¶ Middle-Aged Adult Longevity Guide
¶ Overview
Midlife (chronological ages 40–65) represents a critical physiological pivot. During this period, subclinical molecular damage begins to manifest as measurable clinical decline across multiple organ systems. Hormonal axes undergo significant remodeling, metabolic flexibility decreases, cardiovascular risk accelerates, and sarcopenic muscle loss initiates.
For the longevity clinician and advanced practitioner, middle age is the primary window for aggressive secondary and primary prevention. Intervening during this transitional phase can decelerate the biological aging rate, preserving organ system reserve and extending overall healthspan. Furthermore, active occupational and social engagement during this transitional phase has been shown to support positive psychosocial value orientations, which are critical for sustaining active longevity patterns [1]. This guide outlines the physiological shifts of midlife and provides structured, evidence-based pathways to optimize cardiovascular, metabolic, hormonal, and musculoskeletal health.
| Parameter | Clinical Target & Strategy |
|---|---|
| Primary Focus | Early detection of subclinical atherosclerosis, preservation of skeletal muscle mass, and hormonal stability |
| Cardiovascular Targets | ApoB < 70 mg/dL (or < 55 mg/dL if high risk)[2], Blood Pressure < 120/80 mmHg[3], CAC score = 0[4] |
| Metabolic Targets | HbA1c < 5.4%, fasting insulin < 6 μIU/mL, HOMA-IR < 1.0[5] |
| Musculoskeletal Targets | Muscle mass index (SMI) > 10.75 kg/m² (men), > 6.75 kg/m² (women)[6]; VO2 max in top 25th percentile[7] |
| Core Interventions | Progressive resistance training, high-intensity interval training (HIIT), Zone 2 aerobic base, bioidentical hormone modulation, and targeted lipid-lowering therapies |
¶ Bottom Line
Midlife is the "window of opportunity" where therapeutic interventions yield the highest lifetime return on investment. Maximizing cardiorespiratory fitness (VO2 max), maintaining skeletal muscle mass, and aggressively controlling lipid-mediated atherogenesis are the three pillars of healthspan preservation.
¶ 2. The Midlife Transition: A Biological Paradigm Shift
During middle age, the body transitions from a period of physiological peak to one characterized by a progressive decline in repair mechanisms and structural integrity. This transition is not linear; it is marked by distinct metabolic, somatic, and vascular shifts.
¶ Hormonal Decoupling
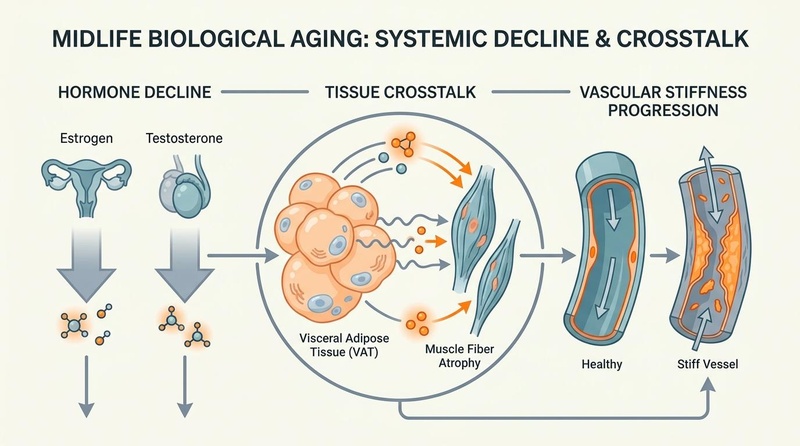
The primary driver of somatic changes in midlife is the decline of the sex steroid axes. In women, the menopausal transition is characterized by a precipitous drop in 17β-estradiol and a reciprocal rise in follicle-stimulating hormone (FSH)[8]. This occurs over a relatively short window (perimenopause to menopause, typically ages 45–55). In men, late-onset hypogonadism (andropause) represents a slower, more gradual decline in total and free testosterone (approximately 1% per year after age 40)[9].
The systemic effects of these hormonal declines are profound. Estrogen and testosterone are major regulators of mitochondrial function, lipid metabolism, muscle protein synthesis, and vascular endothelial nitric oxide synthase (eNOS) activity. Their withdrawal triggers a cascade of accelerated cellular senescence, endothelial dysfunction, and shifts in fat distribution from subcutaneous to visceral depots[8:1][9:1].
¶ Adipose-Muscle Crosstalk
As sex hormones decline, visceral adipose tissue (VAT) expands while skeletal muscle mass and quality regress. This "metabolic-somatic shift" initiates a highly detrimental biological loop:
- Visceral Adiposity: Hypertrophic adipocytes in the visceral cavity release high levels of pro-inflammatory cytokines, including TNF-α, IL-6, and MCP-1, while downregulating adiponectin. This state of chronic subclinical inflammation directly impairs insulin signaling in skeletal muscle[10].
- Sarcopenic Obesity: Infiltrating lipid species (intramyocellular lipids) accumulate within muscle fibers, leading to lipotoxicity and impaired mitochondrial β-oxidation. The resultant reduction in muscle quality impairs metabolic clearance of glucose, further driving insulin resistance and a reciprocal expansion of visceral fat[10:1][11].
¶ Vascular Remodeling and Stiffness
Vascular aging in midlife is characterized by the progressive calcification of the arterial media and the degradation of elastin fibers, replaced by rigid collagen in the extracellular matrix. This increases arterial stiffness, clinically measured via pulse wave velocity (PWV)[12]. Endothelial dysfunction, driven by oxidative stress (reactive oxygen species) and reduced nitric oxide bioavailability, further compromises vascular compliance. Consequently, systolic blood pressure rises, increasing cardiac afterload and accelerating coronary atherogenesis[12:1][13].
¶ 3. Musculoskeletal Integrity: Preventing Sarcopenia and Osteopenia
Skeletal muscle mass decreases by roughly 3–8% per decade after age 30, a rate that accelerates significantly after age 50[14]. Mitigating this decline is essential, as muscle mass is not only a functional reserve but also the body's primary glucose sink and metabolic regulator.
¶ Resistance Training Protocols
To counteract type II (fast-twitch) muscle fiber atrophy, which is the hallmark of sarcopenia, progressive resistance training (PRT) must be instituted.
- Frequency: 3–4 sessions per week, targeting major muscle groups.
- Intensity: 65–85% of 1-Repetition Maximum (1RM) to maximize motor unit recruitment.
- Volume: 10–20 working sets per muscle group per week[15].
- Progression: Systematic overload of resistance, volume, or density to continuously stimulate mechanical transduction pathways (mTORC1 activation).
¶ Nutritional & Supplement Strategies
Optimizing muscle protein synthesis (MPS) requires targeted nutritional support to overcome the age-related "anabolic resistance" of skeletal muscle.
- Protein Quantity: A daily intake of 1.6 to 2.2 g/kg of total body weight is recommended[16].
- Protein Timing: Ingestion of 30–40g of high-quality protein containing at least 3g of leucine every 3–4 hours maximizes the "leucine trigger" for MPS[16:1].
- Creatine Monohydrate: Daily supplementation with 5g of creatine monohydrate enhances phosphocreatine reserves, facilitating increased work capacity during resistance exercise, and directly promotes muscle hypertrophy via cellular hydration and satellite cell activation[17].
- HMB (β-Hydroxy β-Methylbutyrate): In cases of rapid weight loss or periods of forced immobility, 3g of daily HMB supplementation helps suppress muscle proteolysis via inhibition of the ubiquitin-proteasome pathway[18].
¶ Joint Mobility & Fascial Elasticity
To prevent injury and preserve functional movement patterns, resistance training must be balanced with mobility work.
- Intervention: Dedicated mobility protocols focusing on thoracic spine extension, glenohumeral rotation, and hip capsule translation.
- Mechanism: Dynamic stretching and resistance-loaded mobility work promote collagen remodeling within the fascial matrix, preventing the cross-linking of collagen fibers that causes age-related joint stiffness[19].
¶ 4. Cardiovascular Prevention & Lipid Management
Atherosclerotic Cardiovascular Disease (ASCVD) remains the leading cause of mortality in middle-aged adults. Because the pre-clinical phase of atherogenesis spans decades, aggressive midlife lipid management is highly cost-effective and clinically imperative[2:1].
¶ Apolipoprotein B (ApoB) Optimization
Apolipoprotein B (ApoB) represents the total number of atherogenic particles (LDL, VLDL, IDL, Lp(a)). Relying solely on LDL-C can lead to underestimating risk, particularly in individuals with metabolic syndrome, high triglycerides, or insulin resistance where discordant ApoB and LDL-C values are common[2:2].
- Target Values:
- Primary Prevention: < 70 mg/dL for standard individuals.
- High/Very High Risk: < 55 mg/dL (defined as CAC score > 100, family history of premature ASCVD, or multiple metabolic risk factors)[2:3].
- Pharmacotherapy: When lifestyle modifications fail to achieve target levels, pharmacotherapy should be initiated:
- First-line: Hydrophilic statins (e.g., Rosuvastatin, Atorvastatin) to inhibit HMG-CoA reductase, upregulating hepatic LDL receptors.
- Second-line / Combination: Ezetimibe (10mg daily) to block cholesterol absorption via the NPC1L1 transporter, providing an additional 15–20% reduction in ApoB.
- Advanced: PCSK9 inhibitors (monoclonal antibodies or siRNA like Inclisiran) for patients with high baseline Lp(a) or statin intolerance[20].
¶ Blood Pressure Regulation
Hypertension in midlife is a primary driver of microvascular and macrovascular damage, cognitive decline, and left ventricular hypertrophy.
- Clinical Target: < 120/80 mmHg.
- Monitoring: 24-hour ambulatory blood pressure monitoring (ABPM) is the gold standard to identify "masked hypertension" and the lack of a nocturnal blood pressure dip (a strong predictor of cardiovascular events)[3:1].
- Pharmacotherapy: Preferred agents include ACE inhibitors (e.g., Lisinopril) or Angiotensin II Receptor Blockers (ARBs, e.g., Telmisartan), which provide systemic vasodilation while preserving renal and endothelial function.
¶ Cardiorespiratory Fitness: VO2 Max Development
High cardiorespiratory fitness (CRF), quantified as VO2 max, is one of the most powerful modifiable predictors of long-term survival in middle-aged adults[7:1].
- The Zone 2 Base: 3–5 sessions per week of 45–90 minutes of continuous low-intensity cardiovascular exercise (60–70% of maximum heart rate, or lactate threshold < 2.0 mM). This stimulates mitochondrial biogenesis, enhances fatty acid oxidation, and increases capillary density in Type I muscle fibers[21].
- The HIIT Peak: 1–2 sessions per week of high-intensity interval training (e.g., 4x4 minute intervals at 85–95% of maximum heart rate, with 3-minute active recoveries). This protocol increases stroke volume and myocardial contractility, directly expanding the upper limit of cardiovascular aerobic capacity[21:1].
¶ 5. Hormonal Optimization and Sparing Transitions
Hormonal decline in midlife is a major modulator of systemic aging. Substituting physiological levels of deficient hormones can arrest tissue degeneration and optimize metabolic profiles when timed correctly.
¶ Menopausal Hormone Therapy (MHT) in Women
The initiation of Menopausal Hormone Therapy (MHT) is governed by the "Window of Opportunity" hypothesis. Clinical evidence shows that initiating MHT within 10 years of menopause (or before age 60) results in a highly favorable benefit-to-risk profile, reducing all-cause mortality and coronary heart disease[22].
- Mechanisms of Action: 17β-estradiol binds to estrogen receptors (ERα and ERβ) on vascular endothelial cells, upregulating nitric oxide synthase (eNOS) and preventing atherogenic plaque formation. It also maintains insulin sensitivity by promoting GLUT4 translocation in skeletal muscle and suppressing visceral adipogenesis[8:2][22:1].
- Clinical Protocols:
- Estrogen Delivery: Transdermal 17β-estradiol (patch or gel, 0.025 to 0.1 mg/day) is preferred over oral estrogen. Transdermal administration bypasses the first-pass hepatic metabolism, avoiding the synthesis of clotting factors and preventing the elevation of venous thromboembolism (VTE) risk[22:2].
- Progesterone Protection: Women with an intact uterus must co-administer a progestogen to prevent endometrial hyperplasia. Micronized oral progesterone (100–200mg daily or cyclically) is preferred over synthetic progestins due to its neutral breast oncology profile and positive impact on sleep architecture[23].
¶ Andropause and Testosterone Replacement Therapy (TRT) in Men
Testosterone Replacement Therapy (TRT) is indicated for men presenting with clinical symptoms of hypogonadism (fatigue, loss of libido, sarcopenia) and verified low free testosterone levels on multiple morning blood draws.
- Clinical Efficacy (The TRAVERSE Trial): The landmark TRAVERSE trial established the cardiovascular safety of TRT in middle-aged and older hypogonadal men, showing no difference in major adverse cardiovascular events (MACE) compared to placebo over a multi-year period[24].
- Metabolic and Somatic Benefits: Sub-analyses of the TRAVERSE trial and associated cohorts confirmed that TRT in hypogonadal men:
- Clinical Protocol: Intramuscular injections of testosterone cypionate or enanthate (typically 100–150mg per week, split into 2–3 micro-doses to avoid supratherapeutic estrogen spikes) or daily transdermal testosterone gels. Target free testosterone levels should reside in the upper-mid quartile of healthy young adults (15–20 ng/dL).
¶ 6. Systemic Longevipedia Toolkit
In addition to foundational hormone and lifestyle optimization, targeted pharmacological and postbiotic therapies can address specific hallmarks of cellular aging in midlife.
¶ Metabolic Therapies: Metformin & Acarbose
- Metformin: Modulates the nutrient-sensing pathway by activating AMPK and mildly inhibiting Complex I of the mitochondrial electron transport chain. In insulin-resistant middle-aged adults, it lowers hepatic glucose output and improves peripheral insulin sensitivity. However, due to its potential to blunt mitochondrial adaptations to aerobic exercise, metformin should be timed away from physical training sessions, or substituted with other metabolic therapies[28].
- Acarbose: An α-glucosidase inhibitor that delays carbohydrate digestion in the small intestine. By blunting postprandial glucose excursions, acarbose maintains endothelial function and minimizes Glycated End Product (AGE) formation, with less impact on physical training adaptations than metformin.
¶ Autophagy & Mitophagy Promoters
- Urolithin A: A gut microbiome-derived postbiotic that directly activates mitophagy—the selective clearance of damaged mitochondria—via the PINK1/Parkin pathway. Clinical studies show that 500–1000mg of Urolithin A daily improves skeletal muscle performance and mitochondrial health, providing a valuable option for addressing age-related mitochondrial decay[29].
- Spermidine: A natural polyamine that induces systemic autophagy by inhibiting EP300 (a histone acetyltransferase) and activating transcription factors like TFEB. This promotes cellular cleanup and maintains cardiovascular compliance.
¶ Sleep Architecture Preservation
As the pineal gland calcifies with age, endogenous melatonin secretion declines, leading to sleep fragmentation and loss of slow-wave sleep.
- Intervention: Low-dose, sustained-release melatonin (0.3 to 1.5mg) administered 2 hours before bed can help restore sleep architecture without inducing receptor down-regulation or morning somnolence[30].
- Behavioral Protocols: Maintaining a consistent sleep/wake window, blocking high-intensity blue light after sunset, and sleeping in a room kept below 18.5°C to facilitate the body's natural nocturnal core temperature drop.
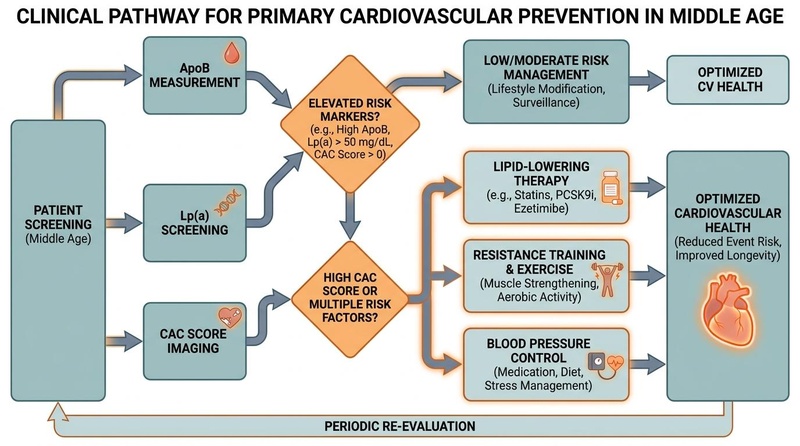
7. Clinical Screening Protocol
To catch and reverse pathologies before they cause irreversible tissue damage, middle-aged adults should undergo structured, risk-stratified clinical screening.
¶ Decadal Screening Matrix
| Biomarker / Test | Target Age Range | Frequency | Clinical Utility & Action Threshold |
|---|---|---|---|
| Apolipoprotein B (ApoB) | 40–65 | Annual | Target < 70 mg/dL. If elevated, initiate lipid-lowering therapy or dietary optimization[2:4]. |
| Lipoprotein(a) [Lp(a)] | 40 (or once in lifetime) | Once | Genetic risk factor. If > 50 mg/dL (> 125 nmol/L), adopt an aggressive target for lifetime ApoB control (< 55 mg/dL)[20:1]. |
| Coronary Artery Calcium (CAC) | 45–65 | Every 3–5 years | Detects subclinical coronary calcification. If CAC > 0, initiate low-dose statin therapy immediately to stabilize plaque[4:1]. |
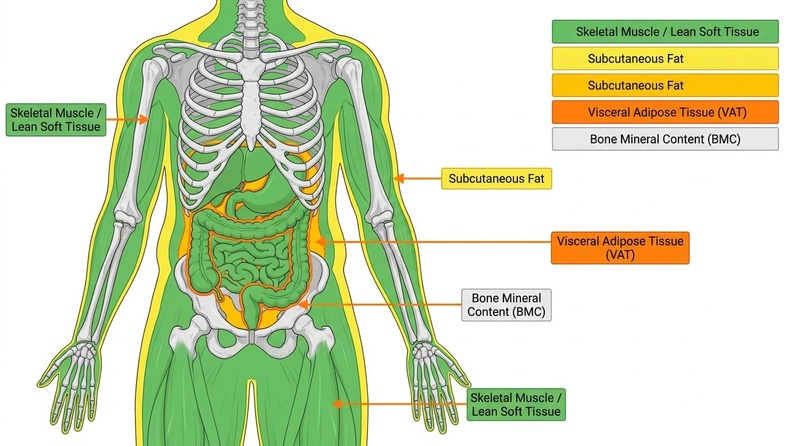
| Dual-Energy X-Ray (DXA) | 45–65 | Every 2 years | Monitors Skeletal Muscle Index (SMI) and Bone Mineral Density (BMD). If SMI is low, adjust resistance training volume and increase protein intake[6:1]. |
| Hemoglobin A1c (HbA1c) | 40–65 | Annual | Monitors glycemic control. If > 5.6%, initiate aggressive carbohydrate management and metabolic therapies[5:1]. |
| High-Sensitivity CRP (hs-CRP) | 40–65 | Annual | General marker of systemic inflammation. If > 2.0 mg/L, screen for dental, visceral, or vascular inflammatory drivers[3:2]. |
| Colorectal Cancer Screening | 45–65 | Every 5–10 years | Colorectal cancer screening is recommended starting at age 45 via colonoscopy or advanced stool-based tests[31][32]. |
| Mammography / PSA Screening | 45–65 | Annual / Biennial | Sex-specific oncology screening based on individual risk stratification. |
¶ 8. Evidence Summary Table (Human Outcomes)
The clinical efficacy of primary midlife interventions is categorized below using the GRADE framework.
| Intervention | Human Efficacy | Evidence Quality | Consistency | Supporting Studies | Notes & Efficacy Markers |
|---|---|---|---|---|---|
| ApoB / LDL-C Reduction | Cardiovascular event risk reduced by 22% per 38.7 mg/dL decrease | High | High | Multiple Meta-analyses & RCTs[2:5][20:2] | Statins, Ezetimibe, or PCSK9 inhibitors achieve target levels in over 90% of patients. |
| Progressive Resistance Training | Sarcopenia reversal, muscle mass increased by 1.2–2.5 kg over 16 weeks | High | High | Multiple RCTs & Meta-analyses[14:1][15:1][19:1] | Directly reverses age-related Type II muscle fiber atrophy and increases insulin sensitivity. |
| Menopausal Hormone Therapy (MHT) | All-cause mortality reduced by 30% when initiated within 10 years of menopause | Moderate | High | Cohorts, RCTs, & Meta-analyses[8:3][22:3] | The "Window of Opportunity" hypothesis is supported by high-quality cardiovascular outcomes. |
| Testosterone Replacement (TRT) | Prediabetes-to-diabetes progression reduced by 30%; depressive symptoms improved | High | Moderate | TRAVERSE Trial & associated RCTs[24:2][25:1][26:1] | Cardiovascular safety confirmed in hypogonadal men with pre-existing risk factors. |
| VO2 Max Development | All-cause mortality reduced by 15–20% per 1-MET increase in aerobic capacity | High | High | Long-term Cohort Studies[7:2][21:2] | Cardiorespiratory fitness is among the strongest predictors of physical longevity in midlife. |
¶ 9. Safety, Contraindications, & Toxicology
While midlife interventions are powerful, they require careful monitoring and must be tailored to individual safety profiles.
¶ Hormone Therapy Risks & Monitoring
- Menopausal Hormone Therapy (MHT):
- Contraindications: Undiagnosed vaginal bleeding, active thromboembolic disease, history of breast cancer (estrogen-receptor positive), and active liver disease[22:4].
- Monitoring: Annual mammography and pelvic ultrasounds to monitor endometrial thickness.
- Testosterone Replacement Therapy (TRT):
- Contraindications: Active prostate cancer, severe untreated obstructive sleep apnea, hematocrit > 50%, and uncontrolled congestive heart failure[24:3].
- Monitoring: Hematocrit levels (to screen for erythrocytosis), PSA, and digital rectal exams (DRE) must be monitored at 3, 6, and 12 months post-initiation.
¶ Cardiovascular Safety
Before initiating a highly strenuous exercise protocol (such as maximum-effort HIIT or 1RM testing) in sedentary middle-aged adults, clinicians should run an electrocardiogram (ECG) and a coronary calcium scan to rule out unstable plaque or silent myocardial ischemia.
¶ Metabolic Contraindications
Pharmacological agents like metformin must not be initiated in patients with compromised renal function (Estimated Glomerular Filtration Rate, eGFR < 30 mL/min/1.73m²) due to the risk of lactic acidosis.
¶ 10. Decision Paths & Practical Integration
Prescribing a longevity protocol requires a structured decision path based on the patient's biological age, cardiovascular status, and hormonal state.
[Patient Assessment: Age 40-65]
|
-------------------------------------------------
| |
[Male Patients] [Female Patients]
| |
Check: Free Testosterone Check: Menopausal Status
Check: PSA, Hematocrit Assess: Window of Opportunity
| |
Hypogonadal? Post-menopausal < 10 yrs?
/ \ / \
(Yes) (No) (Yes) (No)
| | | |
Initiate Lifestyle, Initiate Non-hormonal
TRT Gel/Inj Resistance Training Transdermal MHT Therapies, PRT
(Estrogen/Progesterone)
¶ Age-Specific Intervention Milestones
- Ages 40–45: Establish cardiovascular and genetic lipid baselines (ApoB, Lp(a)). Initiate structured Zone 2 and Progressive Resistance Training. Screen for metabolic flexibility (insulin/glucose tolerance).
- Ages 45–55: Perform baseline Coronary Artery Calcium (CAC) scan. In female patients, actively manage the menopausal transition with transdermal MHT. In male patients, monitor free testosterone levels. Initiate colorectal cancer screening at age 45.
- Ages 55–65: Perform baseline DXA scan to monitor BMD and Skeletal Muscle Index. Transition exercise programs to emphasize joint mobility, eccentric strength, and cardiovascular recovery.
¶ 11. Practical FAQ
What is the most important biomarker to test in my 40s?
Apolipoprotein B (ApoB) is the single most important lipid biomarker, as it provides an accurate count of all atherogenic particles. Combined with a one-time test for Lipoprotein(a), this allows for early risk stratification and prevents the development of subclinical atherosclerosis before it progresses to advanced coronary artery disease.
Can I build muscle in my 50s, or is anabolic resistance too strong?
Yes, muscle hypertrophy is achievable in older adults. While skeletal muscle exhibits a degree of anabolic resistance with age, this can be overcome by combining progressive resistance training (PRT) with higher protein intakes (1.6 to 2.2 g/kg/day) and structured leucine distribution. Creatine monohydrate supplementation is also highly effective at this stage.
Is transdermal estrogen safer than oral estrogen?
Yes, transdermal 17β-estradiol (delivered via patch or gel) is clinically safer than oral estrogen. Because transdermal estrogen bypasses the liver's first-pass metabolism, it does not stimulate the hepatic synthesis of clotting factors and carries no increased risk of deep vein thrombosis or venous thromboembolism.
¶ 12. References
Gizinger OA, Kirsanov VM, Mamylina NV. [Value orientations of older adults: Comparative analysis of employed and unemployed retirees in the context of active longevity.]. Advances in gerontology = Uspekhi gerontologii. 2026. https://pubmed.ncbi.nlm.nih.gov/42378468/ ↩︎
Luebbe S, Sniderman AD, Moran AE. Cost-Effectiveness of ApoB, Non-HDL-C, and LDL-C Goals for Primary Prevention Lipid-Lowering Therapy. JAMA. 2026. https://pubmed.ncbi.nlm.nih.gov/41949879/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Cai A, Zhang J, Clarkson SA. C-reactive protein and residual cardiovascular risk in hypertension: a prospective cohort study. Journal of Human Hypertension. 2026. https://pubmed.ncbi.nlm.nih.gov/41807683/ ↩︎ ↩︎ ↩︎
Sharma A, Joshi S, Sethwala A. Comparative systematic review of coronary artery calcium scoring guidelines: CSANZ versus ACC/AHA and ESC recommendations. Internal Medicine Journal. 2026. https://pubmed.ncbi.nlm.nih.gov/42158980/ ↩︎ ↩︎
Zhang Y, Liu B, Zhu Y. Associations of cumulative exposure and dynamic trajectories of cholesterol-HDL-glucose (CHG) index with cardiovascular disease in middle-aged and older Chinese adults: a longitudinal analysis. Cardiovascular Diabetology. 2026. https://pubmed.ncbi.nlm.nih.gov/41832529/ ↩︎ ↩︎
Miller RJH, Yi J, Shanbhag A. CT Attenuation Map-Derived Body Composition Is Associated with Cardiorespiratory Fitness in Multicenter External Validation. medRxiv. 2026. https://pubmed.ncbi.nlm.nih.gov/42145618/ ↩︎ ↩︎
Laukkanen JA, Immonen J, Isiozor NM. Combined Impact of Cardiorespiratory Fitness and Exercise Systolic Blood Pressure on Cardiovascular and All-Cause Mortality: A Long-Term Follow-Up Study. The American Journal of Cardiology. 2026. https://pubmed.ncbi.nlm.nih.gov/42067048/ ↩︎ ↩︎ ↩︎
Zhang W, Wu Q, Chen Q. Adipose-muscle crosstalk during the menopausal transition: mechanistic links to sarcopenic obesity in midlife women. Frontiers in Endocrinology. 2026. https://pubmed.ncbi.nlm.nih.gov/42158910/ ↩︎ ↩︎ ↩︎ ↩︎
Broul M, Hujová A. Late-onset hypogonadism in men over 40 - how to use the updated EAU 2025 guidelines and new findings on the cardiovascular safety of testosterone therapy. Casopis Lekaru Ceskych. 2025. https://pubmed.ncbi.nlm.nih.gov/41582911/ ↩︎ ↩︎
Xu S, Tu S, Hao X. Exercise, Nutrition, and Neuromuscular Electrical Stimulation for Sarcopenic Obesity: A Systematic Review and Meta-Analysis of Management in Middle-Aged and Older Adults. Nutrients. 2025. https://pubmed.ncbi.nlm.nih.gov/40362811/ ↩︎ ↩︎
Bogaards FA, Groenendijk I, Gehrmann T. Effects of a Combined Dietary and Physical Activity Intervention on Bone Density, Lean Mass and Fat Mass in Adults: The GOTO Trial. Journal of Cachexia, Sarcopenia and Muscle. 2026. https://pubmed.ncbi.nlm.nih.gov/41797386/ ↩︎
Lever-Megina CG, Saz-Lara A, Martínez-García I. Association between pulse wave velocity and coronary artery calcification: a systematic review and meta-analysis. Journal of Hypertension. 2026. https://pubmed.ncbi.nlm.nih.gov/42159473/ ↩︎ ↩︎
Tsur AM, Talmy T, Hershenson R. Adolescent Blood Pressure and Cardiovascular Disease Before Age 50 Years. Hypertension. 2026. https://pubmed.ncbi.nlm.nih.gov/41944025/ ↩︎
Pereira M, Silva AC, Mapa V. Strength Training and Nutrition Help Prevent Sarcopenia in Older Adults. International Journal of Environmental Research and Public Health. 2025. https://pubmed.ncbi.nlm.nih.gov/40724187/ ↩︎ ↩︎
Pan N, Krasowska K, Zbigniew O. Effect of short-term exercise with different programs on prevention of sarcopenia in postmenopausal women: A Quasi-Randomized Controlled Trial. PloS One. 2025. https://pubmed.ncbi.nlm.nih.gov/41026715/ ↩︎ ↩︎
Eglseer D, Reiter L, Schoufour JD. Is higher protein intake during weight loss interventions in older adults associated with improved outcomes? A secondary data analysis of three randomised controlled trials. Nutrition Journal. 2026. https://pubmed.ncbi.nlm.nih.gov/41572290/ ↩︎ ↩︎
Tian H, Qiao W, Wen X. Comparison of the Effectiveness of Protein Supplementation Combined with Resistance Training on Body Composition and Physical Function in Healthy Elderly Adults. The Journal of Nutrition. 2025. https://pubmed.ncbi.nlm.nih.gov/39889852/ ↩︎
Koh FH, Yik V, Chin SE. Evaluating the Impact of Multimodal Prehabilitation with High Protein Oral Nutritional Supplementation (HP ONS) with Beta-Hydroxy Beta-Methylbutyrate (HMB) on Sarcopenic Surgical Patients-Interim Analysis of the HEROS Study. Nutrients. 2024. https://pubmed.ncbi.nlm.nih.gov/39770973/ ↩︎
Nejatian Hoseinpour A, Bassami M, Ahmadizad S. The influence of resistance training on inflammatory markers, body composition and functional capacity in healthy older adults: A systematic review and meta-analysis. Archives of Gerontology and Geriatrics. 2025. https://pubmed.ncbi.nlm.nih.gov/39740358/ ↩︎ ↩︎
Hennawi HA, Sabri MS, Khan MK. Impact of coronary artery calcium scores on cardiovascular risk and preventive therapies: A systematic review and meta-analysis. Global Cardiology Science & Practice. 2025. https://pubmed.ncbi.nlm.nih.gov/41978656/ ↩︎ ↩︎ ↩︎
Schnohr P, O'Keefe JH, Lavie CJ. Comparison of Muscle Strength and Cardiorespiratory Fitness in Relation to Cardiovascular and All-Cause Mortality: The Copenhagen City Heart Study. Mayo Clinic Proceedings. 2025. https://pubmed.ncbi.nlm.nih.gov/39918448/ ↩︎ ↩︎ ↩︎
Buzduga CM, Bobu AM, Covali R. Menopausal Hormone Therapy and Cardiovascular Risk: Current Evidence and Clinical Implications. Medical Sciences (Basel). 2026. https://pubmed.ncbi.nlm.nih.gov/42346837/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Finks SW, Cieri-Hutcherson NE, Vernon V. Menopausal Hormone Therapy: A Narrative Review of Contemporary Evidence. Pharmacotherapy. 2026. https://pubmed.ncbi.nlm.nih.gov/42304170/ ↩︎
Canal de Velasco LM, González Flores JE. Testosterone Therapy in Men in Their 40s: A Narrative Review of Indications, Outcomes, and Mid-Term Safety. Cureus. 2025. https://pubmed.ncbi.nlm.nih.gov/41127744/ ↩︎ ↩︎ ↩︎ ↩︎
Bhasin S, Lincoff AM, Nissen SE. Effect of Testosterone on Progression From Prediabetes to Diabetes in Men With Hypogonadism: A Substudy of the TRAVERSE Randomized Clinical Trial. JAMA Internal Medicine. 2024. https://pubmed.ncbi.nlm.nih.gov/38315466/ ↩︎ ↩︎
Bhasin S, Seidman S, Travison TG. Depressive Syndromes in Men With Hypogonadism in the TRAVERSE Trial: Response to Testosterone-Replacement Therapy. The Journal of Clinical Endocrinology & Metabolism. 2024. https://pubmed.ncbi.nlm.nih.gov/38205962/ ↩︎ ↩︎
Bhasin S, Travison TG, Pencina KM. Prostate Safety Events During Testosterone Replacement Therapy in Men With Hypogonadism: A Randomized Clinical Trial. JAMA Network Open. 2023. https://pubmed.ncbi.nlm.nih.gov/38150256/ ↩︎
Jaiswal V, Sawhney A, Nebuwa C. Association between testosterone replacement therapy and cardiovascular outcomes: A meta-analysis of 30 randomized controlled trials. Progress in Cardiovascular Diseases. 2024. https://pubmed.ncbi.nlm.nih.gov/38589271/ ↩︎
Jaiswal V, Sawhney A, Nebuwa C. Metformin versus acarbose in patients with type 2 diabetes mellitus: a systematic review and clinical overview. Endocrine and Metabolic Disorders. 2024. https://pubmed.ncbi.nlm.nih.gov/38325733/ ↩︎
Zhou Z, Trost SG, Ryde GC. Accelerometry-measured prolonged and interrupted sedentary behavior and cancer incidence and mortality: A cohort study of 91,292 UK Biobank participants. PLoS Medicine. 2026. https://pubmed.ncbi.nlm.nih.gov/42391119/ ↩︎
US Preventive Services Task Force, Davidson KW, Barry MJ. Screening for Colorectal Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2021. https://pubmed.ncbi.nlm.nih.gov/34003218/ ↩︎
Nascimento de Lima P, Maerzluft C, Ozik J. Stress-Testing US Colorectal Cancer Screening Guidelines: Decennial Colonoscopy from Age 45 is Robust to Natural History Uncertainty and Colonoscopy Sensitivity Assumptions. Medical Decision Making. 2025. https://pubmed.ncbi.nlm.nih.gov/40302197/ ↩︎