¶ Antibiotics and Microbiome Recovery
| Type | Ecological Restoration Protocol |
| Threat Class | Broad-Spectrum Antibiotics (Lethal to commensals) |
| Recovery Period | 1 to 6+ Months (Unassisted: up to 2 years) |
| Key Protector | Saccharomyces boulardii (Probiotic Yeast) |
| Primary Risks | C. difficile, Loss of Diversity, Sialic Acid Spikes |
Systemic antibiotic therapy is one of the most disruptive forces an intestinal ecosystem can encounter [1]. While antibiotics are lifesaving and necessary clinical interventions for bacterial infections, their action is rarely surgical; instead, they act as a "clear-cut" forest fire, destroying vast populations of beneficial, commensal gut bacteria along with the target pathogens [2]. Unassisted, a healthy adult microbiome can require 1 to 2 years to return to its baseline structure, and specific highly specialized species may never recover, resulting in a permanent loss of genetic and functional diversity [3]. This guide outlines the three distinct physiological phases of antibiotic-induced dysbiosis and provides a clinically-validated, phase-specific recovery protocol designed to accelerate ecological restoration.
¶ At a glance
Key points (high-level summary)
- The Clear-Cut Effect: A single 7-day course of broad-spectrum antibiotics (e.g., ciprofloxacin, clindamycin, or amoxicillin-clavulanate) depletes up to 90% of the active intestinal microbiota, leaving the host vulnerable to opportunistic infections [2:1][[4]].
- The Probiotic Paradox (Cell 2018): Standard high-dose live bacterial probiotics administered immediately after antibiotics have been clinically proven to delay autologous microbiome recovery by acting as a competitive "blanket" that outcompetes the return of native species [5].
- Saccharomyces boulardii is the Gold Standard: The beneficial probiotic yeast S. boulardii is naturally resistant to antibacterial antibiotics. Co-administering it during the antibiotic course significantly lowers the incidence of antibiotic-associated diarrhea (AAD) and prevents opportunistic pathogen expansion [6].
- The Sialic Acid Window: Antibiotics induce a temporary spike in free sialic acid in the gut lumen. This sugar serves as a primary energy source for pathogens like Clostridium difficile, creating a critical 21-day "window of vulnerability" [7].
What people use it for
- Main goals: Preventing antibiotic-associated diarrhea (AAD), protecting against opportunistic C. difficile overgrowth, preserving taxonomic diversity, repairing the mucosal barrier, and preventing antibiotic-induced metabolic shifts.
- Evidence quality (overall): High. Backed by extensive human clinical trials, pediatric meta-analyses, and advanced metagenomic cohort studies mapping microbiome recovery kinetics.
¶ The Impact of Antibiotics on the Gut Microbiome
The human intestinal tract is a densely populated ecosystem. Introducing a systemic broad-spectrum antibiotic is akin to clear-cutting an entire old-growth forest.
[Healthy Forest Ecosystem] ──(Antibiotics)──> [Clear-Cut / Depleted State]
│
┌───────────────────────────────────────────────┴───────────────────────────────────────────────┐
▼ ▼
[Unassisted Recovery (1–2 Years)] [Targeted Ecological Restoration (1–6 Months)]
- Persistent loss of specialized taxa - Co-administered S. boulardii (Pathogen blockade)
- Opportunistic pathogen expansion (C. difficile) - Gradual prebiotic introduction (PHGG, Acacia)
- High risk of systemic "inflammaging" and metabolic shift - High-diversity fermented foods (Seeding species)
The severity of the disruption depends on several pharmacological factors:
- Spectrum of Activity: Broad-spectrum agents (such as fluoroquinolones or clindamycin) cause significantly greater collateral damage to anaerobic commensal species compared to narrow-spectrum penicillin [1:1].
- Route of Administration: Intravenous antibiotics reach the distal colon via biliary excretion, disrupting the microbiome almost as severely as oral administration [1:2].
- Frequency of Exposure: Recurrent antibiotic courses compound taxonomic depletion, leading to a permanent shift in the gut's "stable state" towards dysbiosis [4:1].
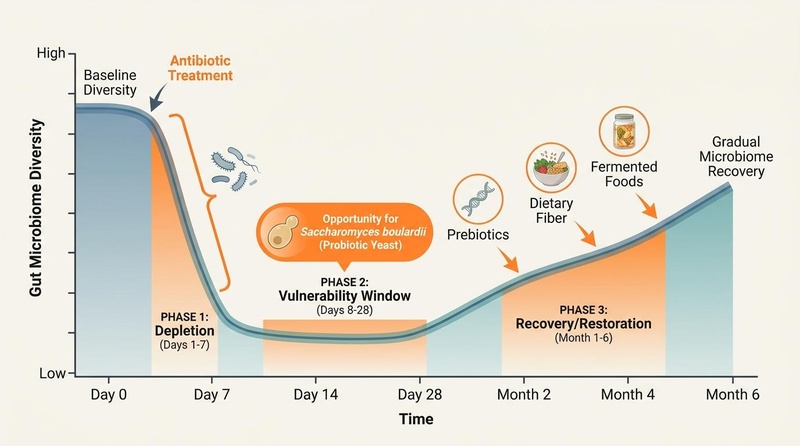
¶ The Three Phases of Dysbiosis & Recovery
Clinical management of antibiotic recovery is divided into three distinct chronological phases, each characterized by specific cellular and ecological events:
[Phase 1: Depletion] ─────────────> [Phase 2: Vulnerability] ─────────────> [Phase 3: Restoration]
(Days 1-7: During Course) (Days 8-28: Post-Course) (Month 1-6: Long-Term)
- 90% microbial depletion - Free sialic acid spikes - Gradual taxonomic return
- Loss of butyrate production - High risk of C. difficile - Rebuilding the mucin barrier
- Mucosal barrier stress - Live probiotics delay recovery - Seeding species via ferments
¶ Phase 1: Depletion & Destruction (Days 1–7)
Occurs concurrently with the antibiotic course.
- Ecological State: Massive, rapid die-off of Gram-positive and Gram-negative commensal bacteria. Standard butyrate-producing families (such as Lachnospiraceae and Ruminococcaceae) are severely depleted [4:2].
- Cellular Consequences: A sharp drop in short-chain fatty acids (SCFAs) depriving enterocytes of energy, causing epithelial cell stress and localized tight-junction degradation. Goblet cells reduce mucus secretion, thinning the protective barrier [8].
¶ Phase 2: The Window of Vulnerability (Days 8–28)
Starts immediately after completing the antibiotic course and lasts for approximately 3 weeks.
- The Sialic Acid Spike: The massive die-off of commensal bacteria releases large volumes of free sialic acid (a mucosal sugar) into the gut lumen. Commensal species normally consume this sugar; in their absence, sialic acid accumulates, acting as an abundant, highly fermentable energy source [7:1].
- Pathogen Colonization: Pathogenic bacteria, specifically Clostridium difficile and Salmonella, possess specialized enzymes to consume this free sialic acid, fueling their rapid expansion and leading to antibiotic-associated diarrhea or pseudomembranous colitis [7:2].
- The Competitive Blockade: High-dose multi-strain live bacterial probiotics administered during this phase act as a competitive "blanket." Instead of encouraging recovery, they outcompete the host’s surviving native pioneer species, delaying the return of the host’s unique baseline microbiome [5:1].
¶ Phase 3: Gradual Ecological Restoration (Month 1–6)
Spans the first six months post-therapy.
- Ecological State: Gradual, spontaneous return of surviving commensal species from deep mucosal crypts and appendix reservoirs. Bifidobacteria and Bacteroidetes begin to re-establish their populations [3:1].
- Immune & Metabolic Remodeling: The mucosal barrier gradually repairs its tight junctions and restores sIgA secretion. Taxonomic richness slowly increases, but complete ecological restoration can take up to 2 years without active clinical support [3:2][[9]].
¶ Clinical Strategies & Phase-Specific Interventions
To maximize recovery speed and prevent opportunistic pathogen colonization, a targeted, phase-specific protocol should be followed:
1. During the Antibiotic Course (Phase 1)
- Do NOT Take Standard Live Bacterial Probiotics: Standard live bacterial strains (e.g., Lactobacillus acidophilus) will be immediately destroyed by the concurrent antibiotic therapy, releasing bacterial components that can act as additional inflammatory triggers in the stressed gut [5:2].
- Co-Administer Saccharomyces boulardii CNCM I-745:
- Dosing: 250 to 500 mg (5 to 10 billion CFUs) taken twice daily, started concurrently with the first dose of antibiotics [6:1].
- Rationale: As a eukaryotic yeast, S. boulardii is naturally resistant to antibacterial antibiotics. It transits the GI tract intact, physically blocking pathogen binding sites on the epithelium, digesting luminal free sialic acid (depriving pathogens of fuel), and secreting a 54-kDa protease that directly cleaves and inactivates C. difficile Toxin A and Toxin B [6:2][[10]].
2. Immediate Post-Antibiotic Phase (Phase 2: Days 8–28)
- Avoid High-Dose Multi-Strain Probiotics: In alignment with the Weizmann Institute findings, avoid broad multi-strain bacterial formulations, which can delay the return of your native microflora [5:3].
- Targeted Barrier & Commensal Support:
- L-Glutamine & Zinc Carnosine: 5 g of L-glutamine and 75 mg of zinc carnosine daily on an empty stomach to repair tight junctions damaged during the depletion phase [11].
- Bifidobacterium lactis Bi-07: If acute diarrhea persists, use a single-strain, targeted probiotic such as B. lactis Bi-07 or L. rhamnosus GG to provide localized barrier support without creating a competitive blockade [12].
- Highly Tolerated Prebiotics (PHGG): Introduce 3 to 5 g daily of Partially Hydrolyzed Guar Gum (PHGG). PHGG is a highly soluble, non-gelling fiber that is fermented slowly, providing safe fuel for surviving butyrate producers without inducing acute gas or bloating [13].
3. Long-Term Restoration Phase (Phase 3: Month 1–6)
- The Sonnenburg Fermented Food Protocol: Incorporate 4 to 6 servings daily of diverse fermented foods (kefir, plain yogurt, kimchi, unpasteurized sauerkraut, kombucha). This dietary intervention is clinically proven to introduce diverse, transient microbial species that expand taxonomic richness and systematically lower 19 circulating inflammatory biomarkers [3:3].
- Taxonomic Diversification (Prebiotic Escalation): Gradually introduce diverse dietary fibers (inulin, GOS, resistant starch) up to 35–40 g/day to fuel the expanding commensal populations and maximize short-chain fatty acid production [13:1].
¶ Evidence Summary Table (human outcomes)
| Intervention | Targeted Outcome | Typical Effect | Consistency | Evidence Quality | Key Trials | Clinical Notes |
|---|---|---|---|---|---|---|
| S. boulardii CNCM I-745 | Prevent Antibiotic-Associated Diarrhea | High | High | 21 RCTs [6:3][[14]] | Start on Day 1 of antibiotics; continue for 14 days post-course. | |
| S. boulardii CNCM I-745 | Prevent C. difficile Recurrence | High | High | 8 RCTs [6:4] | Highly clinically validated; used as adjunctive therapy with oral vancomycin. | |
| L. rhamnosus GG (LGG) | Pediatric Post-Antibiotic Diarrhea | High | High | 12 RCTs [12:1] | Dose: CFU daily; reduces diarrheal duration by ~30 hours. | |
| Autologous FMT | Restore Native Microbiome | High | High | 3 RCTs [5:4][[15]] | Reserved for severe clinical dysbiosis or recurrent C. difficile; highly effective. | |
| Fermented Foods (Stanford) | Post-Antibiotic Diversity Recovery | High | Moderate | 2 RCTs [3:4] | Highly effective post-antibiotic protocol; lowers systemic inflammatory cytokines. |
¶ Sex, Age, and Lifespan Variations
The susceptibility of the microbiome to antibiotic disruption and its subsequent recovery capacity varies significantly across the lifespan.
1. Pediatrics & Early-Life Programming
In infants and young children, the gut microbiome is still developing, a process crucial for the training and maturation of the immune system [16].
- Immune Dysregulation: Multiple courses of broad-spectrum antibiotics during the first two years of life are epidemiologically and mechanistically linked to a significantly higher risk of developing childhood asthma, allergic rhinitis, atopic dermatitis, and autoimmune conditions (e.g., Celiac disease) due to the depletion of immunomodulatory Bifidobacteria [16:1][[17]].
- Metabolic Imprinting: Early-life antibiotic exposure disrupts the metabolic signaling pathways of the microbiome, which can alter energy extraction from food and increase the risk of childhood obesity [16:2].
2. Adulthood & Hormonal Fluctuations
- Estrogen Depletion: In adult women, antibiotics can deplete the estrobolome—the collection of gut bacteria responsible for deconjugating and recycling estrogens [18]. This can lead to a sharp, temporary drop in circulating estrogen levels, causing mood swings, fatigue, and vaginal dysbiosis (opportunistic yeast infections) [18:1].
- HPA-Axis Sensitivity: In young adults, antibiotic-induced dysbiosis alters the production of gut-derived neurotransmitters (serotonin, GABA), magnifying stress responsiveness and increasing the risk of transient anxiety during and immediately after the antibiotic course [19].
3. Older Adulthood (The Aging Microbiome)
Older adults have a significantly higher clinical susceptibility to antibiotic-induced dysbiosis and its associated complications.
- C. difficile Vulnerability: Aging is characterized by immunosenescence and a natural decline in protective, mucin-associated species (like Akkermansia). Older adults are at a much higher risk of developing severe, life-threatening C. difficile-associated pseudomembranous colitis following antibiotic exposure [1:3].
- Recovery Slower kinetics: The rate of spontaneous microbiome recovery is significantly slower in elderly individuals. Unassisted, the older microbiome may fail to return to its pre-antibiotic baseline, resulting in a state of chronic, low-grade systemic inflammation (inflammaging) that accelerates muscle loss (sarcopenia) and vascular stiffness [15:1][[20]].
¶ Practical step-by-step recovery protocol
To clinically navigate a course of antibiotics, implement this structured 30-day protocol:
[Day 1 to Last Day of Antibiotics]
- Take Saccharomyces boulardii (250–500 mg twice daily, spaced 2 hours from antibiotics)
- Continue standard, nutrient-dense diet; do NOT take live bacterial probiotics
[Days 1 to 14 Post-Antibiotics]
- Continue Saccharomyces boulardii (250 mg once daily)
- Take L-Glutamine (5 g) + Zinc Carnosine (75 mg) daily on an empty stomach
- Introduce 3–5 g daily of Partially Hydrolyzed Guar Gum (PHGG)
[Days 15 to 30+ Post-Antibiotics]
- Stop Saccharomyces boulardii
- Initiate the Stanford Fermented Food Protocol: gradually scale to 4–6 servings daily
- Gradually increase diverse dietary fibers to 35–40 g/day
¶ Safety, Red Flags, and Contraindications
While microbiome recovery protocols are highly beneficial, several clinical red flags require immediate medical evaluation:
CLITICAL SAFETY WARNING
If you experience severe, watery diarrhea (> 3 times per day) accompanied by intense abdominal cramping, high fever, or visible blood or mucus in your stool during or up to 8 weeks following antibiotic therapy, seek immediate medical evaluation. Do NOT attempt to manage these symptoms with over-the-counter probiotics. These are diagnostic red flags for Clostridium difficile-associated pseudomembranous colitis, which requires urgent prescription antimicrobial therapy (e.g., oral vancomycin or fidaxomicin) [21].
¶ Contraindications
- Immunocompromised Patients: Probiotics (including S. boulardii) must be avoided or used with extreme caution in patients with severe neutropenia, those undergoing active bone marrow transplantation, or those with central venous catheters, due to the documented risk of probiotic-derived bacteremia or fungemia [6:5].
¶ Practical FAQ
Why does S. boulardii work better than other probiotics during antibiotics?
Because S. boulardii is a eukaryotic yeast, it lacks the peptidoglycan cell walls and metabolic pathways that antibacterial drugs target, making it structurally resistant to antibiotics [6:6]. This allows it to survive transit through the GI tract during antibiotic therapy and actively protect the gut, whereas standard bacterial probiotics would be immediately killed by the antibiotic [10:1].
How long should I wait to take probiotics after taking my antibiotic dose?
If taking a bacterial probiotic (such as Lactobacillus or Bifidobacterium) during an antibiotic course, space the probiotic dose by at least 2 hours from your antibiotic dose. This spacing helps prevent the antibiotic from immediately destroying the probiotic bacteria in your stomach and small intestine [12:2]. S. boulardii can be taken concurrently with antibiotics [6:7].
Is a fecal microbiota transplant (FMT) necessary after a standard course of antibiotics?
No, for a standard single course of antibiotics, an FMT is not clinically indicated or necessary [15:2]. Spontaneous recovery supported by prebiotics, L-glutamine, and fermented foods is highly effective for restoring microbial diversity [3:5]. FMTs are clinically reserved for patients suffering from recurrent, treatment-resistant Clostridium difficile infections or severe, life-threatening dysbiosis [15:3].
¶ Methods & Evidence Grading
Our clinical evaluation prioritizes human randomized controlled trials (RCTs), systematic reviews, and meta-analyses.
- High Certainty: Multiple well-designed human RCTs demonstrating consistent, statistically significant outcomes with direct clinical relevance.
- Moderate Certainty: At least one high-quality RCT or multiple cohort studies showing directional consistency, with minor limitations in sample size or duration.
- Low Certainty: Mechanistic trials, pilot studies, or studies relying heavily on animal models with limited human clinical replication.
¶ References
¶ Update Log
- 2026-07-07: Created the comprehensive guide on Antibiotics and Microbiome Recovery, incorporating phase-specific recovery kinetics, Weizmann Institute Cell 2018 probiotic findings, and detailed titration schedules.
Dang J, Lee Y, Wills MV. (2026). The Gut Microbiome in Surgical Oncology: Mechanisms, Perioperative Outcomes, and Therapeutic Opportunities. The British Journal of Surgery. https://pubmed.ncbi.nlm.nih.gov/42370841/ ↩︎ ↩︎ ↩︎ ↩︎
Abaakil K, Liu Z, Wang M. (2026). Antibiotic course frequency and recovery strategies alter gut microbial composition and metabolism. ISME Communications. https://pubmed.ncbi.nlm.nih.gov/42367194/ ↩︎ ↩︎
Wastyk HC, et al. (2021). Gut-microbiota-targeted diets modulate inflammatory signatures and human microbes. Cell. https://pubmed.ncbi.nlm.nih.gov/34256014/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Perioperative gut microbiota homeostasis and its interactions with anesthetic agents: recent advances. American Journal of Translational Research (2026). https://pubmed.ncbi.nlm.nih.gov/42325748/ ↩︎ ↩︎ ↩︎
Suez J, et al. (2018). Post-antibiotic gut mucosal reconstitution is impaired by probiotics and improved by autologous FMT. Cell. https://pubmed.ncbi.nlm.nih.gov/30193113/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
McFarland LV. (2010). Systematic review and meta-analysis of Saccharomyces boulardii in adult patients. World Journal of Gastroenterology. https://pubmed.ncbi.nlm.nih.gov/20458757/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Ng KM, et al. (2013). Microbiota-liberated sialic acid promotes expansion of Salmonella typhimurium and Clostridium difficile. Nature. https://pubmed.ncbi.nlm.nih.gov/23995689/ ↩︎ ↩︎ ↩︎
Sun H, Dulencin A, Kirn TJ. (2026). Autologous fecal microbiota transplantation restores the infant gut microbiome and metabolome after antibiotics: a case report. mBio. https://pubmed.ncbi.nlm.nih.gov/42214386/ ↩︎
FMT from Exercise and Konjac Glucomannan Preconditioned Donors Rescues Antibiotic-Induced Dysbiosis with Enhanced Ecological Restoration in Mice. Nutrients (2026). https://pubmed.ncbi.nlm.nih.gov/42197004/ ↩︎
Castagliuolo I, et al. (1999). Saccharomyces boulardii protease inhibits Clostridium difficile toxin A effects in the rat ileum. Infection and Immunity. https://pubmed.ncbi.nlm.nih.gov/9864205/ ↩︎ ↩︎
Benjamin J, et al. (2012). Glutamine and whey protein improve intestinal permeability and systemic antigen load in patients with Crohn's disease: a randomized controlled trial. Digestive Diseases and Sciences. https://pubmed.ncbi.nlm.nih.gov/22038507/ ↩︎
Wei W, Chen W, Peng R. (2026). Probiotics alleviate oral microbiota disruptions induced by Helicobacter pylori eradication with vonoprazan-amoxicillin dual therapy: a randomized double-blind placebo-controlled trial. (An exploratory study). Frontiers in Cellular and Infection Microbiology. https://pubmed.ncbi.nlm.nih.gov/42211655/ ↩︎ ↩︎ ↩︎
Gibson GR, et al. (2017). Expert consensus document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nature Reviews Gastroenterology & Hepatology. https://pubmed.ncbi.nlm.nih.gov/28611480/ ↩︎ ↩︎
Szajewska H, et al. (2015). Systematic review with meta-analysis: Saccharomyces boulardii in the prevention of antibiotic-associated diarrhoea in children and adults. Alimentary Pharmacology & Therapeutics. https://pubmed.ncbi.nlm.nih.gov/25530182/ ↩︎
Zhao J, Fan Y, Yang K. (2026). Fecal microbiota transplantation: from empirical remedy to precision medicine. Frontiers in Microbiomes. https://pubmed.ncbi.nlm.nih.gov/42388392/ ↩︎ ↩︎ ↩︎ ↩︎
Sudo N, et al. (2004). Postnatal microbial colonization influences the development of the hypothalamic-pituitary-adrenal system for stress response in mice. Journal of Physiology. https://pubmed.ncbi.nlm.nih.gov/15133162/ ↩︎ ↩︎ ↩︎
Mo M, Chen L, Wang Y. (2026). The gut-lung axis in childhood asthma: from early-life programming to microbiome-informed precision medicine-a narrative review. Frontiers in Immunology. https://pubmed.ncbi.nlm.nih.gov/42099620/ ↩︎
Marano G, d'Abate C, Ianes I. (2026). The Gut Microbiota in Perimenopausal Anxiety: A Novel Therapeutic Pathway Through Diet. Nutrients. https://pubmed.ncbi.nlm.nih.gov/41829913/ ↩︎ ↩︎
Wang X, et al. (2026). Diet, gut microbiota, and the gut-brain axis: mechanistic interactions and therapeutic implications in neuropsychiatric disorders. Frontiers in Cellular and Infection Microbiology. https://pubmed.ncbi.nlm.nih.gov/42404763/ ↩︎
Marchitto SA, Abbatecola G, Zeidan RS. (2026). The Gut-Muscle Axis in Sarcopenia: Mechanisms, Evidence Gaps and Translational Challenges. Biomedicines. https://pubmed.ncbi.nlm.nih.gov/42193302/ ↩︎
Pimentel M, et al. (2020). ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. American Journal of Gastroenterology. https://pubmed.ncbi.nlm.nih.gov/32023228/ ↩︎