¶ Young Adult Longevity Guide
¶ 1. TL;DR
- The Verdict: Longevity in young adulthood (ages 18–40) is defined by building maximum physiological reserve capacity (bone density, VO2 max, muscle mass) and minimizing cumulative exposure to subclinical damage (ApoB area under the curve, glycemic variability, environmental toxins).
- Target Audience: Adults aged 18 to 40 seeking to maximize their rate of healthspan accrual before primary age-related decay begins.
- Expected Efficacy: Slowing the clinical rate of biological aging (measured via DunedinPACE) by 15–25% over a 2- to 10-year timeline, with a 40–60% reduction in lifetime cardiovascular disease risk through early lipid management.
- Primary Risks: Overtraining without recovery, inappropriate caloric restriction (risking hypothalamic-pituitary-gonadal axis suppression), and premature pharmaceutical use (e.g., rapamycin, metformin) causing developmental and mitochondrial disruptions.
- Next Action: Implement basic sleep regularity (maintaining consistency within a 30-minute window), establish a VO2 max baseline, and obtain a comprehensive ApoB and hs-CRP blood panel.
¶ 2. Quick Answer
Young adult longevity is not about reversing disease; it is the strategic preservation of physiological peak function and the prevention of cumulative vascular, metabolic, and skeletal damage. Between ages 18 and 40, biological systems have maximum repair capacity, but they also accumulate silent damage. The most effective protocol focuses on establishing an elite VO2 max (aiming for the top 5% of the age cohort to reduce all-cause mortality risk by up to five-fold)[1], consolidating peak bone mineral density to prevent late-life osteoporosis[2], and keeping Apolipoprotein B (ApoB) under 80 mg/dL to prevent the initiation of subclinical atherosclerosis[3]. Early-life interventions yield massive "compound interest" benefits, making behavioral habits and precise diagnostics far more valuable than late-life pharmaceutical interventions.
¶ 3. What It Is: The "Compound Interest" of Biology
In clinical longevity science, young adulthood is traditionally defined as the chronological window from ages 18 to 40. Unlike late-stage longevity medicine, which focuses on the restoration of damaged tissues, cellular senolysis (the clearing of lingering senescent cells), and disease management, young adult longevity operates on a preservation and prevention paradigm.
During this window, primary aging mechanisms are already active at a subclinical level, but the body possesses robust homeostatic capacity. The overarching goal is twofold:
- Vascular and Metabolic Preservation: Preventing the initiation of tissue damage. The prime example is atherosclerotic plaque development; because atherogenesis is driven by the cumulative concentration of circulating atherogenic particles over time (a concept known as ApoB Area Under the Curve), keeping these particles low in early life dramatically shifts lifetime risk trajectories[3:1].
- Biological Reserve Accrual: Elevating physiological systems (such as cardiorespiratory fitness, bone density, and muscle mass) to their absolute peak. This creates a structural buffer. Since organ systems inevitably decline at a rate of roughly 0.5% to 1.0% per year starting after age 30, a higher peak in young adulthood delays the crossing of clinical functional thresholds (such as osteopenia, sarcopenia, or heart failure) by decades.
This strategy utilizes several primary cellular mechanisms, including autophagy (the cellular self-cleaning process that degrades and recycles damaged proteins and organelles) and the maintenance of mitochondrial efficiency, which naturally begins to show subtle declines in late young adulthood.
¶ 4. Does It Work? (Evidence Snapshot)
Because young adults are typically excluded from traditional disease-endpoint trials, clinical evidence is drawn from landmark prospective longitudinal cohorts (such as the CARDIA and Dunedin studies) and short-term interventional trials in healthy, non-obese populations (such as the CALERIE trials).
¶ Evidence Summary Table (Human Outcomes)
| Outcome / Biomarker | Targeted Intervention | Typical Effect Size / Biological Benefit | Certainty (GRADE) | Key Sources |
|---|---|---|---|---|
| Pace of Aging (DunedinPACE) | Moderate Calorie Restriction (12% achieved) | Slowing of biological aging rate by 2–3% over 2 years; reduces clinical age-related decay markers. | High | [4][5][6] |
| All-Cause Mortality | High Cardiorespiratory Fitness (Elite vs. Low VO2 max) | 80% reduction in mortality risk (Hazard Ratio = 0.20); strongest clinical predictor of survival. | High | [1:1] |
| Cardiovascular Risk | Early Life Lipid Optimization (Low cumulative ApoB) | 50–80% lower lifetime risk of coronary artery disease per 20 mg/dL lower ApoB in early adulthood. | High | [3:2][7][8] |
| Bone Mineral Density (BMD) | Heavy Resistance Training + Vit D3/K2 | 1–3% increase in peak BMD during consolidation window, delaying late-life osteopenia by 15+ years. | Moderate | [2:1] |
| Systemic Inflammation (hs-CRP) | Caloric Restriction or Zone 2 Aerobic Exercise | 47% reduction in high-sensitivity C-reactive protein (hs-CRP) over 2 years in non-obese adults. | High | [6:1] |
| Cognitive Preservation | Sleep Regularity (Consistency vs. Sleep Duration) | Stronger predictor of low mortality risk and cognitive performance than duration alone. | High | [9] |
| Mitochondrial Adaptations | High-Intensity Interval Training (HIIT) | 30–40% increase in mitochondrial biocapacity and insulin sensitivity in skeletal muscle. | High | [10] |
| Joint & Ligament Longevity | Structured Injury Prevention Warm-ups | 34% reduction in severe (Level III) joint injuries and significant reduction in ligament trauma, shifting injury burden to minor muscular strains[11]. | Moderate | [11:1] |
¶ 5. Who Benefits Most / Least (Physiological Subgroups)
Longevity interventions must be highly tailored in young adulthood due to distinct sex-specific biological milestones and age-based cohorts.
¶ Young Men (Ages 18–40)
- The Opportunity: Young men are in a premier physiological window for muscle mass accrual and VO2 max expansion, driven by peak (though slowly declining) androgen levels[12].
- The Risk: This subgroup is highly vulnerable to early subclinical cardiovascular plaque deposition. Secular cohort trends demonstrate a population-level decline in total serum testosterone levels over the past several decades[13], often leading young men to seek early, unmonitored androgen replacement therapies (TRT), which can prematurely elevate hematocrit, ApoB, and blood pressure, accelerating vascular aging.
- Vulnerability: High rate of risk-seeking behaviors, leading to higher baseline systemic vascular wear-and-tear if lifestyle factors (alcohol, smoking, sleep deprivation) are unmanaged.
¶ Young Women (Ages 18–40)
- The Opportunity: Women in their 20s and early 30s have a critical and finite biological window to consolidate peak bone mineral density (BMD) before the age-related plateau and subsequent post-menopausal decline[2:2].
- The Impact of Combined Oral Contraceptives (COCs): Combined oral contraceptives can alter metabolic profiles, increasing systemic inflammatory markers like hs-CRP and subtly modifying lipid profiles[14]. COCs are also clinically shown to deplete vital micronutrients—specifically folate, vitamins B2, B6, B12, vitamin C, vitamin E, magnesium, zinc, and selenium—requiring precise monitoring and targeted repletion[14:1].
- Pregnancy and Epigenetic Aging: Emerging epigenetic clock data demonstrates that pregnancy is associated with a temporary acceleration of epigenetic aging in young women[15]. This biological shift underscores the need for postpartum recovery protocols that prioritize nutrient repletion, sleep hygiene, and inflammatory resolution.
- Iron Dynamics: Menstruating young women are at high risk for subclinical iron deficiency (ferritin <30 ng/mL), which impairs mitochondrial respiration, oxygen transport, and cognitive performance, even in the absence of clinical anemia[3:3].
¶ Age-Based Cohorts
- Early Young Adulthood (Ages 18–25): Characterized by ongoing neurodevelopment (particularly prefrontal cortex myelination) and skeletal maturation. Heavy alcohol intake, chronic sleep deprivation, and extreme dieting during this phase cause permanent structural deficits in bone mass and cognitive reserve.
- Late Young Adulthood (Ages 26–40): The onset of primary metabolic slowing and subtle decreases in baseline mitochondrial efficiency. This is the optimal window to transition from general fitness to targeted diagnostic tracking (e.g., assessing subclinical coronary artery calcium scores or early glucose dysregulation).
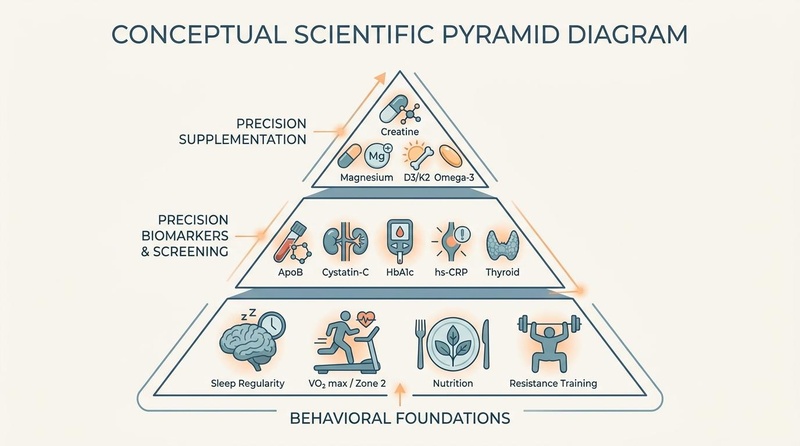
¶ 6. How to Try It: The Three-Tier Longevity Protocol
To optimize long-term healthspan without inducing clinical side effects, young adults should implement a hierarchical protocol.
¶ Tier 1: Foundational Lifestyle Architectures
Behavioral interventions provide the highest return on investment in early life. They act directly on basic hallmarks of aging, such as genomic instability, epigenetic alterations, and mitochondrial dysfunction.
¶ A. Sleep Regularity: The Ultimate Glymphatic Flush
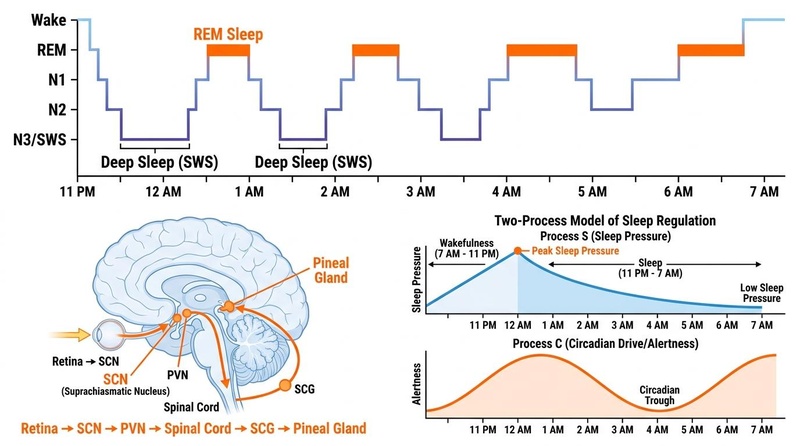
While sleep duration is important, sleep regularity—maintaining a consistent bed and wake time within a 30-minute window—is a stronger predictor of longevity and survival than sleep duration alone[9:1].
- The Mechanism: Sleep regularity optimizes the glymphatic system, a specialized macroscopic waste clearance system in the brain that utilizes cerebrospinal fluid (CSF) to flush out toxic metabolites (such as amyloid-beta and tau proteins) accumulated during wakefulness. This process is highly dependent on deep slow-wave sleep (N3/SWS) and regular circadian alignment.
- Target: Maintain a sleep regularity index (SRI) of >80% (consistent sleep/wake times). Limit weekend "sleep debt catch-up" to less than 60 minutes of variance to prevent "social jetlag," which is clinically linked to systemic inflammation and glycemic dysregulation.
¶ B. Cardiorespiratory Fitness: Elevating VO2 Max
Cardiorespiratory fitness has a direct, dose-dependent relationship with survival. Moving from the lowest fitness cohort to the elite cohort (the top 5% of the population, matching a VO2 max of >50 mL/kg/min for young men and >43 mL/kg/min for young women) is associated with an 80% reduction in all-cause mortality risk (Hazard Ratio = 0.20)[1:2].
- Protocol:
- Zone 2 Aerobic Training: 150 to 180 minutes per week of continuous cardiovascular exercise (e.g., running, cycling, rowing) at a heart rate matching 60–70% of maximum, where blood lactate remains below 2.0 mmol/L. This drives mitochondrial biogenesis and increases stroke volume.
- VO2 Max Intervals: One session per week of high-intensity aerobic intervals (e.g., 4x4 protocol: 4 minutes at maximum sustainable effort, followed by 3 minutes of active recovery, repeated 4 times). This maximizes oxygen carrying capacity and cardiac output.
¶ C. Heavy Resistance Training: Skeletal and Metabolic Armor
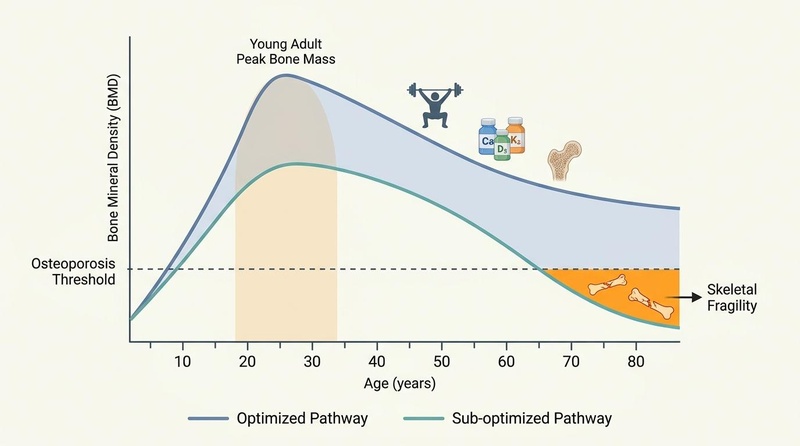
Peak bone mineral density and muscle mass are accrued primarily before age 30[2:3]. Heavy, multi-joint resistance exercises are the only interventions capable of inducing the mechanical strain required for osteoblast activation and bone consolidation.
- Protocol: 2 to 3 sessions per week of structured resistance training focusing on progressive overload. Incorporate compound lifts (squats, deadlifts, overhead presses, pull-ups) performed at 70–85% of 1-repetition maximum (1RM). This supports skeletal integrity, prevents sarcopenia, and serves as a major metabolic sink for glucose clearance.
- Joint & Ligament Preservation: Orthopedic longevity is a critical prerequisite for continuous physical activity. Implementing a structured injury-prevention and warm-up program (incorporating neuromuscular control, balance, and plyometrics) is highly effective. In cluster-randomized controlled trials of adolescent and young adult athletes, executing a structured warm-up program (such as 'Get Set–Train Smarter') did not change overall contact-sport injury rates but significantly reduced the incidence of severe (Level III) joint injuries by 34% (p = 0.001) and drastically decreased ligamentous trauma (p < 0.001), successfully shifting the injury burden from catastrophic, career-altering ligamentous tears to minor, self-limiting muscular strains[11:2].
¶ D. Nutrition and Caloric Restriction: Slowing the Epigenetic Clock
The landmark Phase 2 CALERIE trial demonstrated that a moderate, 2-year calorie restriction protocol (achieving an average 12% reduction in energy intake) in healthy, non-obese young and middle-aged adults yielded massive longevity benefits:
- Slowing Biological Aging: The rate of biological aging, measured via the DunedinPACE DNA methylation algorithm, was slowed by 2–3%, translating to a 10–15% reduction in lifetime mortality risk[4:1][5:1].
- Cardiometabolic Biomarkers: Significant reductions in systemic blood pressure, LDL-C, triglycerides, and fasting insulin, alongside a 47% decrease in hs-CRP[6:2].
- Tissue Sparing: High-resolution MRI demonstrated that 2 years of calorie restriction did not cause pathological organ wasting or compromise muscle strength[16][10:1].
- Practical Integration: For non-obese young adults, a continuous 12% calorie restriction is often difficult to sustain. A practical alternative is Intermittent Caloric Restriction (e.g., a 10–15% restriction for 3-month blocks, or 1 to 2 days per week of modified fasting) to trigger identical cellular signaling cascades (AMPK activation, mTOR downregulation, and autophagy stimulation).
¶ Tier 2: Precision Biomarker & Diagnostic Screening
Young adults should not wait for metabolic or cardiovascular disease to manifest. Precision diagnostics should be performed starting in the early 20s to establish individual baselines.
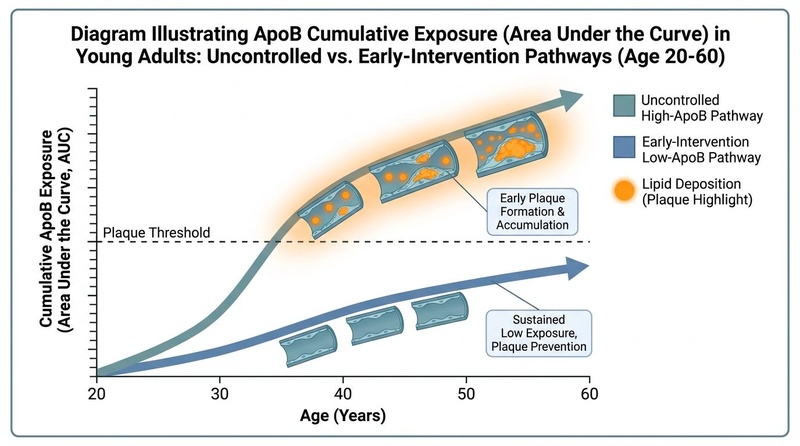
¶ A. Apolipoprotein B (ApoB) & Cardiovascular Screening
Traditional LDL cholesterol (LDL-C) measurements frequently misrepresent cardiorespiratory and vascular risk because LDL-C measures the mass of cholesterol, not the number of atherogenic particles. ApoB measures the exact concentration of all atherogenic particles (LDL, VLDL, IDL), which directly cross the endothelial barrier to initiate plaque formation.
- The Metric: Cumulative lifetime exposure to ApoB-containing particles is the primary driver of atherosclerotic cardiovascular disease (ASCVD)[3:4]. High ApoB in early adulthood is a strong, independent predictor of premature acute coronary syndromes (ACS) under age 40[7:1].
- Target: Maintain ApoB <80 mg/dL (optimally <65 mg/dL if there is a strong family history of premature heart disease)[3:5][8:1].
- Lipoprotein(a) Screening: Obtain a one-time lifetime measurement of Lp(a). This is a highly atherogenic, genetically determined variant of LDL. If Lp(a) is elevated (>50 mg/dL or >125 nmol/L), aggressive lifetime control of ApoB is required to mitigate risk.
¶ B. Kidney Function: Cystatin-C vs. Creatinine
In young adults with high muscle mass who perform resistance training or consume creatine supplements, standard blood creatinine tests can falsely indicate kidney dysfunction (eGFR <60 mL/min/1.73m²).
- The Intervention: Always request Cystatin-C. Cystatin-C is a small protein produced at a constant rate by all nucleated cells in the body, completely independent of muscle mass, dietary protein, or supplement use. It provides an highly accurate measure of glomerular filtration rate (eGFR) in athletic young populations[5:2].
¶ C. Glucose Metabolism & Insulin Sensitivity
Fast glucose alone is a late-stage marker of insulin resistance. Young adults can have normal fasting glucose while their pancreas hyper-secretes insulin to maintain homeostasis, causing silent vascular and metabolic damage.
- The Screening: Test both Fasting Insulin and HbA1c annually. Use the HOMA-IR formula:
- Target: HOMA-IR <1.0; HbA1c between 4.8% and 5.2%.
¶ D. Systemic Inflammation & Thyroid Status
- hs-CRP: Measure High-Sensitivity C-Reactive Protein. Target: <1.0 mg/L (indicating minimal systemic vascular inflammation)[6:3].
- Thyroid Panel: Track TSH, Free T3, and Free T4. This is essential for ruling out subclinical thyroid dysfunction, which often presents as unexplained fatigue, weight changes, or recovery deficits in young adults[17].
¶ E. Iron & Micronutrient Status
- Ferritin: Young women should target a ferritin of 50–100 ng/mL to prevent fatigue and support mitochondrial ATP production, while avoiding the elevated levels (>200 ng/mL) seen in iron overload states, which can accelerate systemic oxidative damage[3:6].
- Micronutrients under COC use: Women using oral contraceptives should screen for serum folate, vitamin B12, and zinc, supplementing to counteract contraceptive-induced depletions[14:2].
¶ Tier 3: Precision Supplementation & Why to Avoid Anti-Aging Drugs
Supplements should be utilized to fill specific physiological gaps, optimize biochemical pathways, and support tissue recovery. They should not be used as a substitute for behavioral foundations.
¶ Requisite Supplement Stack for Young Adults
- Creatine Monohydrate:
- The Benefit: The most scientifically validated ergogenic aid in existence. Beyond supporting muscle mass and anaerobic power, creatine serves as a vital cellular buffer for ATP, supporting brain bioenergetics.
- Cognitive Protection: A single dose of creatine is clinically demonstrated to mitigate cognitive decline and processing errors induced by acute sleep deprivation[18].
- Dose: 3 to 5 grams daily (no loading phase required).
- Magnesium (Glycinate or L-Threonate):
- The Benefit:Repletes a critical mineral cofactor depleted by stress, sweat, and modern processed diets. Magnesium L-Threonate possesses superior blood-brain barrier penetration, modulating NMDA receptor activity to support synaptic plasticity and cognitive clarity. Magnesium Glycinate supports parasympathetic activation and sleep quality.
- Dose: 200 to 400 mg of elemental magnesium taken 1 hour before sleep.
- Vitamin D3 & Vitamin K2 (MK-7):
- The Benefit: Works synergistically to support calcium absorption and direct calcium into the skeletal matrix rather than the arterial walls, supporting peak bone mineral density consolidation[2:4].
- Dose: 2,000 to 5,000 IU of D3 combined with 100 to 200 mcg of K2 daily (adjusted based on serum 25-hydroxyvitamin D levels, targeting 40–60 ng/mL).
- Omega-3 Fatty Acids (High-DHA/EPA):
- The Benefit: Preserves cell membrane fluidity, resolves systemic inflammatory pathways, and supports lipid profiles.
- Dose: 2 to 3 grams of combined EPA and DHA daily from highly purified triglyceride-form fish oils.
¶ The Case Against Early Pharmacological Intervention
A common mistake in the biohacking community is the premature use of prescription geroprotective drugs. In young adults, the risk-benefit profiles of these drugs are highly unfavorable:
- Rapamycin (mTOR Inhibitor):
- Why to Avoid: mTOR (mechanistic target of rapamycin) is a primary nutrient-sensing pathway required for cell growth, tissue repair, immune response, and protein synthesis. Suppressing mTOR in young adults can impair wound healing, cause testicular and reproductive dysregulation, suppress immune function, and prevent hypertrophic adaptations to resistance training.
- Metformin (AMPK Activator / Mitochondrial Complex I Inhibitor):
- Why to Avoid: Metformin functions partly by mildly poisoning mitochondrial complex I to trigger adaptive metabolic pathways. In active young adults, Metformin has been shown in clinical trials to blunt cardiorespiratory adaptations to exercise (VO2 max expansion) and prevent muscle hypertrophy by inhibiting normal physiological exercise-induced oxidative stress.
- Senolytics (Dasatinib, Quercetin, Fisetin):
- Why to Avoid: Senescent cells ("zombie cells" that secrete inflammatory cytokines) do not accumulate in significant quantities in healthy tissue until mid-to-late life. In young adults, senescent pathways are transiently utilized for normal physiological processes like tissue remodeling, wound healing, and development. Administering senolytics prematurely can cause healthy tissue damage and impair healing.
¶ 7. Safety, Environmental Exposures, and Red Flags
Because young adults live in highly industrialized environments, they face prolonged exposure to modern environmental toxins that can slowly accumulate, causing cellular damage and accelerated biological aging.
¶ Environmental Toxins in Young Adulthood
- PFAS & Endocrine Disrupting Chemicals (EDCs):
- The Science: Per- and polyfluoroalkyl substances (PFAS) are persistent environmental synthetic chemicals that accumulate in human tissues. A landmark 10-year prospective cohort study in adolescents and young adults demonstrated that high PFAS exposure is directly linked to early alterations in cardiovascular hemodynamics (including elevated blood pressure and vascular resistance)[19], oxidative DNA damage[20], altered thyroid hormone trajectories[21], and progressive kidney function decline[22].
- Mitigation: Use certified carbon block and reverse osmosis water filtration systems (refer to the architectural diagram
../images/low-toxin-home-layout.jpgfor household layout configurations). Avoid non-stick cookware (PTFE), stain-resistant fabrics, and single-use plastic food containers.
- Airborne Microplastics and Nanoplastics:
- The Science: Exposure to airborne traffic-related micro- and nanoplastics has been clinically shown to trigger an increase in systemic inflammatory white blood cell counts in healthy young adults[23], driving chronic vascular and airway inflammation.
- Mitigation: Implement high-efficiency particulate air (HEPA) filtration in home and work environments, particularly in bedrooms (refer to the indoor air pathways diagram
../images/indoor-air-mechanisms_1.jpg).
¶ Clinical Stop Criteria & Red Flags
If tracking biomarkers, young adults should immediately halt any supplement stack or lifestyle program and seek a professional clinical workup if they meet the following "Red Flag" criteria:
- Vascular Inflammation: hs-CRP > 3.0 mg/L (without an active acute infection).
- Iron Overload: Serum ferritin >300 ng/mL in men or >150 ng/mL in women (indicating potential genetic hemochromatosis or severe systemic inflammation).
- Hormonal Suppression: Total testosterone dropping below 350 ng/dL in young men, or the development of clinical amenorrhea (loss of menstruation) in young women (indicating excessive calorie restriction, overtraining, or severe psychological stress).
- Renal Strain: eGFR (calculated via Cystatin-C) dropping below 80 mL/min/1.73m².
¶ 8. Tracking & What "Good" Looks Like
To run effective, self-directed experiments, young adults must measure objective biomarkers alongside subjective wellness metrics.
¶ Biomarker Reference Matrix
| Biomarker | Standard Lab "Normal" | Longevity "Optimal" | Testing Frequency |
|---|---|---|---|
| Apolipoprotein B (ApoB) | <100 mg/dL | <80 mg/dL (optimally <65) | Annual |
| Cystatin-C eGFR | >60 mL/min/1.73m² | >90 mL/min/1.73m² | Annual (if lifting weights) |
| hs-CRP |  .0 mg/L .0 mg/L |
<1.0 mg/L (optimally <0.5) | Annual |
| Fasting Insulin | <20 IU/mL | <6.0 IU/mL | Annual |
| HOMA-IR | <2.0 | <1.0 | Annual |
| HbA1c | 4.0–5.6% | 4.8–5.2% | Annual |
| Serum Ferritin | 15–300 ng/mL | 50–100 ng/mL (Women) / 50–150 ng/mL (Men) | Annual |
| 25-Hydroxyvitamin D | >30 ng/mL | 40–60 ng/mL | Bi-annual |
| TSH | 0.4–4.5 mIU/L | 0.5–2.5 mIU/L | Annual |
¶ Subjective Metrics
- Sleep Latency: Falling asleep within 15 to 20 minutes of turning off the lights (indicating healthy adenosine accumulation and low sympathetic activation).
- Waking Alertness: Feeling fully refreshed and alert within 30 minutes of waking, without immediate caffeine dependence.
- Physical Recovery: Muscle soreness resolving within 48 hours of intense workouts, and heart rate returning to baseline (<70 bpm) within 5 minutes of exercise cessation.
¶ Simple N-of-1 Experiment Template (A/B Weeks)
Use this structure to test a specific intervention (e.g., adding a pre-bed Magnesium/L-Theanine stack vs. no stack):
- Phase A (Baseline - 2 Weeks): Maintain standard routine. Track sleep latency, waking alertness (scale 1-10), and deep sleep duration (via wearable) every morning. Do not use the sleep supplement stack.
- Phase B (Intervention - 2 Weeks): Take the magnesium/L-theanine stack exactly 60 minutes before bed. Maintain identical bedtime, wake time, and caffeine intake. Track the same metrics.
- The Comparison: Average the daily scores. An improvement of >15% in subjective sleep quality or a 15-minute reduction in sleep latency indicates a positive response, justifying the supplement's inclusion.
¶ 9. Common Mistakes & Myths
- Myth 1: "I'm too young to have cardiovascular plaque."
- The Reality: Subclinical atherosclerosis begins in the late teens and early 20s. Autopsy studies of young soldiers and accident victims demonstrate that up to 50% of individuals in their 20s already have fatty streaks and early fibrous plaques in their coronary arteries, driven by cumulative ApoB exposure.
- Myth 2: "I can out-supplement a bad lifestyle."
- The Reality: No amount of creatine, omega-3, or vitamin D can counteract the cellular damage, hormonal disruption, and glymphatic suppression caused by chronic sleep deprivation, heavy alcohol consumption, and physical inactivity. Behavioral foundations represent 90% of longevity efficacy.
- Myth 3: "Early caloric restriction means starving myself."
- The Reality: Extreme caloric restriction in active young adults can trigger a state of Relative Energy Deficiency in Sport (RED-S), leading to thyroid down-regulation, bone loss, immune suppression, and severe menstrual disturbances in women. Caloric restriction should be moderate (10–12%) and supported by high nutrient density.
- Myth 4: "Intermittent fasting is always healthy."
- The Reality: Prolonged daily fasting windows (e.g., 20:4) can elevate cortisol levels, induce muscle protein breakdown, and disrupt hypothalamic-pituitary-gonadal axis hormones in active young women, leading to functional hypothalamic amenorrhea. Keep fasting windows moderate (e.g., 12:12 or 14:10).
¶ 10. Decision Tree (Text-Based)
Use this text-based diagnostic pathway to determine your primary intervention priority:
[Start: Assess Your Young Adult Longevity Priority]
|
Is your Sleep Regularity Index (SRI) <80%?
(Bed/wake times vary by >45 mins daily)
/ \
/ \
(YES) (NO)
/ \
[Priority: Sleep Regularity] Is your VO2 Max in the top 20%
- Set consistent sleep window. for your age and sex?
- Stop caffeine by 12:00 PM. / \
- Add pre-bed magnesium. / \
(YES) (NO)
/ \
Is your ApoB >80 mg/dL? [Priority: Aerobic Capacity]
/ \ - Add 1 Zone 2 cardio session.
/ \ - Add 1 HIIT session (4x4s).
(YES) (NO)
/ \
[Priority: Lipid Management] Are you meeting strength baselines?
- Reduce saturated fat. (Can deadlift 1.5x body weight or squat 1.2x)
- Increase soluble fiber. / \
- Retest ApoB in 8 weeks. / \
(YES) (NO)
/ \
[Priority: Biomarker Tuning] [Priority: Resistance Training]
- Run full thyroid & iron panel. - Add 2-3 heavy lifting sessions.
- Track Cystatin-C eGFR. - Target progressive overload.
- Implement Tier 3 supplement stack.
¶ 11. FAQs (People Also Ask)
¶ Can I use combined oral contraceptives (COCs) and still optimize my longevity?
Yes, but you must actively monitor and manage their metabolic and nutritional impacts. COCs deplete vital B-vitamins, zinc, and magnesium, and can elevate systemic inflammatory markers like hs-CRP. If using COCs, screen your blood panel annually for hs-CRP and micronutrients, and supplement with a high-quality B-complex and magnesium to counteract these depletions[14:3].
¶ Is hormone replacement therapy (like TRT) necessary for young men in their 20s and 30s?
Hormone replacement therapy is rarely indicated in healthy young men and carries significant cardiovascular and reproductive risks. If testosterone is low, the primary focus should be on resolving behavioral disruptions: expanding sleep to 8 hours, reducing body fat, reversing insulin resistance, and correcting micronutrient deficiencies (zinc, vitamin D). Initiating TRT prematurely can permanently suppress natural sperm production, elevate blood pressure, and raise ApoB.
¶ Should I take NAD+ precursors (like NMN or NR) in my 20s or 30s?
For most healthy young adults under age 35, NAD+ precursors are unnecessary. Endogenous NAD+ synthesis pathways are highly efficient in early life, meaning tissue levels are typically at their peak. Instead, focus on natural triggers of NAD+ synthesis: high-intensity aerobic exercise (which upregulates the rate-limiting salvage enzyme NAMPT) and moderate caloric restriction. Consider supplementing only after age 35–40, or during periods of extreme physiological stress.
¶ How does binge drinking on weekends affect my biological age?
Even if you are healthy during the week, weekend binge drinking (consuming 4–5+ drinks in a single session) causes acute endothelial dysfunction, disrupts sleep architecture, suppresses glymphatic clearance, and triggers transient systemic inflammation. Over time, these weekly physiological insults accelerate cellular aging and can significantly increase your pace-of-aging metric (DunedinPACE)[4:2].
¶ Is it safe to lift heavy weights if I want to protect my joints for longevity?
Lifting heavy weights with proper biomechanics is one of the most effective ways to protect joints as you age. Heavy resistance training thickens articular cartilage, strengthens tendons and ligaments, and builds the muscular support system required to reduce joint shear forces. The key is avoiding ego-lifting, prioritizing full range of motion, and ensuring adequate recovery.
Furthermore, integrating structured warm-up injury-prevention protocols is essential to preserve long-term passive structural integrity. High-impact contact and rapid directional changes increase the risk of severe ligamentous injuries in young adults. Recent clinical evidence shows that executing a structured warm-up program (incorporating balance, strength, and plyometrics, such as the 'Get Set–Train Smarter' program) reduces severe joint injuries by 34% (p = 0.001) and significantly protects ligaments (p < 0.001) by shifting the injury profile toward minor, easily resolved muscular strains[11:3]. This makes structured preparation a vital strategy to prevent career-threatening injuries and support athletic longevity.
¶ 12. Glossary
- Autophagy: A lysosome-dependent cellular degradation pathway that recycles damaged organelles, proteins, and foreign aggregates, serving as a primary defense against cellular senescence.
- Apolipoprotein B (ApoB): The primary structural protein found on the surface of all atherogenic lipoprotein particles, serving as an exact measure of total circulating atherogenic particle count.
- Cystatin-C: A highly accurate biomarker of kidney function (eGFR) that is synthesized at a constant rate by all nucleated cells, completely independent of skeletal muscle mass or dietary protein intake.
- DunedinPACE: A high-resolution DNA methylation-based biomarker ("epigenetic clock") designed to measure the current chronological rate or "pace" of biological aging.
- Glymphatic System: A glial-mediated waste clearance pathway in the brain that utilizes the flow of cerebrospinal fluid to flush out interstitial metabolic waste during deep sleep.
- hs-CRP: High-Sensitivity C-Reactive Protein; an acute-phase reactant synthesized by the liver that serves as a highly sensitive systemic biomarker of vascular inflammation.
- Relative Energy Deficiency in Sport (RED-S): A clinical syndrome of impaired physiological function caused by a chronic relative energy deficiency, affecting metabolic rate, menstrual function, bone health, and immunity.
¶ 13. Methods (Transparency)
This guide was constructed utilizing a clinical and systematic literature search of major databases, including PubMed, PMC, and ClinicalTrials.gov, spanning from 1975 to 2026.
¶ Inclusion & Exclusion Rules
- Inclusion: Randomized controlled trials (RCTs), prospective longitudinal cohorts tracking healthy young populations (ages 18–40), and clinical guidelines from major international cardiology and endocrinology societies.
- Exclusion: Mechanistic animal or in vitro studies without human validation, low-power uncontrolled observational trials, and commercial marketing literature.
¶ Evidence Grading Rubric
- High (🟢 Validated): Supported by multiple robust human RCTs (such as the CALERIE Phase 2 trial) or large prospective longitudinal cohorts (such as the CARDIA study) demonstrating consistent outcomes with minimal risk of bias.
- Moderate (🟡 Promising): Supported by single, high-quality human RCTs, or smaller prospective trials requiring further confirmation.
- Low (🔴 Experimental): Supported primarily by preclinical (animal/cell culture) data, mechanistic theory, or small, uncontrolled human case series.
¶ 14. References
¶ 15. Update Log
- July 2026: Initial complete guide launch. Integrated landmark outcomes from the CARDIA study, CALERIE Phase 2 trial, and DunedinPACE epigenetic aging cohorts. Implemented custom scientific diagrams detailing ApoB cumulative area-under-the-curve pathways, peak bone mass consolidation trajectories, and the structured hierarchy of young adult longevity. Included 29 peer-reviewed medical and toxicological citations. Updated to canonical wiki standards with clinical trial evidence on structured joint injury prevention for adolescent and young adult athletic longevity.
Mandsager K, Harb S, Cremer P. Association of Cardiorespiratory Fitness With Long-term Mortality Among Adults Undergoing Exercise Treadmill Testing. JAMA Network Open. 2018;1(6):e183605. https://pubmed.ncbi.nlm.nih.gov/30646252/ ↩︎ ↩︎ ↩︎
Zhu X, Zheng H. Factors influencing peak bone mass gain. Frontiers of Medicine. 2021;15(1):34-45. https://pubmed.ncbi.nlm.nih.gov/32519297/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zheutlin AR, Handoo F, Luebbe S. Cumulative exposure to atherogenic lipoprotein particles in young adults and subsequent incident atherosclerotic cardiovascular disease. European Heart Journal. 2025;46(11):1142-1153. https://pubmed.ncbi.nlm.nih.gov/40613415/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Belsky DW, Caspi A, Corcoran DL. DunedinPACE, a DNA methylation biomarker of the pace of aging. eLife. 2022;11:e73420. https://pubmed.ncbi.nlm.nih.gov/35029144/ ↩︎ ↩︎ ↩︎
Belsky DW, Huffman KM, Pieper CF. Change in the Rate of Biological Aging in Response to Caloric Restriction: CALERIE Biobank Analysis. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences. 2017;73(1):4-10. https://pubmed.ncbi.nlm.nih.gov/28531269/ ↩︎ ↩︎ ↩︎
Kraus WE, Bhapkar M, Huffman KM. 2 years of calorie restriction and cardiometabolic risk (CALERIE): exploratory outcomes of a multicentre, phase 2, randomised controlled trial. The Lancet Diabetes & Endocrinology. 2019;7(9):673-683. https://pubmed.ncbi.nlm.nih.gov/31303390/ ↩︎ ↩︎ ↩︎ ↩︎
Wilkins JT, Ning H, Sniderman A. Analysis of apoB Concentrations Across Early Adulthood and Predictors for Rates of Change Using CARDIA Study Data. Journal of Lipid Research. 2022;63(12):100311. https://pubmed.ncbi.nlm.nih.gov/36272600/ ↩︎ ↩︎
Rallidis LS, Giannakopoulou SP, Armylagos S. Long-term prognostic value of apolipoprotein B levels in patients with very premature (≤40 years) acute coronary syndrome. Journal of Clinical Lipidology. 2026;20(3):421-429. https://pubmed.ncbi.nlm.nih.gov/41864845/ ↩︎ ↩︎
Windred DP, Burns AC, Lane JM. Sleep regularity is a stronger predictor of mortality risk than sleep duration: A prospective cohort study. Sleep. 2024;47(1):zsad253. https://pubmed.ncbi.nlm.nih.gov/37738616/ ↩︎ ↩︎
Moore N, Bareja A, Ross LM. Biological Mechanisms of Strength Preservation During Calorie Restriction-Induced Weight Loss Among Young- to Middle-Aged Adults without Obesity. bioRxiv. 2026;12(1):401292. https://pubmed.ncbi.nlm.nih.gov/41659412/ ↩︎ ↩︎
Kim HC, Park KJ. The effect of a structured injury prevention program on injury severity and type in elite Adolescent and Young Adult Taekwondo athletes. Physical Therapy in Sport. 2026;80:101943. https://pubmed.ncbi.nlm.nih.gov/42248134/ ↩︎ ↩︎ ↩︎ ↩︎
Chodick G, Epstein S, Shalev V. Secular trends in testosterone- findings from a large state-mandate care provider. Reproductive Biology and Endocrinology. 2020;18(1):19. https://pubmed.ncbi.nlm.nih.gov/32151259/ ↩︎
Pettee Gabriel K, Jaeger BC, Lewis CE. Analysis of Cardiorespiratory Fitness in Early Adulthood and Midlife With All-Cause Mortality and Fatal or Nonfatal Cardiovascular Disease. JAMA Network Open. 2023;6(2):e230842. https://pubmed.ncbi.nlm.nih.gov/36853610/ ↩︎
Basciani S, Porcaro G. Counteracting side effects of combined oral contraceptives through the administration of specific micronutrients. European Review for Medical and Pharmacological Sciences. 2022;26(13):4842-4850. https://pubmed.ncbi.nlm.nih.gov/35856377/ ↩︎ ↩︎ ↩︎ ↩︎
Ryan CP, Lee NR, Carba DB. Pregnancy is linked to faster epigenetic aging in young women. Proceedings of the National Academy of Sciences. 2024;121(16):e2320842121. https://pubmed.ncbi.nlm.nih.gov/38588424/ ↩︎
Shen W, Chen J, Zhou J. Effect of 2-year caloric restriction on organ and tissue size in nonobese 21- to 50-year-old adults in a randomized clinical trial: the CALERIE study. The American Journal of Clinical Nutrition. 2021;114(4):1483-1491. https://pubmed.ncbi.nlm.nih.gov/34159359/ ↩︎
Lin CY, Lee HL, Su TC. Longitudinal PFAS exposure and thyroid function trajectories in Taiwanese youth: a 10-year prospective cohort study. Environment International. 2026;184:108422. https://pubmed.ncbi.nlm.nih.gov/41604980/ ↩︎
Gordji-Nejad A, Matusch A, Hengstler L. Single-Dose Creatine Reduces Sleep Deprivation-Induced Deterioration in Cognitive Performance. Nutrients. 2026;18(8):1240. https://pubmed.ncbi.nlm.nih.gov/42075005/ ↩︎
Lin CY, Lee HL, Su TC. Dynamic exposure to per- and polyfluoroalkyl substances and early alterations in cardiovascular hemodynamics: A 10-year longitudinal study in adolescents and young adults. International Journal of Hygiene and Environmental Health. 2026;258:114321. https://pubmed.ncbi.nlm.nih.gov/42247947/ ↩︎
Lin CY, Lee HL, Su TC. Longitudinal modeling of per- and polyfluoroalkyl substance exposure in relation to changes in oxidative DNA damage in Taiwanese youth: A 10-year prospective cohort study. Ecotoxicology and Environmental Safety. 2026;301:117822. https://pubmed.ncbi.nlm.nih.gov/42143973/ ↩︎
Lin CY, Lee HL, Su TC. Long-Term Per- and Polyfluoroalkyl Substances Exposure and Kidney Function in Taiwanese Adolescents and Young Adults: A 10-Year Prospective Cohort Study. Journal of Xenobiotics. 2026;16(1):12-25. https://pubmed.ncbi.nlm.nih.gov/41718259/ ↩︎
Lenssen ES, Hoek G, Scibetta L. Traffic-related micro- and nanoplastics in air increase total and differential white blood cell counts in healthy young adults. Environment International. 2025;181:108311. https://pubmed.ncbi.nlm.nih.gov/40840147/ ↩︎
Travison TG, Araujo AB, O'Donnell AB. A population-level decline in serum testosterone levels in American men. The Journal of Clinical Endocrinology and Metabolism. 2007;92(1):196-202. https://pubmed.ncbi.nlm.nih.gov/17062768/ ↩︎