¶ Microneedling
| Indication | Atrophic scars, Alopecia, Rhytides, Melasma, Striae distensae |
| Access | OTC (Dermarollers) / Clinical (RF/Dermapen) |
| Dosing Sched | Weekly (scalp) to every 4–6 weeks (dermal) |
| Safety Profile | Excellent (non-ablative, preserves epidermis) |
| Key Marker | Erythema, Skin barrier recovery, Systemic minoxidil signs |
| Est. Cost | $50 (home) – $800/session (clinic RF) |
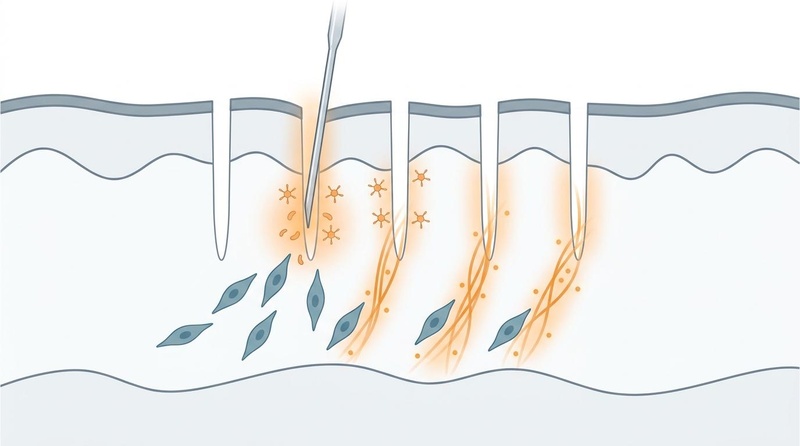
Microneedling, also known as Percutaneous Collagen Induction Therapy (PCIT), is a minimally invasive dermatological procedure that uses arrays of ultra-fine, sterile needles to create controlled microscopic punctures in the skin. By bypassing the stratum corneum without ablating the epidermis, microneedling initiates a localized cascade of wound healing that stimulates neocollagenesis, angiogenesis, and tissue remodeling. Beyond cosmetic facial rejuvenation, this mechanical modality is highly effective as an adjuvant transdermal drug delivery system and has established strong evidence profiles in treating androgenetic alopecia, atrophic acne scars, and dyschromia.
¶ At a glance
¶ Key Points
- Mechanical Signal Transduction: Mechanical micro-injuries trigger a natural healing response, transforming physical pressure into biochemical signals that remodel the extracellular matrix without thermal or chemical damage [1][2].
- Synergistic Adjuvant: While useful as a monotherapy, its highest clinical efficacy is realized when stacked with topical agents (e.g., minoxidil, copper peptides, or tranexamic acid) or autologous blood products (PRP) due to a massive increase in skin permeability [3][4][5][6].
- Safety & Versatility: Because it preserves epidermal structural integrity, it has a superior safety profile compared to ablative lasers or deep chemical peels, with a very low risk of post-inflammatory hyperpigmentation (PIH), making it highly suitable for all skin types (Fitzpatrick I–VI) [7][1:1].
¶ What People Use It For
- Main Goals: Atrophic acne scar remodeling, reversing androgenetic alopecia, mitigating fine lines/wrinkles (rhytides), improving striae distensae (stretch marks), and clearing melasma/pigmentation.
- Evidence Quality: High for androgenetic alopecia (combined with minoxidil) [3:1][8][9] and atrophic scarring (with PRP) [4:1][10][11]; Moderate for rhytides [12][13] and melasma [5:1][14].
¶ What is Microneedling?
Historically derived from subcutaneous subcision techniques pioneered in the 1990s by Orentreich [15], modern microneedling was popularized in the mid-2000s by plastic surgeon Desmond Fernandes as a safe alternative to laser resurfacing [16]. The procedure physically disrupts the skin's outermost barrier, the stratum corneum, creating thousands of microscopic channels (micro-conduits) that extend into the papillary and reticular dermis.

¶ Devices and Technologies
Three primary form factors dominate both clinical and self-directed administration:
- Dermarollers (Manual): Handheld drums studded with fine surgical needles. While cost-effective, manual rollers enter and exit the skin at an angle, which can theoretically cause micro-tearing or "slice" injuries if not used with uniform, perpendicular pressure.
- Dermapens (Motorized): Electronic pens utilizing high-speed reciprocating needle cartridges. These devices insert needles vertically (90-degree angle), minimizing mechanical tearing, allowing precise adjustments to penetration depth (typically 0.1 mm to 2.5 mm), and delivering a significantly higher puncture density per square centimeter.
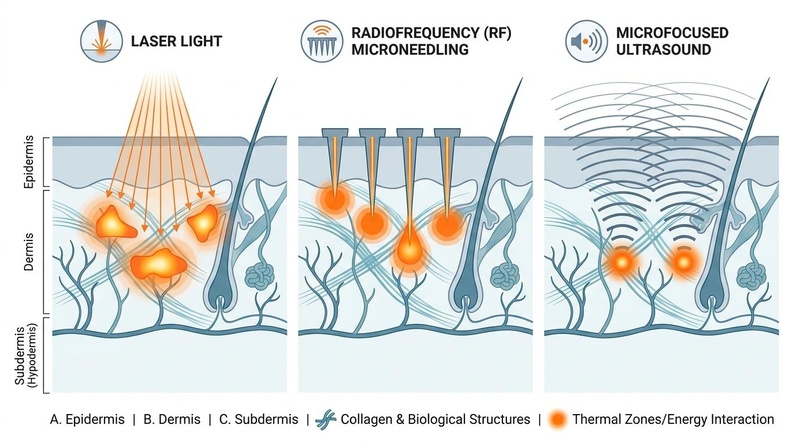
- Radiofrequency (RF) Microneedling: Advanced clinical systems where the needles act as electrodes. Upon reaching the target dermal depth, the needles emit a pulse of radiofrequency energy, generating local electrocoagulative thermal zones that significantly amplify skin tightening and deep scar remodeling [17].
¶ Main Benefits
¶ Skin Rejuvenation & Photoaging
The mechanical stimulation of dermal fibroblasts upregulates the transcription of structural proteins. Clinical systematic reviews confirm that regular sessions significantly reduce wrinkle depth, correct laxity, and restore elasticity by replenishing age-depleted dermal thickness [12:1][18][^Aust2008].
¶ Atrophic Scar Remodeling
In atrophic acne scars, abnormal, dense bands of collagen pull the epidermal surface downward. Microneedling mechanically breaks up these fibrotic scar bands while simultaneously triggering a highly organized deposition of new collagen and elastin fibers, raising the crater floor to match the surrounding tissue [4:2][10:1][1:2]. This process is highly synergistic with [[pages/prp-platelet-rich-plasma|Platelet-Rich Plasma (PRP)]] therapy, which accelerates [[pages/preventing-scars|scar remodeling]] and epidermal repair [11:1]. Comparative studies also evaluate microneedling against chemical peels for atrophic acne scars [19].
¶ Androgenetic Alopecia (Hair Restoration)
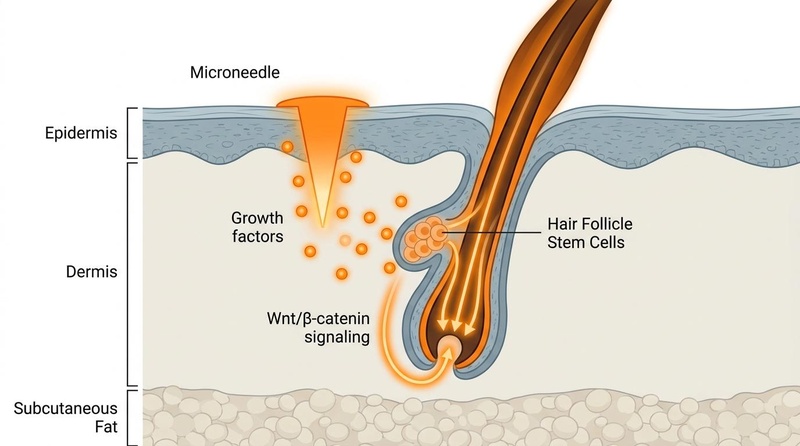
On the scalp, microneedling stimulates the bulge region of hair follicles where stem cells reside. Punctures trigger the release of platelet-derived growth factors and activate Wnt/β-catenin signaling, which shifts dormant telogen-phase follicles back into the active, hair-producing anagen phase [3:2][8:1][20]. This has established microneedling as one of the most powerful non-pharmacological adjuvants in modern [[pages/reversing-hair-loss|androgenetic alopecia]] protocols [9:1].
¶ Transdermal Drug Delivery Enhancement
The hydrophilic nature and molecular weight of many longevity-promoting compounds (e.g., peptides, growth factors, and hyaluronic acid) severely limit their passive diffusion across intact skin. Microneedling increases transdermal bioavailability by several orders of magnitude, converting topical application into a direct, deep-tissue delivery system [6:1][18:1][1:3]. This is particularly useful for delivering larger peptides such as [[peptides/ghk-cu|GHK-Cu (copper tripeptide-1)]] directly to the dermis [6:2].
¶ Striae Distensae & Stretch Mark Remodeling
Striae distensae represent a form of dermal scarring characterized by flattened epidermis and ruptured elastic fibers. Microneedling at deeper dermal thresholds (1.5 mm to 2.0 mm) induces neocollagenesis and neoelastinogenesis within these atrophic regions, significantly improving texture, depth, and pigmentation of both striae rubra and striae alba [21][22].
¶ Pigmentary Regulation (Melasma/Hyperpigmentation)
For pigmentary disorders like melasma, shallow needling (0.5 mm to 1.0 mm) enhances the absorption of topical depigmenting agents (such as tranexamic acid, vitamin C, or kojic acid) deep into the basal layer [5:2][14:1]. Radiofrequency microneedling has also shown efficacy for melasma [23].
¶ Evidence summary table (human outcomes)
The following matrix synthesizes findings from key systematic reviews, meta-analyses, and randomized clinical trials:
| Outcome | Effect | Consistency | Evidence Quality | Trials | Notes (protocol, population, and duration) |
|---|---|---|---|---|---|
| Atrophic Acne Scars (PRP Stack) | High | Low–Very Low (GRADE) | 14 RCTs | Combined PRP + microneedling increases odds of >50% improvement (Goodman's scale) by 2.97-fold compared to needling alone [4:3][10:2][11:2]. | |
| Atrophic Acne Scars (Topical Insulin Stack) | High | Low–Very Low (GRADE) | 9 RCTs | Microneedling with topical insulin shows comparable efficacy to PRP for post-acne scars [24]. | |
| Atrophic Acne Scars (vs. Chemical Peels) | Moderate | Moderate | 12 RCTs | Microneedling and chemical peels show comparable efficacy, with combinations often being superior [19:1]. | |
| Androgenetic Alopecia | High | Moderate | 12 RCTs | 1.0–1.5 mm scalp needling stacked with topical 5% minoxidil generates 4-fold greater hair count increases than minoxidil alone [3:3][8:2][9:2]. | |
| Skin Rejuvenation / Wrinkles | High | Moderate | 21 RCTs | Multi-session protocols (0.5–1.5 mm) lead to high patient-reported satisfaction (83%) and documented wrinkle reduction [12:2][13:1][^Aust2008]. | |
| Melasma Clearance | High | Moderate | 8 RCTs | 0.5–1.0 mm needling combined with topical tranexamic acid (TXA) or depigmenting agents outperforms topical monotherapy at 12 weeks [5:3][14:2][23:1]. | |
| Striae Distensae (Stretch Marks) | Moderate | Low | 14 RCTs | 1.5–2.0 mm needling significantly improves texture and pigmentation of both striae rubra and striae alba [21:1][22:1][^Sun2024]. |
¶ Mechanisms of Action
¶ Percutaneous Collagen Induction (PCI)
The biological response to microneedling is categorized into three distinct, overlapping physiological phases [2:1]:
- Hemostasis & Inflammation (Days 1–3):
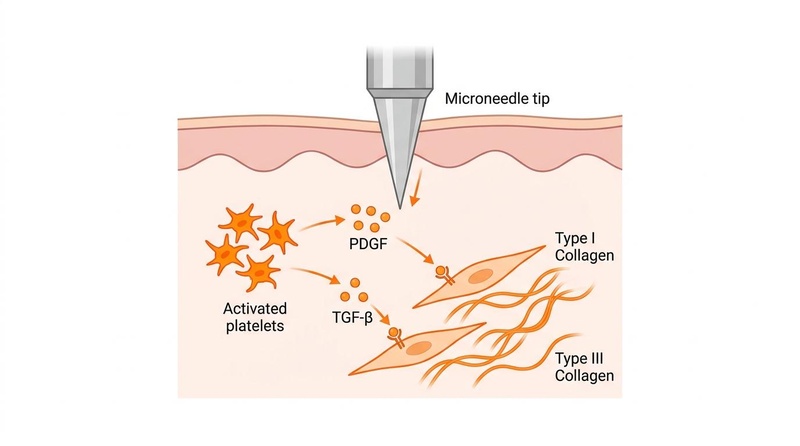
Physical needle penetration disrupts local capillaries, causing micro-bleeding and platelet activation. Degranulating platelets release critical cell-signaling proteins, including Platelet-Derived Growth Factor (PDGF), Transforming Growth Factor-alpha (TGF-α), and Transforming Growth Factor-beta (TGF-β) [1:4][2:2]. Neutrophils and macrophages infiltrate the micro-wounds to clear cellular debris and stimulate angiogenesis. - Proliferation & Fibroplasia (Days 3–14):
Dermal fibroblasts are activated and migrate into the micro-conduits, proliferating and laying down a temporary extracellular matrix rich in fibronectin. Fibroblasts synthesize Type III collagen (the rapid-wound-healing collagen subtype), elastin, and glycosaminoglycans [1:5][2:3]. Neovascularization is highly active, stimulated by local Vascular Endothelial Growth Factor (VEGF) release. - Dermal Remodeling & Maturation (Day 14 to 1 Year+):
The temporary Type III collagen matrix is gradually degraded by metalloproteinases and replaced with highly organized, parallel bundles of Type I collagen (the primary structural collagen found in healthy, youthful skin). This transition increases skin tensile strength, thickens the dermis, and tightens the cutaneous architecture over several months [1:6][2:4].
¶ The "Demarcation Current"
On a biophysical level, the metal needle's penetration into living tissue creates a physical disruption in the resting electrical potential of the cellular membranes. This electrical shift generates a localized "demarcation current" [1:7]. The change in bioelectric potential acts as a powerful physical signal that upregulates intracellular calcium concentration, directly stimulating fibroblast migration, cellular proliferation, and gene expression without requiring chemical or thermal triggers.
¶ Dosage & Protocols
¶ Needle Depth Hierarchy
Selecting the correct needle depth is critical to targeting the specific anatomical layer of the skin associated with different cosmetic and structural goals:
| Depth Range | Anatomical Target | Biological Goal | Typical Applications | Suggested Frequency |
|---|---|---|---|---|
| 0.25 mm – 0.3 mm | Stratum corneum & Epidermis | Enhance permeability; minor epidermal cell turnover | Skincare product penetration (hyaluronic acid, GHK-Cu) [18:2]. | 2–3 times per week |
| 0.5 mm – 1.0 mm | Papillary Dermis | Stimulate basal layer; moderate collagen deposition | Fine lines, superficial wrinkles, hyperpigmentation, mild acne scars [13:2]. | Every 2–4 weeks |
| 1.5 mm – 2.0 mm | Reticular Dermis | Deep collagen remodeling; stimulate follicular bulge | Deep acne scars, surgical scars, striae distensae, scalp needling [3:4][8:3][21:2]. | Every 4–6 weeks |
| 2.5 mm | Deep Reticular Dermis | Max mechanical disruption; deep remodeling | Severe contracture scars, deep hypertrophic scars (in-clinic only) [1:8][2:5]. | Every 6–8 weeks |
¶ Sanitization & Device Safety (At-Home Protocol)
Because microneedling breaks the physical barrier of the skin, strict hygiene protocols are non-negotiable to prevent biofilm development, local infections, or foreign body reactions:
- Sterilization: Motorized Dermapen cartridges must be strictly single-use and disposed of immediately. Manual dermarollers used at home must be fully submerged in 70% isopropyl alcohol for 30 minutes before and immediately after every session, allowed to air dry completely, and stored in a clean, protective case.
- Skin Preparation: The treatment area must be thoroughly cleansed with a gentle cleanser followed by a local antiseptic (e.g., isopropyl alcohol, chlorhexidine, or hypochlorous acid) to sterilize the skin surface.
- Device Lifespan: Manual rollers should be discarded after 10 to 12 uses, as the fine needle tips dull or bend over time, leading to micro-tearing of the epidermis ("fish-hooking") and an increased risk of scarring.
¶ Safety, Contraindications, & Systemic Absorption
¶ Systemic Absorption Risks
While enhancing transdermal delivery is a primary clinical benefit of microneedling, it introduces significant risks when coupled with inappropriate topicals.
CRITICAL CLINICAL CAUTION
Creating deep dermal micro-channels converts localized topical applications into systemic delivery vectors. Applying highly concentrated, non-sterile cosmetics, acidic formulations, or vasoactive drugs (such as minoxidil or steroids) immediately after deep needling (depths > 0.5 mm) can lead to rapid systemic absorption. In the case of minoxidil, this can trigger cardiovascular side effects including hypotension, heart palpitations, and tachycardia [25][7:1].
Furthermore, introducing non-sterile cosmetic ingredients (e.g., fragrances, preservatives, emulsifiers, or heavy silicone bases) into the open dermis can trigger chronic foreign-body granulomatous reactions, localized hypersensitivity, or severe contact dermatitis [7:2].
¶ Contraindications
Microneedling should not be performed under any of the following clinical conditions [7:3][1:9]:
- Active Local Infection: Active acne vulgaris (specifically pustular or cystic lesions), herpes simplex (risk of viral autoinoculation and systemic spreading), impetigo, or warts.
- Keloidal Diathesis: A known history of keloid scarring, as needling can trigger abnormal, excessive fibroproliferation.
- Systemic Therapies: Concurrent use of oral isotretinoin (Accutane) within the past 6 months (due to impaired wound healing and increased risk of atypical scarring).
- Compromised Healing: Active local eczema, psoriasis, severe rosacea, uncontrolled diabetes mellitus, concurrent immunosuppressive therapies, or active use of mTOR inhibitors such as [[supplements/rapamycin|Rapamycin (Sirolimus)]] (due to impaired fibroblast proliferation, anti-angiogenic properties, and delayed collagen synthesis [2:6]).
¶ Practical Integration & Stacks
¶ The Hair Growth Stack (Alopecia Protocol)
Combining scalp needling with 5% topical minoxidil is highly effective, but requires strict timing to avoid systemic absorption [3:5][8:4][25:1]:
- Weekly Scalp Needling: Perform microneedling at a depth of 1.0 mm to 1.5 mm on a clean, dry scalp until mild erythema is achieved.
- Timing Window: Do NOT apply minoxidil immediately. Wait a full 24 hours after needling before resuming topical minoxidil applications [25:2]. This allows the micro-channels to initiate closure, limiting systemic cardiovascular exposure while still benefiting from the upregulated growth factor cascade.
¶ The Scar Remodeling Stack (PRP Synergy)
Combining Platelet-Rich Plasma (PRP) with microneedling significantly accelerates scar clearance and reduces downtime [4:4][10:3]:
- Clinical Administration: Autologous blood is centrifuged to isolate the concentrated platelet fraction.
- Synergy: PRP is applied topically during the needling process, allowing the needles to push the growth factors deep into the dermal matrix, and immediately post-procedure to coat the skin.
¶ The Peptides & Rejuvenation Stack
For age-reversal and collagen synthesis, combining non-irritating peptides can yield dramatic results:
- Superficial Needling: Limit depth to 0.25 mm–0.5 mm on a clean face.
- Copper Peptides (GHK-Cu): Apply sterile, high-purity GHK-Cu serum immediately after needling. Polymeric microneedle pre-treatment has been shown to increase GHK-Cu dermal penetration by up to several folds, directly amplifying collagen synthesis and tissue repair [6:3].
¶ The Post-Recovery Photobiomodulation Stack
Integrating Red Light Therapy (PBM) can dramatically accelerate healing and downregulate post-procedure redness [1:10]:
- Erythema Reduction: Expose the treated area to red light (wavelengths between 630–670 nm at a target fluence of 4–8 J/cm²) immediately following a microneedling session. This modulates inflammatory cytokines, shifting fibroblasts into an anti-fibrotic remodeling phase and mitigating post-procedural swelling [1:11]. Applying [[pages/red-light-therapy|Red Light Therapy (RLT)]] immediately post-needling significantly accelerates skin recovery and enhances therapeutic synergy.
¶ Practical FAQ
How long does it take to see results from microneedling?
Initial skin brightening and mild plumping can be observed within 1–2 weeks due to epidermal cell turnover. However, true structural remodeling (collagen maturation and scar revision) takes a minimum of 4 to 12 weeks, with continuous histological improvements progressing up to a year after a treatment series [12:3][1:12].
Can I use a dermaroller every single day?
No. Deeper medical needling (0.5 mm or deeper) must be spaced 4 to 6 weeks apart because the collagen remodeling cascade takes several weeks to complete [1:13][2:7]. Needling too frequently interrupts this delicate healing cycle, which can cause chronic inflammation, degrade existing structural proteins, and increase the risk of hyperpigmentation or scarring. Only ultra-shallow cosmetic rollers (0.2 mm–0.25 mm) used strictly for increasing topical product absorption may be used 2–3 times per week [18:3].
What is the optimal needle depth for treating hair loss?
Clinical studies on androgenetic alopecia consistently use depths of 1.0 mm to 1.5 mm on the scalp [3:6][8:5]. This depth is required to reach the follicular bulge region located in the upper dermis, where hair follicle stem cells reside. Shallower depths (under 0.5 mm) are insufficient to trigger the necessary hair growth factors or activate the Wnt/β-catenin cascade.
Is radiofrequency (RF) microneedling superior to standard microneedling?
For skin tightening, deep wrinkles, and severe atrophic acne scars, RF microneedling is clinically superior. Standard microneedling relies solely on mechanical trauma to induce collagen, whereas RF needling simultaneously delivers targeted electrical thermal energy deep into the dermis. This double action causes instant collagen fiber contraction and generates a significantly larger wound healing response, though it carries higher entry costs and slightly more downtime [17:1].
How should I care for my skin immediately after a session?
For the first 24 hours, treat the skin as an open wound. Cleanse only with cool water or a very gentle, fragrance-free cleanser. Apply pure hyaluronic acid to maintain deep hydration. Avoid all makeup, physical sunscreens, retinoids, vitamin C, and exfoliating acids, and strictly avoid direct sun exposure.
¶ References
Singh A, et al. Microneedling: Advances and widening horizons. Indian Dermatology Online Journal. 2016;7(4):244-254. https://pmc.ncbi.nlm.nih.gov/articles/PMC4976400/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
StatPearls. Microneedling. NCBI Bookshelf. 2024. https://www.ncbi.nlm.nih.gov/books/NBK459344/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Pei S, et al. Efficacy and safety of combined microneedling therapy for androgenic alopecia: A systematic review and meta-analysis of randomized clinical trials. Journal of Cosmetic Dermatology. 2024;23(5):1560-1572. https://pubmed.ncbi.nlm.nih.gov/38239003/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kang C, Lu D. Combined Effect of Microneedling and Platelet-Rich Plasma for the Treatment of Acne Scars: A Meta-Analysis. Frontiers in Medicine. 2022;8:788754. https://pmc.ncbi.nlm.nih.gov/articles/PMC8882957/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Tan MG, et al. Microneedling as an adjuvant to topical therapies for melasma: A systematic review and meta-analysis. Journal of the American Academy of Dermatology. 2022;86(4):797–810. https://pubmed.ncbi.nlm.nih.gov/33857549/ ↩︎ ↩︎ ↩︎ ↩︎
Kang L, et al. Microneedle-Mediated Delivery of Copper Peptide Through Skin. Pharmaceutical Research. 2015;32(11):3585-3594. https://pubmed.ncbi.nlm.nih.gov/25690343/ ↩︎ ↩︎ ↩︎ ↩︎
Litchman G, et al. A Systematic Review Examining the Potential Adverse Effects of Microneedling. The Journal of Clinical and Aesthetic Dermatology. 2021;14(1):45–54. https://pmc.ncbi.nlm.nih.gov/articles/PMC7869810/ ↩︎ ↩︎ ↩︎ ↩︎
Dhurat R, et al. A Randomized Evaluator Blinded Study of Effect of Microneedling in Androgenetic Alopecia: A Pilot Study. International Journal of Trichology. 2013;5(1):6-11. https://pmc.ncbi.nlm.nih.gov/articles/PMC3746236/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Abdi R, et al. Evaluating the efficacy and safety of combined microneedling therapy versus topical Minoxidil in androgenetic alopecia: a systematic review and meta-analysis. Archives of Dermatological Research. 2025;317(1):12. https://link.springer.com/article/10.1007/s00403-025-04032-1 ↩︎ ↩︎ ↩︎
Juhasz ML, et al. Platelet-rich plasma use for treatment of acne scars: an overview of systematic reviews. Blood Transfusion. 2023. https://pmc.ncbi.nlm.nih.gov/articles/PMC11073618/ ↩︎ ↩︎ ↩︎ ↩︎
Li H, Jia B, Zhang X. Comparing the efficacy and safety of microneedling and its combination with other treatments in patients with acne scars: a network meta-analysis of randomized controlled trials. Archives of Dermatological Research. 2024;316(8):543. https://pubmed.ncbi.nlm.nih.gov/39110247/ ↩︎ ↩︎ ↩︎
Hou A, et al. Microneedling: Where do we stand now? A systematic review of the literature. Journal of Plastic, Reconstructive & Aesthetic Surgery. 2017;70(9):1241-1248. https://pubmed.ncbi.nlm.nih.gov/28690124/ ↩︎ ↩︎ ↩︎ ↩︎
Alster TS, Graham PM. Microneedling: A Review and Practical Guide. Dermatologic Surgery. 2018;44(3):397-404. https://pubmed.ncbi.nlm.nih.gov/28796657/ ↩︎ ↩︎ ↩︎
Feng X, et al. The efficacy and safety of microneedling with topical tranexamic acid for melasma treatment: A systematic review and meta-analysis. Journal of Cosmetic Dermatology. 2024. https://onlinelibrary.wiley.com/doi/10.1111/jocd.15965 ↩︎ ↩︎ ↩︎
Orentreich DS, Orentreich N. Subcutaneous incisionless (subcision) surgery for the correction of depressed scars and wrinkles. Dermatologic Surgery. 1995;21(6):543-549. https://pubmed.ncbi.nlm.nih.gov/7774134/ ↩︎
Fernandes D. Minimally invasive percutaneous collagen induction. Oral and Maxillofacial Surgery Clinics. 2005;17(1):51-63. https://pubmed.ncbi.nlm.nih.gov/18088764/ ↩︎
Kumar N, et al. Effectiveness of Radiofrequency Microneedling in the Treatment of Dermatological Conditions: A Systematic Review. Aesthetic Plastic Surgery. 2026 Apr. https://pubmed.ncbi.nlm.nih.gov/42047762/ ↩︎ ↩︎
Badran MM, et al. Skin penetration enhancement by a microneedle device (Dermaroller) in vitro: Dependency on needle size and applied formulation. European Journal of Pharmaceutical Sciences. 2009;36(4-5):511-523. https://pubmed.ncbi.nlm.nih.gov/19088764/ ↩︎ ↩︎ ↩︎ ↩︎
Agu-Jefferson I, et al. Microneedling Versus Chemical Peels for Atrophic Acne Scars: A Systematic Review and Meta-Analysis. Cureus. 2026 May. https://pubmed.ncbi.nlm.nih.gov/42281674/ ↩︎ ↩︎
Gupta AK, et al. Microneedling and Its Use in Hair Loss Disorders: A Systematic Review. Journal of Cosmetic Dermatology. 2021;21(1):120-130. https://pmc.ncbi.nlm.nih.gov/articles/PMC8776974/ ↩︎
Sun X, et al. Microneedling Therapy for Striae Distensae: Systematic Review and Meta-Analysis. Aesthetic Plastic Surgery. 2024. https://pubmed.ncbi.nlm.nih.gov/38509316/ ↩︎ ↩︎ ↩︎
Kaur T, et al. Comparative study of microneedling monotherapy versus microneedling with autologous platelet-rich plasma for the treatment of stretch marks (striae distensae) and post-surgical scars. Journal of Cosmetic Dermatology. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11619171/ ↩︎ ↩︎
Kumar N, et al. The Efficacy and Safety of Radiofrequency Microneedling for Melasma: A Systematic Review and Qualitative Evidence Synthesis. Aesthetic Surgery Journal Open Forum. 2026 Jan. https://pubmed.ncbi.nlm.nih.gov/42253423/ ↩︎ ↩︎
Albazee E, et al. Microneedling with Topical Insulin Versus Microneedling with Platelet-rich Plasma for Post-Acne Scars: A Systematic Review and Meta-Analysis with Trial Sequential Analysis. Aesthetic Plastic Surgery. 2026 Jun 21. https://pubmed.ncbi.nlm.nih.gov/42324392/ ↩︎
Hairgenetix. Minoxidil + Microneedling Meta-Analysis (2023). Research Summary. https://hairgenetix.com/blogs/articles/minoxidil-microneedling-meta-analysis-abdi-2023 ↩︎ ↩︎ ↩︎