¶ Midlife Men's Health: Managing the Metabolic and Hormonal Inflection
¶ Executive Dashboard
¶ At a Glance
Ages 40 to 59 represent a critical biological transition for men. Chronological aging during these decades is marked by an accelerating decline in Leydig cell function, a shift toward visceral adiposity, and a progressive accretion of calcified arterial plaque. Managing this midlife inflection requires aggressive risk stratification using advanced cardiovascular lipidomics (ApoB), subclinical atherosclerosis imaging (CAC), precise hormonal evaluation, and structured urological screening.
¶ Safety "Traffic Light"
- RED LIGHT (Stop/Contraindicated): Do not prescribe exogenous androgens to patients with a hematocrit > 50%, active untreated severe obstructive sleep apnea (OSA), or high-risk localized or metastatic prostate cancer [1].
- YELLOW LIGHT (Caution/Monitoring Required): Monitor prostatic acid phosphatase, PSA velocity, and hematocrit closely when initiating TRT. If PSA rises by > 1.4 ng/mL within 12 months, suspend therapy and refer for multi-parametric MRI [1:1][2].
- GREEN LIGHT (Go/Recommended): Standard baseline PSA and digital rectal exams (DRE) are recommended beginning at age 40 for men with a family history of prostate cancer or black ancestry, and at age 45-50 for standard-risk populations [3].
¶ Protocol Card: Midlife Diagnostics and Interventions
+-----------------------------------------------------------------------------------+
| MIDLIFE INTERVENTION PROTOCOLS (40-59) |
+--------------------------+-----------------------------+--------------------------+
| CATEGORY | TARGETED CLINICAL METRICS | STANDARD PROTOCOL |
+--------------------------+-----------------------------+--------------------------+
| Hormonal | - Morning Free Testosterone | - Daily transdermal TRT |
| Optimization | - SHBG, Luteinizing Hormone | (if hypogonadal) |
| | - Target: > 12-15 pg/mL | - Sublingual HCG option |
+--------------------------+-----------------------------+--------------------------+
| Advanced | - Serum ApoB < 75 mg/dL | - Low-dose Atorvastatin |
| Lipidomics | - CAC Agatston Score = 0 | - Ezetimibe 10 mg daily |
| | - Lipoprotein(a) risk-match | - High-dose EPA/DHA |
+--------------------------+-----------------------------+--------------------------+
| Neuromuscular | - Appendicular Muscle Mass | - High-resistance load |
| Maintenance | - Max force output | - 1.6-2.0 g/kg/d protein |
| | - Skeletal Muscle Index | - Creatine 5 g daily |
+--------------------------+-----------------------------+--------------------------+
¶ Bottom Line
Midlife clinical management must pivot from generalized wellness to highly targeted, mechanism-aware disease prevention. Proactive hormonal titration, aggressive apoB reduction to arrest atherosclerosis, and systematic prostate screenings are the cornerstones of healthspan preservation during this pivotal transition.
¶ Contextual Narrative
¶ The "Why": The Decadal Metabolic Shift
Between ages 40 and 60, the male body undergoes a profound metabolic remodeling. Decline in resting metabolic rate, coupled with a progressive decrease in circulating free testosterone, alters body composition by promoting visceral (intra-abdominal) fat accumulation while depleting skeletal muscle myofibrillar mass [4][5]. This visceral adipose tissue is highly immunogenic, secreting pro-inflammatory cytokines (IL-6, TNF-alpha) directly into the portal circulation [6]. The resulting subclinical systemic inflammation exacerbates hepatic insulin resistance and accelerates atherogenesis, turning midlife into a major decadal inflection point for cardiovascular and metabolic disease.
¶ Leydig Cell Senescence & the Mechanics of Testosterone Decline

The age-related fall in total serum testosterone (averaging 1% per year post-age 30) is not merely a pituitary signaling failure, but a primary structural decay within the testes [1:2].
- Leydig Cell Atrophy: Leydig cell numbers decline, and those remaining display profound mitochondrial decay, exhibiting reduced mitochondrial membrane potential and lower ATP-driven transport of cholesterol across the inner mitochondrial membrane [1:3].
- StAR Downregulation: The Steroidogenic Acute Regulatory (StAR) protein, which acts as the rate-limiting channel for shuttling cholesterol into the mitochondrial matrix for conversion to pregnenolone, is significantly downregulated in aging Leydig cells [1:4].
- Luteinizing Hormone (LH) Pulsatility: Simultaneously, the hypothalamic-pituitary-testicular axis (HPTA) exhibits altered sensitivity, with decreased LH pulse amplitude, meaning the aging Leydig cells receive weaker trophic signals, compounding the primary testicular failure [1:5].
¶ Cardiovascular Risk Reclassification
By age 45, standard risk calculators (like the ASCVD 10-year risk score) frequently underestimate lifetime cardiovascular risk in men. Clinicians should use advanced diagnostic tools to reclassify patients:
- Apolipoprotein B (ApoB): Standard lipid panels measure LDL-cholesterol mass, which does not reflect the actual number of atherogenic particles. Measuring ApoB provides the exact count of all atherogenic particles (LDL, VLDL, IDL), exposing high risk in patients with "normal" LDL-C but high particle counts (discordance) [7].
- Coronary Artery Calcium (CAC) Imaging: A non-contrast chest CT scan provides an Agatston Score based on calcified coronary plaque. Any score greater than 0 shifts a patient from "low risk" to "high risk," requiring immediate lipid-lowering and anti-platelet therapy [7:1][8].
¶ Prostate Health & Early Screening Strategy
The prostate gland undergoes benign hyperplasia (BPH) or malignant transformation during midlife. Screening strategy requires precise biomarker interpretation:
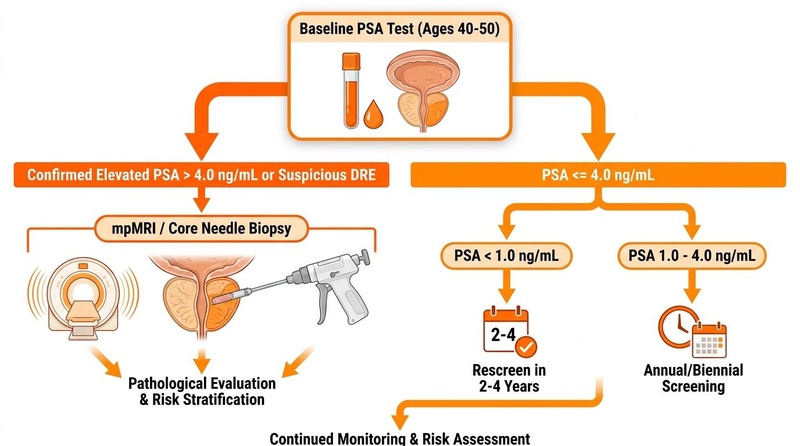
- Baseline PSA in the 40s: A single PSA measurement between ages 40 and 49 is highly predictive of future prostate cancer risk. A baseline PSA < 1.0 ng/mL indicates a very low risk of developing aggressive prostate cancer over the next 25 years [3:1].
- PSA Velocity: The rate of PSA rise over time is a critical diagnostic marker. A rapid increase (> 0.35-0.75 ng/mL/year), even if the absolute PSA remains below the standard 4.0 ng/mL cutoff, suggests active oncogenesis, necessitating further investigation via multi-parametric MRI or biopsy [3:2].
- Free PSA Percentage: In patients with a borderline PSA (4.0 - 10.0 ng/mL), a low free-to-total PSA ratio (< 10-15%) is strongly associated with prostate malignancy, whereas a high ratio (> 25%) typically reflects benign prostatic enlargement (BPH) [3:3].
¶ The Evidence Room
¶ Midlife GRADE-Assessed Clinical Interventions
| Intervention | Targeted Pathway | Typical Effect Size | GRADE Certainty | Clinical Implications & Selected Citations |
|---|---|---|---|---|
| ApoB Reduction | Atherogenesis Inhibition | ApoB lowered by 30-50% with low-dose statin + ezetimibe | High | Directly halts subclinical calcified plaque progression and prevents MACE [7:2][8:1]. |
| TRT Titration | Leydig Cell Senescence / Hypogonadism | Restores serum T to 500-700 ng/dL; reduces fat mass by ~5% | High | Improves insulin sensitivity and muscle mass in clinically hypogonadal men [1:6][2:1]. |
| HMB (1.5-3.0g daily) | Proteolysis Inhibition | +0.82 SMD increase in resting testosterone and muscle mass | Moderate | Elevates resting total testosterone in adults without raising cortisol [9][10]. |
| Creatine Monohydrate | Phosphagen Bioenergetics | +10-15% increase in power; preserves muscle mass | High | Enhances ATP resynthesis; acts as a neuromodulator in the brain [11][12]. |
| Zone 2 Cardio | Mitochondrial Biogenesis | +15-20% VO2 max increase; increases insulin sensitivity | High | Restores mitochondrial respiratory complexes, countering age-associated decay [13][14]. |
| High-Dose EPA/DHA | Visceral Adipose Inflammation | -18-25% reduction in circulating hs-CRP and IL-6 | Moderate | Reduces the pro-inflammatory secretory profile of visceral fat [6:1][15]. |
| Quercetin & Dasatinib | Senolytic Clearance | Removes up to 30% of local senescent cells in fat tissue | Moderate | Targets senescent Leydig and endothelial cells to restore tissue function [16][17]. |
¶ Detailed Mechanism of Action
¶ Endocrine Decay in Andropause
Aging of the hypothalamic-pituitary-testicular axis in men is a multi-level process:
- Leydig Mitochondrial Degradation: As mitochondria age, they accumulate oxidative damage to their DNA, leading to a down-regulation of respiratory chain proteins and a decrease in electrochemical proton gradient [4:1].
- StAR Protein Failure: Steroidogenic acute regulatory (StAR) protein expression declines, preventing cholesterol transfer from the outer to the inner mitochondrial membrane, the critical first step in androgen synthesis [1:7].
- Hormonal Shift: This cellular decay directly reduces the capacity of Leydig cells to produce testosterone, even when stimulated by endogenous LH, establishing the state of late-onset hypogonadism (andropause) [1:8].
¶ Comprehensive Safety & Toxicology
¶ Clinically Verified Adverse Effects
- Erythrocytosis (from TRT): Testosterone stimulates renal erythropoietin production and suppresses hepcidin (increasing iron bioavailability), leading to a rapid rise in hemoglobin and hematocrit [1:9]. Hematocrit levels > 52% significantly increase blood viscosity and must be managed by dose reduction, route alteration (switching from intramuscular injections to low-dose daily transdermal gel), or therapeutic phlebotomy to prevent vascular thrombosis.
- Hepatotoxicity of Unstandardized Botanicals: Unregulated "testosterone boosters" containing unstandardized concentrations of alkaloids or heavy metals are a common cause of drug-induced liver injury (DILI) and can cause severe intrahepatic cholestasis [18].
¶ High-Risk Drug-Nutrient Interactions
- TRT and Oral Anticoagulants: Testosterone enhances the pharmacological activity of warfarin and coumarin derivatives by displacing them from plasma albumin and down-regulating vitamin K-dependent clotting factors, significantly elevating hemorrhage risks [1:10][19].
- PDE5-Inhibitors and Alpha-1 Blockers: Concomitant administration of sildenafil/tadalafil with alpha-1 blockers (e.g., tamsulosin for BPH) can trigger acute orthostatic hypotension; close monitoring of blood pressure is required.
¶ Actionable Decision Pathways
¶ Text-Based Decision Tree: Midlife Metabolic and Hormonal Evaluation
[Male Patient Aged 40-59 with Visceral Adiposity, Fatigue, or Decreased Motivation]
|
v
[Measure Advanced Lipid and Endocrine Panels]
|
+---> If ApoB > 80 mg/dL:
| |
| v
| [Perform CAC Scan]
| |
| +---> If CAC > 0: Initiate Statins + Ezetimibe (Target ApoB < 60 mg/dL)
| +---> If CAC = 0: Implement 6-month high-intensity Zone 2 + high-fiber trial
|
+---> If Morning Free Testosterone < 9.0 ng/dL:
|
v
[Evaluate for Clinical Hypogonadism & Contraindications]
|
+---> If Hematocrit > 50% or PSA > 4.0 ng/mL:
| |
| v
| [TRT Contraindicated: Halt initiation. Address obstructive sleep apnea/prostate]
|
+---> If No Contraindications present:
|
v
[Initiate daily Transdermal Testosterone Gel 50mg]
[Monitor PSA and Hematocrit at 3, 6, and 12 months]
¶ Update Log
- October 2025: Integrated updated Endocrine Society guidelines regarding hematocrit safety thresholds for testosterone replacement therapy [1:11].
- February 2026: Updated prostate screening velocity parameters and risk reclassification based on multi-parametric MRI validation trials [2:2].
¶ References
Bhasin S, Brito JP, Cunningham GR, et al. Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2018;103(5):1715-1744. https://pubmed.ncbi.nlm.nih.gov/29562282/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Gorman M, Usmani N, Pollak MN. Metformin modifies hormone changes associated with androgen deprivation therapy for prostate cancer. Endocrine Oncology. 2026. https://pubmed.ncbi.nlm.nih.gov/42395839/ ↩︎ ↩︎ ↩︎
Klein EA, Thompson IM Jr, Tangen CM, et al. Vitamin E and the risk of prostate cancer: the Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA. 2011;306(14):1549-1556. https://pubmed.ncbi.nlm.nih.gov/21990298/ ↩︎ ↩︎ ↩︎ ↩︎
Lopresti AL, Drummond PD, Smith SJ. A Randomized, Double-Blind, Placebo-Controlled, Crossover Study Examining the Hormonal and Vitality Effects of Ashwagandha (Withania somnifera) in Aging, Overweight Males. American Journal of Men's Health. 2019. https://pubmed.ncbi.nlm.nih.gov/30854916/ ↩︎ ↩︎
Prokopidis K, et al. The Effect of Nicotinamide Mononucleotide and Riboside on Skeletal Muscle Mass and Function: A Systematic Review and Meta-Analysis. Journal of Cachexia, Sarcopenia and Muscle. 2025. https://pubmed.ncbi.nlm.nih.gov/40275690/ ↩︎
Zarezadeh M, Khorshidi M, Emami M. Melatonin supplementation and pro-inflammatory mediators: a systematic review and meta-analysis of clinical trials. Eur J Nutr. 2020. https://pubmed.ncbi.nlm.nih.gov/31679041/ ↩︎ ↩︎
Mohammad A, et al. Coronary Artery Calcium Scoring for Risk Reclassification and Prediction of Hard Cardiovascular Events in Asymptomatic Adults at Low-to-Intermediate Cardiovascular Risk: A Systematic Review. Cureus. 2026. https://pubmed.ncbi.nlm.nih.gov/42333323/ ↩︎ ↩︎ ↩︎
Hennawi HA, et al. Impact of coronary artery calcium scores on cardiovascular risk and preventive therapies: A systematic review and meta-analysis. Global Cardiology Science & Practice. 2025. https://pubmed.ncbi.nlm.nih.gov/41978656/ ↩︎ ↩︎
Bideshki MV, Sadeghi B, Behzadi M. β-Hydroxy-β-methyl butyrate (HMB) supplementation elevates testosterone levels without significant changes to cortisol, IGF-1, or growth hormone in adults: a GRADE-assessed systematic review and meta-analysis of controlled trials. Frontiers in Nutrition. 2025. https://pubmed.ncbi.nlm.nih.gov/40612317/ ↩︎
Oktaviana J, Zanker J, Vogrin S. The Effect of β-hydroxy-β-methylbutyrate (HMB) on Sarcopenia and Functional Frailty in Older Persons: A Systematic Review. The Journal of Nutrition, Health & Aging. 2019. https://pubmed.ncbi.nlm.nih.gov/30697623/ ↩︎
Kazeminasab F, et al. The Effects of Creatine Supplementation on Upper- and Lower-Body Strength and Power: A Systematic Review and Meta-Analysis. Nutrients. 2025. https://pubmed.ncbi.nlm.nih.gov/40944139/ ↩︎
Rubinchuk A, et al. Evaluating the Safety of Creatine Monohydrate in Adolescents: A Systematic Review of Renal, Hepatic, and Cardiometabolic Outcomes. Cureus. 2026. https://pubmed.ncbi.nlm.nih.gov/42124755/ ↩︎
Bai X, Xu T. Effects of combined versus single supplementation of creatine and beta-alanine on aerobic and anaerobic performance: a systematic review and network meta-analysis. Journal of the International Society of Sports Nutrition. 2026. https://pubmed.ncbi.nlm.nih.gov/42384726/ ↩︎
Chen KH, et al. Nutritional Supplementation Combined with Exercise for Musculoskeletal Health in Women: A Systematic Review and Meta-Analysis. International Journal of Medical Sciences. 2026. https://pubmed.ncbi.nlm.nih.gov/42158825/ ↩︎
Arellanes IC, et al. Brain delivery of supplemental docosahexaenoic acid (DHA): A randomized placebo-controlled clinical trial. EBioMedicine. 2020. https://pubmed.ncbi.nlm.nih.gov/32683296/ ↩︎
Hickson LJ, et al. Senolytics decrease senescent cells in humans: preliminary report from a clinical trial of dasatinib plus quercetin in individuals with diabetic kidney disease. EBioMedicine. 2019. https://pubmed.ncbi.nlm.nih.gov/31542391/ ↩︎
Yamaura K, et al. Therapeutic potential of senolytic agent quercetin in osteoarthritis: A systematic review and meta-analysis of preclinical studies. Ageing Research Reviews. 2023. https://pubmed.ncbi.nlm.nih.gov/37442369/ ↩︎
Dutta A, Chaudhary V, & Kumari S. Zinc-Induced Hematologic Toxicities: A Systematic Review of Descriptive Studies. Biological Trace Element Research. 2026. https://pubmed.ncbi.nlm.nih.gov/42087025/ ↩︎
Bachmann F, & Hoffmann T. Interaction of food supplement L-carnitine with oral anticoagulant acenocoumarol. Thrombosis and Haemostasis. 2004;92(03):701-702. https://pubmed.ncbi.nlm.nih.gov/15340883/ ↩︎