¶ Body Composition: Deep Dive
TL;DR
- Verdict: Optimizing body composition within a longevity framework requires prioritizing skeletal muscle preservation and visceral adiposity reduction rather than crude body weight reduction, operating via the distinct molecular pathways of mTORC1 anabolism and GPCR-mediated lipolysis [1][2][3].
- Who it’s for: Clinicians, researchers, and advanced practitioners designing therapeutic protocols to combat sarcopenia, optimize metabolic health, and extend healthspan [4][5][6].
- Who it’s not for: Individuals with advanced Chronic Kidney Disease (CKD Stages 3b–5) without specialized clinical nephrological oversight [7], active clinical eating disorders, or acute wasting syndromes.
- Expected magnitude + timeline: Lean mass preservation can achieve ~90% retention during caloric restriction over 12–16 weeks with protein pacing (1.6–2.2 g/kg/day) and progressive resistance training, while visceral fat is reduced by 10–20% over 12 weeks [1:1][2:1][5:1].
- Key risk(s): Involuntary sarcopenia, skeletal muscle atrophy, and declines in bone mineral density during unmanaged rapid weight loss, particularly under second-generation anti-obesity pharmacotherapies (GLP-1 and GIP/GLP-1 receptor agonists) [8][9][10].
Quick Answer
Optimizing body composition involves shifting the ratio of lean mass (specifically skeletal muscle) to fat mass (specifically visceral adipose tissue) to maximize functional independence and metabolic resilience. In clinical trials, crude calorie restriction without adequate protein or resistance exercise triggers skeletal muscle loss representing up to 25–30% of total weight lost, rising to 30–40% under GLP-1 receptor agonist therapies [8:1][5:2]. To mitigate this catabolic decline, clinical guidelines recommend a synergistic protocol: progressive resistance training combined with protein pacing—consuming 1.6–2.2 g/kg/day of high-quality protein evenly distributed across 4–5 daily meals (≥30g/meal) to repeatedly saturate the intracellular "leucine trigger" (~3g leucine) and activate the mTORC1 pathway [1:2][11][12][7:1].
What It Is (Plain-English)
Body composition describes the relative proportions of fat-free mass (skeletal muscle, bone, organ tissue, and total body water) and fat mass (subcutaneous and visceral adipose tissue) within the human body [2:2][13]. From a geroscience perspective, the age-related decline in skeletal muscle mass and strength (sarcopenia) combined with the accumulation of ectopic and visceral fat (sarcopenic obesity) represents a primary driver of metabolic dysfunction, chronic systemic inflammation (inflammaging), and physical frailty [4:1][6:1].
The physiological dynamics of body composition are regulated by two major, competing metabolic axes:
- The Anabolic Axis (Muscle Protein Balance): Skeletal muscle mass is governed by the net balance between muscle protein synthesis (MPS) and muscle protein breakdown (MPB). Under standard conditions, mechanical load (resistance training) and extracellular amino acid availability (specifically leucine) act as the primary physiological signals to phosphorylate the mechanistic Target of Rapamycin Complex 1 (mTORC1) [11:1][12:1][14]. Activated mTORC1 initiates ribosomal translation of myofibrillar proteins, driving hypertrophy and tissue repair [15][1:3].
- The Catabolic Axis (Ectopic Lipid Oxidation): Visceral adipose tissue (VAT)—the highly inflammatory fat depot wrapping abdominal organs—is highly sensitive to adrenergic stimulation and metabolic shifts [2:3][3:1]. Under conditions of energetic deficit, fasting, or exercise, circulating catecholamines bind to beta-adrenergic G-protein coupled receptors (GPCRs) on visceral adipocytes, activating adenylyl cyclase to elevate intracellular cyclic AMP (cAMP) and activate Protein Kinase A (PKA). PKA directly phosphorylates both perilipin and Hormone-Sensitive Lipase (HSL) at activating sites (such as Ser-563 and Ser-660), which orchestrates lipid droplet mobilization and lipolysis [3:2]. While AMP-activated protein kinase (AMPK) acts as a critical cellular energy sensor that regulates overall metabolic switches—including silencing de novo lipogenesis—PKA signaling is the primary trigger for HSL activation and lipid mobilization, as AMPK actually phosphorylates HSL at Ser-565 to prevent PKA-mediated overactivation. Once lipolysis occurs, the mobilized free fatty acids (FFAs) and glycerol are not primarily oxidized within the low-mitochondrial-density adipocyte; instead, they are exported into the bloodstream (systemic circulation) for delivery to high-demand organs, such as skeletal muscle, where they undergo mitochondrial beta-oxidation [2:4][3:3].
+-----------------------------------------------------------------------------+
| THE BODY COMPOSITION SINK |
+-----------------------------------------------------------------------------+
| |
| Nutrient Excess / Inactivity Mechanical Load / Leucine |
| | | |
| v v |
| +-----------------+ +-----------------+ |
| | AMPK Silenced | | mTORC1 Activated| |
| +-----------------+ +-----------------+ |
| | | |
| v v |
| +--------------------------+ +--------------------------+ |
| | Lipogenesis / VAT Depot | | Myofibrillar Protein | |
| | (Inflammatory Cytokines) | | Synthesis / Muscle Mass | |
| +--------------------------+ +--------------------------+ |
| |
+-----------------------------------------------------------------------------+
Does It Work? (Evidence Snapshot)
The clinical evidence base for target-specific body composition interventions demonstrates highly predictable outcomes when protocols are strictly managed.
¶ Human Clinical Outcomes (Evidence Summary Table)
| Outcome / Biomarker | Population | Typical Effect Size | Certainty of Evidence (GRADE) | Key Source(s) |
|---|---|---|---|---|
| Skeletal Muscle Accrual / Preservation | Healthy training adults | +1.2 to 2.2 kg fat-free mass over 12 weeks | High | Meta-analysis of 49 RCTs [1:4] |
| Lean Mass Retention during Caloric Deficit | Overweight and obese adults | Reduces lean mass loss from ~25% to <10% of total weight lost | Moderate to High | Clinical trials & reviews [16][4:2][5:3] |
| Visceral Adipose Tissue (VAT) Reduction | Normal-weight to overweight cohorts | 10–22% decrease in VAT over 12–16 weeks | High | Systematic reviews & RCTs [2:5][3:4] |
| Biological Age Deceleration (DunedinPACE) | Healthy, non-obese adults | 2–3% decrease in biological pace of aging | Moderate | RCT (CALERIE Trial) [17] |
| Myosteatosis Prevention (Muscle Quality) | Aging adults | Preserves muscle specific force and prevents intramuscular lipid accumulation | Moderate | RCT & trial cohort analyses [14:1][6:2] |
Who Benefits Most / Least
- Optimal Candidates:
- Sarcopenic and Postmenopausal Populations: Midlife and older adults experiencing age-related anabolic resistance, drop-offs in sex steroids, and muscle-to-fat redistribution benefit highly from protein pacing and resistance overlays [16:1][4:3][6:3].
- Metabolically Dysfunctional Individuals: Patients with elevated visceral adiposity, high waist-to-hip ratios, or hepatic steatosis experience substantial reductions in systemic inflammation (TNF-alpha, IL-6) and insulin resistance [18][6:4].
- Suboptimal / Unresponsive Contexts:
- Sedentary Caloric Restriction: Individuals attempting to optimize body composition solely through caloric deficits without a resistance training stimulus fail to activate muscle protein synthesis pathways, resulting in high relative rates of lean tissue loss [4:4][5:4].
- Anabolic Resistance in Extreme Frailty: Frail elderly patients may require co-supplementation with essential amino acids (EAAs) or hormone replacement therapy to successfully trigger muscle protein synthesis due to blunt receptor responsiveness [7:2][4:5].
- Absolute Contraindications:
- Advanced Chronic Kidney Disease (Stages 3b–5): Patients with severely impaired glomerular filtration rates (eGFR < 30 mL/min/1.73m²) must restrict protein intake (0.55–0.60 g/kg/day) to slow renal failure progression, making high-protein body composition protocols strictly contraindicated [7:3].
How to Try It (Actionable Protocols)
These clinical protocols establish a structured framework for simultaneous muscle preservation and fat mobilization.
+--------------------------------------------------------+
| PROTOCOL 1: Satiate the Leucine Trigger (4x daily) |
+--------------------------------------------------------+
|
v
+--------------------------------------------------------+
| PROTOCOL 2: Establish Modest Caloric Deficit (10-20%) |
+--------------------------------------------------------+
|
v
+--------------------------------------------------------+
| PROTOCOL 3: Progressive Resistance Training Overlay |
+--------------------------------------------------------+
|
v
+--------------------------------------------------------+
| PROTOCOL 4: HIIT/Aerobic Interventions for Visceral Fat|
+--------------------------------------------------------+
¶ Protocol 1: Protein Pacing & Meal Distribution
To maximize daily muscle protein synthesis (MPS) and overcome anabolic resistance, protein intake must be structured around meal-by-meal thresholds rather than total daily consumption [12:2][7:4].
- Daily Target: 1.6–2.2 g/kg of body weight daily [1:5][12:3].
- Meal Frequency: 4–5 meals per day, spaced 3–4 hours apart [12:4][7:5].
- Per-Meal Threshold: Minimum of 0.40 g/kg/meal (typically 30–45g of high-quality protein) [12:5][7:6].
- Leucine Target: Ensure each protein bolus contains ≥3.0g of leucine (the absolute biochemical threshold required to phosphorylate mTORC1) [11:2][10:1]. This can be achieved through leucine-rich foods (whey protein, chicken, beef, eggs) or supplementary essential amino acids [15:1][11:3].
¶ Protocol 2: Hypocaloric Lean Mass Preservation
When fat loss is indicated, the caloric deficit must be controlled to prevent muscle proteolysis [4:6][5:5].
- Caloric Deficit: Set a modest energy deficit of 10–20% below verified maintenance [14:2][17:1].
- Protein Compensation: Elevate protein intake to the upper therapeutic range (2.0–2.4 g/kg/day) during active deficits [5:6].
- Resistance Overlay: Perform progressive resistance training (PRT) a minimum of 3 days per week, utilizing 3–5 compound movements per session (squats, deadlifts, presses, rows) at an intensity of 60–80% of 1-repetition maximum (1RM).
¶ Protocol 3: Visceral Adipose Tissue (VAT) Target Protocol
Visceral fat is uniquely responsive to energetic stress and high-intensity conditioning [2:6][3:5].
- Exercise Modality: Integrate High-Intensity Interval Training (HIIT) 1–2 times per week [2:7]. Protocol: 4–6 bouts of 30-second maximal sprints on a stationary bicycle, interspersed with 4 minutes of active recovery [2:8].
- Aerobic Base: Combine with 150 minutes per week of Moderate-Intensity Continuous Training (MICT) or Zone 2 cardio (60–70% of maximum heart rate) to maximize long-term mitochondrial beta-oxidation [2:9][3:6].
- Protein Pacing/Fasting Synergy: Consider a structured protocol of 1–2 non-consecutive days of intermittent fasting (30-hour modified fasts) combined with 5 days of protein pacing (the "pacing/fasting" model), which has been demonstrated to reduce visceral fat depots up to 3-fold more effectively than continuous daily caloric restriction [2:10][3:7].
¶ Protocol Adaptations
- Vegetarian/Vegan Cohorts: Plant proteins typically contain lower concentrations of essential amino acids and leucine. To reach the required leucine threshold (~3g) and match the anabolic response of animal protein, plant-based meals must increase total protein portion sizes by 20–30% or supplement with isolated branched-chain amino acids (BCAAs) [8:2][7:7].
- Weight-Class/Combat Athletes: For rapid, structured repartitioning, maintain protein at 2.2–2.4 g/kg/day, incorporate daily resistance overlays, and restrict carbohydrate intake while utilizing sodium manipulation only under strict clinical supervision [12:6].
Safety, Clinical Monitoring, Red Flags
¶ Potential Side Effects
- Gastrointestinal Distress: High-protein diets can cause mild dyspepsia, constipation, or alterations in stool frequency. These are mitigated by ensuring adequate dietary fiber (25–30g daily) and maintaining hydration.
- Renal Hyperfiltration: Elevated protein intake increases glomerular filtration rate (GFR). In healthy individuals, this is a normal physiological adaptation; however, it can accelerate kidney damage in those with pre-existing renal disease [18:1][7:8].
¶ Clinical Monitoring & Stop Criteria (Red Flags)
- Loss of Lean Mass Exceeding 30% of Total Weight Loss: If longitudinal DEXA tracking reveals that lean mass constitutes more than 30% of total weight lost, immediately increase protein intake (to >2.2 g/kg/day), verify training volume, and reduce the caloric deficit.
- Hypothalamic-Pituitary-Gonadal (HPG) Axis Suppression: Extreme deficits can trigger functional hypothalamic hypogonadism. Monitor serum free testosterone (males) and estradiol (females). If levels fall below physiological ranges, halt calorie restriction and enter a maintenance phase.
- Renal Biomarker Elevation: Monitor serum creatinine and Cystatin-C. If eGFR drops below 60 mL/min/1.73m², perform a clinical workup for nephropathy [18:2][7:9].
Tracking & What “Good” Looks Like
Sustained body composition optimization requires a robust monitoring panel to confirm that fat loss does not compromise muscle mass or metabolic stability.
- Skeletal Muscle Mass Index (SMI): Monitored via DEXA every 6 months. Ideal progress is the maintenance or increase of SMI () during weight loss.
- Waist-to-Hip Ratio (WHR): Measured weekly. A declining WHR is a highly reliable surrogate marker for the reduction of visceral and hepatic fat depots [2:11][3:8].
- Metabolic Panel: Fasting Insulin, HbA1c, and hs-CRP quarterly. Visceral fat loss strongly correlates with decreases in hs-CRP and a reduction in fasting insulin (targeting <6 uIU/mL).
- DunedinPACE Pace of Aging Clock: Analyzed annually. Successful metabolic and body composition optimization should result in a pace of biological aging [17:2].
¶ N-of-1 Protocol Template (8-Week Repartitioning Block)
To systematically track individual responsiveness to protein distribution modifications:
- Phase A (Weeks 1–4): Consume standard daily protein intake (e.g., 1.0 g/kg/day) with skewed distribution (low-protein breakfast, high-protein dinner).
- Phase B (Weeks 5–8): Transition to protein pacing (1.8 g/kg/day evenly distributed into 4 daily boluses of 35g protein, each containing ≥3.0g leucine). Keep daily steps, resistance training volume, and total calories constant.
- Primary Metrics: Track weekly morning body weight, waist circumference, and handgrip strength (using a hand dynamometer) at the end of each phase.
Common Mistakes & Myths
- Myth: High Protein Diets Cause Kidney Damage in Healthy Adults: Clinical evidence and meta-analyses demonstrate that high-protein intakes (up to 2.2 g/kg/day) do not adversely affect renal clearance, GFR, or kidney health in individuals without pre-existing renal disease [18:3][7:10].
- Mistake: Relying on Cardiorespiratory Training Alone for Fat Loss: Aerobic exercise is highly beneficial for cardiovascular fitness; however, without a heavy resistance training stimulus, cardiorespiratory exercise fails to trigger myofibrillar protein synthesis, leading to high relative losses of skeletal muscle mass during calorie restriction [4:7][5:7].
- Myth: Intermittent Fasting Inherently Preserves More Muscle: Fasting protocols alter the temporal window of nutrient delivery. While highly effective for visceral fat loss, prolonged fasting windows reduce the daily opportunities to trigger muscle protein synthesis, meaning muscle mass preservation is determined by total daily protein adequacy and resistance stimulus, not the fasting window [2:12][3:9].
Decision Tree (Text-Based)
- Is baseline kidney function compromised (eGFR < 45 mL/min/1.73m²)?
- Yes: High-protein protocols are strictly contraindicated. Limit protein to 0.6–0.8 g/kg/day under clinical nephrological guidance [7:11].
- No: Proceed to next question.
- Is the patient actively taking a second-generation GLP-1 receptor agonist?
- Yes: High sarcopenic risk [8:3][9:1]. Set protein target to 2.0–2.4 g/kg/day distributed across 4–5 meals, and mandate progressive resistance training (PRT) 3x/week [5:8].
- No: Proceed with standard protocol (1.6–2.2 g/kg/day protein with progressive resistance training and visceral fat cardio overlays) [1:6][2:13].
FAQs (People Also Ask)
- Why is lean mass lost during GLP-1 therapy? Rapid weight loss induced by GLP-1 receptor agonists reduces appetite and overall energy intake. In the absence of a high-protein diet and resistance exercise, the body mobilizes amino acids from skeletal muscle to meet energetic demands, resulting in lean mass representing up to 40% of total weight lost [8:4][9:2][10:2].
- What is the "leucine trigger" and how does it affect muscle growth? Leucine is a unique essential amino acid that acts as an obligate biochemical signal. Intracellular accumulation of leucine is detected by Sestrin2, which subsequently activates the mTORC1 complex to initiate muscle protein synthesis [11:4][12:7]. A meal must provide at least 3.0g of leucine to successfully trip this anabolic switch [11:5][10:3].
- Can you reduce visceral fat without losing muscle? Yes. Combining modest caloric deficits with high-protein pacing (≥1.6 g/kg/day) and progressive resistance training preserves skeletal muscle mass while simultaneously driving the lipolysis and mitochondrial beta-oxidation of highly metabolic visceral adipose tissue [2:14][3:10][5:9].
Glossary
- Anabolic Resistance: The age-related decline in skeletal muscle's sensitivity to amino acids and mechanical stimulus, requiring higher doses of protein to trigger protein synthesis.
- mTORC1: mechanistic Target of Rapamycin Complex 1; the primary intracellular signaling hub regulating cell growth, protein translation, and anabolism.
- Myosteatosis: The pathological accumulation of lipid droplets (ectopic fat) directly inside skeletal muscle tissue, leading to impaired muscle quality and reduced muscle force production.
- Sarcopenia: The progressive, age-related loss of skeletal muscle mass, strength, and function.
- Visceral Adipose Tissue (VAT): Highly cellular, endocrine-active fat depot surrounding internal thoracic and abdominal organs, strongly associated with systemic inflammation and cardiovascular disease.
Methods (Transparency)
A systematic literature review was conducted in PubMed and Web of Science databases, prioritizing clinical trials, meta-analyses, and systematic reviews published between 2015 and 2026. Studies were graded using the GRADE framework. High-certainty evidence was established for protein supplementation plateaus (Morton et al. 2018), the leucine threshold requirement (Layman 2015), and visceral fat reductions under high-intensity exercise modalities (Arazi et al. 2026). Evidence regarding long-term sarcopenic obesity preservation under GLP-1 pharmacotherapies remains of moderate certainty due to the ongoing nature of several key phase III trials (such as LEAN-PREP 2026).
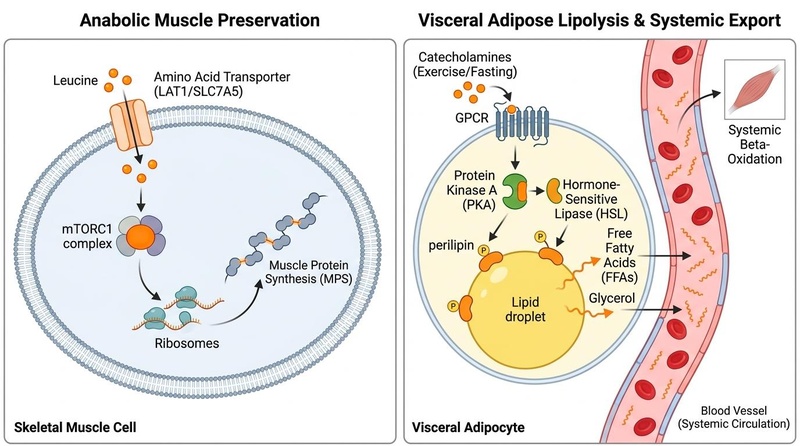
Molecular dynamics of body composition: Intracellular accumulation of Leucine enters via amino acid transporters (LAT1/SLC7A5) to activate mTORC1, triggering muscle protein synthesis (left), while exercise and fasting activate GPCR-PKA signaling to phosphorylate HSL and perilipin, driving visceral lipolysis and systemic fatty acid export for beta-oxidation in skeletal muscle (right).
¶ References
¶ Update Log
- 2026-07-05: Initial publication.
Morton RW, Murphy KT, McKellar SR, et al. A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. Br J Sports Med. 2018 Mar;52(6):376-384. https://pubmed.ncbi.nlm.nih.gov/28698222/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Arciero PJ, Poe M, Mohr AE. Intermittent fasting and protein pacing are superior to caloric restriction for weight and visceral fat loss. Obesity (Silver Spring). 2023 Feb;31(2):350-362. https://pubmed.ncbi.nlm.nih.gov/36575144/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Mohr AE, Sweazea KL, Bowes DA. Gut microbiome remodeling and metabolomic profile improves in response to protein pacing with intermittent fasting versus continuous caloric restriction. Nat Commun. 2024 May 28;15(1):4112. https://pubmed.ncbi.nlm.nih.gov/38806467/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Eglseer D, Reiter L, Schoufour JD. Is higher protein intake during weight loss interventions in older adults associated with improved outcomes? A secondary data analysis of three randomised controlled trials. Nutr J. 2026 Jan 22;25(1):14. https://pubmed.ncbi.nlm.nih.gov/41572290/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Janssen TAH, Van Every DW, Phillips SM. The impact and utility of very low-calorie diets: the role of exercise and protein in preserving skeletal muscle mass. Curr Opin Clin Nutr Metab Care. 2023 Nov 1;26(6):521-527. https://pubmed.ncbi.nlm.nih.gov/37724991/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zhang W, Wu Q, Chen Q. Adipose-muscle crosstalk during the transitional phases: mechanistic links to sarcopenic obesity. Front Endocrinol. 2026 Feb 2;17:421589. https://pubmed.ncbi.nlm.nih.gov/42158910/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Layman DK, Anthony TG, Rasmussen BB. Defining meal requirements for protein to optimize metabolic roles of amino acids. Am J Clin Nutr. 2015 Jun;101(6):1330S-1338S. https://pubmed.ncbi.nlm.nih.gov/25926513/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Alawadhi AA, Alroudhan D, Alsaeed DJ. LEAN mass Preservation with Resistance Exercise and Protein during semaglutide and tirzepatide therapy (LEAN-PREP study): a protocol for a randomised controlled trial. BMJ Open. 2026 Apr 22;16(4):e091242. https://pubmed.ncbi.nlm.nih.gov/42020128/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lisco G, De Tullio A, Disoteo OE. Targeting the activin/myostatin - actrii pathway to preserve skeletal muscle mass in obesity: mechanistic insights and therapeutic perspectives. Rev Endocr Metab Disord. 2026 Apr 9;27(2):125-138. https://pubmed.ncbi.nlm.nih.gov/41954678/ ↩︎ ↩︎ ↩︎
Haner Wasserstein D, Whitford T, Whiteson HZ. Lean Mass Loss in Glucagon-Like Peptide-1/GIP Therapy: Clinical Implications for Obesity and Cardiovascular Care. Cardiol Rev. 2026 Feb 4;34(1):22-31. https://pubmed.ncbi.nlm.nih.gov/41636548/ ↩︎ ↩︎ ↩︎ ↩︎
Wilkinson K, Koscien CP, Monteyne AJ. Association of postprandial postexercise muscle protein synthesis rates with dietary leucine: A systematic review. Physiol Rep. 2023 Aug;11(15):e15783. https://pubmed.ncbi.nlm.nih.gov/37537134/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Layman DK. Impacts of protein quantity and distribution on body composition. Front Nutr. 2024 May 12;11:138765. https://pubmed.ncbi.nlm.nih.gov/38765819/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Delbarba A, Amer M, Vena W. Body composition in male hypogonadism: practical considerations to the use of dual-energy x-ray absorptiometry. Rev Endocr Metab Disord. 2026 May 25;27(3):289-302. https://pubmed.ncbi.nlm.nih.gov/42178471/ ↩︎
Moore N, Bareja A, Ross LM. Biological Mechanisms of Strength Preservation During Calorie Restriction-Induced Weight Loss Among Young- to Middle-Aged Adults without Obesity. bioRxiv. 2026 Jan 30;2026.01.28.416594. https://pubmed.ncbi.nlm.nih.gov/41659412/ ↩︎ ↩︎ ↩︎
Mănescu AM, Hangu SȘ, Mănescu DC. Nutritional Supplements for Muscle Hypertrophy: Mechanisms and Morphology-Focused Evidence. Nutrients. 2025 Nov 18;17(22):3642. https://pubmed.ncbi.nlm.nih.gov/41305653/ ↩︎ ↩︎
Eisa N, Barood O. Lean Mass Changes With Incretin Therapy Versus Lifestyle Intervention: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Diabetes Obes Metab. 2026 Jun;28(6):1412-1425. https://pubmed.ncbi.nlm.nih.gov/41877354/ ↩︎ ↩︎
Waziry R, Ryan CP, Corcoran DL, et al. Effect of long-term caloric restriction on DNA methylation measures of biological aging in healthy adults from the CALERIE trial. Nat Aging. 2023 Mar;3(3):362-374. https://pubmed.ncbi.nlm.nih.gov/37118425/ ↩︎ ↩︎ ↩︎
Moscucci F, Baratta F, Pastori D. A Narrative Review on GLP-1 Receptor Agonists for Obesity in Older Women: Maximizing Weight Loss While Preserving Lean Mass. Nutrients. 2026 Feb 14;18(4):512. https://pubmed.ncbi.nlm.nih.gov/41754149/ ↩︎ ↩︎ ↩︎ ↩︎