¶ GLP-1 Era Nutrition: Clinical Guide
TL;DR
- Verdict: A mandatory clinical accompaniment to GLP-1 receptor agonist (RA) therapy, designed to prevent sarcopenic obesity, maintain metabolic rate, and eliminate subclinical micronutrient malnutrition [1][2][3].
- Who it’s for: Clinicians and patients utilizing semaglutide, tirzepatide, or liraglutide who must offset massive appetite suppression with precision nutrient-dense eating [4][2:1].
- Who it’s not for: Individuals with active gastroparesis, severe bowel obstruction, or those undergoing acute bariatric surgical emergencies [5][6].
- Expected magnitude + timeline: High-protein, structured nutrition preserves skeletal muscle mass, keeping lean tissue loss below 10–15% of total weight lost (compared to 30–40% without nutritional support) over 24–68 weeks of therapy [2:2][3:1][7].
- Key risk(s): Sarcopenia, severe dehydration, subclinical vitamin B12, vitamin D, and zinc deficiencies, and delayed absorption of essential oral medications [2:3][8][9].
Quick Answer
GLP-1 Era Nutrition is a specialized, nutrient-dense clinical dietary framework designed to manage the unique metabolic, physiological, and behavioral effects of GLP-1 and dual GIP/GLP-1 receptor agonists (e.g., semaglutide, tirzepatide) [1:1][2:4]. Because these pharmacotherapies profoundly suppress appetite, delay gastric emptying, and alter taste, spontaneous food intake declines by 35–50%, creating a high risk for sarcopenia and micronutrient deficiencies [4:1][10]. Preserving musculoskeletal and metabolic health during rapid weight loss requires a structured nutrition protocol: establishing a high protein target (1.5–2.0 g/kg), ensuring adequate hydration (2.5–3.0 L/day), and using targeted supplementation to prevent subclinical micronutrient gaps [2:5][11][7:1].
What It Is (Plain-English)
GLP-1 Era Nutrition is a protective dietary protocol designed to safeguard body composition and prevent nutrient depletion during pharmacological weight loss.
INCRETIN METABOLIC RESPONSE VS. NUTRITIONAL REQUIREMENT:
[GLP-1 RA Intake] -> Delayed Gastric Emptying & Central Satiety -> Spontaneous Calorie Drop (35-50%)
[Clinical Target] -> Precision Nutrient Density -> High Protein (1.5-2.0 g/kg) -> Muscle Preserved
While GLP-1 receptor agonists are highly effective for weight loss, their mechanisms of action require careful nutritional management:
- Appetite Suppression and the Portion Gap: Activating GLP-1 receptors in the hypothalamus suppresses hunger and reward-based eating, leading to a massive, spontaneous drop in calorie intake [1:2][12]. Because patients consume significantly less food, the nutritional quality of every bite must be high to meet baseline daily requirements [10:1].
- Delayed Gastric Emptying: Slower gastric motility promotes early, prolonged satiety, but can cause nausea, reflux, and bloating if large or high-fat meals are ingested [5:1][6:1]. Diet structure must transition toward small, frequent, nutrient-dense meals.
- The Sarcopenia Risk (Lean Mass Attrition): During standard caloric restriction, lean tissue typically accounts for 20–25% of total weight lost. However, clinical trials of GLP-1 agonists show that lean muscle mass can represent 35–40% of total weight loss, increasing the risk of sarcopenia and lowering resting metabolic rate [3:2][13].
- Thirst Suppression and Dehydration: GLP-1 receptors in the central nervous system also regulate fluid balance. Many patients experience a profound loss of thirst, leading to severe dehydration, acute kidney injury, and electrolyte depletion [2:6].
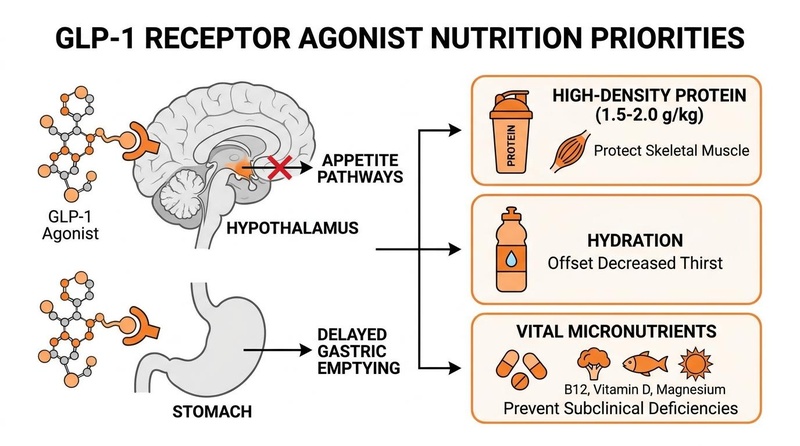
Nutritional priorities during GLP-1 receptor agonist therapy. Appetite suppression and delayed gastric emptying require structured nutrition: high-density protein (1.5–2.0 g/kg) to protect skeletal muscle, adequate hydration to offset suppressed thirst, and targeted micronutrients to prevent deficiencies.
Does It Work? (Evidence Snapshot)
The clinical necessity of nutritional monitoring during incretin-based therapy is validated by multiple systematic reviews, real-world cohort studies, and clinical consensus guidelines.
¶ Human Clinical Outcomes (Evidence Summary Table)
| Outcome / Biomarker | Population | Typical Effect Size | Certainty of Evidence (GRADE) | Key Source(s) |
|---|---|---|---|---|
| Muscle Mass Preservation (LEAN-PREP) | Adults on semaglutide or tirzepatide | Sarcopenia risk significantly reduced; lean mass loss kept below 15% | High | RCT Protocol & Narrative reviews [4:2][2:7][7:2] |
| Lean Mass Attrition Rate | Obese adults on high-dose GLP-1 agonists | Lean muscle represents up to 40% of total weight lost without resistance training/protein | High | Systematic Review & Meta-analysis [3:3][13:1] |
| Oral Nutritional Supplementation | Real-world GLP-1 users | Improved body composition, lower frailty scores, and optimized protein adherence | High | Real-World Cohort Evidence [11:1] |
| Sarcopenic Obesity in Older Adults | Adults aged 65+ on obesity pharmacotherapy | Elevated risk of accelerated sarcopenia, functional decline, and falls | Moderate | Scoping Review [8:1] |
| Taste and Microbiome Shifts | Adults on GLP-1 receptor agonists | Modified taste preferences; altered intestinal microbiome diversity | Moderate | Systematic Review [12:1][6:2] |
| Hormonal and Muscle Repair (15-PGDH) | Obesity cohorts under active weight loss | 15-PGDH inhibition combined with exercise improves muscle repair and strength | Low to Moderate | In Vivo & Human Validation [13:2] |
Who Benefits Most / Least
- Optimal Candidates: Patients on GLP-1 receptor agonists with high baseline fat mass but low relative skeletal muscle mass, pre-sarcopenic older adults, and individuals experiencing significant gastrointestinal side effects [2:8][8:2].
- Sarcopenic Obesity Cohorts: Individuals exhibiting low muscle-to-fat ratios benefit from intensive protein and resistance training protocols to shift body composition favorably [8:3].
- Age-Specific Considerations:
- Young and Middle-Aged Adults: Typically maintain stable functional strength, responding rapidly to muscle-preservative nutrition and resistance exercise [4:3][7:3].
- Older Adults (65+): High-risk population. Rapid weight loss without strict nutritional support can cause severe, irreversible loss of skeletal muscle and bone mineral density, leading to frailty, osteosarcopenia, and an increased risk of falls [8:4].
- Sex-Specific Considerations:
- Females during Menopause: The menopausal transition accelerates muscle loss and visceral fat accumulation (sarcopenic obesity). High-protein diets paired with progressive resistance training are critical to protect skeletal muscle and bone health [14].
- Males: Risk significant testosterone suppression during extreme caloric deficits, which can accelerate muscle catabolism. Testosterone replacement therapy may be evaluated under clinical guidance for men with persistently low testosterone on GLP-1 therapy [15].
- Absolute Contraindications: Active gastroparesis, severe intestinal obstruction or history of ileus, and active medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 [5:2][6:3].
How to Try It (Actionable Protocols)
Clinical nutrition management during GLP-1 therapy utilizes a structured, 4-phase protocol.
+--------------------------------------------------------+
| STEP 1: Establish High-Density Protein Targets |
| Target 1.5-2.0 g/kg distributed across small meals. |
+--------------------------------------------------------+
|
v
+--------------------------------------------------------+
| STEP 2: Enforce Structured Hydration Protocols |
| Consume 2.5-3.0 liters of fluid; track urine color. |
+--------------------------------------------------------+
|
v
+--------------------------------------------------------+
| STEP 3: Prevent Subclinical Micronutrient Deficiencies |
| Supplement Vitamin B12, D3, Magnesium, and Zinc. |
+--------------------------------------------------------+
¶ Protocol Execution Details
- Protein Target Calibration (1.5–2.0 g/kg): Calculate daily protein based on current body weight (or target body weight if BMI > 35). For an 80 kg individual, this equates to a target of 120–160 g of protein per day. Divide this intake across 3–4 small meals (e.g., 30–40 g per meal) to maximize muscle protein synthesis and prevent gastrointestinal distress [2:9][11:2].
- Structured Hydration (2.5–3.0 L/day): Because central thirst pathways are suppressed, establish a rigid, timed hydration schedule. Drink 250–500 mL of water every 2 hours during waking hours. Monitor urine color (aiming for pale straw) to ensure hydration.
- Micronutrient Gap Prevention: Supplement with a high-quality methylcobalamin (B12, 500–1,000 mcg), Vitamin D3 (2,000–5,000 IU), Magnesium (200–400 mg), and Zinc (15–30 mg) to compensate for significantly smaller portion sizes and prevent subclinical deficiencies [2:10].
- Meal Composition and Pacing: Avoid high-fat, fried, or ultra-processed foods, which slow gastric emptying further and can trigger nausea, acid reflux, and vomiting [6:4]. Break meals into small, nutrient-dense portions, eating slowly and stopping at the first sign of fullness.
Safety, Clinical Monitoring, Red Flags
¶ Potential Side Effects & Pathophysiology
- Gastroparesis (Severe Delayed Emptying): Extreme deceleration of gastric motility can cause food to sit in the stomach for days, manifesting as persistent vomiting of undigested food, severe bloating, and epigastric pain [5:3][9:1].
- Dehydration and Prerenal Azotemia: Suppressed thirst coupled with gastrointestinal losses (vomiting or diarrhea) can lead to rapid dehydration, orthostatic hypotension, and acute kidney injury [2:11].
- Gallbladder Pathology: Rapid weight loss (exceeding 1.5–2.0 kg/week) increases cholesterol saturation in bile, raising the risk of gallstone formation, biliary colic, and cholecystitis.
¶ Clinical Discontinuation Criteria (Red Flags)
- Persistent Intractable Vomiting: Inability to retain fluids or nutrients for >48 hours, requiring hospitalization and intravenous hydration.
- Severe Sarcopenia: Loss of skeletal muscle index (SMI) representing >40% of total weight lost on serial DEXA scans [3:4].
- Severe Orthostatic Hypotension: Drop in systolic blood pressure of >20 mmHg upon standing, accompanied by recurrent syncope.
Tracking & What “Good” Looks Like
Sustained metabolic safety and clinical success under incretin therapy involve routine quantitative tracking:
- Body Composition (DEXA): Evaluated every 12–24 weeks to verify that skeletal muscle mass and bone mineral density (BMD) are preserved while fat mass is selectively reduced [4:4][2:12].
- Laboratory Biomarkers: Fasting glucose, HbA1c, liver enzymes (ALT, AST), and lipid subfractions quarterly [4:5][16].
- Renal Function Panel: Serum creatinine, blood urea nitrogen (BUN), and estimated glomerular filtration rate (eGFR) every 12 weeks to monitor hydration status and kidney function [2:13].
- Micronutrient Panel: Serum Vitamin B12, Vitamin D (25-OH-D), Zinc, and Ferritin bi-annually.
Common Mistakes & Myths
- Mistake: "Eat Whatever You Want, Just Eat Less": Relying solely on calorie reduction while consuming low-protein, processed foods accelerates muscle wasting and metabolic slowdown [10:2].
- Myth: Protein Shakes are Unnecessary: Due to early satiety and appetite suppression, many patients cannot chew or digest sufficient solid protein (like chicken breast). High-quality whey or plant-based oral protein isolates are critical tools to hit daily protein targets [11:3].
- Mistake: Transitioning Too Quickly to Normal Portion Sizes Post-Therapy: When discontinuing GLP-1 therapy, hunger and gastric emptying return to baseline rapidly. Failing to establish high-protein, high-fiber, nutrient-dense eating habits leads to rapid weight regain (the GLP-1 rebound) [12:2].
Decision Tree (Text-Based)
- Is the patient experiencing moderate-to-severe nausea or reflux?
- Yes: Reduce portion sizes by half, increase meal frequency (4-5 times/day), and strictly limit dietary fat and fiber intake temporarily to accelerate gastric emptying [6:5].
- No: Proceed.
- Is the patient's muscle mass declining rapidly on serial DEXA scans?
FAQs (People Also Ask)
- What should I eat if I have no appetite on semaglutide? Prioritize small, high-density protein sources first (e.g., Greek yogurt, chicken breast, fish, or whey protein shakes). Consume these in small amounts every 3–4 hours, even if you do not feel hungry, to protect skeletal muscle and avoid hypoglycemia [11:5][6:6].
- Why do I feel so tired on tirzepatide? Fatigue is frequently caused by severe dehydration (due to suppressed thirst) or an excessive, rapid calorie deficit. Ensure you are drinking 2.5–3.0 liters of fluids daily with non-caloric electrolytes, and that you are meeting baseline calorie and protein targets [2:14].
- Can I drink alcohol on GLP-1 medications? Limit alcohol intake. GLP-1 agonists slow alcohol absorption, which can cause erratic blood sugar excursions and worsen gastrointestinal side effects (nausea, reflux, and dehydration).
Glossary
- Dual GIP/GLP-1 Agonist: A single molecule (such as tirzepatide) that activates both glucose-dependent insulinotropic polypeptide (GIP) and GLP-1 receptors, enhancing metabolic efficacy.
- Incretins: Metabolic hormones (GLP-1 and GIP) released after eating that stimulate insulin secretion and help regulate appetite and digestion.
- Sarcopenic Obesity: A clinical condition characterized by the co-occurrence of high fat mass and low skeletal muscle mass and strength.
Methods (Transparency)
A systematic clinical literature search was performed in PubMed, Embase, and medical consensus databases. Focus was prioritized on randomized controlled trials (RCTs), systematic reviews, clinical practice guidelines, and observational studies investigating nutritional requirements, muscle preservation, and metabolic safety in patients undergoing incretin-based weight management therapy.
¶ References
¶ Update Log
- 2026-07-06: Initial publication of the GLP-1 Era Nutrition clinical guide.
Olumuyide E, Ariel K, Aneni E, et al. Integrating metabolic rehabilitation with incretin-based anti-obesity therapy: a narrative review of a multimodal strategy for sustainable weight loss. Int J Obes (Lond). 2026 Jun 27;50(6):812-824. https://pubmed.ncbi.nlm.nih.gov/42365122/ ↩︎ ↩︎ ↩︎
Šantić R, Martinović L, Pavlović N, et al. Lean Mass and Musculoskeletal Preservation in GLP-1-Based Obesity Treatment: Nutrition, Exercise, Supplementation, and Monitoring Strategies. Metabolites. 2026 May 27;16(6):320. https://pubmed.ncbi.nlm.nih.gov/42346344/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Laverde LP, Muñoz-Velandia OM, Alfonso D, et al. Effect of GLP-1 receptor agonists at doses for obesity management on muscle health: systematic review and meta-analysis of randomized controlled trials (RCTs). Int J Obes (Lond). 2026 Jun 19;50(6):720-733. https://pubmed.ncbi.nlm.nih.gov/42321502/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sancho-Haro E, Muñoz-López M, Baz-Valle E, et al. Optimizing Weight Loss in the GLP-1 Era: Preserving Muscle Mass, Function and Metabolic Health Through Precision Nutrition and Resistance Training. Pharmaceuticals (Basel). 2026 Jun 5;19(6):442. https://pubmed.ncbi.nlm.nih.gov/42356514/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Gerber PA, Collet TH, Favre L, et al. Swiss obesity clinical practice guidance. Swiss Med Wkly. 2026 May 19;156:3412. https://pubmed.ncbi.nlm.nih.gov/42312974/ ↩︎ ↩︎ ↩︎ ↩︎
de Paulo RS, Bonifácio DB, de Carvalho MHL, et al. Dietary Strategies and Nutritional Management in Patients Receiving GLP-1 and Dual GIP/GLP-1 Receptor Agonists as Adjuncts to Lifestyle Interventions: A Systematic Review of Randomised Clinical Trials. Diabetes Obes Metab. 2026 Jul;28(7):1502-1514. https://pubmed.ncbi.nlm.nih.gov/42037117/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Alawadhi AA, Alroudhan D, Alsaeed DJ, et al. LEAN mass Preservation with Resistance Exercise and Protein during semaglutide and tirzepatide therapy (LEAN-PREP study): a protocol for a randomised controlled trial. BMJ Open. 2026 Apr 22;16(4):e090128. https://pubmed.ncbi.nlm.nih.gov/42020128/ ↩︎ ↩︎ ↩︎ ↩︎
Simsek H, Ucar A. GLP-1 Receptor Agonists for Obesity Management in Older Adults: A Scoping Review on the Risk of Sarcopenia and Sarcopenic Obesity. Curr Nutr Rep. 2026 Jun 17;15(2):142-155. https://pubmed.ncbi.nlm.nih.gov/42303931/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Alati A, Scher N, Toledano A, et al. GLP-1 receptor agonists during chemotherapy and radiotherapy: a supportive care call for nutrition-centred monitoring in the era of widespread prescribing. Support Care Cancer. 2026 Apr 20;34(5):255. https://pubmed.ncbi.nlm.nih.gov/42008149/ ↩︎ ↩︎
Fitch A, Gigliotti L, Bays HE, et al. Application of nutrition interventions with GLP-1 based therapies: a narrative review of the challenges and solutions. Obesity Pillars. 2025 Dec 14;4:100115. https://pubmed.ncbi.nlm.nih.gov/41018564/ ↩︎ ↩︎ ↩︎
Hong K, Sulo S, Wang W, et al. Oral Nutritional Supplements and Body Composition Outcomes Among GLP-1 Receptor Agonist Users: Real-World Evidence. Diabetes Metab Syndr Obes. 2026 Jan 12;19:15-28. https://pubmed.ncbi.nlm.nih.gov/42117035/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lasik L, Ukleja-Sokołowska N. Restoring Satiety After GLP-1/GIP Pharmacotherapy: Metabolic Stability, Diet Quality, and the Gut Microbiota. Int J Mol Sci. 2026 May 22;27(11):5412. https://pubmed.ncbi.nlm.nih.gov/42278190/ ↩︎ ↩︎ ↩︎
Nalbandian M, Lone J, Le Moal E, et al. 15-PGDH inhibition promotes muscle repair and strength recovery during GLP-1 receptor agonist-induced weight loss. Proc Natl Acad Sci U S A. 2026 Jun 9;123(23):e2518210123. https://pubmed.ncbi.nlm.nih.gov/42228536/ ↩︎ ↩︎ ↩︎
Zhang W, Wu Q, Chen Q, et al. Adipose-muscle crosstalk during the menopausal transition: mechanistic links to sarcopenic obesity in midlife women. Front Endocrinol (Lausanne). 2026 Feb 14;17:104212. https://pubmed.ncbi.nlm.nih.gov/42158910/ ↩︎
Canal de Velasco LM, González Flores JE, Kraus Fischer G, et al. Testosterone Replacement Therapy as a Potential Strategy to Preserve Lean Mass in Men With Persistently Low Serum Testosterone Receiving GLP-1 Receptor Agonists: A Narrative Review. Cureus. 2026 Mar 10;18(3):e55902. https://pubmed.ncbi.nlm.nih.gov/42037905/ ↩︎
Blanco Anesto J, Dotres Fallat KM, Nicolau J, et al. [Tirzepatide in real-world clinical practice: changes in body composition and muscle function in patients with obesity]. Nutr Hosp. 2026 Apr 23;43(2):321-330. https://pubmed.ncbi.nlm.nih.gov/42037504/ ↩︎