¶ Cellular Senescence Interventions
| Indication | Targeting age-related disease & cellular aging (investigational/off-label) |
| Access | Rx (Dasatinib, UBX1325), OTC (Fisetin, Quercetin), Clinical trials |
| Dosing Sched | Intermittent (senolytics) or continuous (senomorphics) |
| Safety Profile | Moderate (clinical pilot protocols) to High (oncological dose profiles) |
| Key Marker | p16INK4a, p21CIP1, SASP factors (IL-6, IL-8, MCP-1), soluble IL-23R |
| Est. Cost | $20 - $500+/month (regimen-dependent) |
Cellular senescence interventions, comprising senolytics (which selectively clear senescent cells) and senomorphics (which suppress their chronic secretory signaling), represent a key paradigm in translational geroscience. While initially validated in animal models showing dramatic extensions of healthspan and physical function, human translation has progressed to Phase 1 and Phase 2 clinical trials targeting specific inflammatory and degenerative pathologies, including idiopathic pulmonary fibrosis, diabetic kidney disease, diabetic macular edema, and Alzheimer's disease[1][2][3][4][5][6].
¶ At a glance
¶ Key points
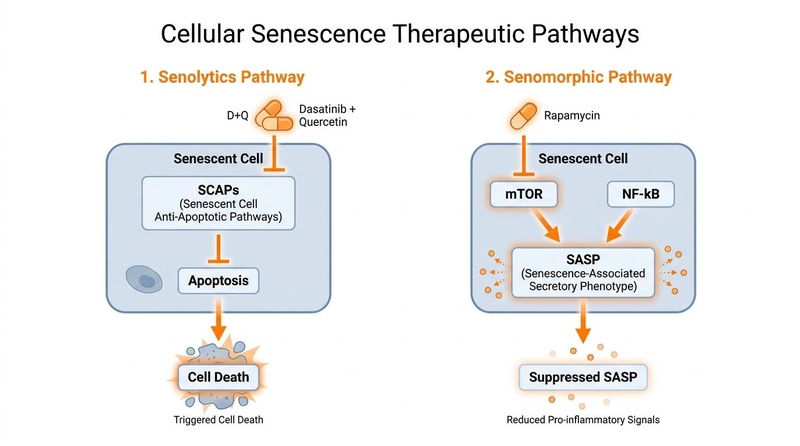
- Targeted Removal: Senolytics exploit the unique, temporary dependencies of senescent cells on survival pathways to selectively trigger their apoptosis (programmed cell death) without harming surrounding healthy tissue[7].
- SASP Suppression: Senomorphics do not kill senescent cells but rather suppress the Senescence-Associated Secretory Phenotype (SASP)—the toxic mix of pro-inflammatory cytokines, chemokines, and matrix metalloproteinases that drives systemic "inflammaging" and tissue degradation[2:1][8].
- Clinically Validated Regimens: Early-stage human trials with the combination of Dasatinib and Quercetin (D+Q) have confirmed feasibility, tissue-level target engagement, and physical performance improvements in conditions like Idiopathic Pulmonary Fibrosis (IPF) and Diabetic Kidney Disease (DKD)[1:1][2:2].
- Localized Senolysis: Intravitreal administration of the BCL-xL inhibitor UBX1325 (foselutoclax) has demonstrated safety and durable improvements in visual acuity and retinal structure in patients with diabetic macular edema (DME)[5:1][6:1].
- Emerging Frontier Modalities: Preclinical breakthroughs are driving next-generation therapies, including CAR T-cells targeting the urokinase-type plasminogen activator receptor (uPAR) and senolytic vaccines targeting markers like GPNMB, aiming for long-lasting, precise clearance[9][10][11].
¶ What people use it for
- Combating Age-Related Inflammaging: Reducing chronic systemic inflammation fueled by senescent cell accumulation, which contributes to conditions like giant cell arteritis and polymyalgia rheumatica[12].
- Physical Function Preservation: Improving functional capacity, mobility, and frailty indices in older age[1:2][7:1].
- Targeting Specific Degenerative Pathologies: Addressing conditions such as pulmonary fibrosis, diabetic nephropathy, osteoarthritis, Alzheimer's disease, and lens aging/cataracts[1:3][2:3][3:1][4:1][13].
¶ What It Is
Cellular senescence is a cell state characterized by a stable, irreversible arrest of the cell cycle, accompanied by phenotypic alterations including chromatin reorganization, metabolic active enlargement, and secretion of a pro-inflammatory profile (the SASP)[2:4][8:1]. Senescence is triggered by cellular stressors, including telomere attrition, DNA damage, oncogenic activation, and oxidative stress.
While transient senescence serves key physiological roles during embryogenesis, tissue remodeling, and wound healing, the chronic accumulation of senescent cells with age leads to pathological consequences. These "zombie cells" resist apoptosis through upregulated Senescent Cell Anti-Apoptotic Pathways (SCAPs) while chronically secreting pro-inflammatory molecules that disrupt neighboring cells, promote tissue fibrosis, and exhaust stem cell niches[8:2][14][7:2].
In the context of lens aging, senescent lens epithelial cells (LECs) are particularly vulnerable to oxidative stress, leading to p53/p21 and p16/Rb pathway activation, which disrupts lens homeostasis and accelerates cataract formation[13:1]. Similarly, cellular senescence and its associated SASP contribute to the pathogenesis of inflammatory rheumatic disorders like giant cell arteritis (GCA) and polymyalgia rheumatica (PMR) by driving inflammation and tissue damage[12:1].
¶ Mechanism in 60 seconds
Senescent cells survive by hijacking anti-apoptotic mechanisms (such as the BCL-2, PI3K/AKT, and p53/FOXO4 networks) to ignore cell death signals. Senolytics act as targeted biochemical wrenches, disrupting these SCAP networks (e.g., inhibiting BCL-xL or interrupting the FOXO4-p53 interaction) to selectively tip the senescent cell into apoptosis[15][14:1][7:3]. Alternatively, senomorphics act as signaling brakes (primarily inhibiting the mTOR or NF-κB pathways) to turn off the production of SASP factors, effectively silencing the cell's toxic inflammatory output without killing the cell itself[8:3].
¶ Does It Work? (Evidence Summary Table: Human Outcomes)
The clinical evidence for cellular senescence interventions in humans is emerging, with pilot trials confirming target engagement and safety, alongside some preliminary efficacy signals.
| Outcome / Goal | Effect* | Consistency** | Evidence Quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Physical Performance (IPF) | Moderate | Moderate | 2 Pilot Trials | D+Q (D: 100 mg/d, Q: 1250 mg/d) for 3 consecutive days/week for 3 weeks improved 6-minute walk distance and chair-stand speed[1:4][9:1]. | |
| Tissue Clearance (DKD) | High | Moderate | 1 Open-Label | D+Q (D: 100 mg/d, Q: 1000 mg/d) for 3 consecutive days reduced p16+ and p21+ cells in adipose tissue biopsies and lowered circulating SASP factors at day 11[2:5]. | |
| Bone Metabolism (Osteoporosis) | Low | Moderate | 1 RCT | Cyclic D+Q in postmenopausal women confirmed target engagement/safety, but bone mineral density changes were not statistically significant[3:2]. | |
| Adiposity & Inflammatory Markers | High | Moderate | 2 RCTs | Daily Fisetin (100 mg/d) combined with exercise over 12 weeks significantly reduced pro-inflammatory adipokines and upregulated the lipid mediator Maresin-1[16][17]. | |
| Cognitive Decline (Alzheimer's) | Moderate | Low | 1 Pilot Trial | STOMP-AD trial demonstrated that intermittent D+Q over 12 weeks was safe, well-tolerated, and showed exploratory reductions in CSF chemokine SASP profiles[4:2][18]. | |
| Diabetic Macular Edema (DME) | High | Moderate | 1 Phase 1, 1 Phase 2 RCT | Intravitreal UBX1325 (foselutoclax) was safe, well-tolerated, and led to rapid, durable improvements in visual acuity and central subfield thickness over 24-48 weeks[5:2][6:2]. | |
| Atherosclerosis Modification | Low | Very Low | Preclinical Only | Preclinical models show clearance of senescent foam cells; human clinical trials evaluating cardiovascular outcomes are currently lacking[14:2][19]. | |
| Intestinal Regeneration | Low | Very Low | Preclinical Only | Insufficient human data. Anti-uPAR CAR T-cells show powerful recovery of mucosal barrier and fitness in aging animal models, but human testing has not commenced[10:1]. | |
| Life Extension (Seno-Vaccination) | Low | Very Low | Preclinical Only | Insufficient human data. GPNMB-targeted senolytic vaccines extended remaining lifespan in progeroid mice; clinical safety and efficacy in humans remain completely unstudied[11:1][20]. |
- *Effect: Compact renderer encoding is utilized. Direction:
u(upward/increase),d(downward/decrease),e(no effect),q(unclear/insufficient data). Magnitude:0-3. Impact:p(positive),n(negative),x(neutral/unknown). - Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree).
- *Trials: Number of completed clinical trials or pilot studies informing the specific human outcome.
¶ Mechanisms of Action
To selectively target or silence senescent cells, therapeutic interventions leverage distinct biochemical, molecular, and cellular pathways.
STRESSORS (DNA Damage, Telomeres, ROS)
│
▼
SENESCENT STATE
│
┌──────────────────┴──────────────────┐
▼ ▼
SCAP PATHWAYS (Survival) SASP SECRETION (Toxic)
(BCL-2, AKT, p53-FOXO4) (IL-6, IL-8, MMPs)
│ │
(Inhibited by Senolytics) (Suppressed by Senomorphics)
(e.g., D+Q, Fisetin, FOXO4-DRI) (e.g., Rapamycin, Metformin)
│ │
▼ ▼
APOPTOSIS TISSUE SILENCING
(Cell Death & Clearance) (Resolution of Inflammation)
¶ 1. Senescent Cell Anti-Apoptotic Pathways (SCAPs)
Senescent cells develop defense mechanisms to resist the apoptosis that typically eliminates dysfunctional cells. They depend on specific SCAP networks to survive[8:4][7:4]:
- BCL-2 / BCL-xL Pathway: Anti-apoptotic proteins block the mitochondrial release of cytochrome c. Senolytics like Quercetin and Navitoclax inhibit these proteins, enabling cell death pathways to proceed.
- Ephrins and Tyrosine Kinases: Dasatinib, a multi-site tyrosine kinase inhibitor, disrupts cell survival networks that rely on Ephrin receptors, predisposing senescent cells to apoptosis. When combined with Quercetin, D+Q acts synergistically, with Dasatinib destabilizing the cell and Quercetin initiating programmed cell death[7:5].
- FOXO4-p53 Axis: In senescent cells, the transcription factor FOXO4 binds to and sequesters p53 in the cell nucleus, keeping it from triggering apoptosis. The synthetic peptide FOXO4-DRI (D-Retro-Inverso) acts as a competitive antagonist, disrupting this binding. Once liberated, p53 translocates to the mitochondria to induce apoptosis, demonstrating high specificity for senescent cells over healthy counterparts[15:1][14:3].
¶ 2. SASP Regulation (Senomorphics)
Instead of killing the cell, senomorphics target downstream inflammatory signaling pathways to prevent the synthesis and release of SASP factors[8:5]:
- mTOR Inhibition: The kinase mTOR is a master regulator of protein translation. Senomorphics like Rapamycin block mTOR Complex 1 (mTORC1), which selectively decreases the translation of SASP mRNAs (including IL-6 and IL-1β) without affecting normal cellular protein synthesis.
- AMPK Activation & NF-κB Suppression: Metformin activates AMP-activated protein kinase (AMPK), which suppresses the activity of NF-κB, the primary transcription factor driving inflammatory gene transcription. This downregulates the SASP, helping resolve chronic tissue inflammation.
¶ Emerging Frontier Interventions
Beyond small-molecule senolytics and senomorphics, the frontier of geroscience is shifting toward precision, immune-mediated clearance strategies.