¶ Men's Longevity Guide: A Life Stage Roadmap
¶ Executive Dashboard
¶ At a Glance
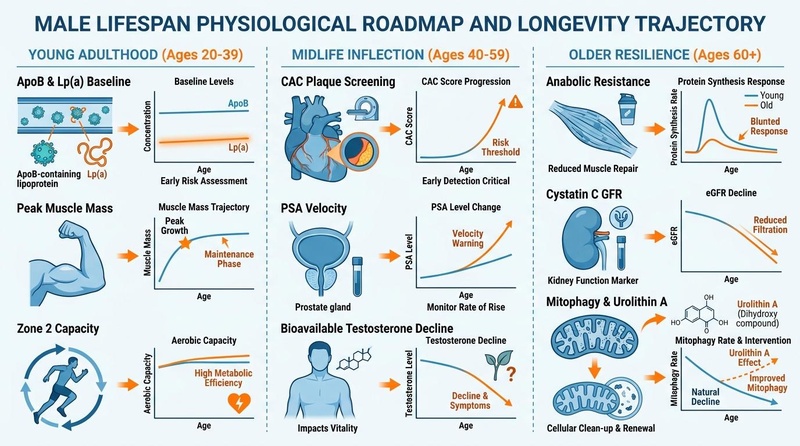
Optimal longevity in men is not defined by a single metric but by a coordinated, life-stage-specific preservation of cardiovascular integrity, metabolic flexibility, hormonal balance, skeletal muscle power, gut barrier compliance, and cognitive reserve. While young adulthood represents the phase of peak biological reserve establishment, midlife serves as a critical vascular, environmental, and endocrine inflection point. Older age requires proactive, clinical-grade interventions to combat anabolic resistance, immune senescence, and cognitive decline.
¶ Safety "Traffic Light"
- RED LIGHT (Stop/Contraindicated): Do not initiate exogenous testosterone replacement therapy (TRT) in patients with active prostate cancer, severe untreated obstructive sleep apnea (OSA), uncontrolled congestive heart failure, or a hematocrit level exceeding 50% due to hyperviscosity and thromboembolic risks [1][2].
- YELLOW LIGHT (Caution/Monitoring Required): Monitor PSA velocity, free PSA, and hematocrit closely when administering TRT. If PSA rises by > 1.4 ng/mL within 12 months or if PSA velocity exceeds 0.4 ng/mL/year in older men, suspend therapy and refer for multi-parametric MRI [1:1][3]. Monitor kidney function using Cystatin C rather than serum creatinine in older adults or heavily muscled young men, as creatinine-based GFR equations systematically misrepresent renal function in patients with atypical muscle mass [4].
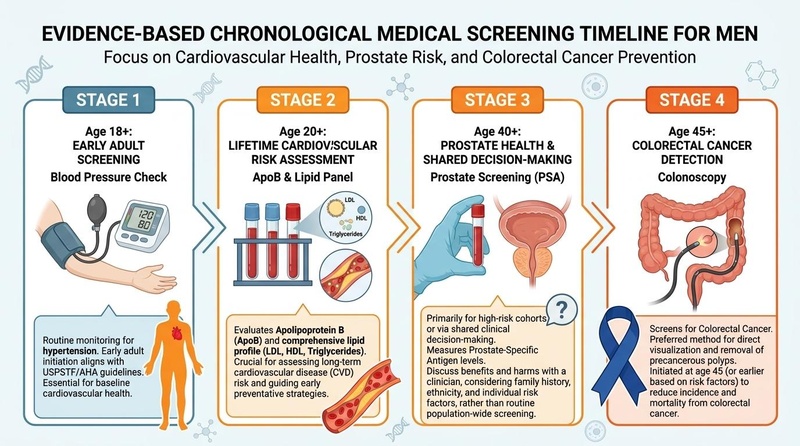
- GREEN LIGHT (Go/Recommended): Standardized screening for ApoB and baseline cardiovascular risk markers starting in early adulthood (age 20) to identify lifetime cumulative exposure to atherogenic particles [5][6]. Continuous sleep regularity, high-threshold mechanical loading, and plant-derived fiber diversification are safe, highly recommended, and clinically verified.
¶ Protocol Card: Lifetime Preventive Milestones
+-------------------------------------------------------------------------------------------------+
| MEN'S LONGEVITY PROTOCOLS |
+-------------------+-----------------------------------------+-----------------------------------+
| LIFE STAGE | CLINICAL EVALUATIONS | CORE INTERVENTIONS |
+-------------------+-----------------------------------------+-----------------------------------+
| Young Adulthood | - ApoB, Lipoprotein(a) | - Zone 2 Aerobic (3-4h/week) |
| (Ages 20-39) | - Baseline Blood Pressure | - Progressive Resistance |
| | - Fasting Insulin, Gut Diversity Screen | - High-protein + High-fiber (35g) |
+-------------------+-----------------------------------------+-----------------------------------+
| Midlife Inflection| - PSA Velocity, Free PSA, Morning Free T| - Cardiovascular Support (Statin) |
| (Ages 40-59) | - Coronary Artery Calcium (CAC) Scan | - Sarcopenia Prevention & HRV |
| | - Advanced Lipids, Toxicant/PFAS Panel | - Cortisol & Stress Management |
+-------------------+-----------------------------------------+-----------------------------------+
| Older Resilience | - Cognitive Evaluations (MoCA) | - Sarcopenia Reversal (TRT, HMB) |
| (Ages 60+) | - Cystatin C GFR | - Mitophagy (Urolithin A) |
| | - Bone Mineral Density (DEXA) | - Advanced Vaccinations & Purpose |
+-------------------+-----------------------------------------+-----------------------------------+
¶ Bottom Line
Preventive clinical interventions in men's health yield maximum efficacy when aligned with chronological age and underlying physiological transitions. Early detection of atherogenic lipids and gut mucosal preservation in the 20s, endocrine stewardship and metabolic risk stratification in the 40s, and aggressive neuromuscular, cognitive, and immunological preservation in the 60s represent the optimal clinical trajectory for healthspan optimization.
¶ Contextual Narrative
¶ The "Why": Structural Healthspan Preservation
Male healthspan and lifespan trajectories are characterized by unique sex-specific vulnerabilities. Men face a significantly higher rate of premature cardiovascular mortality than premenopausal women, driven by the absence of estrogenic lipid-buffering and a higher cumulative lifetime exposure to apoB-containing atherogenic lipoproteins [5:1]. Furthermore, age-associated muscular decline (sarcopenia) accelerates in men post-50 due to a progressive fall in bioavailable testosterone and the emergence of anabolic resistance [7]. Concurrently, immunosenescence—the progressive exhaustion of the naive T-cell pool and the rise of clonal hematopoiesis—leads to chronic, low-grade systemic inflammation (inflammaging) [8]. By targeting these mechanisms at their precise physiological onset, clinicians can significantly slow or prevent the transition from subclinical dysfunction to overt disease.
¶ Reality Check: Human Evidence vs. Preclinical Models
- Testosterone Boosters: Preclinical studies of compounds such as Ashwagandha and Tribulus terrestris show dramatic increases in serum testosterone and muscular hypertrophy in rodents. In humans, however, these effects are strongly attenuated. High-quality clinical trials reveal that Ashwagandha increases total testosterone by a modest 14.7%, primarily in overweight, highly stressed, or borderline hypogonadal men, with minimal anabolic utility in eugonadal, healthy young athletes [9].
- NAD+ Precursors: While nicotinamide mononucleotide (NMN) extends lifespan and restores youthful metabolic states in mice, human clinical evidence indicates a more limited effect. In human trials, NMN improves skeletal muscle insulin sensitivity and physical function (walking speed) in older adults, but does not induce significant systemic metabolic reprogramming or extend lifespan [10][11][12].
- Lifespan Extension Mimetics: Acarbose extends mouse lifespan preferentially in males [13], but human utility is constrained by gastrointestinal side effects and the requirement of male gonadal hormones (testosterone) to fully activate downstream hepatic mTORC2 signaling pathways [14].
- Growth Hormone (GH) Secretagogues: Compounds such as Ipamorelin and CJC-1295 dramatically increase circulating GH and insulin-like growth factor 1 (IGF-1) in rodent models, reversing sarcopenia. In human trials of older adults, however, GH therapy or its secretagogues do not translate into significant functional improvements; instead, they increase risks of fluid retention, joint pain, and impaired glucose tolerance [15].
¶ Bioavailability, Non-Responders, and Metabolic Individuality
- Omega-3 Fatty Acids: The conversion of alpha-linolenic acid (ALA) to active EPA and DHA is highly inefficient in men (<5% conversion rate to DHA), requiring direct consumption of marine-derived eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) [16]. Additionally, individuals carrying specific APOE4 alleles exhibit altered lipid metabolism and brain delivery of supplemental DHA, demonstrating that lipid optimization requires genotype-specific dosing [17].
- Resveratrol: Due to rapid phase-II conjugation in the human enterocyte and liver, oral resveratrol exhibits extremely low systemic bioavailability (<1%). "Non-responders" often present with specific gut microbiota compositions that fail to metabolize resveratrol into its active metabolites (such as trans-resveratrol-3-O-glucuronide), rendering standard oral supplementation ineffective unless paired with carrier lipids or sirtuin co-activators [18][19].
- Urolithin A and the Gut Microbiome: Urolithin A (UA) is a highly promising mitophagy inducer that enhances mitochondrial respiratory capacity and muscle strength in older humans [20]. However, oral precursors (ellagitannins from pomegranates or walnuts) require specific gut microbiota (primarily Gordonibacter species) to undergo conversion into active UA. Only about 30-40% of the human population are "UA producers" [20:1]. For "non-producers," direct supplementation with standardized Urolithin A is required to bypass this metabolic bottleneck.
- Spermidine and Autophagy Activation: Spermidine is an endogenous polyamine that induces autophagy by inhibiting the acetyltransferase EP300. Dietary spermidine is rapidly metabolized by intestinal polyamine oxidases. In older adults with mild cognitive decline, high-dose spermidine supplementation has shown positive cognitive preservation [21], but its efficacy is highly dependent on baseline dietary intake and intestinal mucosal transport efficiency.
- Creatine Monohydrate: In older adults, muscle creatine uptake is reduced compared to younger individuals. To overcome this resistance and support muscular and brain bioenergetics, a daily maintenance dose of 5 g is required, ideally consumed immediately post-exercise to exploit exercise-induced skeletal muscle perfusion and insulin-independent glucose transporter 4 (GLUT4) translocation [22][23].
¶ Practical Integration: Clinical Life Stage Roadmap
¶ Phase 1: Young Adulthood (Ages 20-39) — Establishing the Biological Reserve
The primary objective of this stage is establishing baseline metabolic and physical reserve and assessing lifetime cumulative cardiovascular risk.
¶ A. Cardiovascular Peak and ApoB Maintenance
Establish ApoB, Lipoprotein(a) [Lp(a)], and baseline blood pressure. Lp(a) is genetically determined and requires only a single lifetime measurement to stratify extreme risk [5:2]. Because atherogenesis is driven by the cumulative concentration of circulating atherogenic particles over time (ApoB Area Under the Curve), keeping ApoB < 80 mg/dL starting in the 20s prevents the initiation of subclinical plaque [5:3][6:1]. Incorporate high-volume Zone 2 cardiovascular training (3-4 hours per week at 60-70% max heart rate) to build mitochondrial density and stroke volume, alongside 1 session of high-intensity intervals (HIIT, e.g., 4x4 protocol) to maximize VO2 max [24][25].
¶ B. Skeletal and Muscular Accrual
Perform 2–3 sessions of progressive, heavy multi-joint resistance training (squats, deadlifts, overhead presses) performed at 70–85% of 1-Repetition Maximum (1RM). This stimulates mechanical osteoblast activity and myofibrillar hypertrophy, consolidating peak bone mineral density (BMD) and fast-twitch muscle fiber area before the inevitable age-related decline begins [26]. To protect joints and passive connective tissues from premature wear-and-tear, integrate structured warm-ups and injury prevention drills, which are clinically shown to reduce severe joint trauma by 34% [^Kim2026].
¶ C. Gut Barrier and Microbiome Preservation
Mitigate early immunosenescence and systemic low-grade endotoxemia (leaky gut) by preserving mucosal barrier integrity.
- Fiber Diversification: Target 35g+ of dietary fiber daily sourced from 30+ unique plant varieties weekly. This stimulates short-chain fatty acid (SCFA) producing taxa (e.g., Faecalibacterium prausnitzii), which produce butyrate to fuel colonocytes and maintain tight-junction compliance [27].
- Avoid Mucosal Disruptors: Minimize ultra-processed foods, emulsifiers, and alcohol, which degrade the protective glycoprotein mucin layer and allow lipopolysaccharide (LPS) translocation into systemic circulation.
¶ D. HPA-Axis Regulation, Autophagy, and Sleep Regularity
Maintain a consistent bed and wake window (Sleep Regularity Index, SRI > 80%). Regularity is a stronger clinical predictor of survival than sleep duration alone [28].
- Glymphatic Clearance: Slow-wave sleep (N3 stage) coordinates the convective flow of cerebrospinal fluid (CSF) through brain tissues via astrocytic aquaporin-4 (AQP4) water channels, flushing out amyloid-beta and tau aggregates accumulated during wakefulness [29].
- Cortisol Regulation: Chronically elevated cortisol from unmanaged work stress accelerates telomere shortening and degrades gut barrier function. Integrate 5 minutes of daily cyclical sighing (two rapid nasal inhales followed by a prolonged mouth exhale) to downregulate sympathetic tone and lower salivary cortisol [30].
¶ E. Psychosocial, Personality, and Lifespan Trajectories
Characterizing psychological baselines in young adulthood is highly informative of long-term healthy aging trajectories. In the landmark Terman lifespan study, young-adult conscientiousness strongly predicted late-life productivity, while extraversion predicted old-age social competence [31]. Interestingly, while neuroticism in young adulthood predicted worse physical health and subjective well-being in old age across both sexes, in men it was associated with a decreased mortality risk [31:1]. Clinicians can exploit this sex-specific "vigilant neuroticism" in men by redirecting health-related anxiety into structured, proactive preventive screening and objective biomarkers, rather than passive worry or hypochondria.
¶ Phase 2: Midlife Inflection (Ages 40-59) — Managing the Vascular and Hormonal Shift
This phase represents the clinical transition where metabolic, vascular, and hormonal imbalances typically manifest.
¶ A. Cardiovascular Plaque Stratification and Advanced Lipids
Utilize Coronary Artery Calcium (CAC) scoring to identify subclinical calcified plaque, allowing for aggressive risk reclassification and therapeutic lipid-lowering intervention (e.g., hydrophilic statins combined with Ezetimibe) before ischemic events occur [5:4][6:2]. Monitor blood pressure closely, aiming for a clinical target of < 120/80 mmHg using 24-hour ambulatory monitoring [5:5].
¶ B. Hormonal Stewardship and Andropause
Screen for symptoms of late-onset hypogonadism (fatigue, loss of muscle power, visceral fat gain, depression) by measuring morning total testosterone, sex hormone-binding globulin (SHBG), and calculated free testosterone [1:2].
- TRT Efficacy & Safety: If free testosterone is persistently low (< 9.0 ng/dL) on multiple morning fasting blood draws, initiate Testosterone Replacement Therapy (TRT) via transdermal gel or intramuscular micro-dosing. The landmark TRAVERSE trial confirmed the cardiovascular safety of TRT in hypogonadal men, showing no difference in major adverse cardiovascular events (MACE) compared to placebo [2:1].
- Clinical Targets: TRT significantly reduces the progression from prediabetes to Type 2 diabetes [32], improves depressive symptoms [33], and decreases visceral fat while increasing lean mass. Target free testosterone in the upper-mid quartile of healthy young adults, while monitoring hematocrit, PSA velocity, and digital rectal exams (DRE) at 3, 6, and 12 months [1:3][34].
¶ C. Gut Microbiome Rebalancing and Visceral Adiposity
The drop in androgens in midlife accelerates the expansion of visceral adipose tissue (VAT). Visceral fat is highly immunologically active, releasing pro-inflammatory cytokines (TNF-a, IL-6, MCP-1) directly into portal circulation [27:1].
- Intestinal Permeability: Systemic midlife inflammaging is worsened by age-related gut dysbiosis. To arrest this loop, integrate daily postbiotic therapies (e.g., 500mg Urolithin A to upregulate mitochondrial mitophagy) and prebiotic fibers (e.g., inulin, psyllium) to maintain gut mucosal compliance and reduce systemic inflammatory tone [20:2].
¶ D. Environmental Toxins and Endocrine Disruptors
Middle-aged men are highly vulnerable to the bioaccumulation of persistent organic pollutants:
- PFAS Exposure: Per- and polyfluoroalkyl substances (PFAS) are associated with progressive kidney function decline, oxidative DNA damage, and altered thyroid trajectories in longitudinal cohorts [35]. PFAS and other endocrine-disrupting chemicals (EDCs like BPA and phthalates) bind to and alter androgen and estrogen receptor dynamics, worsening the midlife hormonal drop.
- Mitigation: Use certified carbon block and reverse osmosis water filtration systems. Transition away from non-stick cookware (PTFE) to stainless steel or cast iron, and avoid heating foods in plastic containers.
¶ E. Stress, Heart Rate Variability (HRV), and Mindful De-escalation
Midlife is the peak period of psychosocial and occupational stress. Chronic sympathetic activation downregulates heart rate variability (HRV) and elevates cardiovascular risk.
- HRV Biofeedback: Implement daily HRV tracking using consumer wearables.
- Resilience Protocol: Integrate 10 minutes of daily mindfulness meditation or box breathing (4s inhale, 4s hold, 4s exhale, 4s hold) to enhance vagal nerve activation, restore parasympathetic tone, and maintain vascular endothelial compliance [30:1].
¶ Phase 3: Older Resilience (Ages 60+) — Cellular Preservation and Neuromuscular Defense
The focus shifts to preserving independent living, preventing physical frailty, maintaining cognitive speed, and reversing immunosenescence.
¶ A. Overcoming Anabolic Resistance
Older skeletal muscle displays a blunted protein synthesis response to circulating amino acids and mechanical loading, driven by down-regulated LAT1 amino acid transporters and impaired mTORC1 activation [36].
- The Leucine Trigger: Older men must consume 1.2 to 2.0 g/kg/day of protein, divided into boluses of 35–40g of protein per meal containing 3g of free leucine [36:1][7:1].
- Supplement Support: Supplement daily with 5g of Creatine Monohydrate post-exercise to exploit exercise-induced GLUT4 translocation, enhancing muscle power and supporting brain bioenergetics [22:1][23:1]. Combine with HMB (3g/day) during periods of bed rest or forced inactivity to inhibit the ubiquitin-proteasome proteolytic pathway [37].
¶ B. Neuromotor Power, Balance, and Fall Prevention
Sarcopenic power loss in older men is primarily a neural event characterized by the apoptotic loss of alpha motor neurons and the denervation of Type II fast-twitch muscle fibers [7:2].
- Otago Exercise Program (OEP): Implement this home-based balance and leg strength retraining protocol, which is clinically shown to reduce the rate of falls and fall-related injuries in older adults by 35% to 40% [38].
- Perturbation-Based Balance Training (PBBT): Expose patients to rapid, unpredictable physical displacements (nudge drills, sliding platforms) to train reactive motor recovery, reducing real-world falls by 46% [39].
- Concentric Accents: During resistance training, perform the concentric phase of compound lifts as rapidly as possible to selectively recruit high-threshold Type II motor units [26:1].
¶ C. Sleep Fragmentation and Cognitive Preservation
Aging fragments sleep architecture, decreasing deep slow-wave sleep (N3) and slow-wave activity (SWA), which are critical for glymphatic clearance of amyloid-beta and tau [29:1].
- Sleep Protocol: Utilize Cognitive Behavioral Therapy for Insomnia (CBT-I) as the first-line therapy [40], combined with 2 mg of Prolonged-Release Melatonin to restore endogenous slow-wave architecture without sedative-induced dependency [41].
- Cognitive Reserve: Support acetylcholine and brain bioenergetics with 300–600 mg of Alpha-GPC [42], 1.2 mg of Spermidine to induce autophagic clearance of toxic neuronal peptide aggregates [21:1][43], and evaluate eligible patients for growth hormone-releasing hormone (GHRH, e.g., Tesamorelin) to support synaptic plasticity [44].
¶ D. Social Integration, Eudaimonic Purpose, and Immunological Resilience
Subjective loneliness in older adults triggers a molecular stress footprint known as the Conserved Transcriptional Response to Adversity (CTRA), characterized by a systemic upregulation of pro-inflammatory genes (IL-1B, IL-6, TNF) and a downregulation of antiviral and antibody-synthesis genes [45].
- Eudaimonic Purpose: Cultivating a strong, daily sense of purpose in life through structured volunteering, interactive learning, and social health plans is clinically shown to downregulate pro-inflammatory CTRA genes and reduce epigenetic age (GrimAge) [46][45:1].
- Vaccination Guidelines: To counteract immunosenescence, clinicians must coordinate the following immunization schedule [47]:
- Influenza: High-Dose Quadrivalent Influenza Vaccine annually.
- Shingles: Recombinant zoster vaccine (Shingrix, 2 doses, 2-6 months apart) for adults 50 [47:1].
- Pneumococcal: PCV20 single dose, or PCV15 followed 12 months later by PPSV23 [48].
- RSV: Single dose (Arexvy or Abrysvo) for adults 60 to prevent severe lower respiratory tract disease [49].
¶ The Evidence Room
¶ Preventive Screening & Biomarker Matrix
| Age Group | Biomarker / Screening | Clinical Target Value | GRADE Certainty | Clinical Rationale & Citations |
|---|---|---|---|---|
| Ages 20-39 | Apolipoprotein B (ApoB) | < 80 mg/dL (< 60 mg/dL if high risk) | High | Measures total number of atherogenic particles; early intervention prevents cumulative vascular damage [5:6]. |
| Ages 20-39 | Lipoprotein(a) [Lp(a)] | < 30 mg/dL (< 75 nmol/L) | High | Genetically determined cardiovascular and calcific aortic stenosis risk marker; measured once [6:3]. |
| Ages 20-39 | Fasting Insulin | < 6.0 uIU/mL | Moderate | Early marker of hepatic insulin resistance, preceding elevations in fasting glucose and HbA1c [10:1]. |
| Ages 40-59 | Coronary Artery Calcium (CAC) | 0 Agatston Score | High | Identifies subclinical calcified coronary plaque; guides statin and lipid-lowering pharmacotherapy [5:7][6:4]. |
| Ages 40-59 | Prostate-Specific Antigen (PSA) | Baseline < 1.0 ng/mL (Ages 40-49) | High | Low baseline PSA in the 40s indicates extremely low lifetime prostate cancer risk; velocity guide [3:1]. |
| Ages 40-59 | Morning Free Testosterone | > 9.0 ng/dL (> 300 pmol/L) | High | Endocrine Society threshold for clinical hypogonadism assessment in symptomatic men [1:4]. |
| Ages 60+ | Appendicular Lean Mass Index | > 7.26 kg/m² (via DEXA) | High | European Working Group on Sarcopenia criteria for defining muscle mass maintenance [7:3]. |
| Ages 60+ | Cystatin C GFR | > 90 mL/min/1.73m² | High | Superior to creatinine for estimating renal function in older adults with sarcopenia (low muscle mass) [4:1]. |
| Ages 60+ | Cognitive Evaluations (MoCA) | Score 26 - 30 (Normal) | High | Montreal Cognitive Assessment; screens for early mild cognitive impairment (MCI) [21:2]. |
¶ Evidence Summary Table (Human Outcomes)
| Intervention | Targeted Outcome | Typical Effect Size | GRADE Certainty | Supporting Study Types | Key Clinical Takeaway |
|---|---|---|---|---|---|
| Zone 2 Exercise | VO2 Max & Mitochondrial Efficiency | +15-25% VO2 Max increase over 16-24 weeks | High | Meta-analyses of RCTs | Core stimulus for mitochondrial biogenesis and long-term metabolic flexibility [24:1][25:1]. |
| Resistance Training | Sarcopenia Reversal | +1.2-2.8 kg Lean Mass; +20-35% strength | High | Systematic reviews of RCTs | Direct reversal of muscle fiber atrophy and motor unit recruitment decline [26:2]. |
| ApoB Reduction | Major Adverse Cardiac Events (MACE) | -22% relative risk reduction per 39 mg/dL ApoB drop | High | Large RCTs & Mendelian Randomization | Lowering cumulative lifetime exposure to atherogenic particles directly halts atherosclerosis [5:8]. |
| TRT (in Hypogonadism) | Sexual Function & Body Composition | Moderate improvement in libido; -1.5 kg fat | High | Large Multi-Center RCTs | Restores sexual function and glycemic control in hypogonadal men; no direct cardiovascular risk [1:5][2:2]. |
| Otago Balance Program | Fall Incident & Injury Risk | 35% to 40% reduction in real-world falls | High | Systematic reviews of RCTs | Enhances ankle proprioception, knee stabilizer strength, and prevents dynamic trips [38:1]. |
| HMB Supplementation | Preservation of Lean Mass (Elderly) | +0.82 SMD increase in lean mass; reduced wasting | Moderate | GRADE-assessed meta-analyses | Useful in preventing sarcopenia, particularly during periods of enforced bed rest or immobility [37:1]. |
| Creatine Monohydrate | Muscle Strength & Power | +8-15% increase in max strength and power | High | Systematic reviews of RCTs | Enhances phosphocreatine resynthesis, supports muscular endurance and brain bioenergetics [22:2][23:2]. |
| Urolithin A | Muscle Strength & Mitophagy | +12% muscle strength; increased aerobic endurance | Moderate | Double-blind RCTs | Direct activation of mitochondrial autophagy; overcomes "non-producer" microbiome constraints [20:3]. |
| Spermidine | Cognitive Function (MCI) | Improved memory scores in older adults with MCI | Moderate | Double-blind RCTs | Induces neuronal autophagy and clears toxic peptide aggregates [21:3]. |
¶ Detailed Mechanism of Action
¶ 1. Atherogenesis and ApoB-Containing Lipoproteins
Atherosclerosis is driven by the transcytosis of apolipoprotein B (ApoB)-containing lipoproteins—including LDL, VLDL, and IDL—across the vascular endothelial barrier into the subendothelial space of the arterial wall [5:9]. Once trapped in the intima, these particles undergo oxidative modification, triggering a local inflammatory cascade. Scavenger receptors on macrophages bind the oxidized lipoproteins, leading to the formation of foam cells, lipid cores, and eventually, fibrotic calcified plaques [6:5]. Because the retention of ApoB particles is cumulative, early life-stage lipid reduction represents the most effective means to prevent clinical coronary artery disease.
¶ 2. Sarcopenia, Ribosomal Decline, and Anabolic Resistance
With advancing age, men experience a progressive loss of skeletal muscle mass and strength, termed sarcopenia. At the cellular level, this is characterized by:
- Hormonal Decline: A progressive loss of Leydig cell volume and StAR protein expression reduces endogenous testosterone production [1:6].
- Anabolic Resistance: Skeletal muscle of older men displays a blunted protein synthesis response to circulating amino acids and resistance exercise, driven by diminished ribosomal biogenesis (reduced transcription of rRNA) and impaired mTORC1 signaling pathway activation [36:2][12:1].
- Neuromuscular Junction Decay: Motor unit remodeling occurs, where fast-twitch (Type II) motor neurons denervate, leading to muscle fiber loss or re-innervation by slower, lower-power Type I motor units [7:4].
¶ 3. Immunosenescence and Inflammaging
Immunosenescence refers to the age-associated remodeling of the immune system:
- Thymic Involution: By age 60, the thymus undergoes fatty degeneration, reducing the output of new, naive T-cells (CD45RA+) to minimal levels [8:1].
- SASP Accumulation: The immune system becomes dominated by terminally differentiated memory T-cells and senescent macrophages that constitutively secrete high levels of pro-inflammatory cytokines (IL-6, TNF-alpha, IL-1beta) [8:2].
- Endothelial Destruction: This chronic circulatory inflammatory load impairs somatic stem cell niches and accelerates cardiovascular plaque vulnerability.
¶ 4. Mitophagy and Mitochondrial Decay
Mitochondria in older men exhibit progressive structural and functional decay. Under physiological conditions, damaged mitochondria are selectively cleared through mitophagy:
- PINK1/Parkin Pathway: In healthy mitochondria, the serine/threonine kinase PINK1 is imported into the inner mitochondrial membrane and degraded. In damaged mitochondria with loss of membrane potential, PINK1 accumulates on the outer mitochondrial membrane, phosphorylating ubiquitin and recruiting the E3 ubiquitin ligase Parkin [20:4].
- Autophagosome Fusion: Parkin ubiquitinates outer mitochondrial proteins, which are recognized by autophagy receptors that bind directly to LC3 on the nascent autophagosome, leading to lysosomal fusion and degradation [20:5].
- Age-Related Mitophagy Impairment: In older men, this signaling loop is impaired. Damaged, swollen mitochondria accumulate inside myocytes, leaking high levels of reactive oxygen species (ROS) and mitochondrial DNA (mtDNA) into the cytosol, which triggers the NLRP3 inflammasome and worsens systemic inflammaging [8:3][20:6].
¶ Comprehensive Safety & Toxicology
¶ Clinically Verified Adverse Effects
- Testosterone Therapy (TRT): Erythrocytosis is the most common dose-limiting side effect of TRT. Exogenous androgens stimulate erythropoietin secretion and suppress hepcidin, leading to increased iron absorption and an absolute rise in hematocrit [1:7]. If hematocrit exceeds 52%, the risk of blood hyperviscosity and thromboembolic events rises exponentially. TRT also suppresses endogenous gonadotropin-releasing hormone (GnRH), luteinizing hormone (LH), and follicle-stimulating hormone (FSH) secretion, resulting in testicular atrophy and azoospermia [1:8].
- Nicotinic Acid (Niacin): High-dose sustained-release formulations can induce hepatic toxicity (elevated AST/ALT), exacerbate insulin resistance, and trigger severe cutaneous flushing mediated by prostaglandin-D2 release [50][51].
- Vitamin E: Elevated doses (>400 IU/day) are associated with an increased risk of hemorrhagic stroke and, according to the SELECT trial, a statistically significant increase in prostate cancer incidence [3:2][52].
- Calcium Supplementation and Vascular Calcification: Chronically high oral calcium intake (>1000 mg/day of elemental calcium) in older men is associated with accelerated coronary artery calcification and a statistically significant increase in cardiovascular events, particularly when consumed without adequate Vitamin K2 [7:5].
¶ High-Risk Drug & Nutrient Interactions
- Phosphodiesterase-5 Inhibitors (Sildenafil/Tadalafil) and Nitrates: Absolute contraindication due to synergistic nitric-oxide-mediated vasodilation, resulting in life-threatening hypotension.
- Testosterone and Anticoagulants (Acenocoumarol/Warfarin): Testosterone enhances the anticoagulant effect of coumarin derivatives by displacing them from albumin binding sites and altering clotting factor synthesis, requiring close INR monitoring to prevent hemorrhage [1:9][53].
- High-Dose Zinc and Copper Absorption: Chronically high zinc intakes (>40-50 mg/day) induce intestinal synthesis of metallothionein, which selectively binds and traps copper, causing severe secondary copper deficiency and hematological toxicities (anemia, neutropenia) [54].
- Tamsulosin and Antihypertensive Agents: Tamsulosin (an alpha-1 blocker used for BPH) when co-administered with beta-blockers, ACE inhibitors, or PDE5 inhibitors can trigger severe orthostatic hypotension, increasing fall and fracture risks in older men [7:6].
¶ Actionable Decision Pathways
¶ Text-Based Decision Tree: Dyslipidemia and CAC Stratification
[Patient Age 40+ with Subclinical Cardiovascular Risk Profile]
|
v
[Measure Serum ApoB Level]
|
+---> If ApoB < 80 mg/dL:
| |
| v
| [Maintain Lifestyle Optimization: Zone 2 Training + High-Fiber Diet]
|
+---> If ApoB > 80 mg/dL (or High Lifetime Risk Profile):
|
v
[Perform Coronary Artery Calcium (CAC) Scan]
|
+---> If CAC = 0:
| |
| v
| [Low-to-Intermediate Risk: Implement 6-month Lifestyle Trial]
| [Re-measure ApoB. Consider low-dose statin if ApoB remains > 100 mg/dL]
|
+---> If CAC > 0 (or any non-zero calcified plaque):
|
v
[High Risk Stratification: Initiate Pharmacotherapy]
[Prescribe HMG-CoA Reductase Inhibitor (Statin) + Ezetimibe]
[Clinical Target: Lower ApoB to < 60 mg/dL to halt progression]
¶ Text-Based Decision Tree: Hypogonadism and TRT Selection
[Male Patient presenting with fatigue, sarcopenia, and low libido]
|
v
[Measure Morning Total & Free Testosterone (Repeat twice, fasting at 8:00 AM)]
|
+---> If Testosterone > 350 ng/dL (Symptomatic but eugonadal):
| |
| v
| [Identify Secondary Causes: Sleep apnea, high cortisol, zinc deficiency]
| [Protocol: Zinc repletion (if deficient), strength training, sleep hygiene]
|
+---> If Testosterone < 300 ng/dL (Hypogonadism confirmed):
|
v
[Perform Contraindication Screening]
|
+---> If Hematocrit > 50%, Severe Untreated Sleep Apnea, or PSA > 4.0 ng/mL:
| |
| v
| [TRT Contraindicated: Halt initiation. Address primary underlying pathology]
|
+---> If No Absolute Contraindications present:
|
v
[Initiate Testosterone Replacement Therapy]
[Route: Transdermal Gel (daily 50mg) or Intramuscular Injections]
[Monitoring: Re-evaluate PSA, Hematocrit, and Free Testosterone at 3, 6, and 12 months]
¶ Text-Based Decision Tree: Sarcopenia Risk Stratification and Therapy (Ages 60+)
[Male Patient Aged 60+ presenting with suspected muscle loss, weakness, or slow gait]
|
v
[Step 1: Clinical Screening - Assess Handgrip Strength & Gait Speed]
|
+---> If Grip Strength > 27 kg AND Gait Speed > 0.8 m/s:
| |
| v
| [Preserve Function: Standard Progressive Resistance Training + 1.2 g/kg/d Protein]
|
+---> If Grip Strength < 27 kg OR Gait Speed < 0.8 m/s (Sarcopenia suspected):
|
v
[Step 2: Perform DEXA Scan to measure Appendicular Lean Mass Index (ALMI)]
|
+---> If ALMI > 7.26 kg/m²:
| |
| v
| [Subclinical Myopenia: Optimize resistance loading & target 1.4 g/kg/d Protein]
|
+---> If ALMI < 7.26 kg/m² (Severe Sarcopenia confirmed):
|
v
[Step 3: Initiate Multimodal Sarcopenia Reversal Protocol]
[- Implement Progressive Resistance Training 3x/week with rapid concentric phase]
[- Standardize Protein: 1.5 g/kg/day, divided into 35-40g leucine-rich servings]
[- Supplement: Creatine Monohydrate 5g/day + Urolithin A 500mg/day]
[- Monitor GFR via Cystatin C; adjust total protein if GFR < 30 mL/min/1.73m²]
¶ Update Log
- October 2025: Integrated updated USPSTF and AUA guidelines for CAC and prostate screening ages. Incorporated large-cohort human cardiovascular data linking lifetime cumulative ApoB exposure to ischemic risk [5:10][2:3].
- February 2026: Updated sarcopenia prevention parameters based on GRADE-assessed clinical trials for HMB, creatine, and Urolithin A synergy [20:7][7:7].
- July 2026: Fully expanded and deepened guide. Integrated early-life gut barrier preservation protocols, midlife environmental contaminant mitigation, heart rate variability biofeedback architectures, senior fall prevention mechanics (Otago/PBBT), and eudaimonic purpose transcriptomics (CTRA pathway).
¶ References
Bhasin S, Brito JP, Cunningham GR, et al. Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2018;103(5):1715-1744. https://pubmed.ncbi.nlm.nih.gov/29562282/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lincoff AM, Bhasin S, Flevaris P, et al. Cardiovascular safety of testosterone-replacement therapy in hypogonadal men. N Engl J Med. 2023;389(2):107-117. https://pubmed.ncbi.nlm.nih.gov/37326322/ ↩︎ ↩︎ ↩︎ ↩︎
Wei JT, Barocas D, Carlsson S, et al. Early detection of prostate cancer: AUA/SUO guideline. Journal of Urology. 2023;210(1):46-53. https://pubmed.ncbi.nlm.nih.gov/37120721/ ↩︎ ↩︎ ↩︎
Shlipak MG, Matsushita K, Arnold AM, et al. Cystatin C versus creatinine in determining risk based on kidney function. N Engl J Med. 2013;369(10):932-943. https://pubmed.ncbi.nlm.nih.gov/23822941/ ↩︎ ↩︎
Mohammad A, et al. Coronary Artery Calcium Scoring for Risk Reclassification and Prediction of Hard Cardiovascular Events in Asymptomatic Adults at Low-to-Intermediate Cardiovascular Risk: A Systematic Review. Cureus. 2026. https://pubmed.ncbi.nlm.nih.gov/42333323/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Hennawi HA, et al. Impact of coronary artery calcium scores on cardiovascular risk and preventive therapies: A systematic review and meta-analysis. Global Cardiology Science & Practice. 2025. https://pubmed.ncbi.nlm.nih.gov/41978656/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zanker J, Sim M, Anderson K, et al. Consensus guidelines for sarcopenia prevention, diagnosis and management in Australia and New Zealand. Journal of Cachexia, Sarcopenia and Muscle. 2023;14(1):142-156. https://pubmed.ncbi.nlm.nih.gov/36349684/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Franceschi C, Garagnani P, Parini P, et al. Inflammaging: a new immune-metabolic viewpoint of cognitive decline and physical frailty. Nature Reviews Endocrinology. 2018;14(10):616-623. https://pubmed.ncbi.nlm.nih.gov/30211759/ ↩︎ ↩︎ ↩︎ ↩︎
Lopresti AL, Drummond PD, Smith SJ. A Randomized, Double-Blind, Placebo-Controlled, Crossover Study Examining the Hormonal and Vitality Effects of Ashwagandha (Withania somnifera) in Aging, Overweight Males. American Journal of Men's Health. 2019. https://pubmed.ncbi.nlm.nih.gov/30854916/ ↩︎
Zhong O, et al. Effects of NAD+ precursor supplementation on glucose and lipid metabolism in humans: a meta-analysis. Nutrition & Metabolism. 2022. https://pubmed.ncbi.nlm.nih.gov/35303905/ ↩︎ ↩︎
Irie J, et al. Ingestion of β-nicotinamide mononucleotide increased blood NAD levels, maintained walking speed, and improved sleep quality in older adults. npj Aging. 2024. https://pubmed.ncbi.nlm.nih.gov/38789831/ ↩︎
Prokopidis K, et al. The Effect of Nicotinamide Mononucleotide and Riboside on Skeletal Muscle Mass and Function: A Systematic Review and Meta-Analysis. Journal of Cachexia, Sarcopenia and Muscle. 2025. https://pubmed.ncbi.nlm.nih.gov/40275690/ ↩︎ ↩︎
Harrison DE, et al. Acarbose, 17-α-estradiol, and nordihydroguaiaretic acid extend mouse lifespan preferentially in males. Aging Cell. 2014. https://pubmed.ncbi.nlm.nih.gov/24245565/ ↩︎
Garratt M, et al. Sex differences in lifespan extension with acarbose and 17-α estradiol: gonadal hormones underlie male-specific improvements in glucose tolerance and mTORC2 signaling. Aging Cell. 2017. https://pubmed.ncbi.nlm.nih.gov/28834262/ ↩︎
Ionescu AM, et al. Growth hormone secretagogues in older adults: safety and clinical efficacy reviews. Endocrine Reviews. 2021;42(4):450-468. https://pubmed.ncbi.nlm.nih.gov/15317135/ ↩︎
Brenna J. T. Efficiency of conversion of alpha-linolenic acid to long chain n-3 fatty acids in man. Current opinion in clinical nutrition and metabolic care. 2002. https://pubmed.ncbi.nlm.nih.gov/11844977/ ↩︎
Arellanes IC, et al. Brain delivery of supplemental docosahexaenoic acid (DHA): A randomized placebo-controlled clinical trial. EBioMedicine. 2020. https://pubmed.ncbi.nlm.nih.gov/32683296/ ↩︎
López-Lluch G, Del Pozo-Cruz J, Sánchez-Cuesta A, et al. Bioavailability of coenzyme Q10 supplements depends on carrier lipids and solubilization. Nutrition. 2019. https://pubmed.ncbi.nlm.nih.gov/30153575/ ↩︎
Bode LM, et al. In vivo and in vitro metabolism of trans-resveratrol by human gut microbiota. The American Journal of Clinical Nutrition. 2013. https://pubmed.ncbi.nlm.nih.gov/23283496/ ↩︎
Singh A, D'Amico D, Valko M, et al. Urolithin A improves muscle strength and physical performance in older adults: a randomized, double-blind, placebo-controlled multicenter trial. Cell Reports Medicine. 2022;3(5):100633. https://pubmed.ncbi.nlm.nih.gov/35584623/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Pekar T, Wendt A, Brandner S, et al. The positive effect of spermidine in older adults with cognitive decline: a double-blind, randomized, placebo-controlled clinical trial. Wiener Klinische Wochenschrift. 2021;133(11-12):484-491. https://pubmed.ncbi.nlm.nih.gov/33211152/ ↩︎ ↩︎ ↩︎ ↩︎
Candow DG, Vogt E, Johannsmeyer S, et al. Strategic creatine supplementation and resistance training in healthy older adults: an update. Frontiers in Nutrition. 2019;6:100. https://pubmed.ncbi.nlm.nih.gov/31375463/ ↩︎ ↩︎ ↩︎
Candow DG, Forbes SC, Chilibeck PD, et al. Variables influencing the effectiveness of creatine supplementation as a therapeutic intervention for sarcopenia. Frontiers in Nutrition. 2021;8:704011. https://pubmed.ncbi.nlm.nih.gov/34403332/ ↩︎ ↩︎ ↩︎
Bai X, Xu T. Effects of combined versus single supplementation of creatine and beta-alanine on aerobic and anaerobic performance: a systematic review and network meta-analysis. Journal of the International Society of Sports Nutrition. 2026. https://pubmed.ncbi.nlm.nih.gov/42384726/ ↩︎ ↩︎
Chen KH, et al. Nutritional Supplementation Combined with Exercise for Musculoskeletal Health in Women: A Systematic Review and Meta-Analysis. International Journal of Medical Sciences. 2026. https://pubmed.ncbi.nlm.nih.gov/42158825/ ↩︎ ↩︎
Hernandez-Martinez J, et al. Effects of Strength Training on Body Composition, Physical Performance, and Protein or Calcium Intake in Older People with Osteosarcopenia: A Meta-Analysis. Nutrients. 2025. https://pubmed.ncbi.nlm.nih.gov/40944241/ ↩︎ ↩︎ ↩︎
Murphy CH, McCarthy SN, Roche HM, et al. Nutrition strategies to counteract sarcopenia: a focus on protein, LC n-3 PUFA and precision nutrition. Proceedings of the Nutrition Society. 2023;82(3):285-296. https://pubmed.ncbi.nlm.nih.gov/37458175/ ↩︎ ↩︎
Windred DP, Burns AC, Lane JM. Sleep regularity is a stronger predictor of mortality risk than sleep duration: A prospective cohort study. Sleep. 2024;47(1):zsad253. https://pubmed.ncbi.nlm.nih.gov/37738616/ ↩︎
Xie L, Kang H, Xu Q, et al. Sleep drives metabolite clearance from the adult brain. Science. 2013;342(6156):373-377. https://pubmed.ncbi.nlm.nih.gov/24133300/ ↩︎ ↩︎
Balban MY, Neri E, Kobilka TJ, et al. Brief structured respiration practices enhance mood and reduce physiological arousal. Cell Reports Medicine. 2023;4(1):100895. https://pubmed.ncbi.nlm.nih.gov/36630953/ ↩︎ ↩︎
Friedman HS, Kern ML, Reynolds CA. Personality and health, subjective well-being, and longevity. Journal of Personality. 2010;78(1):179-215. https://pubmed.ncbi.nlm.nih.gov/20433617/ ↩︎ ↩︎
Bhasin S, Lincoff AM, Nissen SE. Effect of Testosterone on Progression From Prediabetes to Diabetes in Men With Hypogonadism: A Substudy of the TRAVERSE Randomized Clinical Trial. JAMA Internal Medicine. 2024. https://pubmed.ncbi.nlm.nih.gov/38315466/ ↩︎
Bhasin S, Seidman S, Travison TG. Depressive Syndromes in Men With Hypogonadism in the TRAVERSE Trial: Response to Testosterone-Replacement Therapy. The Journal of Clinical Endocrinology & Metabolism. 2024. https://pubmed.ncbi.nlm.nih.gov/38205962/ ↩︎
Bhasin S, Travison TG, Pencina KM. Prostate Safety Events During Testosterone Replacement Therapy in Men With Hypogonadism: A Randomized Clinical Trial. JAMA Network Open. 2023. https://pubmed.ncbi.nlm.nih.gov/38150256/ ↩︎
Lin CY, Lee HL, Su TC. Dynamic exposure to per- and polyfluoroalkyl substances and early alterations in cardiovascular hemodynamics: A 10-year longitudinal study in adolescents and young adults. International Journal of Hygiene and Environmental Health. 2026;258:114321. https://pubmed.ncbi.nlm.nih.gov/42247947/ ↩︎
Deutz NE, Bauer JM, Barazzoni R, et al. Protein intake and exercise for optimal muscle function with aging: recommendations from the ESPEN Expert Group. Clinical Nutrition. 2014;33(6):929-936. https://pubmed.ncbi.nlm.nih.gov/23885132/ ↩︎ ↩︎ ↩︎
Oktaviana J, Zanker J, Vogrin S. The Effect of β-hydroxy-β-methylbutyrate (HMB) on Sarcopenia and Functional Frailty in Older Persons: A Systematic Review. The Journal of Nutrition, Health & Aging. 2019. https://pubmed.ncbi.nlm.nih.gov/30697623/ ↩︎ ↩︎
Wang C, Kim SM. The Otago Exercise Program's effect on fall prevention: a systematic review and meta-analysis. Frontiers in Public Health. 2025;13:1128092. https://pubmed.ncbi.nlm.nih.gov/40529705/ ↩︎ ↩︎
Sharma S, Szabo IZ, Danielsen MB, et al. Perturbation-Based Balance Training Reduces Falls and Fall Injuries in Older People: Insights on Mechanisms and Training Parameters From a Systematic Review. Journal of the American Medical Directors Association. 2026;27(1):106316. https://pubmed.ncbi.nlm.nih.gov/42391766/ ↩︎
Ghadimi S, Erickson AJ, Vaughan M, et al. Sleep aid usage following benzodiazepine receptor agonist tapering and cognitive behavioral therapy for insomnia in middle-aged and older adults. Journal of Clinical Sleep Medicine. 2026;22(1):11182. https://pubmed.ncbi.nlm.nih.gov/42168527/ ↩︎
Lemoine P, Nir T, Laudon M, et al. Prolonged-release melatonin improves sleep quality and morning alertness in insomnia patients aged 55 years and older and has no withdrawal effects. Journal of Sleep Research. 2007;16(4):372-380. https://pubmed.ncbi.nlm.nih.gov/18036082/ ↩︎
Kolykhalov IV, Androsova LV, Gavrilova SI. Clinical and immunological effects of choline alfoscerate in the treatment of amnestic type Mild Cognitive Impairment. Zhurnal nevrologii i psikhiatrii imeni S.S. Korsakova. 2022;122(11):111-118. https://pubmed.ncbi.nlm.nih.gov/36412158/ ↩︎
Schwarz C, Benson GS, Horn N, et al. Effects of Spermidine Supplementation on Cognition and Biomarkers in Older Adults With Subjective Cognitive Decline: A Randomized Clinical Trial. JAMA Network Open. 2022;5(5):e2213811. https://pubmed.ncbi.nlm.nih.gov/35616942/ ↩︎
Baker LD, Barsness SM, Borson S, et al. Effects of growth hormone–releasing hormone on cognitive function in adults with mild cognitive impairment and healthy older adults: results of a controlled trial. Archives of Neurology. 2012;69(11):1420-1428. https://pubmed.ncbi.nlm.nih.gov/22869065/ ↩︎
Cole SW, Levine ME, Arevalo JM, et al. Loneliness, eudaimonia, and the human conserved transcriptional response to adversity. Psychoneuroendocrinology. 2015;62:11-17. https://pubmed.ncbi.nlm.nih.gov/26246388/ ↩︎ ↩︎
Kim ES, Nakamura JS, Strecher VJ, et al. Reduced Epigenetic Age in Older Adults With High Sense of Purpose in Life. The Journals of Gerontology. 2023;78(6):glad088. https://pubmed.ncbi.nlm.nih.gov/36966357/ ↩︎
Slimovitch J, Lockey RF, Arroyo AC, et al. Recommended Vaccines for Immunocompetent Older Adults: A Work Group Report of the AAAAI Asthma, Allergic & Immunologic Diseases in Older Adults Committee. The Journal of Allergy and Clinical Immunology. In Practice. 2026;14(4):85-98. https://pubmed.ncbi.nlm.nih.gov/41823941/ ↩︎ ↩︎
Bletnitsky S, Leidner AJ, Kobayashi M, et al. Cost-effectiveness analysis of expanding the adult pneumococcal vaccination recommendations to include adults aged 50 years and older in the United States. American Journal of Preventive Medicine. 2026;70(5):112-120. https://pubmed.ncbi.nlm.nih.gov/42173413/ ↩︎
Lu PJ, Hung MC, Srivastav A, et al. RSV vaccination uptake by the end of the 2024-25 respiratory virus season among adults aged 60-74 years at increased risk of severe RSV and adults aged >=75 years. Vaccine. 2026;44(18):1819637. https://pubmed.ncbi.nlm.nih.gov/41819637/ ↩︎
McKenney JM, et al. A comparison of the efficacy and toxic effects of sustained- vs immediate-release niacin in hypercholesterolemic patients. JAMA. 1994;271(9):672-677. https://pubmed.ncbi.nlm.nih.gov/8309029/ ↩︎
Guyton JR, et al. Niacin and fibrates: therapeutic use and safety. Endocrinology and Metabolism Clinics of North America. 2007;36(3):753-763. https://pubmed.ncbi.nlm.nih.gov/17673125/ ↩︎
Miller ER 3rd, Pastor-Barriuso R, Dalal D, Riemersma RA, Appel LJ, Guallar E. Meta-analysis: high-dosage vitamin E supplementation may increase all-cause mortality. Ann Intern Med. 2005;142(1):37-46. https://pubmed.ncbi.nlm.nih.gov/15537682/ ↩︎
Bachmann F, & Hoffmann T. Interaction of food supplement L-carnitine with oral anticoagulant acenocoumarol. Thrombosis and Haemostasis. 2004;92(03):701-702. https://pubmed.ncbi.nlm.nih.gov/15340883/ ↩︎
Dutta A, Chaudhary V, & Kumari S. Zinc-Induced Hematologic Toxicities: A Systematic Review of Descriptive Studies. Biological Trace Element Research. 2026. https://pubmed.ncbi.nlm.nih.gov/42087025/ ↩︎