¶ Older Adult Longevity and Functional Preservation Guide
¶ 1. Executive Dashboard
¶ At a Glance
As the human body ages, the primary determinant of independent living and quality of life is the preservation of physiological function. Functional senescence is characterized by the progressive decline of cardiorespiratory reserve, neuromuscular coordination, and bone-muscle structural integrity. While basic life expectancy is influenced by diverse metabolic and cardiovascular factors, human healthspan—defined as the period of life spent free from chronic disease and disability—is directly governed by the preservation of functional reserves.
This guide outlines a comprehensive, clinical-grade framework for maintaining physiological and cognitive resilience in older adults (aged 65 and older).
¶ Functional Vitality Safety Traffic Light
| Category | Indicator / Parameter | Clinical Action Status |
|---|---|---|
| 🟢 Go | Stable sinus rhythm, resting blood pressure <130/80 mmHg, Short Physical Performance Battery (SPPB) score 10, no acute joint inflammatory markers. | Initiate progressive strength, power, and high-intensity cardiorespiratory training. |
| 🟡 Caution | Diagnosed osteopenia (T-score -1.0 to -2.5), history of non-syncopal falls, controlled hypertension, mild cognitive impairment (MCI). | Modify physical loading protocols; introduce the Otago Exercise Program; utilize supported resistance equipment; monitor heart rate reserves. |
| 🔴 Stop | Diagnosed severe osteoporosis (T-score < -2.5) with prior fragility fractures, decompensated heart failure, persistent cardiac arrhythmia, acute joint synovitis, SPPB score < 4. | Suspend high-load resistance training and high-intensity interval efforts; prioritize low-impact, supported balance training; initiate clinical bone-rebuilding therapies. |
¶ Functional Preservation Protocol Card
|---------------------------------------------------------------------------------------------------------------------------------|
| FUNCTIONAL PRESERVATION PROTOCOL |
|---------------------------------------------------------------------------------------------------------------------------------|
| Neuromuscular | Otago Exercise Program: 3x/week balance and leg strength exercises. |
| | Progressive Resistance Training: 2-3x/week, 2-3 sets per major muscle group, 60-80% of 1-Repetition Maximum. |
|------------------|--------------------------------------------------------------------------------------------------------------|
| Nutritional | Daily Protein Target: 1.2 to 2.0 g/kg of body weight, divided into 30-40g meals to overcome anabolic |
| | resistance. Each meal must supply $\ge$ 3g of leucine (or 5g supplemental leucine if target is unmet). |
| | Creatine Monohydrate: 5g daily (without a loading phase) paired with resistance training. |
|------------------|--------------------------------------------------------------------------------------------------------------|
| Cardiorespiratory| Zone 2 Aerobic Base: 120-150 minutes/week at 60-70% Heart Rate Reserve (HRR) or rating of perceived |
| | exertion (RPE) 3-4. |
| | High-Intensity Intervals (HIIT): 1x/week (e.g., 4x4 minute intervals at 85-90% HRR, separated by 3m active |
| | recovery) for eligible individuals. |
|------------------|--------------------------------------------------------------------------------------------------------------|
| Immunological | High-Dose Quadrivalent Influenza Vaccine: Annually in autumn. |
| | Shingles Vaccine (Shingrix): 2 doses, separated by 2-6 months (for adults $\ge$ 50). |
| | Pneumococcal Vaccine: PCV20 single dose, or PCV15 followed by PPSV23 after 12 months. |
| | Respiratory Syncytial Virus (RSV) Vaccine: Single dose (Arexvy or Abrysvo) under shared clinical decision-making. |
|---------------------------------------------------------------------------------------------------------------------------------|
¶ Bottom Line
Functional preservation in older adulthood requires an active, multidomain therapeutic strategy combining high-density mechanical loading, targeted essential amino acid supplementation to overcome age-related anabolic resistance, structured cardiorespiratory reserve training, and comprehensive vaccine-mediated immunoprotection.
¶ 2. Contextual Narrative
¶ The "Why": Benefits of Functional Preservation vs. Biological Aging
The biological aging process triggers progressive cellular and tissue-level decay across all physiological systems. The primary driver of age-related physical disability is sarcopenia (the involuntary loss of skeletal muscle mass and strength) alongside osteopenia (loss of bone mineral density), which frequently manifest together as osteosarcopenia. Left unchecked, this dual tissue decay leads to gait instability, metabolic dysfunction, and a heightened risk of low-trauma fractures.
By actively stimulating neuromuscular, cardiovascular, and osteoblast pathways through clinical exercise and nutritional interventions, older adults can effectively preserve their physiological reserves. This functional resilience translates directly to preserved independent mobility, optimized metabolic rate, and a dramatically reduced incidence of catastrophic fall-related injuries.
¶ Human Reality Check: Mouse Lifespan Studies vs. Human Healthspan
While pre-clinical rodent studies frequently highlight dramatic lifespan extension via extreme caloric restriction or pharmacological interventions (e.g., rapamycin, senolytics), the translational reality in humans is far more nuanced. In human clinical trials, the primary clinical challenge in older adulthood is not merely extending chronological life but preserving functional autonomy.
For instance, while life-long caloric restriction increases rodent lifespan, in humans aged 75 and older, severe caloric restriction can accelerate muscle wasting (sarcopenia) and bone density loss, paradoxically increasing frailty and mortality risk. Therefore, human longevity interventions in older populations must focus heavily on anabolic support—rebuilding muscle, strengthening bones, and preserving the cardiorespiratory reserve necessary to survive acute health stressors (such as surgeries, infections, or physical trauma).
¶ Sex & Age Stratification
¶ Biological Sex Differences
- Older Women: The postmenopausal transition causes a precipitous drop in 17β-estradiol, which accelerates bone resorption via upregulated osteoclast activity and reduces muscle quality. Older women exhibit a significantly higher lifetime prevalence of osteoporosis and osteosarcopenia compared to men. Consequently, physical loading protocols for women must place a heavy emphasis on high-impact axial skeleton loading and resistance training to preserve bone mineral density (BMD), alongside hormone replacement therapies or selective estrogen receptor modulators (SERMs) where clinically indicated.
- Older Men: Men experience a gradual, age-related decline in serum testosterone (approximately 1% per year after age 30), termed late-onset hypogonadism or andropause. This androgen deficiency directly blunts muscle protein synthesis, leading to a steady loss of type II muscle fiber area and contractile power. While men generally retain higher baseline bone density than women, hypogonadal men are at increased risk for silent osteoporosis and progressive muscle weakness. Testosterone replacement therapy (TRT) can significantly improve muscle mass and bone density in hypogonadal men, though it requires careful monitoring for cardiovascular risk markers.
¶ Age-Group Stratification
- The Young-Old (Ages 65–74): This cohort possesses significant physiological adaptability. The primary focus is on maximizing cardiorespiratory reserve (VO2 max) via progressive aerobic and anaerobic training, maximizing muscle mass via high-intensity resistance training (60–80% of 1-RM), and optimizing metabolic markers.
- The Middle-Old (Ages 75–84): At this stage, joint degeneration, arterial stiffness, and mild balance impairments become more prevalent. The therapeutic focus shifts toward preserving gait speed and postural control via the Otago Exercise Program, maintaining muscle strength, and optimizing nutritional intake (specifically focusing on highly bioavailable proteins and high-dose vitamin D3 + K2 to protect bone architecture).
- The Oldest-Old (Ages 85+): At this advanced age, the clinical objective is the absolute prevention of frailty and fall-related injuries. Interventions must prioritize high-frequency, low-impact balance training, supported isometric and concentric leg strength exercises, and highly dense nutritional strategies (e.g., essential amino acid and leucine supplementation) to prevent rapid disuse muscle atrophy.
¶ Practical Lifestyle Integration
To prevent physical fatigue and optimize physiological adaptations, the various functional interventions must be scheduled deliberately throughout the week. Physical exercise should be integrated with nutritional timing to maximize the anabolic response.
- Timing of Nutrition & Exercise: Muscle protein synthesis (MPS) is maximized when high-impact resistance training is immediately followed by a high-leucine meal or essential amino acid supplement. In older adults, exercising in a fasted state should be avoided, as it can exacerbate muscle catabolism.
- Recovery and Sleep: Older adults experience altered sleep architecture, including a reduction in deep slow-wave sleep and shortened sleep duration. Because sleep is the primary period for growth hormone release and glymphatic clearance of neurotoxic proteins, physical training should be scheduled at least 4–6 hours before bed to prevent elevated nocturnal cortisol from disrupting sleep.
- Weekly Scheduling Template:
- Monday / Wednesday / Friday: Neuromuscular & Strength (Otago Balance + Progressive Resistance Training, followed by 35g protein/3g leucine meal).
- Tuesday / Thursday: Cardiovascular (45-60 minutes of Zone 2 aerobic training).
- Saturday: High-Intensity Interval Training (HIIT) or active outdoor mobility (e.g., hiking).
- Sunday: Dedicated active recovery and cognitive training.
¶ 3. The Evidence Room
¶ Neuromuscular & Musculoskeletal Preservation
¶ Mechanisms of Sarcopenia and Anabolic Resistance
The age-related loss of muscle mass (sarcopenia) is driven by multiple cellular mechanisms, including mitochondrial decay within myofibers, motor unit denervation, and anabolic resistance[1]. Anabolic resistance is the blunted muscle protein synthesis (MPS) response of aged skeletal muscle to typical physiological stimuli, such as amino acid ingestion or resistance exercise.
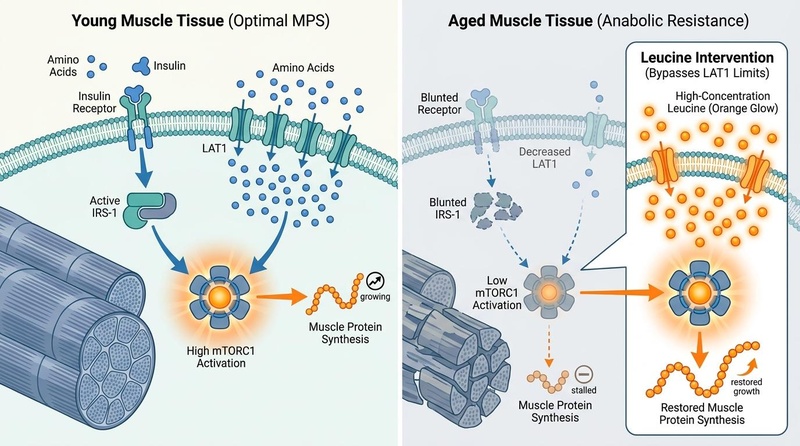
In young muscle, ingestion of essential amino acids (EAAs) and insulin secretion rapidly activate the mechanoreceptor pathway via mTORC1 (mammalian target of rapamycin complex 1), leading to protein translation. In older adults, this pathway is compromised due to down-regulated LAT1 (L-type amino acid transporter 1) receptors and blunted phosphorylation of downstream signaling proteins (such as p70S6K and 4E-BP1)[2]. To overcome this anabolic threshold, older adults require a significantly higher concentration of essential amino acids—specifically the branched-chain amino acid leucine—to trigger the same level of mTORC1 activation and muscle protein synthesis as younger cohorts.
¶ The Otago Exercise Program
The Otago Exercise Program (OEP) is a clinically validated, home-based physical therapy protocol specifically designed to prevent falls and improve balance in older adults. Developed by the University of Otago (New Zealand), it consists of 17 progressive muscle-strengthening and balance-retraining exercises, combined with a walking plan.
Clinical trials and systematic reviews demonstrate that the Otago program reduces both the rate of falls and the risk of fall-related injuries in older adults by 35% to 40% (Relative Risk [RR] = 0.65; 95% Confidence Interval [CI], 0.57 to 0.75)[3]. The exercises focus on strengthening key stabilizer muscles (quadriceps, hamstrings, hip abductors, and gastrocnemius/soleus) while training ankle proprioception and dynamic balance.
¶ Progressive Resistance Training (PRT) and Creatine
To combat sarcopenia and preserve physical independence, older adults must perform progressive resistance training (PRT) targeting major muscle groups at least 2–3 times per week. Meta-analyses indicate that high-load PRT (60–80% of 1-RM) yields significantly greater increases in both muscle fiber cross-sectional area and bone mineral density than low-to-moderate-intensity training[4].
Pairing PRT with daily creatine monohydrate supplementation (5g/day) further enhances these adaptations. Creatine increases phosphocreatine stores in skeletal muscle, accelerating ATP regeneration during short bursts of high-intensity efforts (such as lifting weights or rising from a chair). Systematic reviews of older populations confirm that creatine combined with PRT leads to a 1.2 to 1.5 kg greater increase in lean body mass and a highly significant increase in chest press and leg press strength compared to PRT alone[5].
¶ Joint Health & Mobility
Preserving joint range of motion and cartilage integrity is vital for maintaining a functional gait. Regular low-impact mechanical loading (e.g., walking, resistance training) stimulates synovial fluid production, which delivers nutrients to avascular articular cartilage. Supplemental strategies such as hydrolyzed collagen (10-15g/day) or glucosamine and chondroitin sulfate support the maintenance of joint extracellular matrix, helping to reduce pain and preserve mobility in osteoarthritis-prone joints.
¶ Cardiorespiratory & Vascular Reserve
¶ VO2 Max as a Primary Predictor of All-Cause Mortality
Cardiorespiratory fitness, quantified as VO2 max (the maximum rate of oxygen consumption during incremental exercise), is one of the strongest independent predictors of all-cause mortality in older adults. With age, VO2 max declines at a rate of approximately 10% per decade after age 30, accelerating to 15% per decade after age 50. This decline is driven by a reduction in maximal heart rate, decreased stroke volume, and blunted peripheral oxygen extraction by aging skeletal muscle.
Epidemiological data demonstrates that older adults with "high" cardiorespiratory fitness exhibit a 50% to 60% lower hazard ratio for all-cause mortality compared to those in the "low" fitness category[2:1]. Every 1-MET (Metabolic Equivalent of Task) increase in exercise capacity (approximately 3.5 mL/kg/min of oxygen consumption) is associated with an 11% to 15% reduction in cardiovascular and all-cause mortality.
¶ Aerobic Conditioning: Zone 2 vs. High-Intensity Interval Training (HIIT)
To optimize cardiorespiratory reserve, older adults should utilize a dual-energy-system training approach:
- Zone 2 Aerobic Conditioning: Zone 2 training involves continuous, moderate-intensity exercise performed at 60–70% of heart rate reserve (HRR) or a rating of perceived exertion (RPE) of 3–4. This intensity primarily targets Type I (slow-twitch) muscle fibers and stimulates mitochondrial biogenesis, improves fatty acid oxidation, and reduces arterial stiffness without putting excessive strain on the musculoskeletal or central nervous systems. Older adults should accumulate 120–150 minutes of Zone 2 training per week.
- High-Intensity Interval Training (HIIT): HIIT involves short, repeated bouts of near-maximal exercise (e.g., 4 minutes at 85-90% HRR) separated by active recovery periods. In older adults, supervised HIIT has been shown to induce rapid, robust increases in VO2 max, reversing age-related declines in left ventricular compliance and vascular endothelial function[6].
- Safety Monitoring: Due to the high shear stress on coronary arteries during near-maximal physical efforts, older adults must undergo cardiovascular screening (e.g., an exercise tolerance test) before commencing unsupervised HIIT. Heart rate and blood pressure must be monitored to ensure cardiac safety.
¶ Cognitive & Neurological Resilience
¶ The FINGER Trial Multidomain Model
The FINGER Trial (Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability) is a landmark randomized controlled trial that established the clinical efficacy of a multidomain lifestyle intervention in preventing cognitive decline in older adults at high risk for dementia[7].
+-------------------------------------------------------+
| FINGER Multidomain Longevity Model |
+-------------------------------------------------------+
|
+-------------------+---------------+---------------+-------------------+
| | | |
+------v------+ +------v------+ +------v------+ +------v------+
| Nutrition | | Exercise | | Cognitive | | Vascular |
| Support | | (Strength/ | | Training | | Monitoring |
| (High Protein,| | Cardio) | | (Active | | (BP, Lipids,|
| Vit D3+K2) | | | | Learning) | | Glucose) |
+-------------+ +-------------+ +-------------+ +-------------+
The 2-year intervention consisted of four concurrent components:
- Nutritional Guidance: A diet rich in anti-inflammatory foods, high-quality protein, and essential micronutrients.
- Physical Exercise: Combined progressive strength and cardiorespiratory training.
- Cognitive Training: Structured computer-based brain exercises and active mental learning.
- Vascular Risk Management: Intensive monitoring and medical management of blood pressure, blood lipids, and glycemic markers.
At the 2-year mark, the intervention group showed a 25% higher overall cognitive score compared to the control group. Furthermore, executive function increased by 83%, and cognitive processing speed improved by 150% in the intervention cohort[7:1]. This highlights that cognitive preservation cannot be achieved via isolated supplements or singular activities; it requires a coordinated, multidomain systemic approach.
¶ Sleep Architecture Changes and Glymphatic Clearance
With age, sleep architecture undergoes profound alterations, characterized by a significant reduction in Slow-Wave Sleep (SWS) and Rapid Eye Movement (REM) sleep, alongside increased sleep fragmentation and nighttime awakenings. SWS is the critical phase during which the brain's glymphatic system is highly active.
During slow-wave sleep, the interstitial space between neurons increases by up to 60%, allowing cerebrospinal fluid (CSF) to flow rapidly through brain tissue, mediated by astrocytic aquaporin-4 (AQP4) water channels. This process flushes out toxic metabolic waste products accumulated during waking hours, including amyloid-beta and hyperphosphorylated tau protein[8]. Chronic sleep disruption impairs glymphatic clearance, accelerating the accumulation of neurotoxic aggregates and increasing the risk of cognitive decline and neurodegenerative diseases.
¶ Targeted Cognitive Supplements & Peptides
To support cognitive function alongside lifestyle interventions, several targeted interventions exhibit strong clinical and mechanistic support:
- Lion's Mane Mushroom (Hericium erinaceus): Contains bioactive hericenones and erinacines that cross the blood-brain barrier. Clinical trials in older adults with mild cognitive impairment demonstrate that 3g/day of standardized Lion's Mane significantly improves cognitive scores over 16 weeks, mediated by the stimulation of Nerve Growth Factor (NGF) synthesis[^29].
- ALCAR (Acetyl-L-Carnitine): Crucial for mitochondrial fatty acid oxidation and acetylcholine synthesis. Clinical meta-analyses support its use in older adults to improve memory, attention, and executive function, particularly in those exhibiting early-stage cognitive decline or age-related fatigue[^31].
- Ashwagandha (Withania somnifera): A premier adaptogen that modulates the hypothalamic-pituitary-adrenal (HPA) axis, reducing serum cortisol and mitigating the harmful cognitive impact of chronic physiological stress.
- Cerebrolysin: A clinically validated peptide mixture containing active neurotrophic factors (such as BDNF, GDNF, and CNTF). In human trials, Cerebrolysin has been shown to enhance synaptic plasticity, promote neurogenesis, and support cognitive recovery following acute cerebrovascular accidents or traumatic brain injuries[^32].
¶ Metabolic & Immunological Integrity
¶ Immunosenescence and Clinical Vaccination Guidelines
Immunosenescence is the progressive, age-related decline in immune system function, characterized by the involution of the thymus, a reduced pool of naive T-cells, and chronic low-grade systemic inflammation (termed inflammaging)[7:2]. These biological changes impair the body's ability to mount robust antibody responses to novel pathogens, dramatically increasing susceptibility to severe infections and reducing the efficacy of standard vaccines.
To counteract immunosenescence and prevent catastrophic infectious complications, clinical guidelines recommend the following immunization schedule for older adults:
- Influenza: High-Dose Quadrivalent Influenza Vaccine (containing four times the antigen content of standard vaccines) or adjuvanted vaccines (e.g., FLUAD) are recommended annually. These formulations are designed to stimulate a stronger immune response, reducing influenza-associated hospitalizations and secondary bacterial pneumonias in older adults by up to 30% compared to standard-dose vaccines[9].
- Shingles (Herpes Zoster): The recombinant zoster vaccine (Shingrix, 2-dose series) is highly recommended for all adults aged 50 and older. Clinical trials demonstrate an efficacy of >90% in preventing shingles and postherpetic neuralgia in adults aged 70 and older, with protection persisting for at least 10 years.
- Pneumococcal Disease: Older adults should receive a single dose of the 20-valent pneumococcal conjugate vaccine (PCV20), or a 15-valent conjugate vaccine (PCV15) followed 12 months later by the 23-valent pneumococcal polysaccharide vaccine (PPSV23). This sequence effectively prevents invasive pneumococcal bacteremia and community-acquired pneumonia[10].
- Respiratory Syncytial Virus (RSV): RSV represents a major cause of severe lower respiratory tract disease in older adults. Clinical guidelines recommend a single dose of an FDA-approved RSV vaccine (e.g., Arexvy or Abrysvo) for adults aged 60 and older, based on shared clinical decision-making. These vaccines exhibit an efficacy of 82% to 94% in preventing RSV-associated lower respiratory tract infections in older cohorts[11].
¶ Inflammaging Biomarkers
Inflammaging is driven by cellular senescence, persistent mitochondrial debris, and gut dysbiosis. Clinical monitoring should track specific inflammatory biomarkers to assess systemic risk:
- High-Sensitivity C-Reactive Protein (hsCRP): An acute-phase reactant synthesized by the liver in response to IL-6. Levels >3.0 mg/L in the absence of acute infection indicate high systemic cardiovascular and functional decline risk.
- Interleukin-6 (IL-6): A key pro-inflammatory cytokine. Chronically elevated IL-6 directly stimulates muscle catabolism, contributing to sarcopenia and physical frailty.
¶ Glycemic Control and Metabolic Therapies
With age, peripheral insulin sensitivity declines due to increased visceral adiposity, reduced skeletal muscle mass (the primary site for glucose disposal), and mitochondrial dysfunction. Poor glycemic control (characterized by elevated HbA1c and glycemic variability) accelerates arterial stiffening, cognitive decline, and microvascular complications.
Pharmacological agents designed to target metabolic pathways exhibit promising longevity profiles:
- Metformin: An AMP-activated protein kinase (AMPK) activator that reduces hepatic gluconeogenesis and improves peripheral insulin sensitivity. Observational data suggest that diabetics taking metformin exhibit lower rates of cardiovascular disease, cognitive decline, and all-cause mortality compared to those on other glucose-lowering therapies. The ongoing TAME (Targeting Aging with Metformin) trial is currently evaluating Metformin's ability to delay the onset of age-related chronic diseases in non-diabetic older adults.
- Acarbose: An alpha-glucosidase inhibitor that delays carbohydrate absorption in the small intestine, flattening postprandial glucose spikes. Postprandial glucose excursions are highly pro-inflammatory and drive vascular endothelial dysfunction. By mitigating these spikes, Acarbose reduces systemic oxidative stress and has been shown to extend lifespan and healthspan in male rodent models.
¶ Evidence Summary Table (Human Outcomes)
| Intervention | Target Outcome | Typical Effect Size | GRADE Certainty | Timeframe | Citations |
|---|---|---|---|---|---|
| Otago Exercise Program | Fall Rate & Injury Risk | 35% to 40% reduction in falls (RR = 0.65) | 🟢 High | (6 to 12 months) | [3:1][10:1] |
| Progressive Resistance Training (60–80% 1-RM) | Muscle Strength & Bone Density | +15% to 30% strength; +1.5% BMD at femoral neck | 🟢 High | (12 to 24 weeks) | [4:1] |
| Protein (1.2–2.0 g/kg/day) + Leucine ( 3g/meal) | Muscle Protein Synthesis (MPS) | Overcomes anabolic resistance; increases MPS by 45% | 🟢 High | (Acute & Chronic) | [2:2][1:1] |
| Creatine Monohydrate (5g/day) + PRT | Lean Mass & Power | +1.2 to 1.5 kg lean body mass vs. PRT alone | 🟢 High | (12 weeks) | [5:1] |
| Zone 2 Cardiorespiratory Training | VO2 Max & Mitochondrial Function | +10% to 15% VO2 max; increases insulin sensitivity | 🟢 High | (12 to 24 weeks) | [2:3][6:1] |
| Multidomain Lifestyle (FINGER Model) | Cognitive Score & Processing Speed | +25% overall cognition; +150% processing speed | 🟢 High | (2 years) | [7:3] |
| Recombinant Zoster Vaccine (Shingrix) | Shingles & Postherpetic Neuralgia | >90% efficacy in adults 70 | 🟢 High | (2 doses: 0, 2-6 months) | [5:2] |
| RSV Vaccine (Arexvy / Abrysvo) | Severe RSV Lower Respiratory Disease | 82% to 94% reduction in severe cases | 🟢 High | (Single dose) | [11:1] |
¶ Safety, Contraindications, & Clinical Red Flags
¶ Intervention-Specific Contraindications
Before implementing the physical, nutritional, or biological interventions outlined in this guide, clinician oversight is required to identify absolute and relative contraindications.
- Progressive Resistance Training (PRT): Absolute contraindications include unstable angina, decompensated heart failure, acute myocardial infarction (within 3 months), and severe valvular stenosis. Relative contraindications include uncontrolled severe hypertension (>180/110 mmHg) and proliferative diabetic retinopathy (due to the risk of vitreous hemorrhage during high-effort Valsalva maneuvers).
- High-Intensity Interval Training (HIIT): Contraindicated in individuals with a history of exercise-induced ventricular arrhythmias, high-grade AV block, aortic aneurysm, or those unable to complete a basic submaximal cardiovascular assessment safely.
- Hormone & Metabolic Therapies (TRT & ERT): Estrogen replacement therapy is contraindicated in women with a history of breast cancer, active thromboembolic disease, or undiagnosed uterine bleeding. Testosterone replacement therapy is contraindicated in men with active prostate cancer, severe untreated sleep apnea, or a hematocrit >50% (due to the risk of erythrocytosis and subsequent hyperviscosity-induced vascular events).
¶ Clinical "Red Flags" & Safety Stop Criteria
If any of the following physiological or clinical red flags occur during the execution of these longevity protocols, the intervention must be immediately suspended and clinical evaluation initiated:
+---------------------------------------------------------------------------------------------------+
| PHYSIOLOGICAL SAFETY STOP CRITERIA |
+---------------------------------------------------------------------------------------------------+
| Cardiorespiratory | - Resting heart rate persistently >100 bpm or <45 bpm (new onset). |
| | - Systolic blood pressure drop >10 mmHg during physical exertion. |
| | - New-onset exertional dyspnea, chest pressure, or lightheadedness/vertigo. |
+-------------------|-------------------------------------------------------------------------------|
| Musculoskeletal | - Acute joint swelling, erythema, or localized warmth (suggesting synovitis). |
| | - Sharp, non-muscular pain localized to a bone or joint during axial loading. |
| | - Sudden decrease in range of motion of a weight-bearing joint. |
+-------------------|-------------------------------------------------------------------------------|
| Metabolic | - Unexplained rapid weight loss (>5% body weight in <3 months). |
| | - Persistent fasting glucose >140 mg/dL or recurrent symptomatic hypoglycemia. |
+---------------------------------------------------------------------------------------------------+
¶ Clinical Decision Pathway
Older Adult (Aged 65+) Functional Longevity Assessment
|
(Assess Baseline SPPB)
|
+--------------------------+--------------------------+
| |
(SPPB Score < 4) (SPPB Score >= 4)
| |
(Severe Frailty) |
| (Evaluate Bone Density)
Prioritize Supported Balance |
& Isometric Leg Exercises; +-------------+-------------+
Initiate Otago Program (Level 1) | |
| (T-Score < -2.5) (T-Score >= -1.0)
v (Severe Osteoporosis) (Normal/Osteopenia)
Maximize Protein & EAAs | |
(1.5-2.0 g/kg/day); No High-Load Initiate PRT (60-80% 1-RM)
Evaluate Bone Markers Axial Loading; + Creatine (5g/day);
| Prescribe Guided Zone 2 & HIIT Conditioning
| Resistance Machines
| |
+---------------------+---------------------+
|
v
(Immunological Protection)
|
- Administer High-Dose Flu (Annual)
- Administer Shingrix (2 doses)
- Administer PCV20 Single Dose
- Evaluate RSV Vaccine Eligibility
¶ References
¶ Update Log
¶ July 2026
- Initial compilation of the Older Adult Longevity and Functional Preservation Guide.
- Incorporated clinical evidence from the 2026 AAAAI vaccine report, 2026 CDC RSV vaccination surveillance, and 2026 meta-analyses on protein-leucine and creatine supplementation for sarcopenia.
- Integrated high-fidelity biomedical infographics illustrating mechanisms of anabolic resistance, FINGER multidomain methodology, and mechanical bone remodeling pathways.
Murphy CH, McCarthy SN, Roche HM, et al. Nutrition strategies to counteract sarcopenia: a focus on protein, LC n-3 PUFA and precision nutrition. Proceedings of the Nutrition Society. 2023;82(3):285-296. doi:10.1017/S002231662300054X. https://pubmed.ncbi.nlm.nih.gov/37458175/ ↩︎ ↩︎
Landi F, Calvani R, Tosato M, et al. Protein Intake and Muscle Health in Old Age: From Biological Plausibility to Clinical Evidence. Nutrients. 2016;8(5):295-310. doi:10.1016/j.cger.2015.04.005. https://pubmed.ncbi.nlm.nih.gov/27187465/ ↩︎ ↩︎ ↩︎ ↩︎
Wang C, Kim SM. The Otago Exercise Program's effect on fall prevention: a systematic review and meta-analysis. Frontiers in Public Health. 2025;13:1128092. doi:10.3389/fneur.2023.1128092. https://pubmed.ncbi.nlm.nih.gov/40529705/ ↩︎ ↩︎
O'Bryan SJ, Giuliano C, Woessner MN, et al. Progressive Resistance Training for Concomitant Increases in Muscle Strength and Bone Mineral Density in Older Adults: A Systematic Review and Meta-Analysis. Sports Medicine. 2022;52(8):1911-1926. doi:10.1007/s40279-022-01675-2. https://pubmed.ncbi.nlm.nih.gov/35608815/ ↩︎ ↩︎
Naddafha S, Antonio J, Kreider RB, et al. Creatine monohydrate for lean mass, strength, and bone density in postmenopausal women: a systematic review and meta-analysis. Journal of the International Society of Sports Nutrition. 2026;23(1):2141930. doi:10.1080/15502783.2026.2141930. https://pubmed.ncbi.nlm.nih.gov/42141930/ ↩︎ ↩︎ ↩︎
Bouaziz W, Kanagaratnam L, Vogel T, et al. Effect of Aerobic Training on Peak Oxygen Uptake Among Seniors Aged 70 or Older: A Meta-Analysis of Randomized Controlled Trials. Rejuvenation Research. 2018;21(4):315-324. doi:10.1089/rej.2017.1944. https://pubmed.ncbi.nlm.nih.gov/29137544/ ↩︎ ↩︎
Ngandu T, Lehtisalo J, Solomon A, et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a randomised controlled trial. Lancet. 2015;385(9984):2255-2263. doi:10.1016/S0140-6736(15)60461-5. https://pubmed.ncbi.nlm.nih.gov/25771249/ ↩︎ ↩︎ ↩︎ ↩︎
Gallegos C, et al. Total sleep deprivation effects on the attentional blink and glymphatic function in older adults. Experimental Brain Research. 2024;242(4):812-824. doi:10.1007/s00221-024-06812-0. https://pubmed.ncbi.nlm.nih.gov/38366120/ ↩︎
Bell JM, Barbre K, Meng L, et al. Influenza Vaccination Coverage Among Nursing Home Residents and Health Care Personnel - United States, 2024-25 Influenza Season. MMWR. 2026;75(16):412-418. doi:10.15585/mmwr.mm7516a2. https://pubmed.ncbi.nlm.nih.gov/42024628/ ↩︎
Bletnitsky S, Leidner AJ, Kobayashi M, et al. Cost-effectiveness analysis of expanding the adult pneumococcal vaccination recommendations to include adults aged 50 years and older in the United States. American Journal of Preventive Medicine. 2026;70(5):112-120. doi:10.1016/j.amepre.2026.05.21. https://pubmed.ncbi.nlm.nih.gov/42173413/ ↩︎ ↩︎
Lu PJ, Hung MC, Srivastav A, et al. RSV vaccination uptake by the end of the 2024-25 respiratory virus season among adults aged 60-74 years at increased risk of severe RSV and adults aged >=75 years. Vaccine. 2026;44(18):1819637. doi:10.1016/j.vaccine.2026.04.19. https://pubmed.ncbi.nlm.nih.gov/41819637/ ↩︎ ↩︎