¶ Red Light Therapy
| Mechanism | Photobiomodulation (Cytochrome c oxidase stimulation) |
| Key Spec | Wavelength (630–850 nm) & Irradiance (mW/cm²) |
| Protocol | Heterogeneous (Often 10–20 min, 3–5x weekly) |
| Distance | Contact to 6–12 inches (device-dependent) |
| FDA Class | Class II (various home and clinical panels) |
| Entry Cost | $100 - $2,000+ |
Red Light Therapy (RLT), scientifically known as photobiomodulation (PBM) or low-level light therapy (LLLT), uses specific wavelengths of red and near-infrared (NIR) light to stimulate cellular metabolism and modulate physiological pathways. While widely popularized for skin rejuvenation, wound repair, and muscle recovery, the clinical translation of RLT is constrained by highly heterogeneous protocols, skin pigmentation variables, and a limited depth of high-certainty human clinical evidence[1] [2] [3].
¶ At a glance
Key points
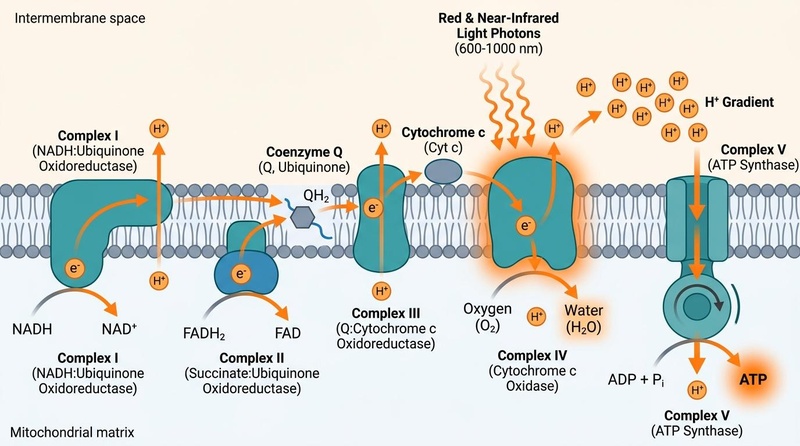
- Mitochondrial Target: Photons in the 600–1100 nm "therapeutic window" are absorbed by cellular chromophores, primarily cytochrome c oxidase, to influence ATP biogenesis and cellular signaling[1:1] [4].
- Clinical Limitations: Despite widespread commercial adoption, the clinical evidence base is characterized by significant heterogeneity in dosing, wavelength selection, and overall study quality, leaving the optimal clinical parameters largely unresolved[1:2] [2:1].
- Skin Pigmentation Impact: Melanin in highly pigmented skin acts as a competitive chromophore, reducing photon penetration and potentially compromising therapeutic efficacy unless protocols are personalized[3:1].
- Illumination Time: Preclinical evidence indicates that longer illumination times may be more critical to therapeutic outcomes than simply increasing total energy density or light intensity[5].
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Tissue Repair / Wound Healing | Moderate | Low | 5+ RCTs | Clinical guidelines are inconsistent; outcomes are heavily dependent on specific parameters like wavelength and energy density [1:3] | |
| Skin Rejuvenation (Wrinkles & Elasticity) | Moderate | Low | 4+ RCTs | Aesthetic outcomes are widely claimed, but trials are often small with high risk of bias and lack of standardized dosing [1:4] | |
| Joint Pain & Inflammation (Arthritis) | Moderate | Low | 6+ RCTs | Evidence is heavily reliant on preclinical models; human trials show highly variable outcomes due to poor parameter controls [5:1] | |
| Muscle Recovery & Performance | Mixed | Low | 5+ RCTs | Results are highly variable; optimal protocols for athletic recovery or performance remain unestablished [1:5] | |
| Hyperpigmentation / Melasma Reduction | Low | Very Low | 2+ RCTs | Extremely limited and conflicting evidence; competitive absorption by melanin poses a risk of hyperthermia and rebound hyperpigmentation in darker skin tones [3:2] |
- *Effect: Number of arrows (1-3) indicates magnitude. Direction: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Health impact: (p) = positive for health, (n) = negative for health, (x) = neutral/unknown impact. Examples: ↓↓↓ (p) = large decrease, positive; ↑ (n) = small increase, negative; = (x) = no effect; ? = unclear.
- *Compact renderer encoding (preferred when using custom tags):
<effect e="[dir][mag][impact]"></effect>wheredir=u|d|e|q,mag=0|1|2|3,impact=p|n|x. Examples:↓↓ (p)-><effect e="d2p"></effect>,= (x)-><effect e="e0x"></effect>,?-><effect e="q0x"></effect>. - IMPORTANT: If using the compact renderer encoding (<effect ...>), do NOT include the text arrows or parentheses next to it. Just use the tag.
- **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- ***Trials: Number of RCTs or total trials informing this outcome (shows evidence depth at a glance)
- REQUIRED: You MUST include a citation key (e.g.
[^1]) in the "Notes" column for every single row. If you claim a result, you must link the specific Meta-Analysis or Key RCT that proves it.
¶ Mechanism of Action
The biological effects of red light therapy are mediated through a cascade of cellular events initiated by the absorption of light by intracellular chromophores:
Mitochondrial Cytochrome c Oxidase Activation: The primary molecular mechanism of photobiomodulation involves the absorption of visible red and near-infrared photons by cytochrome c oxidase (CcO), also known as Complex IV of the mitochondrial electron transport chain[1:6] [4:1]. This absorption is hypothesized to alter the interfacial water layers within the mitochondria, reducing viscosity and enhancing the catalytic efficiency of the respiratory chain[4:2].
ATP Biogenesis & Nitric Oxide Dissociation: Stimulating CcO facilitates the dissociation of inhibitory nitric oxide (NO) from the enzyme's catalytic center. This dissociation restores oxygen binding, accelerates electron transport, and increases the synthesis of adenosine triphosphate (ATP)[4:3]. The liberated NO can then act as a localized vasodilator, improving microcirculation and tissue perfusion.
Oxidative Stress and Retrograde Signaling: Photobiomodulation induces transient, sub-lethal increases in reactive oxygen species (ROS) and cyclic AMP (cAMP) in vitro[5:2]. These signaling molecules trigger downstream transcription factors (such as NF-kB and AP-1), modulating gene expression profiles related to cell survival, proliferation, and anti-inflammatory pathways. However, excessive irradiance can overwhelm these homeostatic mechanisms, inducing harmful oxidative stress and cellular dysfunction.
¶ Key Specs
When evaluating or selecting a red light therapy device, several physical and optical parameters dictate the tissue-level dosing and clinical safety profile:
Wavelength (nm): Light propagation in human skin is highly wavelength-dependent. Red light (620–700 nm) has a shallower penetration depth (approximately 1–3 mm), targeting epidermal and dermal structures. Near-infrared light (700–1100 nm) penetrates deeper into subcutaneous tissues, fascia, and joints due to reduced scattering and absorption by water and hemoglobin[3:3] [6].
Irradiance and Fluence (Dose):
- Irradiance (Power Density): Measured in milliwatts per square centimeter (), irradiance determines the rate of photon delivery to the tissue surface.
- Fluence (Energy Density): Measured in Joules per square centimeter (), fluence represents the total energy delivered over time (). Because a biphasic dose-response exists in photobiomodulation, delivering too much energy can negate therapeutic benefits (the Arndt-Schulz law)[1:7].
Optical Modeling and Tissue Heterogeneity: Light transport through skin is highly complex and characterized by intense scattering. Monte Carlo simulations demonstrate that optical propagation is heavily modified by tissue heterogeneity, such as the thickness of the epidermal layer, background blood perfusion, and localized vascular structures[6:1] [7].
¶ Protocols
Clinical and at-home protocols are highly variable and lack standard consensus. However, critical variables must be managed:
Illumination Time vs. Intensity:
Preclinical models demonstrate that the duration of light exposure may be a more critical factor in determining therapeutic efficacy than either irradiance or total energy density alone[5:3]. For example, in animal models of inflammatory arthritis, longer illumination times (such as 10 to 100 minutes) consistently proved superior in reducing joint swelling and inflammatory markers (such as prostaglandin E2) compared to short, high-intensity exposures of equal or higher energy density[5:4].
The Skin Pigmentation Variable:
Melanin in the epidermis acts as a primary, competitive chromophore that strongly absorbs visible red light[3:4].
- Melanin Interference: In darker skin types (Fitzpatrick scale III–VI), highly concentrated epidermal melanin absorbs a significant fraction of incoming photons, severely impeding light propagation to deeper dermal and subcutaneous targets[3:5] [6:2].
- Racial Bias in Protocols: Standard clinical protocols and commercial device guidelines are almost universally developed based on lighter skin tones (Fitzpatrick types I–II), failing to adjust parameters for higher melanin concentrations. This oversight can lead to sub-therapeutic dosing in darker skin or, conversely, localized thermal injury due to heat generation within the pigmented epidermis[3:6].
- Required Adjustments: To optimize outcomes and prevent disparities, protocols should incorporate personalized parameters—such as adjusted exposure times or modified wavelengths—that account for individual skin pigmentation levels[3:7].
¶ Evidence
The clinical evidence supporting red light therapy across different therapeutic claims remains highly limited and characterized by methodological challenges.
¶ Musculoskeletal and Inflammatory Outcomes
Preclinical models of zymosan-induced arthritis demonstrate that low-level laser therapy (such as 810 nm wavelength) can reduce joint swelling and lower systemic inflammatory markers like prostaglandin E2 (PGE2)[5:5]. However, the translation to human clinical trials of osteoarthritis and rheumatoid arthritis has produced highly mixed and low-certainty results, primarily due to the failure to standardize illumination times, wavelength combinations, and device delivery modes.
¶ Wound Healing and Tissue Repair
The use of RLT to accelerate wound closure and repair is supported by some clinical literature, but the overall quality of evidence is low[1:8]. Outcomes are highly sensitive to technical parameters. For instance, in vitro methods developed to assess oxidative stress show that even minor changes in wavelength or intensity can shift cellular responses from cytoprotective to cytotoxic, making clinical consistency difficult to achieve[1:9] [5:6].
¶ Skin Rejuvenation and Aesthetics
While widely marketed for collagen synthesis and anti-aging, the aesthetic benefits of red light therapy are largely documented in small trials with high risk of bias. Standard commercial guidelines fail to address how individual skin variations, particularly epidermal melanin levels, affect the actual photon dose reaching dermal fibroblasts, leaving clinical efficacy highly unpredictable across diverse populations[1:10] [3:8].
¶ Safety
Although red light therapy is generally regarded as a low-risk intervention, critical safety hazards and contraindications must be managed.
¶ Eye Protection Requirements
Ocular safety is a primary clinical concern during RLT administration. Direct exposure to high-intensity red and near-infrared light can cause significant thermal and photochemical retinal damage, particularly because NIR light is invisible to the human eye and does not trigger the protective blink reflex[1:11].
- Standard Protection: Clinicians and patients must wear wavelength-specific safety goggles or protective eyewear designed to block the exact spectral output of the device.
- Periorbital Precautions: When treating facial or periorbital areas, appropriate opaque shielding is required to prevent accidental ocular exposure.
¶ Skin Safety and Contraindications
- Thermal Injury in Pigmented Skin: Because melanin absorbs light efficiently, individuals with darker skin tones are at a significantly higher risk of experiencing localized warming, hyperthermia, or thermal micro-injury if high-intensity devices are used without protocol adjustments[3:9].
- Photosensitivity: RLT is contraindicated in individuals with active photosensitive skin disorders (such as lupus erythematosus or porphyria) or those currently taking known photosensitizing medications (such as amiodarone, tetracyclines, or systemic retinoids)[1:12].
- Active Malignancy: RLT must not be applied directly over active malignant tumors or suspected cancerous lesions, as its proliferative cellular effects could theoretically accelerate tumor growth.
¶ FAQ
¶ Is red light therapy backed by strong clinical evidence?
No. While there is a substantial body of preclinical and in vitro research, high-quality, large-scale human clinical evidence remains highly limited[1:13]. Most human trials are small, suffer from methodological limitations, and use highly heterogeneous parameters, making it difficult to establish definitive clinical guidelines.
¶ How does skin tone affect red light therapy?
Melanin in darker skin tones acts as a competitive chromophore, absorbing red light before it can reach deeper dermal or subcutaneous tissues[3:10]. Consequently, standard device protocols designed for lighter skin types are often sub-therapeutic or carry a higher risk of localized heat generation in individuals with higher skin pigmentation[3:11].
¶ Can I use red light therapy without eye protection?
No. High-intensity red and NIR light can cause photochemical and thermal damage to the retina. Because near-infrared light is invisible, it does not trigger the natural pupillary constriction or blink reflex, making dedicated, wavelength-specific eye protection essential during use[1:14].
¶ Why is illumination time more important than power density?
Preclinical research shows that longer, controlled light exposure times are more effective at reducing inflammation and joint swelling than delivering a rapid, high-intensity dose of equal energy density[5:7]. High power density can also trigger a biphasic dose-response, where excess intensity actually inhibits cellular healing[1:15].
¶ References
Spongberg CV, Stack ER, Aprigliano C. What to Look for in Red Light Therapy: A Product Guide Backed by Science. Cureus. 2026 Mar 1;18(3):e105378. https://pubmed.ncbi.nlm.nih.gov/42005232/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sommer AP. Revisiting the Photon/Cell Interaction Mechanism in Low-Level Light Therapy. Photobiomodulation, Photomedicine, and Laser Surgery. 2019 Jun;37(6):347-353. https://pubmed.ncbi.nlm.nih.gov/31107170/ ↩︎ ↩︎
Girasol CE, Bachmann L. Is photobiomodulation therapy free from racial bias?: a narrative review of skin pigmentation. Sao Paulo Medical Journal. 2026 Apr 10;144(2):e20253358. https://europepmc.org/article/MED/41983886 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sommer AP. Revisiting the Photon/Cell Interaction Mechanism in Low-Level Light Therapy. Photobiomodulation, Photomedicine, and Laser Surgery. 2019 Jun;37(6):333-334. https://pubmed.ncbi.nlm.nih.gov/31107170/ ↩︎ ↩︎ ↩︎ ↩︎
Castano AP, Dai T, Yaroslavsky I, Cohen R, Aprigliano C. Low-level laser therapy for zymosan-induced arthritis in rats: Importance of illumination time. Lasers in Surgery and Medicine. 2007 Jul;39(6):543-550. https://pubmed.ncbi.nlm.nih.gov/25867757/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Girasol CE, Lobão RMQ, Sampaio MS. Monte Carlo simulations of optical propagation in human skin using experimentally measured laser parameters. Lasers in Medical Science. 2026 Jun 9;41(1):17. https://pubmed.ncbi.nlm.nih.gov/42262662/ ↩︎ ↩︎ ↩︎
Jacques SL. Coupling 3D Monte Carlo light transport in optically heterogeneous tissues to photoacoustic signal generation. Photoacoustics. 2014 Sep 10;2(4):137-142. https://pubmed.ncbi.nlm.nih.gov/25426426/ ↩︎