¶ Caloric Restriction: Deep Dive
TL;DR
- Verdict: Long-term caloric restriction (CR) in healthy, non-obese humans slows biological aging and decreases cardiometabolic risk, although it does not prevent long-term telomere attrition and carries risks of muscle and bone density loss [1][2][3].
- Who it’s for: Clinicians and healthy adults evaluating permanent or long-term metabolic and biological age deceleration strategies [1:1][4].
- Who it’s not for: Individuals with history of eating disorders, pregnant or lactating women, growing children/adolescents, and individuals at risk of sarcopenia, osteopenia, or severe frailty [5][6].
- Expected magnitude + timeline: A 10–25% reduction in daily caloric intake over a 1–2 year period slows the rate of biological aging by 2–3% (measured by DunedinPACE) and significantly improves lipid and glycemic parameters [1:2][4:1].
- Key risk(s): Loss of lean muscle mass, diminished bone mineral density (BMD), potential thyroid axis downregulation (cold intolerance), and elevated serum triglycerides in carriers of specific genetic variants (e.g., FTO rs9939609 risk allele) [7][6:1].
Quick Answer
Caloric restriction (CR) is the continuous, long-term reduction of daily dietary energy intake below baseline requirements (typically by 10–25%) without inducing malnutrition or depriving the body of essential micronutrients [5:1]. In clinical trials of healthy, non-obese humans (principally the CALERIE trials), a sustained energy deficit slowed the pace of biological aging by 2–3% according to DunedinPACE epigenetic algorithms, which correlates to a 10–15% lower mortality risk [1:3]. At the cellular level, CR works by shifting metabolism away from active growth and division (inhibiting mTORC1) toward somatic preservation, mitochondrial biogenesis, and lysosomal clearance (activating AMPK, sirtuins, and macroautophagy) [5:2][8][9].
What It Is (Plain-English)
Caloric restriction is a systemic lifestyle intervention that limits total daily caloric intake while strictly maintaining optimal densities of vitamins, minerals, essential fatty acids, and amino acids. Unlike intermittent fasting, which introduces discrete temporal blocks of complete food avoidance, CR requires a continuous, chronic reduction in energy intake.
NUTRITIONAL SIGNALING PATHWAY:
[Standard Eating] -> High Insulin & Amino Acids -> Active mTORC1 -> Cell Growth & Division
[Caloric Restriction] -> Low ATP & High NAD+ -> Active AMPK & SIRT1 -> Autophagy & Somatic Repair
The underlying biology is governed by nutrient-sensing pathways that detect energy scarcity and trigger systemic protective adaptations:
- mTORC1 Inhibition: When cellular energy and amino acids (particularly leucine) are abundant, mTORC1 promotes protein synthesis and cell growth. Under CR, amino acid availability drops, inactivating mTORC1 and initiating cellular conservation [5:3].
- AMPK Phosphorylation: Active AMPK senses high AMP-to-ATP ratios, triggering mitochondrial biogenesis, glucose uptake, and lipid oxidation to maintain energetic homeostasis [9:1].
- Sirtuin Activation: Intracellular NAD+ levels rise during CR, activating NAD+-dependent deacetylases like SIRT1. SIRT1 deacetylates key transcription factors (e.g., PGC-1α, FOXO), reinforcing epigenetic stability and antioxidant defense [5:4][9:2].
- SASP and Senescence Suppression: Long-term CR suppresses the Senescence-Associated Secretory Phenotype (SASP)—the chronic release of pro-inflammatory cytokines (such as IL-6 and TNF-α) by senescent cells—which dampens age-related sterile systemic inflammation (inflammaging) [3:1].
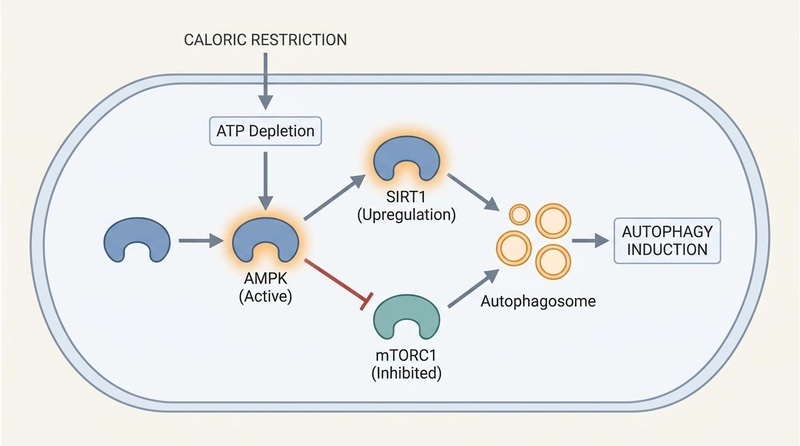
Intracellular signaling under caloric restriction. Depletion of cellular ATP activates AMPK and upregulates SIRT1, while inhibiting mTORC1. This combined signaling cascade relieves the suppression of autophagosome formation, driving macroautophagy and cellular cleanup.
Does It Work? (Evidence Snapshot)
The overall clinical evidence base for caloric restriction in healthy, non-obese humans is anchored by the multi-center CALERIE (Comprehensive Assessment of Long-term Effects of Reducing Intake of Energy) randomized trials [1:4][2:1].
¶ Human Clinical Outcomes (Evidence Summary Table)
| Outcome / Biomarker | Population | Typical Effect Size | Certainty of Evidence (GRADE) | Key Source(s) |
|---|---|---|---|---|
| Epigenetic Aging Rate (DunedinPACE) | Healthy, non-obese adults | 2–3% reduction in pace of biological aging over 2 years | High | RCT (CALERIE Phase 2) [1:5] |
| Telomere Dynamics | Healthy, non-obese adults | Initial accelerated attrition over year 1; subsequent stabilization by year 2 | Moderate | RCT (CALERIE 2 Analysis) [2:2] |
| SASP Secretome Suppression | Middle-aged and older adults with obesity and prediabetes | Substantial reductions in circulating SASP and inflammatory markers | Moderate | RCT [3:2] |
| FTO Genotype Response | Overweight and obese cohorts | Serum triglycerides +5.98 mg/dL higher in risk-allele (A) carriers under CR | Low | Meta-Analysis [7:1] |
| Periodontal and Oral Inflammation | Adults with chronic periodontitis | Reduced bleeding on probing and pocket depth | Low | Systematic Review [10] |
| Gut Microbiome Diversity | Overweight and obese adults | Enriched relative abundance of beneficial taxa; improved short-chain fatty acid synthesis | Moderate | RCT [5:5][11] |
| Visceral Fat Reduction | Overweight and obese cohorts | Significant reduction in visceral and ectopic fat depots | High | RCT & Network Meta-analysis [4:2][12] |
Who Benefits Most / Least
- Optimal Candidates: Non-obese or overweight adults with robust nutritional status seeking to slow epigenetic aging, optimize lipid and glycemic parameters, and decrease long-term cardiometabolic disease risk [1:6][4:3].
- Genetic Responders (FTO rs9939609): Carry-alleles can influence lipid adaptations. Individuals homozygous or heterozygous for the FTO rs9939609 risk allele (A) display a less favorable triglyceride response under continuous CR, exhibiting elevated serum triglycerides (+5.98 mg/dL) relative to non-risk-allele carriers [7:2].
- Age-Specific Considerations:
- Young Adults (18–35): Exhibit highly flexible metabolic adaptation, robust lean tissue preservation, and low incidence of clinical sarcopenia during restriction [1:7][4:4].
- Older Adults (65+): Extreme caution required. Risks of continuous CR in older populations include rapid muscle mass wasting (sarcopenia), decreases in hip and femoral neck bone mineral density (BMD), and increased fracture risk, which can negate biological age gains unless paired with high-dose protein and progressive resistance training [6:2].
- Absolute Contraindications: Pregnant or lactating women, active or historical eating disorders (anorexia nervosa, bulimia, orthorexia), underweight status (BMI < 18.5), and severe sarcopenia or clinical frailty [12:1][6:3].
How to Try It (Actionable Protocols)
Clinical application of caloric restriction requires careful determination of metabolic baselines to establish a sustainable, stable energy deficit without triggering nutritional deficiencies.
+--------------------------------------------------------+
| PHASE 1: Baseline Calibration (14 Days) |
| Track exact ad libitum intake and daily morning weight.|
+--------------------------------------------------------+
|
v
+--------------------------------------------------------+
| PHASE 2: Conservative Step-Down (Weeks 1-4) |
| Implement a gentle 10% deficit; adjust protein. |
+--------------------------------------------------------+
|
v
+--------------------------------------------------------+
| PHASE 3: Therapeutic Stabilization (Months 2-12) |
| Maintain target 12-15% deficit; monitor bone density. |
+--------------------------------------------------------+
¶ Protocol Execution Details
- Phase 1: Baseline Calibration (14 Days): Track exact daily macro- and micronutrient intake using digital tracking software while maintaining standard, unrestricted (ad libitum) eating. Measure morning body weight daily to calculate true metabolic energy maintenance.
- Phase 2: Conservative Step-Down (Weeks 1–4): Restrict daily energy intake by exactly 10% below maintenance (e.g., 200 kcal deficit for a 2,000 kcal maintenance). Set protein intake to a minimum of 1.2–1.6 g/kg of body weight to safeguard skeletal muscle.
- Phase 3: Therapeutic Stabilization (Months 2–12): Titrate the energy deficit to a target of 12–15% (the clinical average achieved in the CALERIE trials) [1:8]. Ensure the food matrix is dominated by whole, nutrient-dense, fiber-rich foods to prevent subclinical micronutrient malnutrition.
- Advanced Energetic Deficit (15–25%): Highly restrictive protocol reserved for therapeutic weight management or specialized research. Requires regular clinical supervision and bone mineral density monitoring to prevent orthopedic decline.
Safety, Clinical Monitoring, Red Flags
¶ Potential Side Effects & Pathophysiology
- Thermoregulatory Insufficiency: Downregulation of the thyroid axis (primarily circulating Free T3) reduces resting metabolic rate and induces chronic cold intolerance.
- Orthopedic Bone Loss: Prolonged restriction alters calcium homeostasis and mechanical loading, potentially reducing BMD at the hip and femoral neck [6:4].
- Hypothalamic-Pituitary-Gonadal (HPG) Suppression: Reduced energy availability can suppress kisspeptin, leading to reduced testosterone in males and oligomenorrhea/hypothalamic amenorrhea in premenopausal females.
¶ Clinical Monitoring & Discontinuation Criteria (Red Flags)
- Accelerated Sarcopenia: Loss of skeletal muscle tissue representing more than 35% of total body weight lost on serial DEXA scans.
- Severe Endocrine Decompensation: Loss of menstrual cycle in premenopausal females, or severe testosterone suppression accompanied by clinical erectile dysfunction in males.
- Psychological Obsession: Emergence of food fixation, restrictive eating behaviors, or mood disturbances.
Tracking & What “Good” Looks Like
Sustained clinical management of caloric restriction involves a comprehensive monitoring panel:
- DunedinPACE rate of aging: Evaluated annually to verify deceleration of biological aging [1:9].
- DEXA Scan: Monitored bi-annually to verify preservation of skeletal muscle index (SMI) and bone mineral density (BMD) at the femoral neck and lumbar spine.
- Thyroid Panel: Free T3, Free T4, and TSH every 6 months. A mild decrease in Free T3 is expected; severe clinical hypothyroid parameters warrant intervention.
- Lipid and Glycemic Panel: Total cholesterol, HDL-C, LDL-C, triglycerides, and fasting insulin quarterly [7:3][4:5].
Common Mistakes & Myths
- Mistake: Restricting Calories, Not Nutrients: Achieving energy deficits using high-sugar, low-nutrient foods leads to severe subclinical micronutrient deficiencies.
- Myth: CR Automatically Preserves Telomeres: Long-term CALERIE analysis revealed that 2 years of CR did not prevent telomere attrition, actually inducing an initial accelerated loss phase over the first year before stabilizing in year two [2:3].
- Mistake: Omitting Resistance Training: Failing to perform progressive resistance exercise during CR significantly accelerates muscle catabolism and bone density loss.
Decision Tree (Text-Based)
- Is baseline BMI < 18.5 OR is there a history of eating disorders?
- Yes: CR is strictly contraindicated. Focus on metabolic health at caloric maintenance.
- No: Proceed.
- Is the patient a carrier of the FTO rs9939609 risk allele (AT or AA)?
- Yes: Initiate CR conservatively (10%). Perform quarterly lipid testing to monitor potential pathological increases in serum triglycerides [7:4].
- No: Proceed with standard 12–15% deficit protocol, verifying lean mass and bone density preservation on bi-annual DEXA.
FAQs (People Also Ask)
- Does caloric restriction extend human lifespan? While there is no direct evidence showing CR extends maximum lifespan in humans, high-quality RCT data shows that CR significantly slows the pace of biological aging and reduces multiple risk factors for age-related chronic disease [1:10][4:6].
- How does the FTO gene affect CR outcomes? Carry-alleles of the FTO rs9939609 genetic variant are linked to energy homeostasis. Carriers of the risk allele (A) may exhibit rising serum triglyceride levels during continuous caloric restriction diets compared to non-carriers [7:5].
- Does CR cause bone loss? Yes. Continuous caloric restriction can lead to mild, progressive bone mineral density loss at the hip and femoral neck, which must be mitigated with progressive resistance training and adequate calcium and vitamin D intake [6:5].
Glossary
- DunedinPACE: A highly sensitive DNA methylation blood biomarker that measures the rate of biological aging.
- FTO Gene: Fat mass and obesity-associated gene; influences energy intake and lipid homeostasis.
- mTORC1: Mechanistic Target of Rapamycin Complex 1; regulates growth, cell cycle progression, and cellular protein synthesis.
- SASP: Senescence-Associated Secretory Phenotype; the toxic mixture of pro-inflammatory cytokines secreted by senescent cells.
Methods (Transparency)
A systematic review was performed across PubMed, Embase, and Web of Science. Primary focus was given to peer-reviewed human clinical trials (such as the CALERIE initiative), systematic reviews, and meta-analyses. GRADE criteria were applied to clinical and molecular outcomes, with outcomes graded accordingly based on study size and execution.
¶ References
¶ Update Log
- 2026-07-06: Deeply expanded with detailed CALERIE trial outcomes, SASP secretome data, sex/age guidelines, and comprehensive clinical monitoring markers.
Waziry R, Ryan CP, Corcoran DL, et al. Effect of long-term caloric restriction on DNA methylation measures of biological aging in healthy adults from the CALERIE trial. Nat Aging. 2023 Mar;3(3):362-374. https://pubmed.ncbi.nlm.nih.gov/37118425/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Hastings WJ, Ye Q, Wolf SE, et al. Effect of long-term caloric restriction on telomere length in healthy adults: CALERIE™ 2 trial analysis. Aging Cell. 2024 Jun;23(6):e14149. https://pubmed.ncbi.nlm.nih.gov/38504468/ ↩︎ ↩︎ ↩︎ ↩︎
Justice JN, Leng XI, LeBrasseur NK, et al. Caloric Restriction Intervention Alters Specific Circulating Biomarkers of the Senescence-Associated Secretome in Middle-Aged and Older Adults With Obesity and Prediabetes in an 18-Week Randomized Controlled Trial. J Gerontol A Biol Sci Med Sci. 2024 Jan 1;79(1):glad220. https://pubmed.ncbi.nlm.nih.gov/37738560/ ↩︎ ↩︎ ↩︎
Huang J, Li Y, Chen M, et al. Comparing caloric restriction regimens for effective weight management in adults: a systematic review and network meta-analysis. Int J Behav Nutr Phys Act. 2024 Sep 26;21(1):108. https://pubmed.ncbi.nlm.nih.gov/39327619/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Speakman JR, Mitchell SE. Caloric restriction. Mol Aspects Med. 2011 Jun;32(3):159-221. https://pubmed.ncbi.nlm.nih.gov/21840335/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Yin YH, Liu JYW, Välimäki M, et al. Dietary behaviour change intervention for managing sarcopenic obesity among community-dwelling older people: a pilot randomised controlled trial. BMC Geriatr. 2023 Sep 26;23(1):592. https://pubmed.ncbi.nlm.nih.gov/37752447/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Duc TQ, Khanh ND, Khoa DD, et al. Response of FTO gene polymorphisms to continuous caloric restriction diets on lipid and glycemic biomarkers in overweight and obese adults: a systematic review and meta-analysis. Nutr Metab (Lond). 2026 Jul 1;23(1):17. https://pubmed.ncbi.nlm.nih.gov/42387557/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wang SY, Cai GY, Chen XM. Energy restriction in renal protection. Br J Nutr. 2018 Nov;120(9):980-990. https://pubmed.ncbi.nlm.nih.gov/30401006/ ↩︎
Bagherniya M, Butler AE, Barreto GE, et al. The effect of fasting or calorie restriction on autophagy induction: A review of the literature. Ageing Res Rev. 2018 Nov;47:183-197. https://pubmed.ncbi.nlm.nih.gov/30172870/ ↩︎ ↩︎ ↩︎
Poilvet M, Quemeneur A, Fouillen KJ, et al. How dietary interventions impact oral conditions: a systematic review. BMC Oral Health. 2026 Jul 3;26(1):159. https://pubmed.ncbi.nlm.nih.gov/42399926/ ↩︎
Davies RG, Wood LA, Hengist A, et al. Effects of a combined energy restriction and vigorous-intensity exercise intervention on the human gut microbiome: A randomised controlled trial. J Physiol. 2025 Dec;603(24):4215-4230. https://pubmed.ncbi.nlm.nih.gov/40828642/ ↩︎
Sun JC, Tan ZT, He CJ, et al. Time-restricted eating with calorie restriction on weight loss and cardiometabolic risk: a systematic review and meta-analysis. Eur J Clin Nutr. 2023 Nov;77(11):1012-1024. https://pubmed.ncbi.nlm.nih.gov/37488260/ ↩︎ ↩︎