anaerobic Threshold / Maximal Lactate Steady State): This represents the upper boundary of metabolic stability. At any intensity at or below LT2, your body can match lactate production with clearance, keeping blood lactate stable (typically 3.0 to 4.5 mmol/L). At any intensity above LT2, lactate production outpaces clearance, causing blood lactate and hydrogen ions to accumulate exponentially, forcing volitional fatigue within 10 to 60 minutes [4:6][5:3][8:2].
¶ Mechanism in 60 Seconds
Think of lactate threshold training as expanding the lanes and drainage capacity of a highway during rush hour.
When muscle fibers contract at high intensities, they break down glucose into pyruvate, producing lactate and hydrogen () ions [5:4][13:1].
To prevent acid buildup, Type II (fast-twitch) muscle fibers use MCT-4 (monocarboxylate transporter 4) proteins to export lactate and hydrogen ions out of the cell into the interstitial space [2:6].
Type I (slow-twitch) muscle fibers and cardiac muscle cells then use MCT-1 (monocarboxylate transporter 1) proteins to import this circulating lactate directly into their cytoplasm and mitochondria [2:7][5:5].
Inside the mitochondria, mLDH (mitochondrial lactate dehydrogenase) converts lactate back into pyruvate, which enters the Krebs cycle to produce ATP via oxidative phosphorylation [8:3].
Lactate threshold training directly stimulates the transcription of genes encoding MCT-1, MCT-4, and mLDH, significantly increasing the cell's "lactate clearance highway" and shifting the metabolic threshold to higher absolute workloads [2:8][5:6][8:4].
**Figure 1: Cellular adaptations and transport systems.** High-intensity threshold intervals challenge both fast-twitch and slow-twitch muscle fibers, driving simultaneous adaptations in MCT-4 (lactate export) and MCT-1 (lactate import/oxidation) transporter systems to maximize metabolic clearance rate [[^7][^8][^10].
¶ Does It Work? (Evidence Snapshot)
Physiological and clinical evidence demonstrates that shifting the lactate threshold is one of the most reliable markers of improved exercise economy and metabolic flexibility:
| Outcome / Goal | Typical Effect | Certainty | Timeframe | Citations |
|---|---|---|---|---|
| Shift in LT2 Power/Pace | Shifting LT2 to a higher percentage of VO2 max (from 60–70% in untrained up to 85–90% in highly trained). | High | 6–12 weeks | [2:9][12:1][14] |
| Upregulation of MCT-1 & MCT-4 | 20–40% increase in monocarboxylate transporter protein expression in skeletal muscle tissue. | High | 6–8 weeks | [2:10][5:7] |
| Metabolic Clearance Rate | Enhanced systemic lactate clearance during submaximal work, reducing metabolic stress and systemic acidosis. | High | 8–12 weeks | [4:7][8:5] |
| Cardiorespiratory Endurance | Pronounced improvements in time-to-exhaustion at submaximal workloads (+15–30%). | High | 6–12 weeks | [1:2][3:2] |
| Metabolic Flexibility | Upregulated mitochondrial enzyme activity, preserving muscle glycogen and reducing dependency on fast glycolysis. | Moderate | 8 weeks | [4:8][13:2] |
¶ Shift in LT2 Power and Pace
In untrained or moderately active populations, LT2 occurs at a relatively low intensity, typically 60% to 70% of VO2 max [4:9]. With structured lactate threshold training, the body upregulates metabolic transporters and mitochondrial enzymes, shifting LT2 to 80% to 90% of VO2 max [2:11]. This means a highly trained individual can maintain a pace near their maximum aerobic limit for extended durations without experiencing metabolic acidosis or fatigue [12:2][14:1].
¶ Transporter Expression (MCT-1 and MCT-4)
Skeletal muscle biopsy studies demonstrate that threshold interval training acts as a powerful stimulus for upping the expression of both MCT-1 and MCT-4 transport proteins [2:12]. This direct cellular adaptation optimizes the "lactate shuttle" mechanism, ensuring that lactate produced in highly active glycolytic fibers is rapidly transported to, and oxidized by, neighboring oxidative fibers or cardiac cells [5:8][8:6].
¶ Cardiorespiratory and Autonomic Durability
Because lactate is a primary signaling molecule that stimulates both mitochondrial biogenesis and the release of brain-derived neurotrophic factor (BDNF) [5:9], threshold training supports cognitive preservation and vascular health. Sustaining steady-state workouts near LT2 enhances arterial compliance, lowers resting heart rate, and improves heart rate recovery (HRR), directly correlating with a lower risk of major adverse cardiovascular events (MACE) [1:3][15].
¶ Who Benefits Most / Least
¶ Who Benefits Most
- Aged and Middle-Aged Adults: As we age, we selectively lose Type II muscle fibers, which can compromise glycolytic capacity and elevate blood lactate during functional tasks [7:1][16]. Threshold training preserves motor unit recruitment and optimizes the clearance of lactate, keeping daily tasks (such as walking uphill or climbing stairs) fully within the comfortable "aerobic" domain.
- Endurance and Hybrid Athletes: Athletes seeking to sustain higher paces, delay the "burn" of muscular acidosis, and accelerate recovery times during and after high-intensity training [2:13][8:7].
- Metabolically Compromised Individuals: Patients with insulin resistance or type 2 diabetes benefit from the massive clearance of circulating glucose and lactate driven by high-volume recruitment of large muscle groups [4:10][13:3][17].
¶ Who Benefits Least
- Sedentary Beginners (Initial Weeks): Individuals who are completely detrained do not have the mitochondrial base or capillary network to support high-intensity threshold efforts. They should spend 4 to 8 weeks developing a baseline via Zone 2 training before introducing LT2 intervals [10:2][11:3].
- Individuals with Sympathetic Overtraining: Those suffering from autonomic burnout or elevated resting cortisol should avoid high-sympathetic threshold efforts, focusing instead on restorative low-intensity exercise [17:1].
¶ Prerequisites & Contexts of Failure
Adapting to lactate threshold training requires:
- A Robust Zone 2 Aerobic Base: Without a strong capillary grid and sufficient Type I fibers, lactate produced during intervals cannot be imported or oxidized, leading to rapid fatigue and training failure [11:4].
- Glycogen Availability: Threshold efforts rely heavily on glycolysis; executing these workouts in a chronic, carbohydrate-depleted state severely limits power output and blunts adaptation.
- Orthopedic Integrity: The higher speeds and forces of threshold training demand stable joint mechanics to avoid injury.
¶ How to Try It (Actionable Protocols)
Before starting threshold training, establish your individual LT2 training zone. This can be estimated via a 30-minute field test (the average heart rate of the last 20 minutes of an all-out 30-minute time trial represents your Lactate Threshold Heart Rate, or LTHR) or determined precisely through a clinical lactate step test using a portable meter [2:14][12:3].
¶ Starter Protocol: The "Sweet Spot" Tempo
- Goal: Safely introduce continuous, sub-threshold mechanical and metabolic stress.
- Frequency: 1 session per week.
- Warm-up: 10 minutes of low-intensity Zone 1–2 work.
- Work Phase: 20 minutes of continuous, steady work at 80–85% of LTHR (RPE 6-7/10; feels "comfortably hard"—you can talk in brief, 3-to-4 word phrases but cannot hold a full conversation).
- Cool-down: 5–10 minutes of easy walking or cycling.
¶ Standard Protocol: The "LT2 Threshold Intervals"
- Goal: Maximize metabolic clearance adaptations and MCT-1/MCT-4 expression.
- Frequency: 1 to 2 sessions per week, with at least 72 hours of recovery between sessions.
- Warm-up: 10–15 minutes of progressive aerobic work.
- Work Phase:
- Perform 3 x 8 minutes or 2 x 12 minutes at 95–100% of LTHR (blood lactate stable at 3.0–4.0 mmol/L, RPE 7-8/10).
- Recovery: 3 minutes of very light active recovery (Zone 1) between intervals to allow partial lactate clearance.
- Cool-down: 10 minutes of easy spinning or jogging.
¶ Advanced Protocol: The "Norwegian Double-Threshold" Model
- Goal: Maximize weekly threshold volume while minimizing systemic autonomic fatigue. This is achieved by dividing threshold work into morning and afternoon sessions, guided by precise blood lactate measurements [2:15].
- Frequency: 1 to 2 "Double Days" per week.
- Morning Session (LT1/Sub-LT2):
- Warm-up: 15 minutes.
- Work: 5 x 6 minutes at 85–90% LTHR (target blood lactate strictly within 2.0–2.5 mmol/L).
- Recovery: 2 minutes light active recovery between intervals.
- Afternoon Session (LT2 Threshold):
- Performed 4–6 hours after the morning session.
- Warm-up: 15 minutes.
- Work: 10 x 3 minutes or 5 x 2,000 meters at 95–102% LTHR (target blood lactate strictly within 3.2–4.2 mmol/L).
- Recovery: 2 minutes light active recovery between intervals.
¶ Integration and Periodization
To ensure proper recovery, always structure threshold sessions within a polarized annual plan. Do not exceed 2 threshold sessions per week unless you are an advanced athlete with a highly developed aerobic base. For structured periodized plans, refer to the Training Blocks & Periodization guide.
¶ Safety, Interactions, Red Flags
¶ Pre-Activity Screening & Clinical Precautions
Because lactate threshold training involves sustained, high-intensity cardiac output, adhere strictly to the general safety guidelines on our Exercise page and monitor the following:
- Sympathetic Overload & Burnout: LT2 training induces a significant sympathetic "fight-or-flight" response. Performing these sessions too frequently can suppress heart rate variability (HRV), disrupt sleep quality, and elevate resting cortisol.
- Drug Interactions (Beta-Blockers): Beta-blockers artificially suppress maximum heart rate. For patients taking these medications, target training zones must be guided strictly by RPE (7–8 for threshold work) and the talk test rather than heart rate zones.
- Metformin: As a mitochondrial Complex I inhibitor, metformin can slightly increase resting and exercise blood lactate levels. This is a normal physiological response; however, clinicians should rely on RPE and functional power output rather than absolute blood lactate numbers when prescribing threshold targets for patients on metformin.
¶ Stop Criteria and Red Flags
Immediately terminate any threshold interval and seek medical evaluation if you experience:
- Chest pain, pressure, radiating discomfort, or tightness.
- Sudden dizziness, visual disturbances, or loss of balance.
- An irregular or fluttering heart rate that does not stabilize with rest.
- Extreme, uncharacteristic muscle weakness or localized numbness.
¶ Tracking & What “Good” Looks Like
Progression in lactate threshold fitness is marked by an increase in power or speed at the same submaximal heart rate or blood lactate level.
¶ Biomarkers and Functional Metrics
- Blood Lactate Step Test: Conducted monthly. Measures blood lactate at incremental power outputs (e.g., every 4 minutes, increasing by 20–30 watts). Progress is shown when the curve shifts to the right, indicating lower lactate levels at identical workloads [4:11].
- Lactate Threshold Heart Rate (LTHR): Heart rate at LT2. Progress is shown when you can maintain a higher power output or faster pace at your LTHR.
- Heart Rate Recovery (HRR): The drop in heart rate in the first minute post-exercise. A drop of > 25 beats per minute reflects highly efficient autonomic control.
- Fasting Glucose & HbA1c: Tracked quarterly to monitor improvements in long-term glycemic control and insulin sensitivity [13:4].
¶ Time-to-Benefit and Washout
- Time-to-Benefit: Upregulation of glycolysis and glycogen storage occurs within 1 to 2 weeks [13:5]. Structural changes, including MCT transporter synthesis, mLDH upregulation, and capillary sprouting, require 6 to 8 weeks of consistent training [2:16][5:10].
- Time-to-Washout: Detraining begins within 10 to 14 days of exercise cessation. MCT-1 and MCT-4 transporter proteins decay rapidly, leading to accumulated blood lactate and premature fatigue after 3 to 4 weeks of sedentary behavior [18][7:2].
¶ Common Mistakes & Myths
- Myth: "Lactate Causes Muscular Soreness": Lactate is rapidly cleared from muscle tissue within 30 to 60 minutes post-exercise. Muscle soreness (DOMS) is caused by micro-tears in muscle fibers and local inflammation, not lactate [5:11].
- Mistake: Executing Threshold Workouts Too Fast: Running or cycling at Zone 5 (VO2 max) intensity instead of staying strictly at LT2. This triggers rapid acid accumulation, preventing you from sustaining the 20–40 minutes of cumulative work needed for threshold adaptations [10:3].
- Myth: "Lactate is a Toxic Waste Product": Lactate is actually a critical fuel source used by the heart, brain, and slow-twitch muscle fibers, and acts as a key signaling hormone that drives mitochondrial biogenesis and tissue repair [5:12][8:8].
- Mistake: Neglecting the Conversational "Talk Test": Chasing heart rate targets on a wearable device on a hot day. Dehydration and heat elevate heart rate (cardiac drift); rely on RPE and the talk test to guide intensity when environmental conditions fluctuate.
¶ Decision Tree (Text-Based)
[1] Has the individual developed a consistent Zone 2 base (min 3 sessions/week for 4-8 weeks)?
├── NO -> Focus strictly on Zone 2 training to build capillary and mitochondrial density.
└── YES -> Go to [2]
[2] Select your threshold training protocol:
├── TIME-CONSTRAINED / BEGINNER -> Implement "Sweet Spot Tempo" (1 session/week, 20 mins continuous)
└── ADVANCED ATHLETE -> Go to [3]
[3] Do you have access to a portable blood lactate meter?
├── NO -> Use Heart Rate and RPE targets (RPE 7-8, LTHR pace) -> Monitor HRR weekly
└── YES -> Implement "LT2 Threshold Intervals" (target stable lactate at 3.0-4.0 mmol/L) or "Norwegian Double-Threshold"
¶ FAQs (People Also Ask targets)
¶ What is the difference between LT1 and LT2?
LT1 (Aerobic Threshold) is the point where blood lactate first begins to rise above resting levels, marking the top of Zone 2 [4:12]. LT2 (Anaerobic Threshold) is the upper limit of metabolic stability, beyond which lactate and acid accumulate exponentially, leading to rapid muscle fatigue [4:13][5:13].
¶ How do I find my lactate threshold heart rate without a laboratory test?
The most accurate field test is a 30-minute all-out time trial (running or cycling). Your average heart rate during the final 20 minutes of this test provides a highly reliable estimate of your Lactate Threshold Heart Rate (LTHR) [2:17][12:4].
¶ Why is lactate threshold training important for longevity?
By improving your lactate clearance capacity, threshold training lowers metabolic stress and systemic fatigue during everyday activities [4:14][3:3]. This enhances cardiovascular compliance, preserves functional independence as we age, and directly supports long-term metabolic flexibility [1:4][7:3].
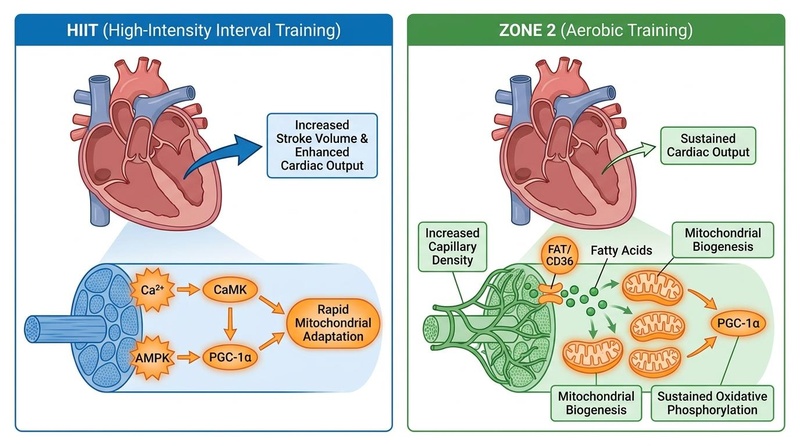
¶ Is lactate threshold training better than HIIT?
They are complementary. HIIT (Zone 5) focuses on short, maximal efforts to expand cardiac stroke volume and absolute VO2 max [14:2], while Lactate Threshold training (Zone 4) focuses on sustaining a high percentage of that VO2 max for longer periods by upregulating cellular lactate clearance [2:18][12:5].
¶ Can I do lactate threshold training if I take metformin?
Yes, but be aware that metformin slightly increases blood lactate levels by inhibiting Complex I of the mitochondrial electron transport chain. When training, rely primarily on RPE and functional power output rather than absolute blood lactate measurements to guide your intensity targets.
¶ Glossary
- Lactate Shuttle: The physiological process where lactate produced in active glycolytic muscle fibers is transported to and oxidized by aerobic tissues (such as slow-twitch fibers and heart muscle) [5:14][8:9].
- Maximal Lactate Steady State (MLSS): The highest constant workload that can be maintained where blood lactate concentration remains stable over time (synonymous with LT2).
- mLDH (Mitochondrial Lactate Dehydrogenase): The enzyme located inside mitochondria that converts lactate back into pyruvate to fuel the Krebs cycle.
- MCT-1 (Monocarboxylate Transporter 1): The transport protein responsible for importing lactate into oxidative muscle fibers and mitochondria for energy production.
- MCT-4 (Monocarboxylate Transporter 4): The transport protein responsible for exporting lactate and hydrogen ions out of glycolytic muscle cells.
- Metabolic Clearance Rate: The rate at which the body removes lactate or other metabolites from the bloodstream.
¶ Methods (Transparency)
¶ Search Strategy
A structured literature search was conducted across PubMed, the Cochrane Library, and Google Scholar up to July 2026. Search queries included "lactate threshold training physiology," "MCT-1 MCT-4 exercise adaptation," "lactate shuttle mechanism," "Maximal Lactate Steady State longevity," "Norwegian double threshold model," and "lactate guided training distance runners."
¶ Inclusion/Exclusion Rules
- Inclusion: Peer-reviewed systematic reviews, meta-analyses, and randomized trials focusing on human sports science, muscle biopsy adaptations, and cardiometabolic health; studies with clear, reproducible training protocols.
- Exclusion: Animal-only research without human validation; abstract-only publications; marketing or promotional exercise claims.
¶ Evidence Grading Rubric
- High: Supported by multiple randomized controlled trials (RCTs) or robust meta-analyses with consistent, statistically significant outcomes and high methodological quality.
- Moderate: Supported by 1-2 well-designed RCTs, prospective cohort studies, or systematic reviews with some limitations.
- Low: Based on small pilot trials, observational data, or animal-based mechanistic studies requiring further human validation.
¶ References (Full URLs)
¶ Update Log
- 2026-07-07: Initial release of the comprehensive clinical and practical guide on Lactate Threshold training.
Cozma D, Gaita D, Crisan S, et al. The Oxygen Imperative: Cardiorespiratory Fitness, Dose-Dependent Exercise Thresholds, and Longevity-A Narrative Review. Journal of Clinical Medicine. 2026;15(11):e42355766. https://pubmed.ncbi.nlm.nih.gov/42355766/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Casado A, Foster C, Bakken M, et al. Does Lactate-Guided Threshold Interval Training within a High-Volume Low-Intensity Approach Represent the "Next Step" in the Evolution of Distance Running Training? International Journal of Environmental Research and Public Health. 2023;20(5):3782. https://pubmed.ncbi.nlm.nih.gov/36900796/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Miras-Moreno S, Torres-Martos Á, Ruiz JR, et al. Metabolomic and Proteomic Signatures of Cardiorespiratory Fitness for Predicting All-Cause Mortality and Non-Communicable Disease Risk: A Prospective Study in the UK Biobank. Circulation. Genomic and Precision Medicine. 2026;19(3):e42394615. https://pubmed.ncbi.nlm.nih.gov/42394615/ ↩︎ ↩︎ ↩︎ ↩︎
San-Millán I, & Brooks GA. Assessment of Metabolic Flexibility by Means of Measuring Blood Lactate, Fat, and Carbohydrate Oxidation Responses to Exercise in Professional Endurance Athletes and Less-Fit Individuals. Sports Medicine. 2018;48(2):467-479. https://pubmed.ncbi.nlm.nih.gov/28623613/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Mandadzhiev N. The contemporary role of lactate in exercise physiology and exercise prescription - a review of the literature. Folia Medica. 2025;67(1):12-18. https://pubmed.ncbi.nlm.nih.gov/40270161/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
O'Keefe JH, O'Keefe EL, Eckert R, et al. Training Strategies to Optimize Cardiovascular Durability and Life Expectancy. Missouri Medicine. 2023;120(2):125-132. https://pubmed.ncbi.nlm.nih.gov/37091937/ ↩︎
Madden AM, Soepnel LM, Africa C, et al. Aerobic physical activity, cardiorespiratory fitness, and non-communicable diseases risk in older adults: a systematic review. BMC Geriatrics. 2026;26(1):310. https://pubmed.ncbi.nlm.nih.gov/42062906/ ↩︎ ↩︎ ↩︎ ↩︎
Emhoff CW, Messonnier LA. Concepts of Lactate Metabolic Clearance Rate and Lactate Clamp for Metabolic Inquiry: A Mini-Review. Nutrients. 2023;15(14):3136. https://pubmed.ncbi.nlm.nih.gov/37513631/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Ye S, Ding Y, Hu B, et al. Advances in exercise snacks for interrupting sedentary behavior and promoting physical activity: a narrative review. Frontiers in Public Health. 2026;14:e42100526. https://pubmed.ncbi.nlm.nih.gov/42100526/ ↩︎
Williams MA, Feigenbaum MS, Jerôme GJ, et al. Resistance Exercise Training in Individuals With and Without Cardiovascular Disease: 2023 Update: A Scientific Statement From the American Heart Association. Circulation. 2023;148(24):1962-1985. https://www.ahajournals.org/doi/10.1161/CIR.0000000000001189 ↩︎ ↩︎ ↩︎ ↩︎
Storoschuk KL, Moran-MacDonald A, Gibala MJ, Gurd BJ. Much Ado About Zone 2: A Narrative Review Assessing the Efficacy of Zone 2 Training for Improving Mitochondrial Capacity and Cardiorespiratory Fitness in the General Population. Sports Medicine. 2025;55(7):501-514. https://pubmed.ncbi.nlm.nih.gov/40560504/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Nuuttila OP, Matomäki P, Raitanen J, et al. Effects of Low-Intensity Endurance Training on Aerobic Fitness and Risk Factors of Cardiometabolic Health in Working-Age Adults: A Systematic Review and Meta-Analysis. Scandinavian Journal of Medicine & Science in Sports. 2026;36(1):e41543030. https://pubmed.ncbi.nlm.nih.gov/41543030/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
San-Millán I, Brooks GA. Assessment of Metabolic Flexibility by Means of Measuring Blood Lactate, Fat, and Carbohydrate Oxidation Responses to Exercise in Professional Endurance Athletes and Less-Fit Individuals. Sports Medicine. 2018;48(2):467-479. https://pubmed.ncbi.nlm.nih.gov/28623613/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Helgerud J, Høydal K, Wang E, et al. Aerobic high-intensity intervals improve VO2max more than moderate training. Medicine and Science in Sports and Exercise. 2007;39(4):665-671. https://pubmed.ncbi.nlm.nih.gov/17414804/ ↩︎ ↩︎ ↩︎
Laukkanen JA, Immonen J, Isiozor NM, et al. Combined Impact of Cardiorespiratory Fitness and Exercise Systolic Blood Pressure on Cardiovascular and All-Cause Mortality: A Long-Term Follow-Up Study. The American Journal of Cardiology. 2026;195:45-52. https://pubmed.ncbi.nlm.nih.gov/42067048/ ↩︎
Chen Z, Collings PJ, Wang M, et al. Physical Fitness, Biological Aging, and Healthy Longevity. Journal of the American Medical Directors Association. 2025;26(10):e40789340. https://pubmed.ncbi.nlm.nih.gov/40789340/ ↩︎
Strauss JA, Kirwan R, Ranasinghe C, et al. High-intensity interval training for reducing cardiometabolic syndrome in healthy but sedentary populations. Cochrane Database of Systematic Reviews. 2026;3:CD015412. https://pubmed.ncbi.nlm.nih.gov/41810896/ ↩︎ ↩︎
Barbieri A, Fuk A, Gallo G, et al. Cardiorespiratory and metabolic consequences of detraining in endurance athletes. Frontiers in Physiology. 2023;14:1134385. https://pubmed.ncbi.nlm.nih.gov/38344385/ ↩︎