¶ Body Scan
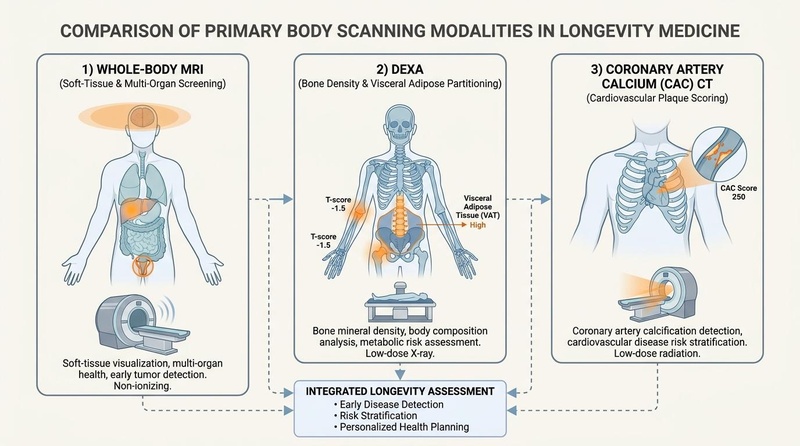
Body scanning technologies offer unparalleled insights into internal health, body composition, and early disease detection, empowering personalized longevity strategies. Whole-body MRI, DEXA, and Coronary Artery Calcium (CAC) CT each provide unique, complementary data crucial for proactive health management.
| Mechanism | MRI: Magnetic Fields, DEXA: X-ray, CT: Ionizing Radiation |
| Key Metrics | Organs, BMD, VAT, CAC Score |
| Primary Use | Early Detection, Risk Stratification |
| FDA Class | Class II/III (Varies) |
| Typical Cost | $500-$2,500+ (per scan) |
¶ At a glance
Body scans are advanced diagnostic tools that go beyond standard check-ups to reveal hidden health insights:
- Whole-Body MRI excels at soft-tissue and multi-organ screening, detecting tumors and other anomalies early [1][2].
- DEXA scans are the gold standard for precise bone mineral density (BMD) and body composition analysis, including critical visceral fat assessment [3][4].
- Coronary Artery Calcium (CAC) CT quantifies calcified plaque in coronary arteries, offering a powerful predictor of cardiovascular event risk and guiding statin/aspirin therapy [5][6].
- Incidental findings are common across all modalities, requiring careful clinical interpretation to avoid overdiagnosis and unnecessary interventions [7].
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Whole-Body MRI | |||||
| Opportunistic Cancer Detection (asymptomatic) | Moderate | Moderate | Meta-analysis of 11 studies [1:1] | 1.1% to 1.5% detection rate in general asymptomatic population. | |
| Incidental Finding Rate (benign) | High | High | Systematic Review [2:1][7:1] | High rate of benign incidentalomas (up to 70%), leading to follow-up scans. | |
| DEXA Scan | |||||
| Bone Mineral Density (Osteoporosis/Osteopenia) | High | High | Clinical consensus [3:1] | T-scores used for diagnosis; standard practice for bone health. | |
| Visceral Adipose Tissue (VAT) Assessment | High | High | Cohort Studies [4:1][8] | Strong predictor of metabolic and cardiovascular risk, refined by DEXA. | |
| Sarcopenia Diagnosis (Muscle Mass) | High | High | Clinical consensus [3:2][9] | Utilizes Appendicular Lean Mass (ALM) for diagnostic criteria. | |
| Coronary Artery Calcium (CAC) CT | |||||
| Cardiovascular Risk Reclassification | High | High | MESA Study, Cohort Studies [5:1][10] | Significantly improves risk prediction beyond traditional factors. | |
| Statin Therapy Guidance (CAC=0) | High | High | Cohort Studies [6:1][11] | Deferral of statins in very low-risk individuals with CAC=0. | |
| Aspirin Therapy Guidance | High | High | MESA Study [12] | Benefit limited to individuals with CAC >=100. |
¶ Mechanism
Each body scan technology operates on distinct physical principles to visualize internal structures and quantify specific health markers:
¶ Whole-Body Magnetic Resonance Imaging (WB-MRI)
WB-MRI uses powerful magnetic fields and radio waves to generate detailed images of soft tissues, organs, blood vessels, and bone marrow without ionizing radiation. Different tissue types respond uniquely to the magnetic fields, allowing for differentiation and the detection of abnormalities like tumors, cysts, and inflammation. Advanced sequences can assess organ function and tissue perfusion [2:2].
¶ Dual-Energy X-ray Absorptiometry (DEXA)
DEXA employs two distinct X-ray energies to differentiate between bone, lean mass, and fat mass throughout the body. This allows for precise quantification of bone mineral density (BMD), an essential metric for osteoporosis diagnosis, and detailed body composition analysis, including regional fat distribution such as visceral adipose tissue (VAT) [3:3].
¶ Coronary Artery Calcium (CAC) CT
CAC CT uses low-dose X-ray computed tomography to detect and quantify calcified plaque in the coronary arteries. Calcium deposits in the arterial walls are a direct indicator of atherosclerosis, even in asymptomatic individuals. The amount of calcium, measured as an Agatston score, correlates directly with the extent of coronary artery disease and future cardiovascular event risk [5:2].
¶ Key Specs
¶ Whole-Body MRI
- Radiation: None (non-ionizing).
- Scan Time: Typically 45-90 minutes, depending on protocol.
- Coverage: Comprehensive soft tissue, organs, and bone marrow throughout the entire body.
- Resolution: High spatial and contrast resolution for soft tissues.
- Detection: Primary utility in opportunistic cancer screening and detection of a wide range of benign and malignant lesions [1:2].
- Limitations: High cost, potential for false positives (incidentalomas), and contraindications for metallic implants [7:2].
¶ DEXA Scan
- Radiation: Very low-dose ionizing radiation (comparable to natural background radiation).
- Scan Time: 5-15 minutes.
- Coverage: Full body or regional analysis (e.g., hip, spine, forearm, abdomen).
- Metrics: Bone Mineral Density (BMD), total and regional fat mass, lean mass, and visceral adipose tissue (VAT).
- Detection: Osteoporosis, osteopenia, sarcopenia, and precise body fat distribution.
- Limitations: Cannot image soft tissues or organs beyond fat/lean/bone differentiation.
¶ Coronary Artery Calcium (CAC) CT
- Radiation: Low-dose ionizing radiation.
- Scan Time: Very rapid, typically less than 10-15 seconds of scan time.
- Coverage: Specifically targets the coronary arteries.
- Metrics: Agatston score (quantifies calcium volume and density).
- Detection: Subclinical atherosclerosis, cardiovascular risk stratification.
- Limitations: Only detects calcified plaque; cannot visualize non-calcified soft plaque or soft tissue abnormalities.
¶ Protocols
¶ Whole-Body MRI for Asymptomatic Screening
- Frequency: Annual or biennial screening in high-risk individuals (e.g., cancer predisposition syndromes) [13][14]. Less frequent in general asymptomatic population.
- Patient Prep: Fasting for 4-6 hours may be required; removal of all metallic objects.
- Considerations: Importance of an experienced radiologist and a clear protocol for managing incidental findings to minimize unnecessary follow-up [15][16].
¶ DEXA Body Composition & Bone Density
- Frequency: Annually for body composition tracking, every 1-2 years for bone density in at-risk populations.
- Patient Prep: Minimal; avoiding heavy meals before the scan can optimize body composition accuracy.
- Interpretation: T-scores for BMD (Osteoporosis: T-score <= -2.5; Osteopenia: -2.5 < T-score < -1.0). Appendicular Lean Mass Index (ALMI) used for sarcopenia (e.g., <7.0 kg/m² for men, <5.5 kg/m² for women) [9:1]. Visceral Adipose Tissue (VAT) mass or area linked to metabolic syndrome risk [4:2].
¶ Coronary Artery Calcium (CAC) CT
- Frequency: Generally once for baseline risk assessment in intermediate-risk asymptomatic adults. Repeat scans are not routinely recommended unless risk factors change significantly.
- Patient Prep: Minimal; hold beta-blockers or caffeine if advised by clinician to lower heart rate.
- Interpretation: Agatston scores guide risk:
- CAC = 0: Very low risk, often called the "power of zero," indicating a low likelihood of future cardiovascular events, potentially allowing statin deferral [6:2].
- CAC 1-99: Mild plaque, increased risk.
- CAC 100-299: Moderate plaque, increased risk, statin therapy often recommended.
- CAC >= 300 (or >= 400): Extensive plaque, high risk, aggressive risk factor modification and statin therapy strongly recommended [5:3][17].
- Guidelines: Endorsed by ACC/AHA for refining cardiovascular risk in intermediate-risk individuals for statin and aspirin allocation [5:4][18][12:1]. Not indicated for patients with known ASCVD [19].
¶ Evidence
Body scanning technologies provide quantitative, objective data that significantly enhances risk stratification and personalized health interventions.
¶ Whole-Body MRI for Cancer Screening
Systematic reviews and meta-analyses show that WB-MRI can opportunistically detect clinically significant cancers in asymptomatic individuals, with detection rates ranging from 1.1% to 1.5% in general healthy populations [1:3]. However, these screenings also yield a high rate of incidental findings (incidentalomas) that are often benign, leading to further investigations, patient anxiety, and increased healthcare costs [2:3][7:3][20]. Guidelines emphasize structured protocols to manage these findings and minimize overdiagnosis [15:1]. In high-risk populations, such as those with cancer predisposition syndromes like Li-Fraumeni, annual WB-MRI surveillance has demonstrated clinical efficacy and survival advantages [13:1][14:1].
¶ DEXA for Body Composition and Sarcopenia
DEXA is widely recognized as the most accurate method for assessing body composition, providing precise measurements of fat mass, lean mass, and bone mineral density. This precision is crucial for:
- Sarcopenia: Diagnosing age-related muscle loss using Appendicular Lean Mass (ALM) indices [3:4][9:2]. This helps identify individuals at risk of falls, frailty, and metabolic complications.
- Visceral Adipose Tissue (VAT): Quantifying VAT, which is a strong independent predictor of metabolic syndrome, insulin resistance, and cardiovascular disease risk [4:3][8:1]. DEXA's ability to differentiate VAT from subcutaneous fat provides actionable insights for lifestyle interventions.
¶ Coronary Artery Calcium (CAC) Scoring
CAC scoring is a powerful tool for cardiovascular risk assessment, especially in asymptomatic individuals who are at intermediate risk based on traditional risk factors.
- Risk Reclassification: The presence and extent of CAC significantly reclassify an individual's risk for major adverse cardiovascular events (MACE) beyond what is predicted by standard Pooled Cohort Equations [10:1].
- "Power of Zero": A CAC score of zero indicates a very low likelihood of coronary events over the next decade, often allowing for the deferral of statin therapy in otherwise eligible individuals [6:3][11:1].
- Treatment Guidance: CAC scores >=100 are associated with increased cardiovascular risk and generally warrant statin initiation. For aspirin therapy in primary prevention, benefits appear to be limited to those with CAC scores >=100, where the cardiovascular benefits outweigh the bleeding risks [12:2]. Guidelines from major cardiology organizations, including ACC/AHA, endorse CAC scoring for shared decision-making in primary prevention [5:5][17:1][21].
¶ Safety
Each body scanning modality has a distinct safety profile that must be considered:
¶ Whole-Body MRI
- Radiation: No ionizing radiation, making it generally safe for repeated scans.
- Contraindications: Absolute contraindications include certain metallic implants (e.g., pacemakers, some cochlear implants, cerebral aneurysm clips) and claustrophobia.
- Gadolinium Contrast: Some WB-MRI protocols use gadolinium-based contrast agents, which carry a rare risk of nephrogenic systemic fibrosis in patients with severe kidney dysfunction. Non-contrast protocols are often preferred for screening.
- Incidentalomas: The high sensitivity of WB-MRI can detect numerous incidental findings (incidentalomas) that are often benign, leading to anxiety, further unnecessary imaging, and potentially invasive follow-up procedures [7:4]. Careful counseling and a clear management plan are essential.
¶ DEXA Scan
- Radiation: Very low-dose ionizing radiation. The radiation exposure from a full-body DEXA scan is comparable to a cross-country flight or a few days of natural background radiation, making it safe for regular monitoring [3:5].
- Contraindications: Pregnancy.
- Limitations: Not suitable for imaging soft tissues or organs; limited diagnostic utility beyond bone density and body composition.
¶ Coronary Artery Calcium (CAC) CT
- Radiation: Low-dose ionizing radiation. While the dose is low, it is still ionizing radiation, which should be considered when assessing the risk-benefit ratio, especially in younger individuals or those without elevated risk factors.
- Contrast: Typically performed without intravenous contrast, reducing risks associated with contrast agents.
- Overdiagnosis/Over-treatment: Misinterpretation or over-reliance on CAC scores without considering the full clinical picture can lead to unnecessary statin initiation or patient anxiety. Guidelines emphasize its role as a risk-refinement tool, not a standalone diagnostic [5:6]. Not recommended for patients with known cardiovascular disease [19:1].
¶ FAQ
What is the primary benefit of a whole-body MRI?
Whole-body MRI provides detailed imaging of soft tissues and organs without radiation, allowing for early detection of potential abnormalities, including tumors, cysts, and inflammation, across multiple body systems [1:4].
Is a DEXA scan safe for regular monitoring?
Yes, DEXA scans use very low-dose X-ray radiation, comparable to everyday background radiation. This makes them safe for annual or biennial monitoring of bone mineral density and body composition [3:6].
What does a Coronary Artery Calcium (CAC) score of zero mean?
A CAC score of zero indicates a very low amount of calcified plaque in your coronary arteries, often referred to as the "power of zero." It suggests a very low risk of future cardiovascular events and may allow for deferring statin therapy in some individuals [6:4].
Can body scans cure diseases?
No, body scans are diagnostic tools used for early detection and risk stratification. They do not treat or cure diseases. Early detection, however, can enable timely intervention and improve outcomes.
Are there any downsides to whole-body MRI screening?
While radiation-free, WB-MRI can lead to a high rate of incidental findings (incidentalomas), which are often benign but may cause patient anxiety and necessitate further, sometimes invasive, follow-up procedures. Careful clinical management is crucial [7:5].
¶ References
Martins da Fonseca, J., Trennepohl, T., & Pinheiro, L. G. (2026). Whole-body MRI for opportunistic cancer detection in asymptomatic individuals: a systematic review and meta-analysis. European Radiology. https://pubmed.ncbi.nlm.nih.gov/40884613/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kwee, R. M., & Kwee, T. C. (2019). Whole-body MRI for preventive health screening: A systematic review of the literature. Journal of Magnetic Resonance Imaging, 50(5), 1335-1349. https://pubmed.ncbi.nlm.nih.gov/30932247/ ↩︎ ↩︎ ↩︎ ↩︎
Han, A., Bokshan, S. L., Marcaccio, S. E., & Fleming, B. C. (2018). Diagnostic Criteria and Clinical Outcomes in Sarcopenia Research: A Literature Review. Journal of Clinical Medicine, 7(4), 70. https://pubmed.ncbi.nlm.nih.gov/29642478/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Mina, T., Yew, Y. W., Ng, H. K., & Loke, K. Y. (2023). Adiposity impacts cognitive function in Asian populations: an epidemiological and Mendelian Randomization study. The Lancet Regional Health. Western Pacific, 34, 100732. https://pubmed.ncbi.nlm.nih.gov/36851942/ ↩︎ ↩︎ ↩︎ ↩︎
Arnett, D. K., Blumenthal, R. S., Albert, M. A., Buroker, A. B., Goldberger, Z. D., Hahn, E. J., ... & Ziaeian, B. (2019). 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Journal of the American College of Cardiology, 74(10), 1376-1414. https://pubmed.ncbi.nlm.nih.gov/30894319/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Rajan, T., Rozanski, A., & Cainzos-Achirica, M. (2020). Relation of Absence of Coronary Artery Calcium to Cardiovascular Disease Mortality Risk Among Individuals Meeting Criteria for Statin Therapy According to the 2018/2019 ACC/AHA Guidelines. The American Journal of Cardiology, 126, 126-132. https://pubmed.ncbi.nlm.nih.gov/32941817/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
O’Sullivan, J. W., Muntinga, T., Grigg, S., & Ioannidis, J. P. A. (2018). Prevalence and outcomes of incidental imaging findings: umbrella review. BMJ, 361. https://pubmed.ncbi.nlm.nih.gov/29914908/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Linder, N., Solty, K., Hartmann, A., & Puder, J. J. (2019). Half-body MRI volumetry of abdominal adipose tissue in patients with obesity. BMC Medical Imaging, 19(1), 1-8. https://pubmed.ncbi.nlm.nih.gov/31640589/ ↩︎ ↩︎
Coin, A., Sarti, S., Ruggiero, E., Giannini, S., & Manzato, E. (2013). Prevalence of sarcopenia based on different diagnostic criteria using DEXA and appendicular skeletal muscle mass reference values in an Italian population aged 20 to 80. Journal of the American Medical Directors Association, 14(7), 533.e1-533.e8. https://pubmed.ncbi.nlm.nih.gov/23582341/ ↩︎ ↩︎ ↩︎
Akintoye, E., Afonso, L., Bengaluru Jayanna, M., Kumar, A., Njei, I., Rajan, T., ... & Cainzos-Achirica, M. (2021). Prognostic Utility of Risk Enhancers and Coronary Artery Calcium Score Recommended in the 2018 ACC/AHA Multisociety Cholesterol Treatment Guidelines Over the Pooled Cohort Equation: Insights From 3 Large Prospective Cohorts. Journal of the American Heart Association, 10(12), e019771. https://pubmed.ncbi.nlm.nih.gov/34092110/ ↩︎ ↩︎
Spahillari, A., Zhu, J., Ferket, B. S., Cainzos-Achirica, M., Greenland, P., Blaha, M. J., ... & Nasir, K. (2020). Cost-effectiveness of Contemporary Statin Use Guidelines With or Without Coronary Artery Calcium Assessment in African American Individuals. JAMA Cardiology, 5(8), 903-912. https://pubmed.ncbi.nlm.nih.gov/32401264/ ↩︎ ↩︎
Cainzos-Achirica, M., Miedema, M. D., McEvoy, J. W., & Blaha, M. J. (2020). Coronary Artery Calcium for Personalized Allocation of Aspirin in Primary Prevention of Cardiovascular Disease in 2019: The MESA Study (Multi-Ethnic Study of Atherosclerosis). Circulation, 141(19), 1604-1616. https://pubmed.ncbi.nlm.nih.gov/32233663/ ↩︎ ↩︎ ↩︎
Que, F. V. F., Ishak, N. D. B., & Li, S. T. (2025). Utility of Whole-Body Magnetic Resonance Imaging Surveillance in Children and Adults With Cancer Predisposition Syndromes: A Retrospective Study. JCO Precision Oncology. https://pubmed.ncbi.nlm.nih.gov/40138602/ ↩︎ ↩︎
Maoz, A., Chen, N., Umaretiya, P., & Acharya, U. (2025). Prospective Study of Annual Whole-Body Magnetic Resonance Imaging as Part of a Multimodality Screening Program for Individuals With Li-Fraumeni Syndrome. JCO Precision Oncology. https://pubmed.ncbi.nlm.nih.gov/41129770/ ↩︎ ↩︎
Kierans, A. S., Hentel, K. D., & Dodelzon, K. (2026). How to implement a radiologist led whole-body MRI screening program. Radiology Advances. https://pubmed.ncbi.nlm.nih.gov/41878666/ ↩︎ ↩︎
Basar, Y., Alis, D., & Tekcan Sanli, D. E. (2021). Whole-body MRI for preventive health screening: Management strategies and clinical implications. European Journal of Radiology, 137, 109598. https://pubmed.ncbi.nlm.nih.gov/33596499/ ↩︎
Golub, I. S., Termeie, O. G., & Kristo, S. (2023). Major Global Coronary Artery Calcium Guidelines. JACC. Cardiovascular Imaging, 16(1), 1-13. https://pubmed.ncbi.nlm.nih.gov/36599573/ ↩︎ ↩︎
Stone, N. J., & Grundy, S. M. (2019). The 2018 AHA/ACC/Multi-Society Cholesterol guidelines: Looking at past, present and future. Progress in Cardiovascular Diseases, 62(5), 379-388. https://pubmed.ncbi.nlm.nih.gov/31733217/ ↩︎
Murphy, S. J., & Winchester, D. E. (2025). Prevalence of CAC Scoring in Patients With Known Coronary Artery Disease: A Cohort Study on Choosing Wisely. Journal of Evaluation in Clinical Practice. https://pubmed.ncbi.nlm.nih.gov/40581979/ ↩︎ ↩︎
Tarnoki, D. L., Tarnoki, A. D., & Richter, A. (2015). Clinical value of whole-body magnetic resonance imaging in health screening of general adult population. Radiology and Oncology, 49(1), 1-10. https://pubmed.ncbi.nlm.nih.gov/25810696/ ↩︎
Pavlović, J., Bos, D., & Ikram, M. K. (2025). Guideline-Directed Application of Coronary Artery Calcium Scores for Primary Prevention of Atherosclerotic Cardiovascular Disease. JACC. Cardiovascular Imaging. https://pubmed.ncbi.nlm.nih.gov/40047745/ ↩︎