¶ Adenomyosis
| Condition Type | Benign, Estrogen-Dependent Uterine Disorder |
| Primary Symptoms | Heavy Menstrual Bleeding (HMB), Severe Dysmenorrhea, Chronic Pelvic Pain, Dyspareunia, Infertility |
| Primary Diagnosis | Transvaginal Ultrasound (TVUS), Magnetic Resonance Imaging (MRI) |
| First-Line Medical | LNG-IUD, COCPs (continuous), Oral Progestins (Dienogest), NSAIDs, Tranexamic Acid (TXA) |
| Advanced Interventions | GnRH Agonists/Antagonists, Letrozole, Uterine Artery Embolization (UAE), Conservative Surgery |
| Key Risks / Red Flags | Severe Chronic Anemia, Endometrial Ablation Failure, Post-Surgical Uterine Rupture |
| Prevalence | ~1% globally in general population; up to 41–49% in symptomatic and 31% in infertile cohorts |
Adenomyosis is a common, estrogen-dependent gynecological disorder characterized by the benign presence of ectopic endometrial glands and stroma within the myometrium [1][2], which is associated with uterine volume enlargement and peripheral smooth muscle hypertrophy [3]. Historically considered a histopathological diagnosis made retrospectively at hysterectomy, advances in non-invasive imaging have shifted the clinical landscape, revealing a high prevalence of adenomyosis in younger patients presenting with severe pelvic pain and subfertility [4]. In patients with infertility undergoing assisted reproductive technologies (ART), the presence of adenomyosis is associated with lower live birth and clinical pregnancy rates [5].
¶ At a Glance
¶ Header / Overview
Adenomyosis typically presents in reproductive-age individuals with symptoms such as heavy menstrual bleeding (HMB), severe dysmenorrhea, and pelvic pain [6][4:1]. Clinical examination often reveals uterine tenderness on bimanual pelvic exam, which serves as an independent predictor of the disease regardless of uterine size or the presence of concomitant fibroids [7]. Clinical management centers on non-surgical hormone suppression, utilizing intrauterine or oral regimens, while reserving surgical options for uterine-preserving fertility restoration or definitive cure [6:1][8].
¶ Safety "Traffic Light" (Contraindications & Alerts)
- Deep Adenomyosis & Ablation: Traditional endometrial ablation has a high failure rate in patients with deep adenomyosis (invasion >2.5 mm, as defined by McCausland and McCausland in 1998 [9] and verified by Mengerink et al. in 2015 [10]), often leading to persistent symptoms and the subsequent need for salvage hysterectomy [9:1][10:1].
- Hormonal Therapies and Pregnancy: Standard pharmacotherapeutic profiles establish that hormonal suppressive agents (such as combined oral contraceptives, oral progestins like dienogest, and GnRH modulators) are contraindicated during active pregnancy and must be discontinued prior to attempting conception.
- Cardiovascular Risk: Estrogen-containing combined contraceptives should be carefully evaluated for cardiovascular contraindications, especially in older patients or smokers [11].
¶ Protocol Card
An integrated, stepped clinical protocol ensures systematic verification, staging, and escalation of therapeutic modalities [6:2][12]:
| Step | Intervention | Clinical Priority / Dosing | Duration | Primary Clinical Target |
|---|---|---|---|---|
| Step 1 | Diagnostic Verification | Bimanual pelvic examination [13][7:1], Transvaginal Ultrasound (TVUS) [14]. Pelvic MRI if TVUS is inconclusive [14:1][15]. | Baseline / Initial Work-up | Exclude pregnancy, pelvic infection, and malignancy; map co-occurring fibroids or endometriosis [6:3][4:2]. |
| Step 2 | NSAIDs & Antifibrinolytics | Ibuprofen or Mefenamic Acid (scheduled); Tranexamic Acid (TXA) during menses [6:4]. | During menses | Direct pain relief and reduction of heavy blood loss [6:5]. |
| Step 3 | First-Line Suppressive | Levonorgestrel-Releasing Intrauterine Device (LNG-IUD) [16][17] or continuous oral progestins like Dienogest 2 mg daily continuously, as evaluated in 2025 by Vannuccini et al. [12:1]. | Long-term (up to 5–6 years for device [16:1]) | Induce endometrial atrophy, reduce HMB and pain [16:2][17:1]. |
| Step 4 | Advanced Suppression | Oral GnRH Antagonists (Relugolix, Elagolix) with add-back therapy [18][19], or GnRH Agonist depot [18:1]. | Suppression tailored to symptoms [6:6], or 3–6 cycles prior to IVF [20]. | Pronounced hypogonadotropic hypogonadism, uterine and lesion shrinkage [21][22]. |
| Step 5 | Conservative / Surgical | Uterine Artery Embolization (UAE) [23], conservative adenomyomectomy [8:1], or definitive hysterectomy [6:7]. | Individualized | Refractory symptoms, fertility preservation, or definitive cure [6:8][8:2]. |
¶ Bottom Line
Adenomyosis is a highly prevalent, estrogen-dependent condition that is best diagnosed non-invasively via high-resolution transvaginal ultrasound or pelvic MRI. Clinical management centers on long-term medical hormone suppression (using LNG-IUD or continuous progestins) to control heavy menstrual bleeding and dysmenorrhea, reserving conservative surgery or definitive hysterectomy for refractory cases.
¶ What is Adenomyosis?
¶ Pathophysiological Definition
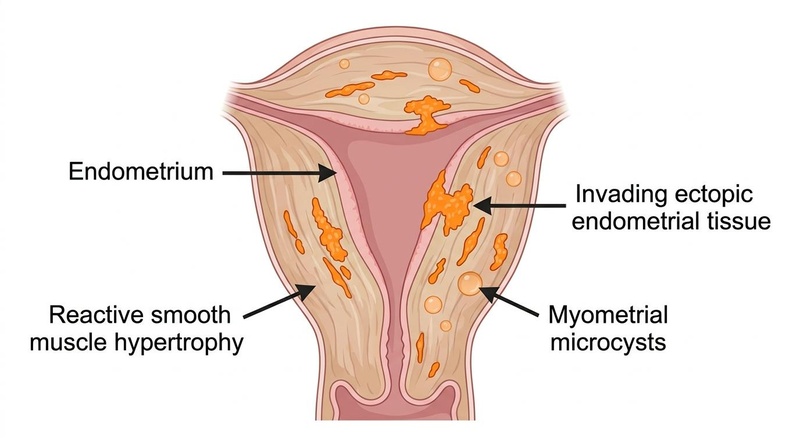
Adenomyosis is a benign gynecological condition characterized by the presence of endometrial glands and stroma pathologically demonstrated within the uterine myometrium [1:1]. This ectopic invasion is associated with uterine volume enlargement and reactive peripheral smooth muscle hypertrophy [3:1]. Ectopic tissue undergoes cyclical hormonal proliferation and micro-hemorrhage [2:1][24], promoting localized tissue changes, angiogenesis, inflammation, and fibrosis [25][26].
Two primary theories of pathogenesis are proposed:
- Invagination Theory: The most accepted model proposes that adenomyosis occurs by direct invagination of the basalis endometrium deep into the myometrium [2:2][27]. The process of invagination and intramyometrial spreading may be facilitated by the non-cyclic, anti-apoptotic activity of the basalis associated with relative hyper-oestrogenic states [2:3].
- De Novo Metaplasia Theory: An alternative model discusses the metaplasia of embryonic pluripotent Müllerian remnants, particularly for pelvic locations outside the uterus (such as retroperitoneal and rectovaginal adenomyotic nodules) [28].
¶ Pathogenesis and Molecular Drivers
Modern next-generation sequencing (NGS) and molecular research have substantially enhanced our understanding of the pathophysiology of adenomyosis:
- Epithelial Somatic KRAS Mutations: Next-generation sequencing has demonstrated that adenomyosis arises as an oligoclonal tissue from cells carrying specific driver mutations, as reviewed by Bulun et al. (2021) [29]. Activating somatic KRAS mutations are specifically located within the endometrial epithelial cells of both the ectopic adenomyotic lesions and adjacent eutopic basalis endometrial glands [29:1].
- Pathophysiological Consequences: Downstream signaling from these somatic KRAS mutations is associated with key pathological features [29:2]:
- Cell Proliferation & Survival: Enhances survival pathways within the myometrial microenvironment [29:3].
- Progesterone Resistance: Contributes to progesterone resistance by downregulating progesterone receptor expression, impairing normal responsiveness to progestin therapies [29:4].
- Estrogen Biosynthesis: Promotes common pathways favoring increased local estrogen production, decreased estradiol metabolism, and a unique estrogen receptor-beta (ESR2)-driven inflammatory process within the myometrium [29:5].
- Intracellular Signaling Cascades: Beyond steroid receptor dysfunction, the initiation and progression of adenomyosis-associated tissue proliferation, migration, invasion, angiogenesis, and fibrosis are driven by several key intracellular pathways. These include the CXCL/CXCR, NLRP3 inflammasome, NF-κB, TGF-β/Smad, VEGF, Hippo/YAP, PI3K/Akt/mTOR, and JAK/STAT signaling networks, representing promising targets for future non-hormonal drug development, as summarized by Zhang et al. (2024) [30].
¶ Relationship with Endometriosis and Leiomyomas
While historically treated as isolated entities, adenomyosis, endometriosis, and uterine leiomyomas (fibroids) are closely related, estrogen-dependent disorders that frequently overlap in clinical practice [1:2][23:1]:
- Co-occurrence Rates: In a large-scale meta-analysis of over 198 million women by Wang et al. (2025) [31], the global prevalence of adenomyosis in the general population was found to be approximately 1%. However, among patients experiencing gynecological symptoms, the prevalence was substantially higher, with estimates ranging between 41% and 49% [31:1], while in patients experiencing infertility, the prevalence of adenomyosis was approximately 31% [31:2]. This condition frequently coexists with other estrogen-dependent pelvic pathologies, such as endometriosis and uterine fibroids, which significantly complicates the clinical presentation and non-invasive diagnostic process [4:3][31:3][13:1][7:2]. (See also: Women's Longevity Guide and Perimenopause and Menopause Longevity).
- Shared Pathobiology: These conditions are estrogen-dependent and share common pathogenic features, derived from estrogen-dependent overproliferation of endometrial-like tissue and its subsequent implantation in ectopic sites [1:3].
- Diagnostic Differentiation: Because their symptoms (such as heavy bleeding and dysmenorrhea) overlap significantly, advanced non-invasive imaging is critical for accurate differentiation [6:9][29:6]. Transvaginal ultrasound (TVUS) serves as a highly accurate first-line diagnostic method [14:2], though magnetic resonance imaging (MRI) is recommended for women with associated leiomyomas to improve diagnostic accuracy and resolve pelvic co-occurrences [32].
¶ Clinical Presentation & Symptoms
The clinical severity of adenomyosis correlates with the extent of myometrial involvement and the severity of the lesions [6:10][4:4].
¶ Core Symptoms
- Heavy Menstrual Bleeding (HMB): Heavy menstrual bleeding is the most common symptom of adenomyosis, presenting in the majority of symptomatic patients (as approximately two-thirds of patients with adenomyosis are symptomatic) [4:5]. Abnormal uterine bleeding is a primary clinical presentation of adenomyosis (classified under the FIGO PALM-COEIN framework), which has a significant impact on quality of life and is often accompanied by severe pain and reduced fecundity [33][34]. These clinical manifestations are linked to complex molecular and cellular alterations, including localized inflammation, tissue fibrosis, and smooth muscle hypertrophy within the myometrium [3:2][25:1][26:1].
- Severe Dysmenorrhea: Dysmenorrhea is a hallmark symptom of adenomyosis, typically characterized by moderate to severe pelvic pain during menstruation, reported by the vast majority of symptomatic patients [6:11]. Pain is managed effectively using progestins or other hormonal suppressive options to suppress ectopic lesion activity [12:2].
- Chronic Pelvic Pain: Approximately two-thirds of patients with adenomyosis are symptomatic, with pelvic pain and heavy menstrual bleeding being the most common clinical presentations [4:6].
- Dyspareunia: Pain during intercourse is a common pelvic symptom of adenomyosis, which frequently co-occurs with endometriosis and can significantly compromise reproductive-age quality of life [12:3][13:2].
- Fertility Associations: Adenomyosis is associated with reduced endometrial receptivity and altered assisted reproductive outcomes [5:1]. This includes alterations in the junctional zone, which normally contributes to uterine peristalsis [35], as well as localized tissue-level inflammation [20:1][25:2] and fibrosis [25:3][26:2]. In patients undergoing assisted reproductive technologies (ART), the condition is associated with lower embryo implantation rates [5:2], lower clinical pregnancy and live birth rates [5:3][20:2], and an increased risk of miscarriage [20:3].
¶ Associated Morbidities & Emergencies
- Iron-Deficiency Anemia: Chronic, heavy menstrual blood loss frequently depletes systemic iron stores, presenting as microcytic anemia characterized by fatigue and dyspnea [4:7]. The management of iron deficiency and iron-deficiency anemia, which often occur secondary to chronic blood loss in adenomyosis, should be addressed using iron replacement therapy to restore systemic iron stores [36].
- Adolescent Presentation: In adolescent populations presenting with severe heavy menstrual bleeding, differential diagnosis requires careful stratification. A systematic review of 2,770 adolescent patients by Hall et al. (2024) found that ovarian-uterine disorders (23.7%) and coagulation disorders (19.4%) represent the most common organic causes of adolescent HMB, although 45.9% of cases remain of indeterminate origin [37].
¶ Diagnostics & Differential Diagnosis
Accurate diagnosis relies on high-resolution non-invasive imaging, which has largely replaced histological evaluation of hysterectomy specimens [6:12][4:8].
¶ Transvaginal Ultrasound (TVUS)
Transvaginal ultrasound is the primary non-invasive diagnostic modality [14:3]. It serves as a reliable first-line tool with high specificity for detecting changes in myometrial texture and uterine volume [4:9][14:4].
Ultrasound signs of adenomyosis are categorized into direct signs (which reflect the presence of ectopic endometrial tissue within the myometrium, such as subendometrial microcysts or echogenic buds) and indirect signs (which reflect reactive changes in the surrounding myometrium, such as asymmetrical wall thickening, fan-shaped shadowing, or an obscured or irregular junctional zone) [38]. While the presence of at least one direct sign represents a strong marker of disease, clinical history and symptoms remain essential, as symptomatic patients may still have highly probable adenomyosis even in the absence of direct ultrasound signs [38:1].
- Ultrasound Elastography: This emerging diagnostic technique measures tissue mechanical properties and elasticity. Ultrasound elastography offers high sensitivity and specificity for confirming adenomyosis lesions, as shown by Brunelli et al. (2023) [39].
¶ Magnetic Resonance Imaging (MRI) Criteria
Pelvic MRI is indicated when transvaginal ultrasound findings are inconclusive, or when detailed mapping of focal versus diffuse disease is clinically necessary [14:5][15:1].
Key MRI criteria include:
- Junctional Zone (JZ) Thickness: As reviewed by Agostinho et al. in 2017 [40], on pelvic MRI, a maximum junctional zone thickness (JZmax) of at least 12 mm on T2-weighted sequences is a highly specific and diagnostic threshold of adenomyosis. For infertile women, a JZ thickness is associated with poor fertility outcomes [41].
- T2-Weighted High-Signal Intensity Foci: Punctate foci of high signal intensity scattered throughout the thickened, hypointense junctional zone represent islands of ectopic endometrial tissue and cystic dilation of glands [40:1].
- Anatomical Phenotypes: Pelvic MRI allows clear distinction between lesions of the external myometrium and those of the internal myometrium, which are associated with distinct epidemiological and clinical characteristics [41:1].
¶ Histopathological Diagnosis
While non-invasive imaging is standard for clinical management, histopathology of hysterectomy or biopsy specimens remains the reference standard [4:10]:
- Standardized Pathology Criteria: Standardized pathology criteria define adenomyosis as the presence of endometrial glands and/or stroma located greater than 2 mm into the myometrium, or involving more than one-third of the total myometrial thickness, in hysterectomy specimens [42]. Routine examination of hysterectomy specimens with benign indications should include 4 to 6 tissue blocks to minimize inter-pathologist variability, and a single gland or stromal focus is sufficient for a definitive diagnosis, as established by the international Delphi consensus study by McCaughey et al. (2025) [42:1]. Hysteroscopic endomyometrial biopsy can also provide tissue-level diagnostic verification before surgery, showing high sensitivity (86.36%) and specificity (90%) [43].
¶ Differential Diagnosis Checklist
To avoid diagnostic errors, clinicians must systematically perform a thorough clinical assessment and select appropriate diagnostic methods:
[ ] Clinical and Bimanual Examination
- Action: Perform bimanual pelvic examination to evaluate uterine tenderness and size [^33][^43].
- Clinical Predictors: Check for uterine tenderness, which is an independent predictor of adenomyosis regardless of whether uterine size is larger or smaller than 14 weeks [^43].
[ ] Transvaginal Ultrasound (TVUS)
- Action: Perform TVUS as the primary first-line diagnostic imaging modality [^25].
- Exclusions: Evaluate myometrial involvement and JZ characteristics [^18][^25].
[ ] Magnetic Resonance Imaging (MRI)
- Action: Recommended as a second-line imaging method if TVUS is inconclusive [^25], or if coexisting leiomyomas are present [^38].
- Exclusions: Map focal vs diffuse disease and evaluate JZmax thickness [^17].
[ ] Hysteroscopic Endomyometrial Biopsy
- Action: Consider hysteroscopic endomyometrial biopsy to complement imaging in cases of abnormal uterine bleeding [^27].
- Exclusions: Provides tissue-level diagnostic verification before surgery, showing high sensitivity (86.36%) and specificity (90%) [^27]. (For managing symptoms of dysmenorrhea, see also the [Period Pain Action Guide](../guides/period-pain-action-guide.md)).
¶ Differential Diagnosis Table
The clinical symptoms of adenomyosis mimic several gynecological, neoplastic, and physiological states. To avoid inappropriate treatment or surgical missteps, these entities must be systematically distinguished.
| Diagnosis | Distinguishing Clinical Features | Key Diagnostic Findings |
|---|---|---|
| Endometriosis | Cyclic pelvic pain, deep dyspareunia, and infertility [1:4]. | Endometriosis and adenomyosis share clinical and pathogenic features and frequently coexist, showing similar estrogen-dependent overproliferation as discussed by Donnez et al. (2024) [1:5]. |
| Uterine Fibroids (Leiomyomas) | Bleeding, pelvic pain, and uterine enlargement [4:11]. | Fibroids and adenomyosis cause overlapping symptoms and frequently coexist, requiring high-resolution imaging (such as transvaginal ultrasonography or MRI) to differentiate the lesions as noted by Schrager et al. (2022) [4:12]. |
| Pelvic Inflammatory Disease (PID) | Bilateral pelvic pain, purulent cervical discharge, tenderness, fever, and acute onset. | Leukocytosis, elevated CRP, positive cervical swab; TVUS showing hydrosalpinx. |
| Endometrial Malignancy / Hyperplasia | Persistent abnormal uterine bleeding in reproductive-aged or postmenopausal women. | Evaluated under the FIGO PALM-COEIN system described by Munro et al. (2011) [44], where malignancy and hyperplasia constitute distinct categories of abnormal uterine bleeding. |
¶ Differential Diagnosis: Excluding Key Mimics
To avoid diagnostic error and inappropriate treatment, clinicians must systematically exclude key mimics—specifically pregnancy, pelvic inflammatory disease (PID), and pelvic/uterine malignancies—prior to establishing a diagnosis of adenomyosis or initiating suppressive therapy [6:13][4:13].
[ ] Pregnancy Exclusion
- Clinical Indicator: Uterine enlargement, softening, amenorrhea, and pelvic congestion can mimic adenomyosis [^20].
- Diagnostic Step: Perform qualitative or quantitative serum/urine beta-hCG testing for all reproductive-age individuals before initiating hormonal suppressive therapies or undergoing procedures [^1].
[ ] Pelvic Infection / PID Exclusion
- Clinical Indicator: Bimanual uterine tenderness, severe chronic pelvic pain, dyspareunia, and abnormal bleeding can overlap with active pelvic infections or pelvic inflammatory disease (PID) [^1][^43].
- Diagnostic Step: Perform bimanual pelvic examination to evaluate for uterine, cervical motion, or adnexal tenderness [^33][^43]. Rule out active pelvic infections clinically prior to embarking on uterine interventions or intrauterine device placement [^1][^20].
[ ] Pelvic & Uterine Malignancy Exclusion
- Clinical Indicator: Abnormal uterine bleeding (AUB), irregular endometrial-myometrial margins, and rapidly growing uterine masses can mimic endometrial carcinoma, uterine sarcoma, or carcinosarcoma [^17][^21].
- Diagnostic Step: Perform transvaginal ultrasound (TVUS) to assess endometrial thickness and stripe regularity [^25]. Conduct endometrial sampling (biopsy) or hysteroscopy-guided biopsy in patients presenting with unexplained or abnormal uterine bleeding to rule out endometrial hyperplasia or malignancy [^1][^21][^27]. Obtain a pelvic MRI to differentiate benign adenomyotic lesions from uterine sarcomas or endometrial stromal sarcomas, utilizing T2-weighted and diffusion-weighted imaging (DWI/ADC, where a relatively high apparent diffusion coefficient suggests a benign lesion) [^17][^47].
¶ Actionable Clinical Protocols
An integrated, stepped clinical protocol ensures systematic verification, staging, and escalation of therapeutic modalities [6:14][12:4].
+-------------------------------------------------------------------------+
| STEP 1: DIAGNOSTIC VERIFICATION & EVALUATION |
| Perform patient clinical history, bimanual pelvic examination (checking |
| for uterine tenderness and size) [^33][^43], and first-line TVUS [^25]. |
| Systematic exclusion of mimics (pregnancy, PID, malignancy) completed |
| prior to starting therapy [^1][^20]. If TVUS is inconclusive or |
| coexisting leiomyomas are present, utilize pelvic MRI as a second-line |
| tool to identify co-occurring pelvic pathologies [^20][^25][^26][^38]. |
+-------------------------------------------------------------------------+
|
v
+-------------------------------------------------------------------------+
| STEP 2: PHENOTYPIC STAGING & CLINICAL PRIORITIZATION |
| Categorize the patient into one of three primary clinical phenotypes: |
| |
| A. Hemorrhagic Phenotype: Dominant HMB, microcytic anemia, or history |
| of acute bleeding episodes [^20][^23]. |
| B. Algic Phenotype: Dominant severe dysmenorrhea and chronic pelvic |
| pain; refractory to over-the-counter analgesics [^3]. |
| C. Reproductive Phenotype: Active or planned fertility/conception |
| goals; history of recurrent implantation failure [^12]. |
+-------------------------------------------------------------------------+
|
v
+-------------------------------------------------------------------------+
| STEP 3: TARGETED THERAPEUTIC PATHWAY ESCALATION |
| Implement phenotype-specific therapeutic pathways: |
| |
| A. Hemorrhagic Escalation: |
| - Anemia screening and monitoring of hemoglobin and ferritin levels; |
| iron replacement initiated according to established guidelines [^23].|
| - First-Line Suppressive: Insert LNG-IUD (gold standard) if uterine |
| volume allows [^9][^13]. |
| - Refractory: Escalate to oral progestins (Dienogest) or GnRH |
| antagonists with add-back therapy [^7][^8]. |
| |
| B. Algic Escalation: |
| - Scheduled NSAIDs starting prior to menses [^1]. |
| - First-Line Suppressive: LNG-IUD [^9] or continuous COCPs [^1][^41].|
| - Second-Line: Oral Dienogest 2 mg daily, shown to be effective over |
| 3 years by Vannuccini et al. in 2025 [^3]. |
| - Refractory: GnRH agonist depot or oral GnRH antagonists |
| with add-back therapy [^7][^8]. |
| |
| C. Reproductive Escalation: |
| - Avoid long-term suppressors that block ovulation [^12]. |
| - For ART preparation: Long-course GnRH agonist suppression |
| prior to frozen embryo transfer (FET) [^12]. |
| - Refractory focal lesions: Specialized conservative surgery |
| (uterine-sparing excision or reduction techniques) with |
| post-operative suppressive therapy [^2][^32]. |
+-------------------------------------------------------------------------+
¶ Pre-treatment Clinical Framework (Embryo Transfer)
To optimize reproductive success, Chandra et al. (2026) outlined a pragmatic, clinically oriented framework for individualizing pre-treatment in infertile women based on uterine and JZ morphology:
- For a uterine volume of 100–200 mL and maximum JZ thickness (JZmax) of 8.5–16 mm: medical pre-treatment with GnRH agonists for 3 to 6 cycles followed by IVF [41:2].
- For a uterine volume of and JZmax of : consideration of uterus-sparing surgery in highly selected patients, followed by IVF with an ultra-long protocol [41:3].
- For a uterine volume of and JZmax of : direct IVF, preferably utilizing an ultra-long protocol combined with a freeze-all and hormone replacement therapy frozen embryo transfer (HRT-FET) strategy [41:4].
¶ Clinical Algorithm for Differential Exclusions
Patient with HMB / Severe Dysmenorrhea / Globular Uterus
│
▼
Perform Bimanual Pelvic Exam &
Serum/Urine beta-hCG
│
┌─────────────────┴─────────────────┐
▼ ▼
beta-hCG Positive beta-hCG Negative
│ │
▼ ▼
Pregnancy Confirmed; Evaluate for PID:
Exclude suppressive therapy Check for cervical motion or
adnexal tenderness, purulent discharge
│
┌─────────────────────┴─────────────────────┐
▼ ▼
Signs of PID No Signs of PID
│ │
▼ ▼
Treat PID with Antibiotics Perform TVUS &
prior to intrauterine device Exclude Malignancy
or uterine procedures - If endometrial stripe
irregular, perform biopsy
- Differentiate focal adenomyoma
from leiomyomas or sarcomas
│
▼
Exclusions Cleared;
Proceed with Adenomyosis Staging
¶ Therapeutic Modalities & Pharmacology
¶ First-Line Medical Therapies
- Non-Steroidal Anti-inflammatory Drugs (NSAIDs): Scheduled dosing of NSAIDs (such as ibuprofen or mefenamic acid) initiated 1–2 days prior to the onset of menses provides direct anti-inflammatory pain relief by inhibiting prostaglandin synthesis, though it does not affect lesion volume or disease progression [6:15].
- Tranexamic Acid (TXA): This antifibrinolytic is administered during menstruation (e.g., 1–1.5 g three to four times daily for up to 4 days) to significantly reduce heavy menstrual blood loss, particularly in patients with contraindications to hormonal therapies [6:16].
- Combined Oral Contraceptive Pills (COCPs): Continuous administration of COCPs is recommended as a first-line option to manage adenomyosis symptoms, specifically tailored to address HMB and pelvic pain by inducing endometrial decidualization and subsequent atrophy [1:6].
¶ Hormonal Suppressive Options
- Levonorgestrel-Releasing Intrauterine Device (LNG-IUD / LNG-IUS): The LNG-IUD is considered the gold-standard medical therapy for symptomatic adenomyosis [16:3]. By releasing levonorgestrel directly into the uterine cavity, it induces profound endometrial atrophy, significantly reducing menstrual blood loss and dysmenorrhea [16:4][17:2]. High-quality cohorts demonstrate sustained efficacy for up to 5 years, though patients with a uterine volume exceeding 150 mL have a higher rate of expulsion and treatment failure [45].
- Oral Progestins (Dienogest & Desogestrel):
- Dienogest: Oral dienogest is highly effective for reducing pelvic pain, outperforming other hormonal options [26:3]. Continuous oral dosing of dienogest at 2 mg daily continuously achieved a 50% composite success rate for resolving chronic pelvic pain and HMB at 6 months, while achieving a 7.3% reduction in uterine volume and a 14% reduction in junctional zone thickness in a randomized trial by Refaat et al. (2026) [46].
- Desogestrel: Continuous desogestrel at 75 mcg daily represents a safe alternative in patients with contraindications to exogenous estrogens [11:1].
- Mifepristone: In a randomized controlled trial by Che et al. (2023), low-dose mifepristone (10 mg daily continuously for 12 weeks) achieved 91.8% effective pain remission, 88.5% complete remission of dysmenorrhea, and a significant mean reduction of 29.3 cm³ in uterine volume compared to placebo [47].
¶ GnRH Agonists & Antagonists
- GnRH Agonists (e.g., Goserelin, Leuprolide): Administered as a monthly depot (e.g., Goserelin 3.6 mg), GnRH agonists induce a temporary hypoestrogenic state, leading to profound shrinkage of ectopic lesions and significant reductions in uterine volume [18:2][25:4]. Due to severe hypoestrogenic side effects and bone mineral density loss, their use is typically restricted to short courses (3 to 6 cycles) or utilized as a pre-treatment before assisted reproductive technology or surgery [41:5].
- GnRH Antagonists (e.g., Relugolix, Elagolix): Oral GnRH antagonists offer immediate, competitive blockade of pituitary GnRH receptors, bypassing the clinical flare effect and allowing dose-dependent estrogen suppression [19:1]. Combined with hormonal add-back therapy (e.g., Relugolix 40 mg, estradiol 1 mg, norethindrone acetate 0.5 mg daily), this regimen significantly reduces uterine volume (22.2% reduction demonstrated in the LIBERTY trials) and manages pain over long-term courses [22:1].
- Aromatase Inhibitors (Letrozole): Pathological gene expression pathways in adenomyosis favor increased local estrogen biosynthesis and progesterone resistance. Low-dose letrozole (2.5 mg three times weekly for 3 months) is an effective, low-cost option that significantly improves symptoms and reduces sonographic features of adenomyosis in patients awaiting IVF, with the unique advantage of preserving regular menstrual cycles [25:5]. Pre-treatment with low-dose letrozole prior to frozen embryo transfer significantly improves endometrial expression of receptivity markers (progesterone receptors and integrin ), achieving reproductive outcomes comparable to GnRH agonist pre-treatment [48].
¶ Non-Surgical & Minimally Invasive Interventions
- Uterine Artery Embolization (UAE): This interventional procedure involves bilateral occlusion of the uterine arteries to induce ischemic necrosis of adenomyotic tissue. In a randomized trial comparing UAE directly to oral dienogest (2 mg/day) over 6 months, UAE achieved significantly higher complete resolution rates for chronic pelvic pain (93.3% vs. 66.7%) and HMB (90.0% vs. 56.7%), yielding an 86.7% composite success rate compared to 50.0% in the dienogest group [46:1]. UAE also achieved superior anatomical outcomes, with a 17.6% reduction in uterine volume and a 33.5% reduction in junctional zone thickness at 6 months [46:2].
- High-Intensity Focused Ultrasound (HIFU): HIFU is a non-excisional, uterus-sparing option that induces thermal necrosis of adenomyotic lesions. Chen et al. (2024) reported a pooled pregnancy rate post-HIFU of 53.4% and a live birth rate of 35.2% [49]. Combining HIFU with a GnRH agonist and a progestin is highly effective for reducing dysmenorrhea pain scores, while combining HIFU with a progestin alone is superior for decreasing uterine volume, lesion size, and recurrence rates [50].
- Microwave Ablation (MWA): Ultrasound-guided MWA and UAE both significantly reduce symptoms. However, the MWA group demonstrates superior postoperative recovery, with significantly shorter hospitalization (0 days vs. 3 days, ) and a faster return to daily activities (3 days vs. 14 days, ) compared to the UAE group [7:3].
CRITICAL CLINICAL WARNING: ENDOMETRIAL ABLATION LIMITATIONS
Endometrial ablation (e.g., thermal, radiofrequency, or rollerball ablation of the uterine cavity) has a high failure rate in patients with deep adenomyosis, which is defined by McCausland and McCausland in 1998 [9:2] and verified by Mengerink et al. in 2015 [10:2] as an invasion deeper than 2.5 mm [9:3][10:3]. Patients with deep endometrial penetration usually have persistent symptoms of heavy bleeding and pain after ablation, and should be offered hysterectomy over repeat ablation procedures [9:4][10:4]. Prior to performing any endometrial ablation for abnormal uterine bleeding, clinicians must systematically evaluate patients to rule out deep adenomyosis using TVUS or pelvic MRI [6:17][9:5].
¶ Surgical Interventions
- Conservative Surgery (Adenomyomectomy): Indicated for patients with symptomatic, focal adenomyosis (adenomyomas) who wish to preserve fertility [8:3]. Surgical techniques include the uterine muscle flap method, asymmetric dissection, or modified reduction techniques to excise focal lesions or cytoreduce diffuse adenomyosis [8:4]. While these procedures preserve uterine architecture, improve symptoms, and facilitate subsequent pregnancy, they carry a significant postoperative risk of uterine rupture during pregnancy and require meticulous suturing [8:5][51]. Laparoscopic adenomyomectomy appears to carry an elevated risk of uterine rupture in subsequent pregnancies compared to open laparotomy [8:6].
- Definitive Surgery (Hysterectomy): Total or subtotal hysterectomy (with preservation of the ovaries if premenopausal) is the only definitive cure for adenomyosis [6:18][4:14]. It is reserved for patients who have completed childbearing, have severe refractory symptoms, or have failed multiple medical or minimally invasive treatments [6:19]. For deep infiltrating endometriosis coexisting with adenomyosis, the ENDORAS randomized controlled trial (Renso et al., 2025) is actively evaluating whether robot-assisted total laparoscopic hysterectomy offers superior safety and lower complication rates compared to standard laparoscopy [35:1].
¶ Clinical Management, Recurrence, & Safety Tradeoffs
¶ Fertility Tradeoffs
The management of adenomyosis in patients wishing to conceive requires balancing symptom suppression against reproductive goals [16:5][5:4]. All effective medical therapies (LNG-IUD, COCPs, Dienogest, GnRH analogues) prevent ovulation or impair implantation, making them incompatible with active conception attempts [6:20]. Conversely, leaving severe adenomyosis untreated is associated with lower clinical pregnancy and embryo implantation rates [5:5], which is linked to JZ remodeling, inflammation, and hypercontractility [20:4].
For patients undergoing IVF/ICSI, a highly successful strategy is the administration of a GnRH agonist depot prior to a frozen embryo transfer (FET) [5:6][20:5]. This temporary suppression with GnRH modulators has been shown to improve clinical pregnancy and live birth rates [5:7][20:6], and is associated with significant reductions in uterine and lesion volume [21:1][22:2]. Additionally, a freeze-all (FET) strategy yields significantly higher clinical pregnancy and live birth rates in patients with endometriosis, whereas the outcomes for patients with isolated adenomyosis remain comparable between FET and fresh ET strategies [52].
¶ Obstetric and Perinatal Complications
Adenomyosis represents an independent risk factor for adverse obstetric and neonatal outcomes [53]:
- Adverse Obstetric Risks: Pregnant patients with adenomyosis are at significantly higher risk for several serious complications, which include:
- Pre-eclampsia and Hypertensive Disorders: A significantly elevated risk of pre-eclampsia and hypertensive disorders of pregnancy is documented in patients with adenomyosis, regardless of whether conception was achieved spontaneously or via ART [53:1][54].
- Preterm Birth (PTB): Elevated odds of preterm delivery are reported consistently in observational cohorts of women with adenomyosis compared to healthy controls [55]. Within adenomyosis cohorts, diffuse phenotypes show a significantly higher risk of preterm birth than focal lesions [54:1].
- Small for Gestational Age (SGA) & Low Birth Weight: Elevated rates of fetal growth restriction and SGA infants are consistently documented [16:6][55:1].
- Miscarriage and Recurrent Pregnancy Loss (RPL): Due to the adverse impact of adenomyotic lesions on the uterine environment, the 2022 ESHRE guidelines for recurrent pregnancy loss established a clinical recommendation to systematically investigate the presence of adenomyosis in patients presenting with RPL [56].
- Clinical Surveillance: Patients with severe adenomyosis should be considered at high obstetric risk and can benefit from early pre-pregnancy counseling and referral to tertiary care centers for close maternal-fetal surveillance [16:7].
¶ Recurrence Dynamics
Adenomyosis is a chronic, progressive condition that typically persists until menopause [4:15].
- Medical Discontinuation: Symptoms and uterine volume regularly return to baseline levels within several months after stopping suppressive medical therapies (LNG-IUD removal, progestin or GnRH antagonist cessation) [12:5][18:3].
- Surgical Recurrence: While conservative surgery (such as adenomyomectomy) is widely utilized to preserve fertility, relapse of symptoms remains a significant clinical challenge [57]. Patients undergoing conservative surgery alone experience a high rate of recurrence for dysmenorrhea and heavy menstrual bleeding at 36 months, which is significantly reduced when surgery is combined with postoperative LNG-IUS placement (32.84% vs. 2.94%, respectively) [58].
¶ Anemia Management Protocol
Chronic, heavy menstrual blood loss in patients with the hemorrhagic phenotype of adenomyosis frequently depletes systemic iron stores, presenting as iron-deficiency (ID) anemia [4:16][36:1]. Standard clinical practice dictates a proactive screening and management protocol:
- Active Screening: Clinicians should routinely monitor hemoglobin (Hb), hematocrit, and ferritin levels in symptomatic adenomyosis patients to identify preclinical iron deficiency and overt anemia [4:17][36:2].
- Oral Iron Replacement Therapy: For stable patients presenting with mild-to-moderate iron-deficiency anemia, oral iron supplementation is initiated as first-line therapy [36:3]. Patients are monitored for gastrointestinal tolerance and compliance, with regular follow-up of blood counts to verify therapeutic response [36:4].
- Intravenous (IV) Iron Replacement Therapy: Intravenous iron therapy is indicated for patients with severe anemia, those who exhibit severe gastrointestinal intolerance or poor response to oral iron, patients with malabsorption syndromes, or those with active hemorrhage exceeding oral absorption capacity [36:5]. Furthermore, pre-operative IV iron replacement is strongly recommended to optimize hemoglobin levels and correct anemia prior to undergoing conservative surgery or hysterectomy, minimizing the risk of perioperative allogeneic blood transfusion [36:6].
¶ Severe Bleeding Risk Management & Emergency Protocol
In cases of acute, severe abnormal uterine bleeding (AUB) causing hemodynamic instability or severe acute anemia, rapid stabilization and management are required [6:21][29:7].
- Emergency Assessment: Clinicians must promptly evaluate patients presenting with acute, heavy uterine hemorrhage for signs of hypovolemia or hemodynamic instability (such as tachycardia or hypotension) [6:22][29:8].
- Emergency Medical Suppression:
- For hemodynamically stable patients with severe bleeding, initial medical management is preferred to avoid surgical risks and preserve fertility [6:23][29:9].
- Stabilization regimens can include high-dose estrogen (oral or intravenous), high-dose combined oral contraceptives, oral progestins, or intravenous tranexamic acid to control active hemorrhage [6:24][29:10].
- Procedural and Surgical Interventions:
- If acute bleeding is refractory to medical therapy or if the patient is hemodynamically unstable, emergency interventions include mechanical uterine tamponade, dilation and curettage (D&C), or urgent uterine artery embolization (UAE) to occlude arterial supply and arrest hemorrhage [23:2][29:11].
- Definitively, emergency hysterectomy is indicated if the hemorrhage is life-threatening and refractory to all conservative medical and interventional procedures [6:25][29:12].
- Long-Term Management: Following stabilization, patients should be transitioned to a maintenance medical suppressive regimen, such as the levonorgestrel-releasing intrauterine system (LNG-IUD) or continuous oral progestins, to prevent recurrence of severe bleeding episodes [12:6][16:8][29:13].
¶ Evidence Summary Table (Human Outcomes)
| Intervention | Target Outcome / Goal | Effect* | Consistency | Evidence Quality | Trials | Clinical Context, Notes & Protocols |
|---|---|---|---|---|---|---|
| Levonorgestrel-IUS (LNG-IUS / LNG-IUD) | Dysmenorrhea Pain Reduction | High | High | Multiple Cohorts & RCTs | Sustained, profound reduction in pain scores; LNG-IUD local release, active for up to 5 years [16:9][17:3]; volume effect is inconsistent in large adenomyosis [45:1]. | |
| Levonorgestrel-IUS (LNG-IUS / LNG-IUD) | Menstrual Flow Reduction (HMB) | High | High | Multiple Cohorts & RCTs | Significant reduction in blood loss by 6–12 months with LNG-IUD [16:10][17:4]. | |
| Oral Dienogest (2 mg daily) | Dysmenorrhea Pain Control | High | High | Multiple RCTs | Continuous oral progestin; shown to be highly effective for reducing pelvic pain, outperforming other hormonal options [12:7][26:4]. | |
| Oral Dienogest (2 mg daily) | Uterine Volume Reduction | High | Moderate | Multiple RCTs | Continuous oral dosing of 2 mg daily continuously achieved a 7.3% reduction in uterine volume and a 14% reduction in junctional zone thickness at 6 months [46:3]. | |
| Mifepristone (10 mg daily) | Dysmenorrhea & Pain Suppression | High | High | Multicenter RCT | Oral dosing of 10 mg daily for 12 weeks; achieved 91.8% effective pain remission and 88.5% complete remission of dysmenorrhea compared to placebo [47:1]. | |
| Mifepristone (10 mg daily) | Uterine Volume Reduction | High | High | Multicenter RCT | Oral dosing of 10 mg daily for 12 weeks; achieved a significant mean reduction of 29.3 cm³ in uterine volume compared to placebo [47:2]. | |
| GnRH Agonists / Antagonists | Uterine & Lesion Volume Reduction | High | High | Multiple RCTs | Profound systemic estrogen suppression; Relugolix/GnRHa achieves significant reductions in uterine and lesion volume [21:2][22:3]; requires hormonal add-back therapy [19:2]. | |
| Uterine Artery Embolization (UAE) | Pelvic Pain & Bleeding Resolution | High | High | Randomized Controlled Trial | UAE achieved significantly higher complete resolution rates for pelvic pain (93.3% vs. 66.7%) and HMB (90.0% vs. 56.7%) at 6 months, outperforming dienogest [46:4]. | |
| Uterine Artery Embolization (UAE) | Uterine Volume Reduction | High | High | Randomized Controlled Trial | UAE achieved a 17.6% reduction in uterine volume and a 33.5% reduction in junctional zone thickness at 6 months [46:5]. | |
| Low-Dose Letrozole (AI) | Dysmenorrhea / Bleeding Improvement | Moderate | Moderate | Pilot Randomized Trial | Letrozole 2.5 mg orally three times weekly for 3 months; comparable to GnRHa in improving symptoms while uniquely preserving regular menses [25:6]. | |
| Low-Dose Letrozole (AI) | Endometrial Receptivity Markers | High | Moderate | Randomized Controlled Trial | Pre-FET letrozole therapy significantly improves endometrial expression of progesterone receptors and integrin [48:1]. | |
| Microwave Ablation (MWA) | Dysmenorrhea & Pelvic Pain | Moderate | Low | Pilot Randomized Trial | Ultrasound-guided MWA significantly reduced dysmenorrhea (NRS decreased from 6 to 1) and improved quality of life, demonstrating faster recovery than UAE [7:4]. | |
| NSAIDs | Acute Dysmenorrhea Relief | Moderate | Moderate | Systematic Reviews | Scheduled dosing provides temporary symptomatic relief but does not shrink lesions or affect disease progression [6:26]. | |
| Conservative Surgery | Fertility Preservation in Focal Disease | Low | Low | Cohort Studies | Specialized uterine-sparing excisional surgery; cytoreduction carries a risk of post-operative uterine rupture during pregnancy [8:7][51:1]. |
*Compact renderer encoding: <effect e="d2p"></effect> where the three-character e attribute code is composed of direction (u/d/e/q), magnitude (0–3), and health impact (p/n/x).
¶ Practical FAQ
How does adenomyosis differ from endometriosis?
Although both are chronic, estrogen-dependent inflammatory disorders that frequently co-exist, they represent distinct anatomical pathologies [1:7]. Endometriosis is defined by the presence of endometrial-like tissue implants outside the uterine cavity, most commonly on the pelvic peritoneum, ovaries, and fallopian tubes [1:8]. Adenomyosis is defined by the invasion of endometrial glands and stroma inside the uterine wall, directly penetrating into the myometrium, which leads to smooth muscle hypertrophy, globular uterine enlargement, and heavy menstrual bleeding [4:18].
Can adenomyosis cause infertility?
Yes, adenomyosis negatively impacts reproductive outcomes. Women with adenomyosis exhibit lower clinical pregnancy and live birth rates, alongside higher risks of miscarriage during IVF cycles, primarily driven by altered uterine peristalsis, chronic localized inflammation, and impaired embryo implantation [5:8][41:6]. Additionally, diffuse adenomyosis is significantly associated with an increased risk of adverse pregnancy outcomes compared to focal adenomyosis, including higher odds of preterm birth and hypertensive disorders of pregnancy [54:2].
Why is endometrial ablation risky for adenomyosis?
Endometrial ablation utilizes thermal energy, radiofrequency, or other modalities to destroy the endometrial lining of the uterine cavity to control heavy bleeding [9:6][10:5]. While effective for superficial endometrial pathologies, ablation has a high failure rate in patients with deep adenomyosis, which is defined as an invasion deeper than 2.5 mm [9:7][10:6]. Trapped ectopic endometrial tissue deep within the myometrium continues to proliferate and bleed cyclically, resulting in persistent pain and bleeding that frequently necessitates a salvage hysterectomy [9:8].
Will my symptoms return after stopping medical therapy?
Yes. Except for a total hysterectomy (which is a definitive cure) or reaching natural menopause, there is currently no permanent cure for adenomyosis [4:19]. All pharmacological suppressive treatments—including the LNG-IUD, oral progestins (dienogest), continuous oral contraceptives, and GnRH agonists/antagonists—work by temporarily suppressing ovarian function and starving the estrogen-dependent lesions [12:8][18:4]. Once these therapies are discontinued, clinical symptoms and uterine volume typically return to baseline levels within several months [12:9][18:5].
Is a hysterectomy the only way to treat adenomyosis?
No, a hysterectomy is the only definitive curative treatment, but multiple uterus-preserving and fertility-sparing medical and interventional options are available [6:27][4:20]. First-line progestins (such as continuous oral dienogest 2 mg or desogestrel 75 mcg) and the LNG-IUS have shown effectiveness for managing symptoms, with management frameworks also established by major clinical societies [6:28][11:2]. Interventional options such as uterine artery embolization (UAE), high-intensity focused ultrasound (HIFU), and microwave ablation (MWA) offer clinically validated, minimally invasive symptom and volume control [7:5][49:1][46:6].
¶ References
Donnez J, Stratopoulou CA, Dolmans MM. Endometriosis and adenomyosis: Similarities and differences. Best Practice & Research Clinical Obstetrics & Gynaecology. 2024;92:102435. https://pubmed.ncbi.nlm.nih.gov/38103509/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bergeron C, Amant F, Ferenczy A. Pathology and physiopathology of adenomyosis. Best Practice & Research Clinical Obstetrics & Gynaecology. 2006;20(4):511-521. https://pubmed.ncbi.nlm.nih.gov/16563870/ ↩︎ ↩︎ ↩︎ ↩︎
Moldassarina RS. Modern view on the diagnostics and treatment of adenomyosis. Archives of Gynecology and Obstetrics. 2023;308(1):15-24. https://pubmed.ncbi.nlm.nih.gov/37060397/ ↩︎ ↩︎ ↩︎
Schrager S, Yogendran L, Marquez CM. Adenomyosis: Diagnosis and Management. American Family Physician. 2022;105(1):64-71. https://pubmed.ncbi.nlm.nih.gov/35029928/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
French HM, Zhang W, Movilla PR, Loring M, Morris SN. Adenomyosis and fertility: does adenomyosis impact fertility and does treatment improve outcomes. Current Opinion in Obstetrics & Gynecology. 2022;34(4):240-247. https://pubmed.ncbi.nlm.nih.gov/35895965/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Dason ES, Maxim M, Sanders A, Papillon-Smith J, Ng D, Chan C, Sobel M. Guideline No. 437: Diagnosis and Management of Adenomyosis. Journal of Obstetrics and Gynaecology Canada. 2023;45(6):101344. https://pubmed.ncbi.nlm.nih.gov/37244746/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Pereira M, Kumari S, Di Francesco L. Preoperative Diagnosis of Symptomatic Adenomyosis: Limitations and Clinical Insights. Cureus. 2025;17. https://pubmed.ncbi.nlm.nih.gov/41607951/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Osada H. Uterine adenomyosis and adenomyoma: the surgical approach. Fertility and Sterility. 2018;109(3):406-417. https://pubmed.ncbi.nlm.nih.gov/29566853/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
McCausland V, McCausland A. The response of adenomyosis to endometrial ablation/resection. Human Reproduction Update. 1998;4(4):354-359. https://pubmed.ncbi.nlm.nih.gov/9825850/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Mengerink BB, van der Wurff AA, ter Haar JF, van der Steeg JW, Weyers S. Effect of undiagnosed deep adenomyosis after failed NovaSure endometrial ablation. Journal of Minimally Invasive Gynecology. 2015;22(2):239-244. https://pubmed.ncbi.nlm.nih.gov/25460320/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Debski R, Kotarski J, Paszkowski T. The statement of Polish Gynecological Society experts on oral use of contraceptive 75 microg desogestrel minipill in different clinical cases--state of art in 2008. Ginekologia Polska. 2009;80(1):62-67. https://pubmed.ncbi.nlm.nih.gov/19323063/ ↩︎ ↩︎ ↩︎
Vannuccini S, La Torre F, Toscano F. Medical treatment for adenomyosis: long term use of progestins. Gynecological Endocrinology. 2025;41(1):2443015. https://pubmed.ncbi.nlm.nih.gov/40424290/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Moïse A, Dzeitova M, de Landsheere L, et al. Endometriosis and Infertility: Gynecological Examination Practical Guide. Journal of Clinical Medicine. 2025;14(6):1234. https://pubmed.ncbi.nlm.nih.gov/40142712/ ↩︎ ↩︎ ↩︎
Tellum T, Nygaard S, Lieng M. Noninvasive Diagnosis of Adenomyosis: A Structured Review and Meta-analysis of Diagnostic Accuracy in Imaging. Journal of Minimally Invasive Gynecology. 2020;27(2):295-305. https://pubmed.ncbi.nlm.nih.gov/31712162/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
O'Shea A, Figueiredo G, Lee SI. Imaging Diagnosis of Adenomyosis. Seminars in Reproductive Medicine. 2020;38(2-03):111-120. https://pubmed.ncbi.nlm.nih.gov/33197946/ ↩︎ ↩︎
Song SY, Lee SY, Kim HY, Park SY, Lee JH. Long-term efficacy and feasibility of levonorgestrel-releasing intrauterine device use in patients with adenomyosis. Medicine. 2020;99(22):e20439. https://pubmed.ncbi.nlm.nih.gov/32481439/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Cho S, Nam A, Kim H, Kim JY, Park JY, Shin JE, Lee HY. Clinical effects of the levonorgestrel-releasing intrauterine device in patients with adenomyosis. American Journal of Obstetrics and Gynecology. 2008;198(4):373.e1-373.e7. https://pubmed.ncbi.nlm.nih.gov/18177833/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Ferrero S, Gazzo I, Perrone U, Barra F. GnRH antagonists for the treatment of fibroids and adenomyosis, current evidence and future perspectives. Expert Opinion on Pharmacotherapy. 2026;27(10):2483109. https://pubmed.ncbi.nlm.nih.gov/42360331/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Barretta M, Vignali M, La Marca A. The oral GnRH antagonists, a new class of drugs in gynecology: from pharmacokinetics to possible clinical applications. Expert Opinion on Drug Metabolism & Toxicology. 2024;20(12):1125-1136. https://pubmed.ncbi.nlm.nih.gov/39666595/ ↩︎ ↩︎ ↩︎
Chandra S, Tjahyadi D, Rachmawati A. Fertility in adenomyosis: surgery or IVF? Minerva Obstetrics and Gynecology. 2026. https://pubmed.ncbi.nlm.nih.gov/42317179/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Yamanaka K, Washio K, Uchida A, et al. Rapid reduction of adenomyosis coexisting with leiomyoma volume during treatment with Relugolix. Gynecological Endocrinology. 2023;39(1):2238407. https://pubmed.ncbi.nlm.nih.gov/37537884/ ↩︎ ↩︎ ↩︎
Catherino WH, Al-Hendy A, Zaim S, et al. Efficacy and safety of relugolix combination therapy in women with uterine fibroids and adenomyosis: subgroup analysis of LIBERTY 1 and LIBERTY 2. Fertility and Sterility. 2025;124(3):415-424. https://pubmed.ncbi.nlm.nih.gov/40320117/ ↩︎ ↩︎ ↩︎ ↩︎
Chen J, Porter AE, Kho KA. Current and Future Surgical and Interventional Management Options for Adenomyosis. Seminars in Reproductive Medicine. 2020;38(2-03):111-120. https://pubmed.ncbi.nlm.nih.gov/33152768/ ↩︎ ↩︎ ↩︎
Tsui KH, Lee WL, Chen CY, et al. Medical treatment for adenomyosis and/or adenomyoma. Taiwanese Journal of Obstetrics & Gynecology. 2014;53(4):459-465. https://pubmed.ncbi.nlm.nih.gov/25510683/ ↩︎
Chapron C, Vannuccini S, Santulli P. Diagnosing adenomyosis: an integrated clinical and imaging approach. Human Reproduction Update. 2020;26(3):285-311. https://pubmed.ncbi.nlm.nih.gov/32097456/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Takeuchi M, Matsuzaki K. Adenomyosis: usual and unusual imaging manifestations, pitfalls, and problem-solving MR imaging techniques. Radiographics. 2011;31(1):99-115. https://pubmed.ncbi.nlm.nih.gov/21257936/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Selntigia A, Molinaro P, Tartaglia S. Adenomyosis: An Update Concerning Diagnosis, Treatment, and Fertility. Journal of Clinical Medicine. 2024;13(17):5102. https://pubmed.ncbi.nlm.nih.gov/39274438/ ↩︎
Donnez J, Van Langendonckt A, Casanas-Roux F, et al. Current thinking on the pathogenesis of endometriosis. Gynecologic and Obstetric Investigation. 2002;54(3):163-174. https://pubmed.ncbi.nlm.nih.gov/12441661/ ↩︎
Leal CRV, Vannuccini S, Jain V. Abnormal uterine bleeding: The well-known and the hidden face. Journal of Endometriosis and Uterine Disorders. 2024;4:100065. https://pubmed.ncbi.nlm.nih.gov/38764520/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zhang H, Li C, Li W. Research Advances in Adenomyosis-Related Signaling Pathways and Promising Targets. Biomolecules. 2024;14(11):1405. https://pubmed.ncbi.nlm.nih.gov/39595579/ ↩︎
Wang MH, Chen JH, Qi XY, et al. Global prevalence of adenomyosis and endometriosis: a systematic review and meta-analysis. Reproductive Biology and Endocrinology. 2025;23(1):104. https://pubmed.ncbi.nlm.nih.gov/41257733/ ↩︎ ↩︎ ↩︎ ↩︎
Bazot M, Cortez A, Darai E. Ultrasonography compared with magnetic resonance imaging for the diagnosis of adenomyosis: correlation with histopathology. Human Reproduction. 2001;16(11):2427-2433. https://pubmed.ncbi.nlm.nih.gov/11679533/ ↩︎
Abbott JA. Adenomyosis and Abnormal Uterine Bleeding (AUB-A)-Pathogenesis, diagnosis, and management. Best Practice & Research Clinical Obstetrics & Gynaecology. 2017;40:68-81. https://pubmed.ncbi.nlm.nih.gov/27810281/ ↩︎
Cheong Y, Cameron IT, Critchley HOD. Abnormal uterine bleeding. British Medical Bulletin. 2017;123(1):103-113. https://pubmed.ncbi.nlm.nih.gov/28910998/ ↩︎
Harmsen MJ, Trommelen LM, de Leeuw RA, et al. Uterine junctional zone and adenomyosis: comparison of MRI, transvaginal ultrasound and histology. Ultrasound in Obstetrics & Gynecology. 2023;62(1):37-46. https://pubmed.ncbi.nlm.nih.gov/36370446/ ↩︎ ↩︎
Vannuccini S, Petraglia F, Carmona F. The modern management of uterine fibroids-related abnormal uterine bleeding. Fertility and Sterility. 2024;122(1):31-41. https://pubmed.ncbi.nlm.nih.gov/38723935/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Hall EM, Ravelo AE, Aronoff SC. Systematic review and meta-analysis of the etiology of heavy menstrual bleeding in 2,770 adolescent females. BMC Women's Health. 2024;24(1):123. https://pubmed.ncbi.nlm.nih.gov/38378571/ ↩︎
Biasioli A, Degano M, Restaino S, et al. Innovative Ultrasound Criteria for the Diagnosis of Adenomyosis and Correlation with Symptoms: A Retrospective Re-Evaluation. Biomedicines. 2024;12(2):459. https://pubmed.ncbi.nlm.nih.gov/38398065/ ↩︎ ↩︎
Brunelli AC, Brito LGO, Moro FAS. Ultrasound Elastography for the Diagnosis of Endometriosis and Adenomyosis: A Systematic Review with Meta-analysis. Ultrasound in Medicine & Biology. 2023;49(3):712-724. https://pubmed.ncbi.nlm.nih.gov/36528440/ ↩︎
Agostinho L, Cruz R, Osório F, Alves J, Setúbal A, Guerra A. MRI for adenomyosis: a pictorial review. Insights into Imaging. 2017;8(6):549-556. https://pubmed.ncbi.nlm.nih.gov/28980163/ ↩︎ ↩︎
Bourdon M, Santulli P, Marcellin L. Adenomyosis: An update regarding its diagnosis and clinical features. Journal of Gynecology Obstetrics and Human Reproduction. 2021;50(10):102228. https://pubmed.ncbi.nlm.nih.gov/34520877/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
McCaughey T, Newman M, Constable L. Standardizing the histopathological diagnosis of adenomyosis: an international Delphi consensus. Histopathology. 2025;87(3):412-425. https://pubmed.ncbi.nlm.nih.gov/40539549/ ↩︎ ↩︎
Laban M, Hassanin AS, Hussain SH. Accuracy of endomyometrial biopsy in diagnosis of adenomyosis: A prospective study. International Journal of Gynaecology and Obstetrics. 2025;168(1):45-52. https://pubmed.ncbi.nlm.nih.gov/40421701/ ↩︎
Munro MG, Critchley HO, Fraser IS. The FIGO classification of causes of abnormal uterine bleeding in the reproductive years. Fertility and Sterility. 2011;95(7):2204-2208. https://pubmed.ncbi.nlm.nih.gov/21496802/ ↩︎
Park DS, Kim ML, Song T, et al. Clinical experiences of the levonorgestrel-releasing intrauterine system in patients with large symptomatic adenomyosis. Taiwanese Journal of Obstetrics & Gynecology. 2015;54(4):415-420. https://pubmed.ncbi.nlm.nih.gov/26384061/ ↩︎ ↩︎
Refaat R, Ammar EAM, Basha MAA. Uterine artery embolization versus dienogest for symptomatic adenomyosis: A randomized controlled trial of short-term efficacy. European Journal of Radiology. 2026;194:112248. https://pubmed.ncbi.nlm.nih.gov/41628502/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Che X, Wang J, Sun W, et al. Effect of Mifepristone vs Placebo for Treatment of Adenomyosis With Pain Symptoms: A Randomized Clinical Trial. JAMA Network Open. 2023;6(6):e2317861. https://pubmed.ncbi.nlm.nih.gov/37307001/ ↩︎ ↩︎ ↩︎
Sharma S, RoyChoudhury S, Chakraborty P. Comparative analysis of low-dose letrozole versus GnRH agonist on implantation markers and IVF outcomes in symptomatic adenomyosis: a randomized trial. Scientific Reports. 2025;15(1):2418. https://pubmed.ncbi.nlm.nih.gov/41476263/ ↩︎ ↩︎
Chen Y, Lin S, Xie X. Systematic review and meta-analysis of reproductive outcomes after high-intensity focused ultrasound (HIFU) treatment of adenomyosis. Best Practice & Research. Clinical Obstetrics & Gynaecology. 2024;92:102431. https://pubmed.ncbi.nlm.nih.gov/38065008/ ↩︎ ↩︎
Song Y, Wang L. Combining Medication With High-Intensity-Focused Ultrasound for Adenomyosis: A Network Meta-Analysis of Randomized Controlled Trials. Journal of Ultrasound in Medicine. 2025;44(3):485-498. https://pubmed.ncbi.nlm.nih.gov/39648811/ ↩︎
Moawad G, Youssef Y, Fruscalzo A. The Impact of Conservative Surgical Treatment of Adenomyosis on Fertility and Perinatal Outcomes. Journal of Clinical Medicine. 2024;13(9):2536. https://pubmed.ncbi.nlm.nih.gov/38731060/ ↩︎ ↩︎
Han Y, Liu C, Liu D. Pregnancy outcomes in freeze-all versus fresh embryo transfer cycles of women with adenomyosis and endometriosis: a systemic review and meta-analysis. Frontiers in Endocrinology. 2025;16:142318. https://pubmed.ncbi.nlm.nih.gov/40438397/ ↩︎
Busnelli A, Di Simone N, Somigliana E. Untangling the independent effect of endometriosis, adenomyosis, and ART-related factors on maternal, placental, fetal, and neonatal adverse outcomes: results from a systematic review and meta-analysis. Human Reproduction Update. 2024;31(1):123-145. https://pubmed.ncbi.nlm.nih.gov/39049473/ ↩︎ ↩︎
Xia Y, Yu H. Systematic review and meta-analysis of adverse pregnancy outcomes with different types of adenomyosis. International Journal of Gynaecology and Obstetrics. 2025;168(2):212-220. https://pubmed.ncbi.nlm.nih.gov/40459223/ ↩︎ ↩︎ ↩︎
Razavi M, Maleki-Hajiagha A, Sepidarkish M. Systematic review and meta-analysis of adverse pregnancy outcomes after uterine adenomyosis. International Journal of Gynaecology and Obstetrics. 2019;145(2):142-149. https://pubmed.ncbi.nlm.nih.gov/30828808/ ↩︎ ↩︎
Bender Atik R, Christiansen OB, ESHRE Guideline Group on RPL. ESHRE guideline: recurrent pregnancy loss: an update in 2022. Human Reproduction Open. 2023;2023(1):hoad002. https://pubmed.ncbi.nlm.nih.gov/36873081/ ↩︎
Wang W, Ma X, Zhang W. Relapse after conservative surgery combined with triptorelin acetate versus conservative surgery only in women with focal adenomyosis: study protocol for a multicenter, prospective, randomized controlled trial. Trials. 2020;21(1):368. https://pubmed.ncbi.nlm.nih.gov/32345377/ ↩︎
Jiang J, Pan Y, Yu J, et al. Laparoscopic adenomyomectomy combined with levonorgestrel-releasing intrauterine system is effective for long-term management of adenomyosis. BMC Women's Health. 2024;24(1):28. https://pubmed.ncbi.nlm.nih.gov/38191409/ ↩︎