¶ VO2 Max Training for Longevity: Deep Dive
VO2 max, or maximal oxygen uptake, represents the maximum volume of oxygen your body can utilize per minute during intense, incremental physical exercise [1][2]. As the gold-standard metric of cardiorespiratory fitness (CRF), VO2 max acts as one of the most powerful and clinically validated predictors of all-cause mortality, healthspan, and resistance to multi-system chronic disease across the human lifespan [1:1][3].

| Indication | Cardiorespiratory Fitness, Lifespan Extension, Metabolic Durability, Brain Volume Preservation |
| Access | Behavioral Intervention |
| Dosing Sched | Weekly (1–2 high-intensity sessions integrated with a Zone 2 base) |
| Safety Profile | Moderate (demands high cardiovascular and orthopedic efforts) |
| Key Marker | VO2 Max (mL/kg/min), LTHR, Resting Heart Rate, Heart Rate Recovery |
| Est. Cost | $0 to variable (clinical metabolic cart test: $150–$300) |
¶ TL;DR (5 bullets max)
- Longevity Gold Standard: VO2 max is arguably the single most robust clinical biomarker for predicting long-term survival, with higher cardiorespiratory fitness directly correlating to an extended healthspan and a delayed onset of age-related diseases [1:2][2:1][4].
- Dual Approach: Optimal VO2 max improvements combine foundational, continuous low-intensity (Zone 2) training to expand peripheral capillary and mitochondrial networks with targeted High-Intensity Interval Training (HIIT) to drive central cardiac stroke volume adaptations [5][6].
- No Upper Limit: The longevity and healthspan benefits of improving VO2 max show no clear upper limit; individuals in the "elite" and "extreme" fitness categories continue to experience incremental reductions in mortality risk compared to highly fit peers [1:3][7].
- Decelerates Aging: Advancing cardiorespiratory fitness significantly decelerates biological and epigenetic aging, helping to preserve multi-system function in older adults [8][9].
- Trackable: VO2 max can be measured accurately in a lab via gas exchange analysis or estimated longitudinally with consumer wearables, making it a highly actionable biomarker [10][11].
¶ Quick Answer (Feature Snippet style)
VO2 max represents the maximal rate at which your heart, lungs, and skeletal muscles can coordinate to transport and utilize oxygen during maximal physical exertion [12][2:2]. It is a powerful quantitative predictor of all-cause and cardiovascular mortality, with each 1-MET (3.5 mL/kg/min) increase in VO2 max associated with a 13% to 15% reduction in all-cause mortality risk [13][4:1]. Improving VO2 max requires a polarized training strategy: establishing a broad, high-volume foundation of Zone 2 cardio (60–70% of maximum heart rate) for metabolic flexibility, combined with 1 to 2 weekly sessions of Zone 5 high-intensity intervals (e.g., Norwegian 4x4 method at 90–95% HRmax) to maximize cardiac stroke volume and oxygen extraction efficiency [14][5:1].
¶ What It Is (Plain-English)
VO2 max, or maximal aerobic capacity, can be thought of as the maximum horsepower of your body's cardiorespiratory engine. It represents the upper ceiling of your body's ability to take oxygen from the air, transport it through your lungs and bloodstream, and deliver it to your muscle cells to produce energy [2:3]. Rather than representing a single organ, VO2 max is a systemic measurement that reflects the integrated performance of your pulmonary, cardiovascular, and muscular systems [12:1][15].
The physiology of VO2 max is governed by the Fick Equation:
Where:
- Central Oxygen Delivery (): Peak cardiac output, which is the product of maximum heart rate and left ventricular stroke volume (how much blood the heart can pump per beat) [5:2].
- Peripheral Oxygen Extraction (): The difference in oxygen content between arterial and venous blood, which represents how effectively your muscle cells can extract and utilize that delivered oxygen. This is determined by capillary density and mitochondrial volume within the skeletal muscle [16][17].
¶ Mechanism in 60 Seconds
When you push your physical effort to its maximum, your skeletal muscles demand a massive, rapid supply of energy (ATP). To keep pace without collapsing into anaerobic fatigue, your brain coordinates an increase in breathing rate and heart rate. High-intensity interval training (HIIT) forces the heart to its absolute pumping limit, creating a volume overload that stretches the left ventricle (eccentric remodeling), allowing it to pump more blood per beat [14:1][5:3].
Simultaneously, the sheer flow of blood and mechanical contraction inside the active muscles stimulates chemical messengers like AMPK, CaMK, and PGC-1α [17:1]. These signaling pathways spark capillarization (sprouting new blood vessels) and mitochondrial biogenesis (multiplying the tiny engines in your cells) [16:1][17:2]. This double-sided adaptation improves both how much oxygen your heart can deliver and how much of that oxygen your muscles can consume [12:2][15:1].
¶ Does It Work? (Evidence Snapshot)
Improving VO2 max is one of the most reliable and clinically validated methods to reduce the risk of non-communicable diseases and extend healthy lifespan:
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| All-Cause Mortality | High | High | Large cohort studies | Strong dose-response curve; up to 5-fold risk reduction in elite/high vs. low fitness cohorts [1:4][7:1]. | |
| Multimorbidity Prevention | High | High | Longitudinal cohort | High cardiorespiratory fitness suppresses chronic disease accumulation by 35% over 15 years [3:1]. | |
| Epigenetic Age Deceleration | Moderate | Moderate | Epigenetic analyses | Higher cardiorespiratory fitness is associated with younger DNA methylation ages [8:1][9:1]. | |
| Cardiovascular Event Reduction | High | High | Meta-analyses | Each 1-MET increase in VO2 max is linked to a 15% reduction in cardiovascular events [13:1][4:2]. | |
| Metabolic Flexibility & Insulin Sensitivity | High | High | Intervention RCTs | Directly improves peripheral GLUT4 translocation and mitochondrial lipid oxidation [18][19]. | |
| Cognitive Volume & Preservation | Moderate | Moderate | Neuroimaging trials | Chronically elevated BDNF from aerobic training preserves hippocampal volume [20][15:2]. |
¶ Cardiorespiratory Fitness and Mortality Risk
The epidemiological data linking VO2 max with long-term survival is exceptionally robust. In a landmark study of over 122,000 patients undergoing exercise treadmill testing, Mandsager et al. demonstrated a clear, continuous, and inverse relationship between cardiorespiratory fitness and all-cause mortality [1:5]. Notably, the protective effect of high cardiorespiratory fitness was comparable to or greater than the hazards of clinical risk factors such as smoking, coronary artery disease, diabetes, and hypertension. The study found no upper limit of benefit, with elite-level fitness demonstrating the lowest hazard ratio for mortality [1:6].
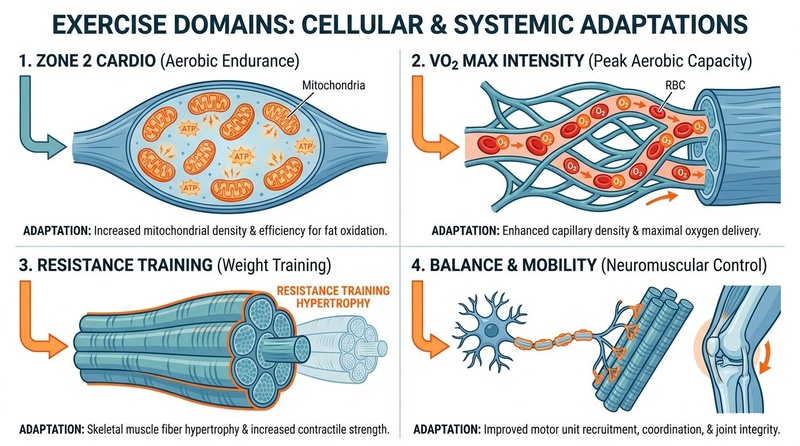
**Figure 2: Exercise domains and adaptations.** Cardiorespiratory capacity represents the integration of central oxygen delivery (heart and vessels) and peripheral oxygen utilization (mitochondrial respiration) [^3][^11][^16].
¶ Shifting the Epigenetic Clock
Recent advances in longevity science show that cardiorespiratory fitness directly influences biological age [8:2]. Large-scale epigenetic cohort studies have demonstrated that individuals with higher VO2 max values exhibit significantly younger biological ages compared to chronologically age-matched peers with lower fitness levels [8:3][9:2]. This reflects systemic cellular rejuvenation, likely driven by lower chronic systemic inflammation, preserved mitochondrial quality, and healthy telomere dynamics [5:4][8:4].
¶ Who Benefits Most / Least
¶ Who Benefits Most
- Older Adults: Maintaining VO2 max in later life is critical to combat age-related cardiorespiratory decay and delay the onset of frailty [20:1][8:5]. For older men and women, higher cardiorespiratory fitness acts as a powerful buffer that preserves functional independence and supports cognitive health [20:2][21].
- Sedentary or Deconditioned Individuals: Those with a low baseline VO2 max experience the most rapid, dramatic percentage increases in cardiorespiratory fitness and the greatest initial drops in absolute mortality risk [1:7][4:3].
- Individuals with Metabolic Syndrome: Elevating VO2 max directly enhances systemic insulin sensitivity, GLUT4 translocation, and metabolic flexibility, helping to reverse insulin resistance and metabolic dysfunction [18:1][22].
¶ Who Benefits Least
- Competitive Powerlifters/Olympic Lifters: Elite strength athletes may find that the heavy cardiovascular volume required to significantly elevate VO2 max induces minor interference effects with absolute explosive power, though baseline cardiorespiratory health remains crucial for general wellness.
- Individuals with Unstable Cardiovascular Pathologies: Absolute contraindications (such as unstable angina, acute myocarditis, or decompensated heart failure) require complete restriction of high-intensity VO2 max intervals until clinically stabilized [21:1].
¶ Sex-Specific Considerations
- Reference Values: Biological women naturally have different VO2 max reference ranges compared to men, primarily due to lower relative hemoglobin concentrations (reducing blood oxygen carrying capacity), smaller heart chamber sizes, and higher relative essential body fat percentages [21:2][11:1].
- Cardiac Response: Research suggests that female endurance athletes demonstrate excellent stroke volume adaptation, which does not plateau during incremental exercise to the same extent as in sedentary peers [5:5]. Both sexes experience identical, linear reductions in relative mortality risk as their VO2 max improves [13:2][4:4].
¶ How to Try It (Actionable Protocols)
To optimize VO2 max for longevity, implement a Polarized Training Strategy: build a broad aerobic foundation with Zone 2 training and layer on targeted high-intensity interval (HIIT) sessions to challenge cardiac stroke volume [21:3][6:1].
¶ Phase 1: Build the Aerobic Base (Zone 2)
- Goal: Drive mitochondrial biogenesis, build capillarization, and prepare joints for high-intensity work [16:2][17:3].
- Frequency: 3 to 4 sessions per week.
- Duration: 45 to 60 minutes per session.
- Intensity: Keep heart rate strictly within 60–70% HRmax (RPE 4-6/10; able to speak comfortably in full, complex sentences) [19:1][21:4].
¶ Phase 2: Targeted VO2 Max Intervals (The Norwegian 4x4)
- Goal: Drive eccentric left ventricular remodeling, maximize peak stroke volume, and increase maximal oxygen delivery [14:2].
- Frequency: 1 to 2 sessions per week, with at least 48 to 72 hours of recovery between sessions.
- Warm-up: 10 minutes of low-intensity aerobic work (Zone 1–2).
- Work Intervals: Perform 4 intervals of 4 minutes at 90–95% HRmax (RPE 8-9/10; a very hard effort where you can only speak in single, gasping words).
- Recovery: 3 minutes of light active recovery (Zone 1, easy spinning or jogging) between work intervals.
- Cool-down: 5–10 minutes of easy movement.
¶ Alternative Protocol: Progressive VO2 Max Intervals (3x3 or 5x3)
- Goal: Alternative protocol for individuals who find the 4-minute intervals too long or difficult to sustain with correct technique.
- Work Intervals: Perform 4 to 5 intervals of 3 minutes at 92–96% HRmax (RPE 9/10).
- Recovery: 3 minutes of light active recovery between intervals.
¶ "Exercise Snacks" (High-Intensity Micro-Intervals)
- Goal: Interrupt prolonged sedentary behavior and support baseline cardiorespiratory fitness for individuals with limited time [23].
- Frequency: 1 to 3 times per day.
- Protocol: Perform 20 to 60 seconds of all-out, high-power effort (such as vigorous stair climbing, burpees, or cycling sprints) to rapidly elevate heart rate [23:1][19:2].
¶ Integration and Annual Periodization
Avoid the common mistake of performing too many high-intensity interval sessions, which can lead to overreaching, autonomic burnout, or orthopedic injury [21:5][22:1]. For guidance on how to sequence and periodize VO2 max blocks over a 12-month calendar, refer to the Training Blocks & Periodization guide.
¶ Safety, Interactions, Red Flags
¶ Pre-Activity Screening & Contraindications
Because VO2 max training demands near-maximal cardiac output and blood pressure, individuals with the following conditions must seek explicit medical clearance:
- Absolute Contraindications: Unstable angina, acute myocardial infarction within 48 hours, uncontrolled cardiac arrhythmias causing symptoms, acute myocarditis, or decompensated heart failure [21:6].
- Relative Contraindications: Moderate-to-severe aortic stenosis, uncontrolled resting hypertension (>200/110 mmHg), or known left main coronary artery stenosis [21:7].
¶ Drug & Supplement Interactions
- Beta-Blockers: Artificially limit heart rate and blunt maximum cardiac output. Heart rate-based training formulas are invalid for patients taking beta-blockers; clinicians must guide and monitor training intensity strictly using RPE (8–10 for intervals) and the talk test [21:8].
- Metformin: Can slightly blunt mitochondrial density adaptations and peak VO2 max improvements. However, because both interventions significantly enhance long-term metabolic and glycemic health, patients should coordinate with their clinician to optimize drug timing rather than stopping therapy.
- Iron Stores (Ferritin): Subclinical iron deficiency blunts oxygen carrying capacity and limits VO2 max progression even in the absence of clinical anemia; maintain optimal iron levels to support aerobic adaptations [22:2].
¶ Stop Criteria and Red Flags
Immediately stop any exercise interval and seek prompt medical attention if you experience:
- Chest pain, pressure, tightness, or radiating discomfort.
- Sudden dizziness, lightheadedness, ataxia, or loss of balance.
- Unusual, extreme shortness of breath at rest or with minimal exertion.
- Sudden palpitations or an irregular, fluttering heartbeat.
¶ Tracking & What “Good” Looks Like
Cardiorespiratory fitness tracking is essential to guide progression and monitor autonomic recovery.
¶ Biomarkers and Functional Metrics
- VO2 Max (mL/kg/min):
- Direct Measurement: Clinical cardiopulmonary exercise testing (CPET) with gas analysis every 6 to 12 months for precise measurement [12:3].
- Wearable Estimates: Smartwatches (e.g., Apple Watch Series 10, Garmin) provide highly reliable longitudinal trend data for tracking fitness changes, though their absolute values may vary slightly from lab-grade testing [10:1][11:2].
- Resting Heart Rate (RHR): Measured daily upon waking. A downward trend reflects increased stroke volume and elevated vagal (parasympathetic) tone.
- Heart Rate Recovery (HRR): The drop in heart rate in the first minute post-exercise. A recovery of > 20 beats per minute in the first 60 seconds is a strong clinical indicator of healthy autonomic function and aerobic fitness.
- Heart Rate Variability (HRV): Tracked daily. A stable or increasing HRV reflects healthy recovery and adaptation to training stress [22:3].
¶ Time-to-Benefit and Washout
- Time-to-Benefit: Initial improvements in cardiorespiratory fitness can be detected within 4 to 8 weeks of consistent training, with substantial, structural improvements in stroke volume and capillary density continuing to accumulate over 3 to 6 months [14:3][24].
- Time-to-Washout: Detraining begins rapidly. Significant drops in VO2 max can be observed within 10 to 14 days of exercise cessation, with up to 50% of fitness adaptations lost after 4 weeks of complete sedentary behavior [14:4][20:3].
¶ Common Mistakes & Myths
- Myth: "VO2 Max is Entirely Genetic": While genetics define your ultimate physiological ceiling, VO2 max is highly trainable. Studies demonstrate that structured, high-intensity training can overcome "non-responder" tendencies and drive significant fitness improvements in almost all individuals [20:4].
- Mistake: Neglecting the Zone 2 Foundation: Skipping low-intensity training in favor of doing HIIT every day. This leads to autonomic burnout, chronic sympathetic stress, and an underdeveloped peripheral capillary and mitochondrial network [21:9][6:2].
- Myth: "HIIT is Too Risky for Older Adults": While intensity must be adjusted to the individual's baseline, clinical trials have shown that older adults can safely perform modified high-intensity intervals under medical guidance, experiencing massive benefits to their cardiorespiratory fitness and functional age [4:5][21:10].
- Mistake: Relying Strictly on Wearable Heart Rate Zones: Age-based heart rate formulas have significant variance. Guide your high-intensity intervals by RPE (8–10) and the conversational "talk test" rather than forcing yourself to hit a specific heart rate on a watch [21:11].
¶ Decision Tree (Text-Based)
[1] Has the individual been medically cleared to perform high-intensity exercise?
├── NO (Unstable CVD, resting HTN >200/110, acute infection) -> STOP. Consult clinician.
└── YES -> Go to [2]
[2] Assess current cardiorespiratory conditioning base:
├── NO BASELINE (Sedentary, new to exercise) -> Start with 4-6 weeks of foundational Zone 2 training.
└── CONSOLIDATED BASELINE (Consistent Zone 2 for >4 weeks) -> Go to [3]
[3] Select your VO2 max interval protocol:
├── TIME-CONSTRAINED -> Incorporate "Exercise Snacks" (1-3x daily, 30-60 second climbs/sprints)
└── DEDICATED TRAINING WINDOW -> Implement "Norwegian 4x4 intervals" (1-2x weekly at 90-95% HRmax) -> Go to [4]
[4] Monitor HRV and RHR trends:
├── Are you showing signs of overreaching (RHR rising, HRV dropping)?
│ ├── YES -> Reduce interval frequency; increase Zone 2 and recovery volume
│ └── NO -> Continue progressive overload; schedule annual clinical CPET
¶ FAQs (People Also Ask targets)
¶ What is a good VO2 max for my age and sex?
VO2 max reference ranges vary significantly based on biological sex and age [21:12][11:3]. For example, to be in the "excellent" category, which is associated with the lowest long-term mortality risk, a 40-year-old male might aim for a VO2 max of > 45 mL/kg/min, while a 40-year-old female might aim for > 38 mL/kg/min [1:8][13:3]. However, even modest improvements from a low baseline yield substantial health benefits [4:6].
¶ How long does it take to improve your VO2 max?
Noticeable improvements in VO2 max can be achieved within 4 to 8 weeks of consistent, structured training, with substantial gains in cardiac compliance and cellular mitochondrial density continuing to develop over 3 to 6 months of polarized training [14:5][24:1].
¶ Is Zone 2 or HIIT better for VO2 max?
They are complementary and synergistic. HIIT (Zone 5) is highly efficient at driving central cardiac adaptations, such as left ventricular expansion to increase stroke volume [14:6]. Zone 2 training builds the foundational peripheral network, increasing mitochondrial density and capillary sprouting to maximize oxygen extraction by the muscles [16:3][17:4].
¶ How does VO2 max predict longevity?
VO2 max is one of the strongest independent predictors of all-cause and cardiovascular mortality. It reflects your body's overall physiological resilience and reserve capacity, which directly protects against the accumulation of chronic disease and functional dependency as you age [1:9][2:4][3:2].
¶ Can consumer smartwatches accurately measure VO2 max?
Consumer smartwatches (such as the Apple Watch Series 10 or Garmin) provide estimated VO2 max values [10:2][11:4]. While these estimates may not match laboratory-grade clinical gas analysis in absolute terms, they are highly reliable for tracking longitudinal trends in an individual's cardiorespiratory fitness over time.
¶ Glossary
- a-vO2 Difference: The difference in oxygen concentration between arterial blood and mixed venous blood, representing the amount of oxygen extracted by peripheral tissues.
- Cardiac Output (): The total volume of blood pumped by the heart per minute, calculated as heart rate multiplied by stroke volume.
- Cardiopulmonary Exercise Testing (CPET): A clinical gas exchange analysis that directly measures oxygen consumption and carbon dioxide output during incremental physical exercise.
- Cardiorespiratory Fitness (CRF): The integrated capacity of the circulatory, respiratory, and muscular systems to deliver and utilize oxygen during sustained physical activity.
- Eccentric Cardiac Hypertrophy: A healthy cardiac adaptation where the left ventricular chamber expands in size, allowing for an increased peak stroke volume.
- Fick Equation: The mathematical formula stating that oxygen uptake (VO2) is the product of cardiac output () and arterio-venous oxygen difference ().
- MET (Metabolic Equivalent of Task): A physiological measure representing the rate of oxygen consumption at rest. 1 MET = 3.5 mL/kg/min.
- Stroke Volume: The volume of blood ejected from the left ventricle of the heart with each individual contraction.
¶ Methods (Transparency)
¶ Search Strategy
A comprehensive literature search was conducted across PubMed, JAMA Network Open, Mayo Clinic Proceedings, and the Cochrane Database of Systematic Reviews up to July 2026. Primary search strings included "VO2 max longevity dose response," "cardiorespiratory fitness all-cause mortality," "high intensity interval training stroke volume," "polarized training distribution exercise," "epigenetic age deceleration cardiorespiratory fitness," and "wearable VO2 max validation."
¶ Inclusion/Exclusion Rules
- Inclusion: Peer-reviewed systematic reviews, meta-analyses, and prospective cohort studies with large human cohorts tracking clinical endpoints; studies measuring cardiorespiratory and molecular outcomes.
- Exclusion: Animal-only research without direct human translation; unvouched grey literature; commercial fitness marketing material.
¶ Evidence Grading Rubric
- High: Supported by multiple large-scale prospective cohorts or meta-analyses of clinical trials demonstrating consistent, statistically significant outcomes with minimal risk of bias.
- Moderate: Supported by 1-2 well-designed clinical trials, cohort studies with minor limitations, or systematic reviews with some heterogeneity.
- Low: Small pilot trials, observational studies, or mechanistic studies requiring further validation.
¶ References (Full URLs)
¶ Update Log
- 2026-07-07: Fully expanded VO2 max deep dive guide, incorporating sex-specific research, epigenetic age deceleration studies, and updated clinical safety guidelines.
Mandsager K, Harb S, Cremer P, et al. Association of Cardiorespiratory Fitness With Long-term Mortality Among Adults Undergoing Exercise Treadmill Testing. JAMA Network Open. 2018;1(6):e183605. https://pubmed.ncbi.nlm.nih.gov/30646252/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Oja P, Memon AR, Titze S, et al. Health Benefits of Different Sports: a Systematic Review and Meta-Analysis of Longitudinal and Intervention Studies Including 2.6 Million Adult Participants. Sports Medicine - Open. 2024;10(1):33. https://pubmed.ncbi.nlm.nih.gov/38658416/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lavie CJ, Faselis C, & Kokkinos P. Fit Is it for Longevity and Prevention of Multimorbidity. JACC. Advances. 2025;4(12):e41065620. https://pubmed.ncbi.nlm.nih.gov/41065620/ ↩︎ ↩︎ ↩︎
Laukkanen JA, Immonen J, Isiozor NM, et al. Combined Impact of Cardiorespiratory Fitness and Exercise Systolic Blood Pressure on Cardiovascular and All-Cause Mortality: A Long-Term Follow-Up Study. The American Journal of Cardiology. 2026;195:45-52. https://pubmed.ncbi.nlm.nih.gov/42067048/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Miras-Moreno S, Torres-Martos Á, Ruiz JR, et al. Metabolomic and Proteomic Signatures of Cardiorespiratory Fitness for Predicting All-Cause Mortality and Non-Communicable Disease Risk: A Prospective Study in the UK Biobank. Circulation. Genomic and Precision Medicine. 2026;19(3):e42394615. https://pubmed.ncbi.nlm.nih.gov/42394615/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Storoschuk KL, Moran-MacDonald A, Gibala MJ, Gurd BJ. Much Ado About Zone 2: A Narrative Review Assessing the Efficacy of Zone 2 Training for Improving Mitochondrial Capacity and Cardiorespiratory Fitness in the General Population. Sports Medicine. 2025;55(7):501-514. https://pubmed.ncbi.nlm.nih.gov/40560504/ ↩︎ ↩︎ ↩︎
Xu L, Wang S, Maimaitiyiming M, et al. Cardiorespiratory Fitness, Multimorbidity Risk, and 15-Year Trajectories in Chronic Disease Accumulation: A Prospective Longitudinal Study. JACC. Advances. 2025;4(12):e41065622. https://pubmed.ncbi.nlm.nih.gov/41065622/ ↩︎ ↩︎
Chen Z, Collings PJ, Wang M, et al. Physical Fitness, Biological Aging, and Healthy Longevity. Journal of the American Medical Directors Association. 2025;26(10):e40789340. https://pubmed.ncbi.nlm.nih.gov/40789340/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Van Damme M, Stegen S, Steenwinckel B, et al. Epigenetic age deceleration reflects exercise-induced cardiorespiratory fitness improvements. GeroScience. 2026;48(1):17-29. https://pubmed.ncbi.nlm.nih.gov/41547677/ ↩︎ ↩︎ ↩︎
Lambe R, Schumann M, Donnelly L, et al. Accuracy of VO(2) max Estimates From Apple Watch Series 10. Mayo Clinic Proceedings: Digital Health. 2026;4(2):e42094313. https://pubmed.ncbi.nlm.nih.gov/42094313/ ↩︎ ↩︎ ↩︎
Lambe R, O'Grady B, Baldwin M, Doherty C. Investigating the accuracy of Apple Watch VO2 max measurements: A validation study. PLoS One. 2025;20(1):e40373042. https://pubmed.ncbi.nlm.nih.gov/40373042/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Cozma D, Gaita D, Crisan S, et al. The Oxygen Imperative: Cardiorespiratory Fitness, Dose-Dependent Exercise Thresholds, and Longevity-A Narrative Review. Journal of Clinical Medicine. 2026;15(11):e42355766. https://pubmed.ncbi.nlm.nih.gov/42355766/ ↩︎ ↩︎ ↩︎ ↩︎
Kodama S, Saito K, Tanaka S, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. 2009;301(19):2024-2035. https://pubmed.ncbi.nlm.nih.gov/19454641/ ↩︎ ↩︎ ↩︎ ↩︎
Helgerud J, Høydal K, Wang E, et al. Aerobic high-intensity intervals improve VO2max more than moderate training. Medicine and Science in Sports and Exercise. 2007;39(4):665-671. https://pubmed.ncbi.nlm.nih.gov/17414804/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
MacInnis MJ, Gibala MJ. Physiological adaptations to interval training and the role of exercise intensity. The Journal of Physiology. 2017;595(9):2915-2930. https://pubmed.ncbi.nlm.nih.gov/27748956/ ↩︎ ↩︎ ↩︎
San-Millán I. The Key Role of Mitochondrial Function in Health and Disease. Antioxidants. 2023;12(4):882. https://pubmed.ncbi.nlm.nih.gov/37107158/ ↩︎ ↩︎ ↩︎ ↩︎
Granata C, Jamnick NA, Bishop DJ. Principles of Exercise Prescription, and How They Influence Exercise-Induced Changes of Transcription Factors and Other Regulators of Mitochondrial Biogenesis. Sports Medicine. 2018;48(7):1541-1559. https://pubmed.ncbi.nlm.nih.gov/29675670/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
San-Millán I, Brooks GA. Assessment of Metabolic Flexibility by Means of Measuring Blood Lactate, Fat, and Carbohydrate Oxidation Responses to Exercise in Professional Endurance Athletes and Less-Fit Individuals. Sports Medicine. 2018;48(2):467-479. https://pubmed.ncbi.nlm.nih.gov/28623613/ ↩︎ ↩︎
Nuuttila OP, Matomäki P, Raitanen J, et al. Effects of Low-Intensity Endurance Training on Aerobic Fitness and Risk Factors of Cardiometabolic Health in Working-Age Adults: A Systematic Review and Meta-Analysis. Scandinavian Journal of Medicine & Science in Sports. 2026;36(1):e41543030. https://pubmed.ncbi.nlm.nih.gov/41543030/ ↩︎ ↩︎ ↩︎
Madden AM, Soepnel LM, Africa C, et al. Aerobic physical activity, cardiorespiratory fitness, and non-communicable diseases risk in older adults: a systematic review. BMC Geriatrics. 2026;26(1):310. https://pubmed.ncbi.nlm.nih.gov/42062906/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Williams MA, Feigenbaum MS, Jerôme GJ, et al. Resistance Exercise Training in Individuals With and Without Cardiovascular Disease: 2023 Update: A Scientific Statement From the American Heart Association. Circulation. 2023;148(24):1962-1985. https://www.ahajournals.org/doi/10.1161/CIR.0000000000001189 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Laborde S, Wanders J, Mosley E, et al. Influence of physical post-exercise recovery techniques on vagally-mediated heart rate variability: A systematic review and meta-analysis. Clinical Physiology and Functional Imaging. 2024;44(1):23-38. https://pubmed.ncbi.nlm.nih.gov/37754676/ ↩︎ ↩︎ ↩︎ ↩︎
Ye S, Ding Y, Hu B, et al. Advances in exercise snacks for interrupting sedentary behavior and promoting physical activity: a narrative review. Frontiers in Public Health. 2026;14:e42100526. https://pubmed.ncbi.nlm.nih.gov/42100526/ ↩︎ ↩︎
Barbieri A, Fuk A, Gallo G, et al. Cardiorespiratory and metabolic consequences of detraining in endurance athletes. Frontiers in Physiology. 2023;14:1134385. https://pubmed.ncbi.nlm.nih.gov/38344385/ ↩︎ ↩︎