¶ Therapeutic Plasma Exchange (TPE)
| Indication | Medical Use (Autoimmune, Neurological, etc.) vs Investigational (Longevity) |
| Access | Rx |
| Dosing Sched | Variable (e.g., Every 24-48h for acute conditions) |
| Safety Profile | Moderate (Well-established risks in clinical settings) |
| Key Marker | Disease-specific biomarkers, electrolyte balance, coagulation |
| Est. Cost | High (Procedure-dependent) |
Therapeutic plasma exchange (TPE) is a medical procedure that involves removing a patient's plasma and replacing it with an appropriate fluid, typically 5% albumin or fresh frozen plasma. This extracorporeal therapy is an established treatment for a variety of antibody- or toxin-mediated diseases, such as thrombotic thrombocytopenic purpura and myasthenia gravis, as recognized by guidelines from organizations like the American Society for Apheresis (ASFA) [1]. While its efficacy in these conditions is well-documented, TPE is also being explored for potential applications in age-related conditions and as a longevity intervention, though evidence in these areas remains largely investigational and requires further robust clinical trials [2][3].
¶ At a glance
Key points (high-level summary)
- Established efficacy: Highly effective for numerous autoimmune, neurological, and hematologic conditions by removing pathogenic substances from the blood [1:1][4][5].
- Longevity potential: Preclinical studies suggest plasma dilution may offer regenerative benefits, but human evidence for anti-aging or epigenetic age reversal is currently insufficient and investigational [2:1][3:1].
- Safety profile: Generally safe when performed by experienced personnel, but carries risks such as hypocalcemia, hypotension, and infection, requiring careful monitoring [6][7][8].
- Versatile application: Protocols are tailored to specific diseases, influencing replacement fluid, volume, and frequency of exchange [1:2][9].
What people use it for
- Main goals: Treating autoimmune diseases, neurological disorders, hematologic conditions, and in some cases, severe inflammation. Investigational use for longevity and age-related decline.
- Evidence quality: High for established indications, Low/Investigational for longevity/anti-aging.
¶ What is Therapeutic Plasma Exchange (TPE)?
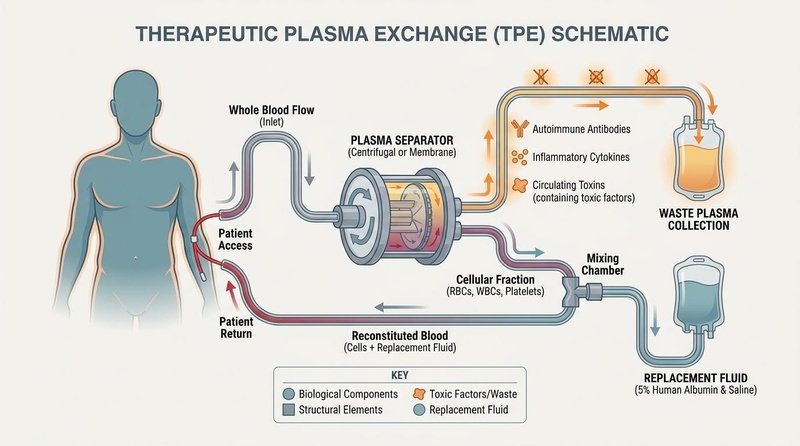
Therapeutic Plasma Exchange (TPE), also known as plasmapheresis, is an extracorporeal blood purification technique used to remove pathological substances from a patient's plasma. The process involves drawing whole blood, separating the plasma from cellular components (red blood cells, white blood cells, platelets) using centrifugal or membrane-based technologies, discarding the patient's plasma, and returning the blood cells reconstituted with a replacement fluid [1:3][4:1][9:1]. The choice of replacement fluid, most commonly 5% albumin or fresh frozen plasma, depends on the specific clinical indication and patient needs [1:4].
¶ Mechanisms of Action
TPE's therapeutic effects stem from several key mechanisms:
- Bulk Removal of Circulating Pathogens: TPE efficiently removes large molecular weight substances from the plasma, including autoantibodies, immune complexes, cryoglobulins, paraproteins, toxins, and inflammatory mediators such as cytokines and complement components. This rapid reduction in pathogenic factors can disrupt disease processes in conditions like autoimmune diseases and certain poisonings [4:2]. One plasma volume exchange can remove approximately 60-70% of intravascular constituents [9:2].
- Dilution and Replacement: The removed plasma is replaced with a fluid that lacks the harmful components. When albumin is used as a replacement, it can dilute existing toxic factors and alter the binding capacity within the plasma, potentially reducing the activity of remaining harmful substances. Fresh frozen plasma provides coagulation factors and immunoglobulins, which may be crucial in specific conditions [1:5][4:3].
- Neutral Blood Exchange Preclinical Evidence: Preclinical studies, particularly in mice, have explored "neutral blood exchange" where old blood plasma is exchanged with saline-albumin. These studies have shown that diluting the plasma with a saline-albumin solution can reduce inhibitory factors and improve tissue repair and function in multiple organs, suggesting a potential role for plasma manipulation in rejuvenating tissues and combating age-related decline [2:2]. However, the direct translation of these preclinical findings to human longevity or anti-aging interventions remains unproven [3:2].
- Immune Modulation: Beyond direct removal, TPE can indirectly modulate the immune system by altering B-cell and autoantibody dynamics, as well as complement activity, contributing to its efficacy in autoimmune disorders [4:4].
Schematic of Therapeutic Plasma Exchange (TPE) and Neutral Blood Exchange (NBE) showing extracorporeal separation, bulk removal of pathogenic circulating factors, and albumin-based plasma replacement.
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Autoimmune Neuromuscular Disorders (e.g., Myasthenia Gravis, GBS) | High | High | Multiple RCTs | Significant improvement in muscle strength and reduction of autoantibodies [5:1][10] | |
| Sepsis/Multiple Organ Dysfunction Syndrome (MODS) (in pediatric ICU) | Moderate | Moderate | Observational, small RCTs | Reduced mortality, though outcomes vary with severity and underlying cause [11][12] | |
| Pediatric Non-Neurological Diseases | Moderate | Moderate | Retrospective studies | Improved clinical outcomes in various conditions including renal and hematologic disorders [13] | |
| Alzheimer’s disease (AMBAR regimen) | Low | Low | 1 RCT (multicenter) | Slowed cognitive decline in moderate AD subsets; requires replication [14][15] | |
| Inflammatory cytokines (e.g., IL-6, TNF-α) | Low | Low | Small RCTs/observational | Transient reduction; effect varies by protocol and disease [16][17] | |
| Lipoprotein(a) (apheresis variants) | High | Moderate | Multiple trials | Significant reduction; technique-specific; not standard TPE [18] | |
| Epigenetic/Biological Age Reversal | Insufficient | Very Low | 0 RCTs | No confirmed human RCT evidence for direct effect [2:3][3:3] |
- *Effect: Number of arrows (1-3) indicates magnitude. Direction: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Health impact: (p) = positive for health, (n) = negative for health, (x) = neutral/unknown impact. Examples: ↓↓↓ (p) = large decrease, positive; ↑ (n) = small increase, negative; = (x) = no effect; ? = unclear.
- **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- ***Trials: Number of RCTs or total trials informing this outcome (shows evidence depth at a glance)
- REQUIRED: You MUST include a citation key (e.g.
[^1]) in the "Notes" column for every single row. If you claim a result, you must link the specific Meta-Analysis or Key RCT that proves it.
¶ Dosage & Protocols
TPE protocols are highly individualized based on the patient's condition, weight, and the specific substance being targeted for removal.
- Volume of Plasma Exchanged: Typically, 1.0 to 1.5 plasma volumes (PV) are exchanged per session. One plasma volume is approximately 40-50 mL/kg of body weight [1:6][9:3]. Exchanging 1 PV removes about 60-70% of a circulating substance, while 2 PVs remove about 80-85% [9:4].
- Replacement Fluid:
- 5% Albumin: The most common replacement fluid, used for most indications due to its oncotic properties and lack of coagulation factors, minimizing the risk of infection or allergic reactions associated with plasma [1:7].
- Fresh Frozen Plasma (FFP): Used when there is a need to replace coagulation factors, such as in thrombotic thrombocytopenic purpura (TTP), or to replace specific plasma proteins [1:8].
- Combination: Sometimes a combination of albumin and FFP is used.
- Anticoagulation: Citrate (ACD-A) is commonly used as an anticoagulant during the procedure. It chelates calcium to prevent clotting in the extracorporeal circuit. Patients must be monitored for citrate-related hypocalcemia, and calcium supplementation may be necessary [6:1][8:1]. Heparin can also be used, particularly in patients with citrate intolerance.
- Frequency: The frequency of TPE sessions varies widely depending on the disease, its severity, and the half-life of the pathogenic substance being removed. For acute autoimmune conditions, sessions may be performed daily or every other day for 3-5 sessions. For chronic conditions or maintenance, weekly or monthly sessions might be prescribed [1:9][9:5].
- Vascular Access: Adequate vascular access is crucial for TPE. This can be achieved through peripheral veins with large bore needles or, more commonly, through a central venous catheter, especially for repeated procedures or in patients with poor peripheral access [1:10].
¶ Dosage at a glance
| Use case | Typical dose/volume | Timing | Notes |
|---|---|---|---|
| Antibody-mediated neurological diseases (e.g., GBS, Myasthenia Gravis) | 1.0–1.5 PV per session | Every 24–48 h (3–5 sessions) | 5% albumin replacement; adjust per labs [1:11][5:2][9:6] |
| Hyperviscosity syndrome | 1.0 PV | Single or repeated as needed | Consider plasma if coagulopathy present [1:12] |
| Pediatric Sepsis/MODS | 1.0–1.5 PV per session | Daily or every other day | 5% albumin, careful monitoring due to pediatric specific risks [11:1][13:1] |
| Alzheimer’s (AMBAR experimental protocol) | Low-volume exchanges | Weekly→monthly per protocol | Albumin replacement ± IVIG; investigational, not standard care [14:1][15:1] |
| Familial Hypercholesterolemia (apheresis variants) | 1.0–1.5 PV | Weekly to bi-weekly | Specific lipoprotein apheresis techniques; not standard TPE [18:1] |
¶ Safety and Contraindications
While generally safe when performed by experienced medical teams, TPE is an invasive procedure with potential side effects and contraindications.