¶ Muscle Preservation During Weight Loss: Clinical Guide
TL;DR
- Verdict: A physiologically vital clinical protocol required during any significant weight loss phase to prevent sarcopenia, protect metabolic rate, and maintain functional skeletal strength [1][2][3].
- Who it’s for: Individuals undergoing caloric restriction, bariatric post-surgery management, or incretin-based weight loss therapy (e.g., semaglutide, tirzepatide) [2:1][4][5].
- Who it’s not for: Individuals undergoing acute metabolic crises, advanced cachexia, or end-stage chronic renal failure where high-dose protein is contraindicated [6].
- Expected magnitude + timeline: High-protein intake (1.6–2.4 g/kg) combined with progressive resistance training maintains skeletal muscle index (SMI) and keeps muscle loss below 10–15% of total weight lost over 12–24 weeks [7][8].
- Key risk(s): Elevated muscle protein breakdown (MPB), suppressed metabolic flexibility, osteosarcopenia, and functional physical decline [9][6:1].
Quick Answer
Muscle preservation during weight loss is the targeted application of nutritional, pharmacological, and exercise interventions to selectively deplete adipose tissue while safeguarding lean skeletal muscle mass [1:1][5:1]. In standard calorie deficits, up to 25–30% of weight lost is derived from lean tissue, which can spike to 40% during rapid pharmacological or bariatric weight loss [2:2][4:1]. This muscle wasting is driven by down-regulated mTORC1 signaling and up-regulated ubiquitin-proteasome protein degradation [1:2][2:3]. Clinically, preventing this catabolism requires a triad of interventions: establishing high protein targets (1.6–2.4 g/kg), ensuring adequate per-meal leucine triggers (2.5–3.0 g) to stimulate muscle protein synthesis (MPS), and performing progressive resistance training to induce mechanical tissue tension [10][1:3][8:1].
What It Is (Plain-English)
Muscle preservation during weight loss is a protective metabolic protocol designed to ensure that body weight reduction is derived selectively from body fat while protecting muscular and bone health.
THE ANABOLIC BALANCE UNDER CALORIC DEFICIT:
[Caloric Deficit alone] -> Suppressed mTORC1 & Active Ubiquitin Pathway -> Muscle Wasting (Sarcopenia)
[Deficit + Protein + Lift] -> High Leucine & Mechanical Tension -> Active mTORC1 -> Muscle Preserved
When the body is in an energy deficit, the cellular environment shifts toward catabolism. Without targeted interventions, skeletal muscle tissue is readily broken down to supply amino acids for hepatic gluconeogenesis:
- mTORC1 and Muscle Protein Synthesis (MPS): mTORC1 is the master regulator of protein translation and cell growth. It is stimulated primarily by cellular energy availability, mechanical tension (lifting weights), and intracellular amino acids (specifically leucine) [1:4]. Under continuous energy deficits, mTORC1 is suppressed, leading to a drop in baseline MPS [2:4].
- The Leucine Trigger: Intracellular leucine concentration is sensed by the Sestrin2 protein, which recruits mTORC1 to the lysosomal membrane for activation [1:5]. Reaching the "leucine trigger" (typically 2.5–3.0 g of leucine per meal, equivalent to ~25–35 g of high-quality whey or animal protein) is required to stimulate muscle protein synthesis during energy deficits. Consuming protein below this threshold fails to activate the anabolic cascade [8:2].
- Ubiquitin-Proteasome Pathway (UPP): The UPP is the primary pathway for muscle protein breakdown (MPB). During low insulin and low amino acid states, muscle-specific E3 ubiquitin ligases (such as MuRF1 and MAFbx) tag muscle contractile proteins for degradation. Progressive resistance training suppresses this pathway, blocking muscle catabolism [1:6][2:5].
- Metabolic Rate Protection: Skeletal muscle tissue is highly metabolically active, accounting for a significant portion of resting energy expenditure (REE). Preserving muscle mass prevents the pathological "adaptive thermogenesis" (metabolic slowing) that commonly triggers early weight loss plateaus and rapid weight rebound [10:1][11].
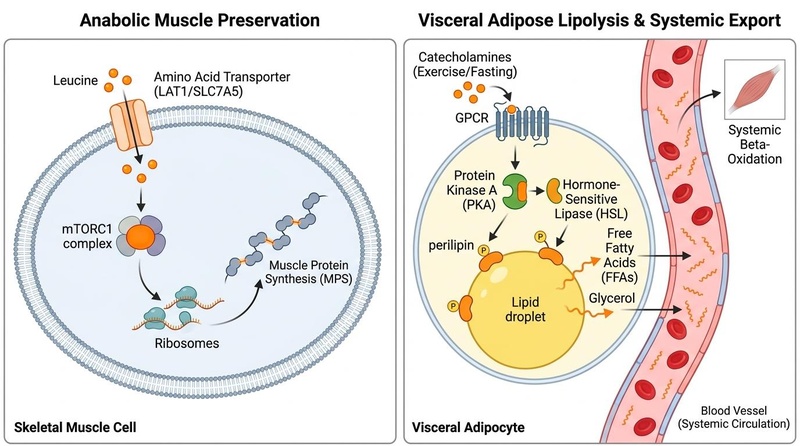
The physiology of muscle preservation and visceral fat loss. (Left Panel) High-density leucine intake stimulates the LAT1 transporter and mTORC1 complex to drive muscle protein synthesis (MPS) and protect skeletal muscle. (Right Panel) Exercise and fasting stimulate catecholamines and hormone-sensitive lipase (HSL) within visceral adipocytes, driving lipolysis and exporting free fatty acids and glycerol for beta-oxidation.
Does It Work? (Evidence Snapshot)
The physiological mechanisms and clinical efficacy of muscle preservation are validated by a high-certainty body of randomized controlled trials (RCTs), systematic reviews, and meta-analyses.
¶ Human Clinical Outcomes (Evidence Summary Table)
| Outcome / Biomarker | Population | Typical Effect Size | Certainty of Evidence (GRADE) | Key Source(s) |
|---|---|---|---|---|
| Lean Mass Preservation (LEAN-PREP) | Adults on incretin-based weight loss therapy | Visceral fat is selectively lost while keeping lean muscle loss below 15% | High | RCT Protocol & Review [1:7][2:6][^17] |
| Protein and Strength in Older Adults | Older adults undergoing a 17-week diet | High-protein diet combined with strength training optimizes plasma metabolome and protects strength | High | RCT [7:1] |
| Combined Whey and Lifting | Adults with metabolic dysfunction (MASLD) under CR | Independent and synergistic effects of resistance training and whey protein on skeletal muscle index | High | RCT [8:3] |
| Protein Efficacy during Weight Loss | Older adults under active weight management | High-protein intake improves functional physical outcomes and quality of life | High | Secondary analysis of 3 RCTs [12] |
| Exercise post-Bariatric Surgery | Bariatric surgery patients | Combined aerobic and resistance training prevents bone loss and sarcopenia | Moderate | Systematic Review [6:2] |
| Incretin vs. Lifestyle Lean Loss | Overweight and obese cohorts | Incretin therapy causes greater absolute lean mass loss than lifestyle unless protein/exercise are managed | Moderate | Systematic Review & Meta-analysis [4:2] |
Who Benefits Most / Least
- Optimal Candidates: Patients undergoing active weight loss programs (caloric restriction, ketogenic diets), individuals on GLP-1 receptor agonist pharmacotherapy, and post-bariatric surgery patients [2:7][6:3][5:2].
- Sarcopenic Obesity and Frail Cohorts: Older adults exhibiting a low ratio of muscle to fat benefit from aggressive muscle-preserving protocols to prevent functional mobility declines [7:2][12:1].
- Age-Specific Considerations:
- Young Adults (18–35): Exhibit highly efficient protein utilization, robust hormonal support, and rapid adaptation to resistance training [1:8].
- Older Adults (65+): Experience "anabolic resistance"—requiring higher relative doses of protein and leucine to stimulate the same level of MPS as younger cohorts. Older adults under calorie deficits must consume at least 1.8–2.2 g/kg of protein and prioritize heavy resistance training to offset rapid muscle and bone loss [7:3][12:2].
- Sex-Specific Considerations:
- Females (specifically Post-Menopausal): Estrogen downregulation during menopause accelerates visceral adiposity and sarcopenia. High-dose protein (up to 2.0 g/kg) paired with progressive resistance training is critical to protect bone mineral density and physical strength [2:8][7:4].
- Males: Risk significant testosterone suppression during steep caloric deficits. Maintaining high protein and resistance training supports natural androgen receptor density, protecting skeletal muscle from catabolism [8:4].
- Absolute Contraindications: Advanced renal failure (estimated GFR < 30 mL/min) without dialytic support where high protein is strictly contraindicated, acute hepatic encephalopathy, and active severe rhabdomyolysis [6:4].
How to Try It (Actionable Protocols)
Preserving muscle mass during weight loss requires a structured, multi-step protocol combining protein calibration, leucine timing, and mechanical resistance.
+--------------------------------------------------------+
| PROTOCOL 1: Calibrate Daily Protein Targets |
| Target 1.6-2.4 g/kg of current body weight daily. |
+--------------------------------------------------------+
|
v
+--------------------------------------------------------+
| PROTOCOL 2: Time the Leucine Trigger (Every 3-4 hours) |
| Consume 2.5-3.0g leucine (25-35g whey) per feeding. |
+--------------------------------------------------------+
|
v
+--------------------------------------------------------+
| PROTOCOL 3: Progressive Resistance Training |
| Perform 3 weekly sessions of progressive lifting. |
+--------------------------------------------------------+
¶ Protocol Execution Details
- Daily Protein Target Calibration (1.6–2.4 g/kg): Establish a daily protein target based on total body weight (or target lean mass if BMI > 35). For a 90 kg individual, this equates to 144–216 g of protein per day.
- Timing the Leucine Trigger: Ensure protein intake is distributed evenly across 3–5 feedings spaced 3–4 hours apart. Each feeding must contain at least 2.5–3.0 g of leucine (or 25–35 g of high-quality protein) to initiate muscle protein synthesis [1:9][8:5]. Protein consumed in smaller, sub-threshold amounts (e.g., snacking on 5 g of protein throughout the day) fails to trigger anabolic signaling.
- Progressive Resistance Training (PRT): Perform at least 3 sessions of structured resistance training per week, focusing on multi-joint compound movements (such as squats, deadlifts, chest presses, and rows). Utilize a weight that brings the muscle close to local failure within 6–12 repetitions to maximize mechanical tension [10:2][1:10].
- Targeted Supplementation:
- Whey Protein Isolate: Consumed post-exercise or between meals to easily hit leucine thresholds [5:3][14].
- Creatine Monohydrate (3–5 g/day): Up-regulates intramuscular phosphocreatine stores, increasing cellular hydration, strength output, and satellite cell activation during energy deficits.
- HMB (Beta-Hydroxy-Beta-Methylbutyrate, 3 g/day): A metabolite of leucine with potent anti-catabolic properties; highly effective at suppressing the Ubiquitin-Proteasome pathway under steep calorie deficits or prolonged fasting.
Safety, Clinical Monitoring, Red Flags
¶ Potential Side Effects & Pathophysiology
- Renal Hyperfiltration: High protein intake increases renal blood flow and glomerular pressure. This is a normal physiological adaptation in healthy kidneys, but can accelerate decline in patients with pre-existing Stage 3–5 chronic kidney disease.
- Gastrointestinal Distress: High protein intake, especially from poorly tolerated dairy concentrates, can cause bloating, flatulence, and constipation (often exacerbated by low dietary fiber).
- Central Nervous System Adaptation (Fatigue): Intense resistance training under calorie deficits can strain the central nervous system, manifesting as persistent daytime lethargy, sleep disturbances, and loss of grip strength.
¶ Clinical Discontinuation Criteria (Red Flags)
- Sarcopenic Decline: A loss of skeletal muscle index (SMI) exceeding 30% of total weight lost on serial DEXA scans [2:9][4:3].
- Renal Decompensation: Rapid rise in serum creatinine or drop in eGFR below 45 mL/min.
- Overtraining Syndrome: Persistent elevated resting heart rate (>10 bpm above baseline), chronic insomnia, and loss of physical strength over 3 consecutive weeks.
Tracking & What “Good” Looks Like
Successful clinical management of muscle preservation during weight loss involves:
- DEXA Scan (Body Composition): Evaluated every 12 weeks to confirm that weight loss is selectively derived from visceral and subcutaneous fat depots while preserving skeletal muscle mass and bone mineral density [1:11][2:10].
- Functional Strength Tracking: Monitoring performance on compound movements. Maintaining or slightly increasing physical strength during weight loss indicates excellent muscle preservation [1:12].
- Urinary Nitrogen and Blood Urea Nitrogen (BUN): Assessed quarterly to monitor protein utilization and nitrogen balance.
- Subjective Energy and Recovery: Assessing subjective muscle soreness (DOMS), morning joint stiffness, and daily vitality levels.
Common Mistakes & Myths
- Mistake: Relying Exclusively on "Cardio" for Weight Loss: Performing high volumes of steady-state cardiovascular exercise without resistance training accelerates muscle protein breakdown and lean mass wasting [10:3][1:13].
- Myth: High Protein Causes Kidney Damage: In individuals with healthy baseline renal function, high-protein diets (up to 2.8 g/kg) do not cause kidney damage, representing a safe and highly effective metabolic strategy.
- Mistake: Low-Protein Snacking: Consuming tiny amounts of protein throughout the day (e.g., 5–10 g every hour) fails to reach the leucine trigger required to activate mTORC1, resulting in poor anabolic efficiency [8:6].
Decision Tree (Text-Based)
- Is the patient over 65 years old or experiencing anabolic resistance?
- Yes: Set daily protein target high (2.0–2.4 g/kg), prioritize whey protein isolate, and implement heavy, progressive resistance training with a focus on lower-body compound movements [7:5][12].
- No: Proceed.
- Is the patient's rate of muscle loss on serial DEXA scans greater than 20% of total weight lost?
FAQs (People Also Ask)
- How much muscle is normally lost during weight loss? Without targeted protein and resistance training, 25–30% of total weight lost is typically derived from lean muscle tissue. On rapid weight loss programs or obesity medications, this can rise to 35–40% [2:12][4:4].
- What is the "leucine trigger"? The leucine trigger is the minimum concentration of the amino acid leucine required within skeletal muscle cells to activate the mTORC1 pathway and initiate muscle protein synthesis. This is typically achieved by consuming 2.5–3.0 g of leucine in a single meal [1:15][8:7].
- Does whey protein help preserve muscle during dieting? Yes, whey protein isolate is highly effective because it has a high concentration of branched-chain amino acids, particularly leucine. It is absorbed rapidly, making it an excellent tool to hit the leucine trigger and support muscle protein synthesis under caloric restriction [5:4][8:8].
Glossary
- Anabolic Resistance: The reduced sensitivity of skeletal muscle to stimulate protein synthesis in response to amino acid consumption and resistance exercise, common in older adults.
- Leucine Trigger: The intracellular leucine threshold required to activate mTORC1 and initiate muscle protein synthesis.
- mTORC1: Mechanistic Target of Rapamycin Complex 1; the primary protein complex that regulates cellular growth and anabolic protein synthesis.
- Sarcopenic Obesity: The co-occurrence of low skeletal muscle mass and high adipose tissue mass, which severely limits physical function.
Methods (Transparency)
A systematic clinical literature search was performed in PubMed, Web of Science, and Embase. Focus was prioritized on randomized controlled trials (RCTs), systematic reviews, and meta-analyses investigating body composition, muscle protein synthesis, leucine kinetics, and progressive resistance training during active energy deficits.
¶ References
¶ Update Log
- 2026-07-06: Initial publication of the Muscle Preservation clinical guide.
Šantić R, Martinović L, Pavlović N, et al. Lean Mass and Musculoskeletal Preservation in GLP-1-Based Obesity Treatment: Nutrition, Exercise, Supplementation, and Monitoring Strategies. Metabolites. 2026 May 27;16(6):320. https://pubmed.ncbi.nlm.nih.gov/42346344/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Alawadhi AA, Alroudhan D, Alsaeed DJ, et al. LEAN mass Preservation with Resistance Exercise and Protein during semaglutide and tirzepatide therapy (LEAN-PREP study): a protocol for a randomised controlled trial. BMJ Open. 2026 Apr 22;16(4):e090128. https://pubmed.ncbi.nlm.nih.gov/42020128/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bosomworth NJ. New drugs for weight loss: Why change in body composition matters and why nutrition and exercise remain paramount. Can Fam Physician. 2025 Nov-Dec;71(11):785-792. https://pubmed.ncbi.nlm.nih.gov/41285626/ ↩︎
De Girolamo G, Sangineto M, Di Gioia G, et al. Muscle health in the modern era of incretin-based therapies. Eur J Clin Invest. 2026 Jan;56(1):e14452. https://pubmed.ncbi.nlm.nih.gov/41328795/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Barana L, De Fano M, Cavallo M, et al. Nutrition and Physical Activity in Optimizing Weight Loss and Lean Mass Preservation in the Incretin-Based Medications Era: A Narrative Review. Nutrients. 2025 Dec 31;18(1):124. https://pubmed.ncbi.nlm.nih.gov/41515247/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Goldenshluger A, Friedman L, Turjeman T, et al. Exercise Modalities to Preserve Muscle Mass and Bone Health After Metabolic Bariatric Surgery. J Cachexia Sarcopenia Muscle. 2026 Jun;17(3):1122-1135. https://pubmed.ncbi.nlm.nih.gov/42057763/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Spahits H, Unterberger S, Aschauer R, et al. Impact of a high-protein diet with and without strength training over 17 weeks on the plasma metabolome in older adults. Age Ageing. 2026 Feb 1;55(2):afad242. https://pubmed.ncbi.nlm.nih.gov/41638233/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kim CB, Sung J, Ahn D, et al. Independent and Combined Effects of Resistance Training and Whey Protein on Skeletal Muscle Mass and Function in Individuals with MASLD Under Caloric Restriction. Nutrients. 2025 Dec 26;17(24):5120. https://pubmed.ncbi.nlm.nih.gov/41515201/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
de Oliveira GS, do Carmo AS, do Carmo SG, et al. Multicomponent Online Intervention Improves Sarcopenia-Related Traits Following Long-Term Metabolic Bariatric Surgery: A Randomized Clinical Trial. Obes Surg. 2026 Jul;36(7):1920-1932. https://pubmed.ncbi.nlm.nih.gov/42168690/ ↩︎
Sancho-Haro E, Muñoz-López M, Baz-Valle E, et al. Optimizing Weight Loss in the GLP-1 Era: Preserving Muscle Mass, Function and Metabolic Health Through Precision Nutrition and Resistance Training. Pharmaceuticals (Basel). 2026 Jun 5;19(6):442. https://pubmed.ncbi.nlm.nih.gov/42356514/ ↩︎ ↩︎ ↩︎ ↩︎
Eisa N, Barood O. Lean Mass Changes With Incretin Therapy Versus Lifestyle Intervention: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Diabetes Obes Metab. 2026 Jun;28(6):1420-1433. https://pubmed.ncbi.nlm.nih.gov/41877354/ ↩︎
Eglseer D, Reiter L, Schoufour JD, et al. Is higher protein intake during weight loss interventions in older adults associated with improved outcomes? A secondary data analysis of three randomised controlled trials. Nutr J. 2026 Jan 22;25(1):9. https://pubmed.ncbi.nlm.nih.gov/41572290/ ↩︎ ↩︎ ↩︎