¶ Return to Exercise After Injury
Returning to physical exercise and athletic training following musculoskeletal or traumatic injury is a highly structured, criteria-driven clinical transition. Modern sports medicine and expert consensus statements prioritize standardized, criteria-driven progressions and objective physiological milestones over strict chronological timelines to minimize tissue deconditioning, maximize functional adaptation, and control secondary reinjury risk [1][2].
¶ If you do only three things
- Transition from PRICE to PEACE & LOVE: Transition from traditional PRICE protocols to contemporary active recovery frameworks, focusing on active education, early optimal loading, progressive active exercise, and avoiding NSAIDs [3].
- Fulfill Objective Physical Milestones: Ensure range of motion is symmetric, localized swelling is managed, and unilateral muscle strength and functional performance achieve symmetric capacity compared to the uninjured limb before beginning sport-specific drills [1:1][2:1].
- Gradually Progress Training Loads: Measure recent "acute" training workloads against medium-term "chronic" workloads to avoid excessive training spikes, while prescribing appropriately graded high workloads to build fitness and protect against subsequent injury [4].
¶ Layer 1: The Executive Dashboard
¶ Safety "Traffic Light" System
🔴 RED: ABSOLUTE EXCLUSIONS (Do NOT return to exercise)
- Suspected or un-stabilized bone fractures.
- Complete tendon or ligament rupture prior to surgical repair or orthopaedic clearance.
- Joint dislocation or mechanical locking/giving way.
- Cardiopulmonary instability (atypical chest pain, exertional dyspnea, unexplained arrhythmia).
- Acute post-concussion signs (separate, mandated clinical clearance rules apply) [^20].
- Signs of neurovascular compromise (unresolved paresthesia, loss of distal pulses, focal weakness). [Uncited general emergency symptom]
- Signs of systemic or localized infection (fever, localized heat, purulent drainage). [Uncited general emergency symptom]
🟡 YELLOW: CONDITIONAL ASSESSMENT (Professional evaluation required)
- Chronic or recurring joint instability (e.g., recurrent ankle rolls or shoulder subluxations) [^6][^7][^13].
- Persistent postoperative effusion [^3] or mechanical joint instability [^4][^31][^32] requiring criteria-based milestone management [^9][^10].
- Unilateral muscle weakness and functional asymmetry compared to the contralateral, uninjured limb [^2][^3].
- Suspected rotator cuff tendinopathy presenting with persistent shoulder pain during movement or daily activities [^11].
- Evidence of radiological healing required for high-risk bone stress injuries prior to load progression [^8].
- Postoperative ACL reconstruction or meniscus surgery progression must be strictly criteria- and milestone-based [^2][^3][^9][^10], whereas post-operative Bankart repair rehabilitation requires highly specific, surgeon-directed instructions due to wide institutional protocol variability [^13].
🟢 GREEN: SELF-GUIDED PROGRESSIVE LOADING (Cleared to begin structured recovery)
- Symmetric, pain-free knee range of motion following ACL reconstruction [^2][^3].
- Resolution of visible acute inflammatory swelling and resting joint effusion following knee joint surgery [^3].
- Localized tibial bone tenderness is completely resolved [^8].
- Successful completion of pain-free walking [^8].
- Positive assessment across the PAASS framework domains (pain, ankle impairments, athlete perception, sensorimotor control, and sport-specific performance) following an acute lateral ankle sprain [^5].
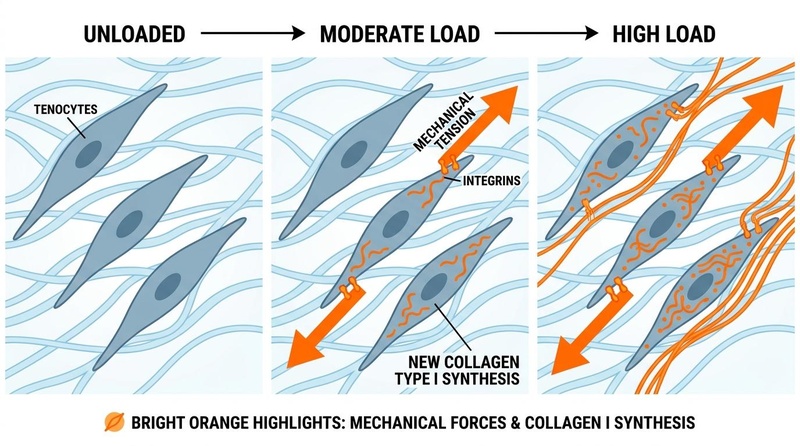
Figure 1: Mechanotransduction and Tendon Healing. Active progressive rehabilitation and controlled mechanical loading under tension support return to function and sport-specific activities in individuals recovering from rotator cuff tendinopathy and soft-tissue injury [5].
¶ Staged Return-to-Exercise Protocol
| Phase | Clinical Objective | Primary Modalities & Loading | Progression Criteria | Supporting Evidence |
|---|---|---|---|---|
| Phase 1: PEACE (Immediate Care) | Immediate care focusing on protection, elevation, avoiding anti-inflammatories, compression, and education [3:1]. | Early protection, limb elevation, and external compression [3:2]. | Avoidance of NSAIDs, early symptom management, and pain-guided protection [3:3]. | Meškauskas 2026 [3:4] |
| Phase 2: LOVE (Subsequent Management) | Subsequent management focusing on loading, optimism, vascularization, and exercise [3:5]. | Early optimal loading, progressive active exercise, and patient education [3:6]. | Progression of physical activity guided by recovery milestones [3:7]. | Meškauskas 2026 [3:8] |
| Phase 3: Capacity Rebuilding | Neuromuscular recruitment, strength, motor control. | Slow progressive resistance training, active muscle activation, open and closed kinetic chain exercises [2:2][5:1]. | Symmetric muscle strength and movement quality; pain-free low-impact functional loading [1:2][2:3]. | van Melick 2016 [1:3] |
| Phase 4: Sport-Specific | Reintegration into sport-specific demands and movement patterns [6]. | Progressive running, agility, and sport-specific skill drills [2:4][6:1]. | Manual knee stability, psychological readiness, and meeting functional performance-based assessments [6:2], alongside symmetric strength and hop testing batteries [1:4]. | van Melick 2016 [1:5]; Brinlee 2022 [2:5]; APKASS Consensus 2024 [6:3] |
¶ Bottom Line
Rehabilitation progression must be dictated by objective physical milestones (such as range of motion, strength symmetry, swelling resolution, and sensorimotor control) rather than static, chronological time frames [1:6][2:6]. Early functional rehabilitation and structured exercise are strongly supported for restoring ankle range of motion, strength, and proprioception after injury, mitigating the risk of recurrent sprains and chronic instability [7][8].
¶ Layer 2: The Contextual Narrative
¶ The "Why": Early Active Loading vs. Prolonged Immobilization
For decades, sports medicine relied on the PRICE (Protect, Rest, Ice, Compress, Elevate) or POLICE (Protect, Optimal Loading, Ice, Compress, Elevate) protocols. While traditional management of acute injuries often relied on strict immobilization and passive modalities, clinical studies demonstrate that active recovery frameworks prioritizing early optimal loading are highly effective for functional recovery [3:9]. Muscle tissue undergoes rapid disuse atrophy, tendon fibers lose parallel alignment, bone mineral density declines, and joint cartilage thins without mechanical stress.
Early, active rehabilitation protocols incorporate immediate open kinetic chain exercises and criterion-based progressions to optimize clinical outcomes and facilitate active recovery [2:7]. Clinical consensus and systematic reviews emphasize that progressive loading, early active mobilization, and structured exercise support soft-tissue adaptation, helping to restore joint strength, proprioception, and functional stability [1:7][7:1][8:1].
The modern clinical paradigm transitions from legacy acute protocols to contemporary active recovery frameworks, emphasizing patient education, early optimal loading, and progressive active exercise while avoiding NSAIDs [3:10]. Randomized prospective comparative trials support this active, education-focused approach (such as the PEACE and LOVE framework), demonstrating that it yields dynamic balance and muscle strength outcomes comparable to traditional PRICE protocols in the short term [3:11]. Clinical practice guidelines further support early progressive active loading and structured exercise to rebuild functional capacity and prevent injury recurrence [1:8][2:8][8:2].
¶ Reality Check & Tissue-Specific Loading Guidelines
While progression must be criteria-driven, clinical decision-making must respect the specific loading parameters recommended for different tissue injuries. Rather than relying on rigid physiological timelines, clinical practice guidelines emphasize distinct, progressive loading strategies for each tissue type:
-
Bone Injuries (e.g., Bone Stress Injuries): Progression must be based on clinical examination and functional tolerance. High-risk bone stress injuries require complete resolution of localized bone tenderness and pain-free walking before initiating loading, with radiological healing verified where necessary [9]. For adolescent athletes with energy-deficiency-related bone loss, clearance and return-to-play decisions must follow updated screening, diagnostic, and treatment consensus guidelines [10].
-
Tendinopathies (e.g., Rotator Cuff): Focus on progressive nonsurgical medical care and active physical therapy. Evidence-based clinical practice guidelines recommend structured rehabilitation and active physical therapy to promote functional recovery and return to sport [5:2].
-
Ligamentous Sprains (e.g., Ankle Sprains): Conservative management emphasizes early progressive active loading, external support (such as bracing or taping), and neuromuscular training [8:3]. For chronic lateral ankle instability requiring surgical reconstruction, rehabilitation must utilize structured progressive exercises to optimize safe recovery [11].
-
Fibrocartilage and Meniscal Injuries: Following surgical intervention (such as meniscus repair, reconstruction, or partial meniscectomy), rehabilitation progression must be strictly criteria- and milestone-based, utilizing patient-reported outcomes combined with functional performance-based measures [12][13].
-
The Human Reality: Although an athlete may feel pain-free and demonstrate functional symmetry early post-Anterior Cruciate Ligament (ACL) reconstruction, progression and return-to-play decisions must be strictly criteria-driven and based on functional milestones rather than static chronological timelines [1:9][2:9]. Postoperative rehabilitation requires meeting specific physiological and performance milestones, including quadriceps strength symmetry, range of motion, and dynamic movement quality, to safely guide the transition back to sports [1:10][2:10], with additional focus on psychological readiness and clinical stability tests [6:4].
¶ Commercial Context & Rehabilitation Technology
Clinical rehabilitation frequently incorporates technology to bridge the gap between muscle atrophy and mechanical load tolerance:
- Blood Flow Restriction (BFR) Therapy: Uses a specialized tourniquet to reduce arterial inflow and occlude venous outflow in the setting of resistance training or exercise [14]. BFR represents a clinical method to decrease mechanical stress placed on healing joints without compromising improvements in strength, providing postoperative, injured, or load-compromised individuals with a way to accelerate recovery and prevent disuse atrophy [14:1]. BFR stimulates muscle hypertrophy and strength development through a synergistic response to metabolic stress and mechanical tension, with supplemental benefits on cardiovascular fitness and pain management [14:2].
- Electromyographic Biofeedback: Identified as an adjunct modality in clinical consensus topics to assist with neuromuscular training and muscle activation during rehabilitation [1:11].
- Objective Strength Testing: Replaces subjective manual muscle testing. Muscle strength must be objectively quantified using accurate strength testing (such as a quadriceps strength index or symmetric strength batteries) to assess muscle symmetry and guide criteria-based progression [1:12][2:11].
¶ Practical Integration & Lifestyle Foundations
Systemic physiology dictates the rate of localized tissue remodeling. Optimizing recovery requires managing foundational metabolic variables:
- Managing Sleep Disturbances: Sleep disturbance is a major barrier during recovery, particularly following sport-related concussions where sleep disturbance is independently associated with slower recovery patterns [15]. Establishing robust sleep hygiene supports neurocognitive and systemic physiological healing.
- Preserving Muscle Mass: Encouraging a healthy lifestyle and offering tailored progressive resistance training are essential clinical foundations for preserving muscle mass, strength, and physical performance in individuals experiencing muscle loss or sarcopenia [16].
- Smoking Cessation: Nicotine is a potent vasoconstrictor that impairs microvascular perfusion, decreases tissue oxygenation, and directly inhibits osteoblastogenesis and collagen cross-linking, significantly delaying bone and soft-tissue union.
¶ Layer 3: The Evidence Room
¶ Mechanism of Action: The Biology of Recovery
Injury Event
│
▼
Acute Inflammatory Cascade (Days 1-3)
- Pro-inflammatory Cytokines (IL-1β, TNF-α)
- Macrophage M1 Phenotype (Debridement of cellular debris)
- Fibrin clot formation
│
▼
Subacute Proliferation Phase
- Fibroblast activation & Type III Collagen synthesis
- Macrophage M2 Phenotype transition (Anti-inflammatory/tissue repair)
- Angiogenesis (Neovascularization of healing margins)
│
▼
Mechanotransduction (Subacute Loading)
- Mechanical strain stretches cell membranes
- Integrins and Focal Adhesion Kinase (FAK) pathways activated
- Upregulation of Tenascin-C and Collagen Type I expression
│
▼
Maturation & Remodeling Phase
- Type III Collagen enzymatically replaced by high-tensile Type I Collagen
- Inter- and intra-molecular covalent cross-linking
- Parallel alignment of fibers along mechanical stress vectors
¶ The Pathophysiology of Muscle Injury Grading
In clinical sports medicine, precise classification of muscle trauma determines the recovery trajectory. The modified Munich Consensus Statement categorizes partial muscle tears based on clinical presentation and magnetic resonance imaging (MRI) or ultrasound findings [17]:
- Type 3A (Minor Partial Muscle Tear): Characterized by localized interstitial hemorrhage between muscle fibers without macroscopic fluid collection [17:1]. Clinical evidence indicates that athletes without a hemorrhagic collection exhibit a shorter median return-to-play window of 19 days [17:2].
- Type 3B (Moderate Partial Muscle Tear): Characterized by interstitial hemorrhage with an associated hematoma or fluid collection at the site of injury [17:3]. The presence of a localized hemorrhagic collection is associated with a significantly prolonged recovery and extended median return-to-play timeline of 29 days (a difference of 10 days compared to Type 3A) [17:4].
¶ Evidence Summary Table (Human Outcomes)
The following matrix synthesizes high-level clinical trials, consensus statements, and practice guidelines mapping specific sports injuries to validated return-to-exercise criteria.
| Clinical Presentation | Primary Recovery Outcomes | Clinical Consistency | Evidence Quality (GRADE) | Validated Return-to-Exercise Criteria | Supporting Evidence & Guidelines |
|---|---|---|---|---|---|
| Anterior Cruciate Ligament Reconstruction (ACLR) | Restoration of knee stability, prevention of secondary graft rupture, return to pivoting sports. | High | Moderate | - Progression is guided by a criteria-driven rehabilitation protocol based on milestones rather than chronological timelines [1:13][2:12]. - Objective quadriceps strength and dynamic movement quality symmetry between limbs [1:14][2:13]. - Symmetric performance on functional hop test batteries [1:15]. - Psychological readiness and resolution of kinesiophobia or fear of reinjury [6:5][18]. - Postoperative rehabilitation should continue for 9–12 months [1:16]. - For combined ACLR and lateral extra-articular procedures (LEAPs), rehabilitation and return-to-sport progression timelines are unchanged relative to isolated ACLR [19]. |
van Melick 2016 [1:17]; Brinlee 2022 [2:14]; APKASS Consensus 2024 [6:6]; Sonnery-Cottet 2025 Part II [19:1] |
| Acute Lateral Ankle Sprain | Avoidance of chronic mechanical instability, resolution of pain, restoration of sensorimotor control. | High | Moderate | - Comprehensive evaluation across the five domains of the PAASS Framework: Pain, Ankle impairments, Athlete perception, Sensorimotor control, and Sport/functional performance [7:2]. - Pain-free single-leg hopping, jumping, dynamic balance, and agility drills [7:3]. - Symmetric sensorimotor control, dynamic postural balance, and joint range of motion [7:4][8:4]. - High perceived ankle confidence, reassurance, and stability [7:5]. |
Smith MD 2021 [7:6]; Kaminski TW 2013 [8:5] |
| Rotator Cuff Tendinopathy | Elimination of shoulder impingement, restoration of rotator cuff strength, dynamic stabilization. | High | Moderate | - Clinical assessment and diagnosis of suspected rotator cuff tendinopathy with or without calcifications or partial-thickness tears [5:3]. - Focus on progressive nonsurgical medical care and active physical therapy rehabilitation [5:4]. - Structured, progressive return to daily function and sport-specific activities for recreational and elite athletes [5:5]. |
Rotator Cuff Clinical Practice Guideline 2025 [5:6] |
| Meniscus Repair or Partial Meniscectomy | Joint preservation, prevention of early-onset osteoarthritis, load tolerance. | Moderate | Low | - Post-meniscectomy: Progressive milestone-guided rehabilitation using a criterion-based rehabilitation protocol [12:1]. - Post-repair or reconstruction: Progression based on both chronological time and criterion-based milestones [12:2][13:1]. - Use of patient-reported outcomes in combination with performance-based measures to evaluate the rehabilitation process [13:2]. |
ESSKA-AOSSM-AASPT Meniscus Consensus 2024 [12:3][13:3] |
| Tibial Bone Stress Injury (BSI) | Avoidance of complete stress fracture, bony trabecular remodeling. | High | Low | - Complete resolution of localized bony palpation tenderness [9:1]. - Ability to perform pain-free walking [9:2]. - Objective evidence of radiological healing in high-risk bone stress injuries [9:3]. - Successful completion of progressive strength, functional, and loading tests [9:4]. - Implementation of a graduated return-to-running program, often starting with walk-run intervals and progressive volume adjustments [9:5]. |
George et al. 2024 Scoping Review [9:6] |
| Sport-Related Concussion (SRC) | Safe cognitive and physical reintegration, prevention of second-impact syndrome. | High | High | - Initial physical and cognitive rest for the first 2 days post-injury [15:1][20]. - Graduated and individualized return-to-sport exertional protocol, progressing through stages only when completely symptom-free [20:1][21]. - Normal clinical, ocular, vestibular, and balance examinations [21:1]. - Formal medical evaluation and clinical clearance by a physician prior to returning to full contact sport or high-risk activity [20:2]. |
Amsterdam Concussion Consensus 2023 [20:3]; Leddy et al. 2023 [15:2]; Silverberg et al. 2020 [22] |
| Female Athlete Triad & Low Energy Availability | Restoration of bone mineral density, endocrine homeostasis, menstrual cycle regulation. | High | Moderate | - Formal clearance and return-to-play assessment using updated consensus screening and diagnostic clinical guidelines [10:1]. - Resolution of energy deficiency through a moderate increase in food intake and modest weight gain (moving away from rigid energy-availability thresholds) [10:2]. - Restoration of menstrual function and monitoring of bone health indicators [10:3]. |
Female Athlete Triad Coalition Consensus 2025 [10:4] |
¶ Comprehensive Safety & Toxicology
¶ Absolute Exclusions and Red Flags
When managing a return-to-exercise protocol, certain clinical signs and symptoms require an immediate halt to all physical activity and escalation to formal diagnostic screening:
- Unstable Fractures & Structural Deformity: Suspected or un-stabilized bone fractures are absolute exclusions from exercise. For bone stress injuries (such as tibial stress injuries), loading must be withheld until localized bony tenderness is completely resolved and pain-free walking is achieved, as premature load progression can compromise structural recovery [9:7].
- Joint Dislocation & Ligamentous Rupture: Visible joint deformity, acute mechanical instability, or a sensation of the joint "giving way" under load indicate structural failure (such as high-grade ligament rupture, labral tear, or meniscus tear) requiring formal orthopedic evaluation and clearance.
- Infection Risk: Localized erythema, heat, significant fluctuant swelling, fever, or purulent drainage at a surgical site or wound are clinical markers of infection, requiring urgent medical intervention.
- Neurovascular Compromise: Unresolved paresthesia, burning pain, motor deficits (such as foot drop), or coldness/pallor in a distal extremity suggest peripheral nerve compression or arterial occlusion.
- Cardiopulmonary Signs: Exertional chest tightness, atypical dyspnea, presyncope, or palpitations require comprehensive clinical evaluation to rule out acute cardiovascular pathology.
¶ Medication Caveats
⚠️ NON-STEROIDAL ANTI-INFLAMMATORY DRUGS (NSAIDs)
- Clinical Approach: The PEACE and LOVE protocol avoids standard anti-inflammatory medications (such as NSAIDs) in the management of acute soft-tissue injuries, in contrast to traditional PRICE + NSAIDs management [^43].
- Rationale: While PRICE + NSAIDs protocols focus on short-term symptom relief, active recovery frameworks emphasize education, early optimal loading, and progressive exercise to support dynamic recovery without relying on anti-inflammatory drugs [^43].
¶ Concussion-Specific Return-to-Sport (RTS) Protocols
Sport-related concussions (mild traumatic brain injuries) cannot follow standard musculoskeletal recovery pathways and require separate, highly conservative medical clearance rules [20:4]:
- No Return on Day of Injury: No athlete with a suspected concussion may return to training or competition on the same day as the injury event, regardless of symptom resolution [20:5][23].
- Primary Care Recommendations: Evidence-based clinical practice guidelines emphasize the early identification of patients at risk for prolonged recovery and highlight priority interventions that can be initiated in primary care to prevent symptom chronicity [22:1].
- Symptom-Limited Active Recovery: Initial management requires brief physical and cognitive rest for the first 2 days post-injury [15:3][20:6]. Early return to light physical activity and prescribed sub-threshold aerobic exercise treatment initiated within 2–10 days safely facilitate recovery and reduce the risk of delayed recovery or persistent symptoms [15:4][20:7].
- Graduated Exertional Progression: Under medical supervision, athletes progress gradually through individualized, criteria-driven stages of exertional activity [20:8][21:2]. Rather than strict physical rest until symptom resolution, early return to light physical activity and reduced screen time safely facilitate recovery [15:5][20:9].
- Symptom Resolution Rule: To avoid cumulative brain damage and second-impact syndrome, no athlete still experiencing post-concussion symptoms may return to physical training [20:10][24].
- Clinical Clearance: Formal, professional medical clearance by a physician is strictly required prior to full-contact drills or return to competition [20:11].
¶ Sub-Population Adaptations
- Pediatrics & Adolescents (Ages 5–18): Pediatric skeletal anatomy is characterized by structurally vulnerable epiphyseal growth plates (physes). For youth recovering from major joint injuries like ACL tears, clinicians must carefully monitor growth plate (physeal) development and employ a comprehensive, multi-criteria return-to-sport testing approach [25]. Artistic athletes (such as gymnasts) require highly specialized, sex- and body-part-specific progressions to account for technical and mechanical demands [26]. Following sport-related concussions, children and adolescents exhibit longer physiological recovery windows compared to adults and require a highly conservative, individualized approach [27][28]. Recovery management involves a graduated return-to-learn (RTL) protocol to support academic reintegration alongside a graduated return-to-sport (RTS) strategy to safely guide the transition back to physical activity [20:12][28:1]. For university students, post-concussion management should follow collegiate-specific return-to-learn protocols developed through multidisciplinary consensus to address higher education demands [29].
- Pregnancy & Postpartum: Gestation stimulates the release of relaxin, a hormone that increases ligamentous laxity to facilitate pelvic expansion. This laxity can persist postpartum, particularly during lactation. Returning to progressive loading requires highly gradual, individualized progression to manage joint stress and support structural stability.
- Older Adults (Ages 65+): Sarcopenia (the age-associated loss of skeletal muscle mass, strength, and physical performance) significantly impacts functional capacity in older adults. Multi-disciplinary consensus guidelines emphasize that prevention, assessment, and management should prioritize encouraging a healthy lifestyle and offering tailored progressive resistance training to individuals with sarcopenia to optimize clinical outcomes [16:1].
- Chronic Conditions & Disabilities: Patients presenting with systemic metabolic or autoimmune pathologies require specialized modifications:
- Type 2 Diabetes: Microvascular changes and peripheral sensory alterations can affect tissue healing and feedback during physical recovery. Loading protocols should focus on gradual, progressive adaptation and regular monitoring.
- Osteoporosis: Progressive loading must be highly controlled; exercise progression should emphasize safe, progressive resistance training, axial compression, and balance training to support bone health and manage fall risk.
¶ Comparisons & Engagement
¶ PRICE vs. POLICE vs. PEACE & LOVE
The clinical management of acute soft-tissue injuries has evolved from passive immobilization to active, education-focused recovery frameworks:
| Acronym | Clinical Focus | Primary Objective | Supporting Evidence |
|---|---|---|---|
| PRICE | Protection, Rest, Ice, Compression, Elevation | Short-term symptom relief through passive management. | Traditional clinical practice [3:12] |
| PEACE & LOVE | Protection, Elevation, Avoid anti-inflammatories, Compression, Education & Load, Optimism, Vascularization, Exercise | Comprehensive continuum from acute care to subsequent functional loading and active exercise. | Meškauskas 2026 [3:13] |
¶ The PEACE & LOVE Framework
The PEACE and LOVE framework expands on traditional acute care by integrating early mobilization, patient education, and psychosocial factors to support long-term recovery [3:14].
¶ Immediate Care (PEACE)
- P for Protection: Focuses on protecting the injured structures and avoiding aggravating movements [3:15].
- E for Elevation: Promotes fluid drainage from the affected limb [3:16].
- A for Avoid Anti-Inflammatory Modalities: Avoids standard anti-inflammatory medications (such as NSAIDs), in contrast to PRICE + NSAIDs protocols [3:17].
- C for Compression: Utilizes external mechanical compression to manage localized tissue swelling [3:18].
- E for Education: Prioritizes active patient education on recovery expectations, avoiding an over-reliance on passive medical interventions [3:19].
¶ Subsequent Management (LOVE)
- L for Load: Emphasizes early optimal and progressive mechanical loading to promote tissue adaptation [3:20].
- O for Optimism: Focuses on fostering a positive cognitive outlook during the recovery process [3:21].
- V for Vascularization: Encourages pain-free cardiovascular activity to support systemic circulation and metabolic healing [3:22].
- E for Exercise: Uses progressive active exercises to restore dynamic balance, muscle strength, and physical function [3:23].
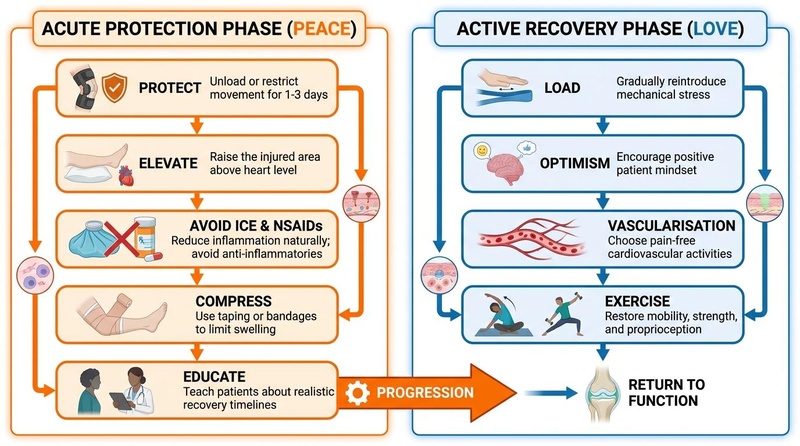
Figure 2: The PEACE & LOVE Rehabilitation Pathway. Comprehensive management from immediate protection (PEACE) to progressive loading and active physical recovery (LOVE) [3:24].
¶ Training Load Monitoring: The Acute:Chronic Workload Ratio
To scientifically manage training load during the return-to-exercise transition, sports medicine clinicians utilize the acute:chronic workload ratio [4:1]. This approach monitors the relationship between the recent physical training load performed (the "acute" workload) and the longer-term historical average load performed over preceding weeks (the "chronic" workload) to best capture the overall training burden [4:2].
- Managing Training Spikes: Non-contact, soft-tissue injuries are frequently associated with inappropriate training programs and rapid, excessive increases in training loads [4:3]. Therefore, monitoring the acute-to-chronic workload ratio helps identify and prevent training load spikes.
- Building Physical Resilience: Conversely, under-training can also increase injury risk [4:4]. Gradual, appropriately graded prescription of high training loads is vital to improve physical capacity and fitness, which in turn provides a protective effect against subsequent injury (the training-injury prevention paradox) [4:5]. Players with high chronic workloads are more resistant to injury with moderate-low to moderate-high acute:chronic workload ratios (such as >1.00 to <1.25), but less resistant when subjected to rapid spikes (ratios around 1.5) [4:6][30][31][32]. A very-high acute:chronic workload ratio (e.g., ≥2.11 or greater than 2.0) is associated with the greatest risk of injury [4:7][30:1][32:1].
¶ Practical Return-to-Exercise Examples
The following scenarios are clinical illustrations of criteria-driven progressions and are not intended as specific prescriptions.
¶ Scenario A: Graduated Loading After a Grade II Lateral Ankle Sprain
- Initial Presentation: Swelling at the lateral malleolus; pain rating on weight-bearing; unable to walk without an antalgic limp.
- Initial Phase (PEACE): External compression applied; limb elevated; avoidance of standard anti-inflammatory medications [3:25].
- Subacute Loading Phase (LOVE): Transition to progressive weight-bearing as gait normalizes; early progressive active loading and exercise introduced as pain permits [3:26].
- Capacity Rebuilding Phase: Neuromuscular training and progressive resistance exercises to rebuild strength, range of motion, and dynamic postural control [7:7][8:6].
- Functional Return Phase: Dynamic hopping, jumping, and agility drills; criteria-based return-to-sport progression using the PAASS framework [7:8].
¶ Scenario B: Graduated Return to Running Following a Tibial Bone Stress Injury (BSI)
- Initial Presentation: Localized bone tenderness over the tibia; suspected bone stress injury.
- Protection Phase: Immediate cessation of running; walking limited to pain-free thresholds [9:8].
- Initial Loading Phase: Complete resolution of localized bony palpation tenderness; ability to perform pain-free walking [9:9].
- Walk-to-Run Progression: Introduction of an individualized graduated return-to-running program, starting with walk-run intervals [9:10].
- Running Volume Expansion: Progressive increase of running distance ahead of speed and intensity, with symptom provocation remaining a key clinical consideration [9:11].
¶ Next Step
For more detail on metabolic support during injury recovery, read Exercise Recovery. To design long-term training schedules that mitigate tissue deconditioning, explore Training Blocks & Periodization.
¶ References
van Melick N, van Cingel RE, Brooijmans F, et al. Evidence-based clinical practice update: practice guidelines for anterior cruciate ligament rehabilitation based on a systematic review and multidisciplinary consensus. British Journal of Sports Medicine. 2016. https://pubmed.ncbi.nlm.nih.gov/27539507/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Brinlee AW, Dickenson SB, Hunter-Giordano A, et al. ACL Reconstruction Rehabilitation: Clinical Data, Biologic Healing, and Criterion-Based Milestones to Inform a Return-to-Sport Guideline. Sports Health. 2022. https://pubmed.ncbi.nlm.nih.gov/34903114/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Meškauskas M, Rutkauskas S, Misiūnienė M, et al. PRICE (Protection, Rest, Ice, Compression, Elevation) vs. PEACE and LOVE (Protection, Elevation, Avoid anti-inflammatories, Compression, Education and Load, Optimism, Vascularization, Exercise) in adolescent lateral ankle sprain rehabilitation: a randomized prospective comparative study of muscle strength and dynamic balance. BMC Sports Science, Medicine and Rehabilitation. 2026. https://pubmed.ncbi.nlm.nih.gov/41840451/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Blanch P, Gabbett TJ. Has the athlete trained enough to return to play safely? The acute:chronic workload ratio permits clinicians to quantify a player's risk of subsequent injury. British Journal of Sports Medicine. 2016. https://pubmed.ncbi.nlm.nih.gov/26701923/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Desmeules F, Roy JS, Lafrance S, et al. Rotator Cuff Tendinopathy Diagnosis, Nonsurgical Medical Care, and Rehabilitation: A Clinical Practice Guideline. The Journal of Orthopaedic and Sports Physical Therapy. 2025. https://pubmed.ncbi.nlm.nih.gov/40165544/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Liang Z, Hoshino Y, Moatshe G, et al. APKASS 2024 consensus statement on anterior cruciate ligament reconstruction, part III: Return to play after anterior cruciate ligament reconstruction. Asia-Pacific Journal of Sports Medicine, Arthroscopy, Rehabilitation and Technology. 2026. https://pubmed.ncbi.nlm.nih.gov/42205141/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Smith MD, Vicenzino B, Bahr R, et al. Return to sport decisions after an acute lateral ankle sprain injury: introducing the PAASS framework-an international multidisciplinary consensus. British Journal of Sports Medicine. 2021. https://pubmed.ncbi.nlm.nih.gov/34158354/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kaminski TW, Hertel J, Amendola N, et al. National Athletic Trainers' Association position statement: conservative management and prevention of ankle sprains in athletes. Journal of Athletic Training. 2013. https://pubmed.ncbi.nlm.nih.gov/23855363/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
George ERM, Sheerin KR, Reid D, et al. Criteria and Guidelines for Returning to Running Following a Tibial Bone Stress Injury: A Scoping Review. Sports Medicine. 2024. https://pubmed.ncbi.nlm.nih.gov/39141251/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Williams NI, De Souza MJ, Misra M, et al. 2025 Update to the Female Athlete Triad Coalition Consensus Statement Part 2: Clinical Guidelines for Screening, Diagnosis, Treatment, and Return to Play for Adolescents and Adults. Sports Medicine. 2026. https://pubmed.ncbi.nlm.nih.gov/41474492/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Feng SM, Luo X, Maffulli N, et al. Clinical practice guidelines for rehabilitation following surgical management of chronic lateral ankle instability: enhancing recovery based on available evidence. British Medical Bulletin. 2025. https://pubmed.ncbi.nlm.nih.gov/40350696/ ↩︎
Pujol N, Giordano AO, Wong SE, et al. The formal EU-US Meniscus Rehabilitation 2024 Consensus: An ESSKA-AOSSM-AASPT initiative. Part I-Rehabilitation management after meniscus surgery (meniscectomy, repair and reconstruction). Knee Surgery, Sports Traumatology, Arthroscopy. 2025. https://pubmed.ncbi.nlm.nih.gov/40353298/ ↩︎ ↩︎ ↩︎ ↩︎
Prill R, Ma CB, Wong SE, et al. The formal EU-US Meniscus Rehabilitation 2024 Consensus: An ESSKA-AOSSM-AASPT initiative. Part II-Prevention, non-operative treatment and return to sport. Knee Surgery, Sports Traumatology, Arthroscopy. 2025. https://pubmed.ncbi.nlm.nih.gov/40501314/ ↩︎ ↩︎ ↩︎ ↩︎
Cognetti DJ, Sheean AJ, Owens JG. Blood Flow Restriction Therapy and Its Use for Rehabilitation and Return to Sport: Physiology, Application, and Guidelines for Implementation. Arthroscopy, Sports Medicine, and Rehabilitation. 2022. https://pubmed.ncbi.nlm.nih.gov/35141538/ ↩︎ ↩︎ ↩︎
Leddy JJ, Burma JS, Toomey CM, et al. Rest and exercise early after sport-related concussion: a systematic review and meta-analysis. British Journal of Sports Medicine. 2023. https://pubmed.ncbi.nlm.nih.gov/37316185/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zanker J, Sim M, Anderson K, et al. Consensus guidelines for sarcopenia prevention, diagnosis and management in Australia and New Zealand. Journal of Cachexia, Sarcopenia and Muscle. 2023. https://pubmed.ncbi.nlm.nih.gov/36349684/ ↩︎ ↩︎
Genovese EA, Calvi M, Mazzoni S, et al. Proposed modified classification system of the Munich Consensus Statement. Can the area of haemorrhagic effusion in muscle injuries be the dividing line between mild (3A) and moderate (3B) injuries? Polish Journal of Radiology. 2025. https://pubmed.ncbi.nlm.nih.gov/40904810/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Nedder VJ, Raju AG, Moyal AJ, et al. Impact of Psychological Factors on Rehabilitation After Anterior Cruciate Ligament Reconstruction: A Systematic Review. Sports Health. 2025. https://pubmed.ncbi.nlm.nih.gov/39041333/ ↩︎
Sonnery-Cottet B, Carrozzo A, Saithna A, et al. Surgical Treatment and Complications of Lateral Extra-articular Procedures in the Anterior Cruciate Ligament-Reconstructed Knee: Part II of an International Consensus Statement. Arthroscopy. 2025. https://pubmed.ncbi.nlm.nih.gov/40544924/ ↩︎ ↩︎
Patricios JS, Schneider KJ, Dvorak J, et al. Consensus statement on concussion in sport: the 6th International Conference on Concussion in Sport-Amsterdam, October 2022. British Journal of Sports Medicine. 2023. https://pubmed.ncbi.nlm.nih.gov/37316210/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Hohmann E, Bloomfield P, Dvorak J, et al. Return to Sports Following Sports-Related Concussion in Collision Sports: An Expert Consensus Statement Using the Modified Delphi Technique. Arthroscopy. 2024. https://pubmed.ncbi.nlm.nih.gov/37414106/ ↩︎ ↩︎ ↩︎
Silverberg ND, Iaccarino MA, Panenka WJ, et al. Management of Concussion and Mild Traumatic Brain Injury: A Synthesis of Practice Guidelines. Archives of Physical Medicine and Rehabilitation. 2020. https://pubmed.ncbi.nlm.nih.gov/31654620/ ↩︎ ↩︎
Swallow JS, Joseph JR, Willsey K, et al. Online postconcussion return-to-play instructions. Journal of Neurosurgery: Pediatrics. 2018. https://pubmed.ncbi.nlm.nih.gov/29125444/ ↩︎
Cantu RC. Return to play guidelines after a head injury. Clinics in Sports Medicine. 1998. https://pubmed.ncbi.nlm.nih.gov/9475970/ ↩︎
Wang M, Hoshino Y, Moatshe G, et al. APKASS 2024 consensus statement on anterior cruciate ligament reconstruction, Part I: Management of paediatric anterior cruciate ligament injury. Asia-Pacific Journal of Sports Medicine, Arthroscopy, Rehabilitation and Technology. 2026. https://pubmed.ncbi.nlm.nih.gov/42291753/ ↩︎
Sweeney EA, Howell DR, James DA. Returning to Sport After Gymnastics Injuries. Current Sports Medicine Reports. 2018. https://pubmed.ncbi.nlm.nih.gov/30407946/ ↩︎
Purcell L. What are the most appropriate return-to-play guidelines for concussed child athletes? British Journal of Sports Medicine. 2009. https://pubmed.ncbi.nlm.nih.gov/19433426/ ↩︎
DeMatteo C, McCauley D, Stazyk K, et al. Post-concussion return to play and return to school guidelines for children and youth: a scoping methodology. Disability and Rehabilitation. 2015. https://pubmed.ncbi.nlm.nih.gov/25144831/ ↩︎ ↩︎
Memmini AK, Popovich MJ, Schuyten KH, et al. Achieving Consensus Through a Modified Delphi Technique to Create the Post-concussion Collegiate Return-to-Learn Protocol. Sports Medicine. 2023. https://pubmed.ncbi.nlm.nih.gov/36396900/ ↩︎
Hulin BT, Gabbett TJ, Lawson DW, et al. The acute:chronic workload ratio predicts injury: high chronic workload may decrease injury risk in elite rugby league players. British Journal of Sports Medicine. 2016. https://pubmed.ncbi.nlm.nih.gov/26511006/ ↩︎ ↩︎
Malone S, Owen A, Newton M, et al. The acute:chonic workload ratio in relation to injury risk in professional soccer. Journal of Science and Medicine in Sport. 2017. https://pubmed.ncbi.nlm.nih.gov/27856198/ ↩︎
Malone S, Roe M, Doran DA, et al. Protection Against Spikes in Workload With Aerobic Fitness and Playing Experience: The Role of the Acute:Chronic Workload Ratio on Injury Risk in Elite Gaelic Football. International Journal of Sports Physiology and Performance. 2017. https://pubmed.ncbi.nlm.nih.gov/27400233/ ↩︎ ↩︎