¶ Arterial Stiffness and Pulse-Wave Velocity
| Mechanism | Pulse-wave velocity (cfPWV, baPWV) & wave reflection analysis (AIx) |
| Key Spec | Aortic transit time, path length distance, central pressure augmentation |
| Protocol | Standardized resting state, stimulant and heavy meal avoidance |
| Distance | cfPWV: 80% of direct carotid-femoral distance; baPWV: automated height-based estimation |
| FDA Class | Class II Diagnostic Device |
| Entry Cost | $1,500 – $15,000 (clinical-grade tonometry / cuff-oscillometry) |
Arterial stiffness, quantified primarily via pulse-wave velocity (PWV), is an independent and highly validated biomarker of vascular aging and cardiovascular risk [1][2]. By reflecting the structural and functional properties of the large elastic arteries, PWV measurements offer clinical and prognostic utility beyond traditional peripheral blood pressure monitoring [2:1][3].
¶ At a glance
Key points
- Does it work? Yes. Carotid-femoral pulse-wave velocity (cfPWV) is universally recognized as the clinical gold standard for non-invasively measuring central arterial stiffness and predicting future cardiovascular events and mortality [1:1][4].
- Who needs it? Primarily individuals with hypertension, prediabetes or diabetes mellitus, metabolic syndrome, and advanced age where precise cardiovascular risk stratification improves clinical management [5][6][7].
- Verdict: Highly valuable tool for clinical risk stratification. While clinical assessments should not be conceptually conflated with simpler consumer-grade tracking metrics, clinical interpretation must strictly account for the confounding effects of age and acute blood pressure changes [8][9].
What people use it for
- Vascular Aging Assessment: Assessing the progressive stiffening of central elastic arteries [3:1].
- Cardiovascular Risk Stratification: Improving the prediction of coronary events, stroke, and mortality, particularly in individuals with moderate blood pressure [5:1][4:1].
- Therapeutic Monitoring: Evaluating the long-term efficacy of antihypertensive, statin, or lifestyle interventions on central hemodynamics [9:1][10][11].
¶ Evidence summary table (human outcomes)
| Clinical Scenario / Outcome | Measured Parameter | Effect | Consistency | Evidence Quality | Trials | Notes (Population, Duration, Dosage) |
|---|---|---|---|---|---|---|
| Cardiovascular Event Risk | cfPWV | High | High | 19 Prospective Cohorts | 1 m/s increase in cfPWV is associated with a 12% increase in risk of total CV events (RR 1.12, 95% CI: 1.07-1.18) [4:2]. | |
| Cardiovascular Mortality | cfPWV | High | High | 19 Prospective Cohorts | 1 m/s increase in cfPWV is associated with a 9% increase in CV mortality (RR 1.09, 95% CI: 1.04-1.14) [4:3]. | |
| Moderate Blood Pressure Risk | cfPWV | High | High | 11 Cohorts (n=15,987) | 1-SD increase in log_e(cfPWV) is associated with a 1.21-fold increase in ASCVD risk among individuals with BP 120-159/80-99 mmHg [5:2]. | |
| Prediabetes & Diabetes Progression | cfPWV | High | High | 37 Clinical Studies | Diabetic and prediabetic populations exhibit significantly higher cfPWV values, showing that central arterial stiffening progresses during prediabetes [6:1]. | |
| Incident Hypertension Prediction | baPWV | High | High | Cohort Study (n=10,360) | Highest quartile of baPWV has hazard ratio of 1.64 in men and 12.36 in women for developing new hypertension over 2.17 years [12]. | |
| Statin Therapy on Wave Reflection | AIx | High | High | 18 RCTs | Statin therapy causes a significant reduction in aortic AIx (WMD: -2.40% overall; -5.04% for heart-rate adjusted AIx 75%) [10:1]. | |
| High-Purity EPA Supplementation | baPWV | Moderate | Moderate | Clinical Trial (n=21 subgroup of n=191) | Sequential administration of high-purity EPA (1,800 mg/day for 6 months) significantly reduced baPWV and increased the plasma EPA/AA ratio in a 21-patient subgroup of the larger n=191 cohort (who initially received a fish-based diet that showed no change in baPWV) [11:1]. | |
| Vegetarian Diet | cfPWV | Moderate | Moderate | Meta-analysis of 7 Studies | Vegetarian dietary patterns are associated with significantly lower cfPWV levels (MD: -0.43 m/s) compared to omnivorous diets [13]. | |
| Habitual Physical Activity | cfPWV | Moderate | Moderate | Meta-analysis of 18 Studies (n=15,573) | Weak but significant negative correlation between habitual physical activity and cfPWV (partial r = -0.08), supporting the vascular benefits of regular exercise [14]. | |
| Sedentary Behavior | cfPWV | Moderate | Moderate | Meta-analysis of 12 Studies | Time spent in sedentary behavior is positively correlated with higher cfPWV (r = 0.23, 95% CI: 0.12 to 0.35, p<0.01) [15]. | |
| Chronic Obstructive Pulmonary Disease | baPWV | High | Moderate | Cohort Study (n=134) | COPD patients exhibit significantly elevated baPWV (1933 vs 1515 cm/s). FEV1 is the strongest independent predictor of arterial stiffness in these patients [16]. | |
| Cognitive Impairment in Metabolic Syndrome | baPWV | Moderate | Moderate | Cross-sectional Study (n=92) | In patients with metabolic syndrome, higher baPWV is strongly associated with poorer working memory and executive function [17]. | |
| Chronic Venous Insufficiency | PWV / AIx | Moderate | Moderate | Case-Control Study (n=110) | PWV and AIx are significantly higher in chronic venous insufficiency patients compared to healthy controls (PWV: 8.92 vs. 8.03 m/s, p=0.001) [18]. |
¶ Mechanism
¶ Biophysics of Pulse-Wave Velocity
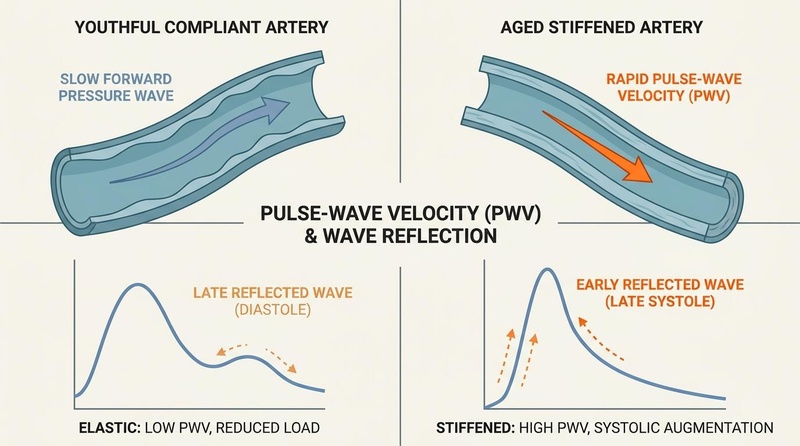
During cardiac systole, the left ventricle contracts and ejects a stroke volume of blood into the ascending aorta. This generates a forward-moving pressure wave that propagates along the arterial tree [3:2]. The speed at which this wave travels is defined as the Pulse-Wave Velocity (PWV) [8:1].
In a healthy, compliant vascular system, the central elastic arteries (such as the aorta) expand during systole to buffer the stroke volume and store potential energy, then recoil during diastole to maintain continuous peripheral tissue perfusion, helping keep central systolic and pulse pressures low [3:3].
With aging and chronic stressors like hypertension, central elastic arteries generally become stiffer and less compliant, accelerating pulse wave propagation as supported by Nichols (2005) [3:4] and Tomiyama (2004) [8:2].
According to the Moens-Korteweg equation, PWV is inversely proportional to the square root of arterial compliance:
Where:
- represents the Young's modulus of the arterial wall (reflecting its intrinsic stiffness).
- is the wall thickness.
- is the vessel radius.
- is the blood density.
Thus, as the vessel walls become stiffer and increases, the pulse wave propagates at a significantly accelerated velocity [3:5].
¶ Wave Reflection and Late Systolic Augmentation
The forward pressure wave generated by the heart eventually reaches points of structural discontinuity in the arterial tree, such as major arterial bifurcations and high-resistance terminal arterioles [3:6]. At these sites, a fraction of the wave is reflected and travels backward toward the central aorta [3:7][19].
Healthy, Elastic Artery:
Forward Wave [===========>]
Reflected Wave [<===========] (Returns late in DIASTOLE; boosts coronary flow)
Stiffened Artery (Vascular Aging):
Forward Wave [=======================>] (Accelerated PWV)
Reflected Wave [<=================] (Returns early in LATE SYSTOLE; increases cardiac load)
In a healthy vascular system characterized by low PWV, the reflected wave travels slowly and returns to the central aorta during diastole [3:8]. This late arrival is physiologically beneficial: it augments diastolic pressure in the ascending aorta, which directly enhances coronary artery perfusion, as the coronary arteries are primarily filled during diastole [3:9].
In contrast, when the central arteries are stiff and PWV is elevated, the forward wave travels rapidly, and the reflected wave returns prematurely to the central aorta during late systole [3:10]. This early wave reflection merges with the forward wave, resulting in systolic pressure augmentation [3:11][19:1]. This premature return has severe hemodynamic consequences [3:12]:
- Elevated Central Systolic & Pulse Pressure: The augmented pressure wave increases central systolic blood pressure [3:13][19:2].
- Increased Left Ventricular Afterload: The heart must pump against an amplified pressure peak, increasing myocardial oxygen demand and causing "wasted left ventricular energy" [3:14].
- Myocardial Mismatch & Hypertrophy: The persistent mechanical stress promotes pathological left ventricular hypertrophy (LVH) and increases susceptibility to heart failure [3:15][20].
- Elevated Circumferential Wall Stress: High systolic and pulse pressures resulting from advanced age or hypertension increase circumferential wall stress [3:16], and PWV correlates with markers reflecting the severity of atherosclerosis [8:3].
¶ The Augmentation Index (AIx) and Its Limitations
The Augmentation Index (AIx) is a widely used clinical measure of wave reflection and systemic arterial stiffness [19:3]. It is calculated as the ratio of Augmentation Pressure (, the difference between the second and first central systolic pressure peaks) to the total central Pulse Pressure () [19:4]:
Despite its widespread use in clinical research, AIx is subject to a profound mathematical and physiological flaw that limits its utility as a direct measure of arterial stiffness [19:5]:
- Ratio Confounding: Because both the numerator () and the denominator () are dynamic pressure variables that change under different cardiovascular states, a parallel increase in both can result in an unchanged or even decreased AIx, despite an actual increase in arterial stiffness [19:6].
- Heart Rate Dependency: AIx is highly dependent on heart rate, and clinicians commonly use heart-rate adjusted values standardized to 75 bpm (AIx@75) to account for this confounding factor [10:2].
- Confounding Covariates: AIx is highly dependent on non-vascular variables, such as peripheral blood pressures and cardiovascular dynamics, making it a complex composite measure rather than a pure reflection of wall structure [19:7].
Therefore, while AIx is useful for evaluating overall wave reflection dynamics and assessing the pressure-lowering effects of vasodilator drugs, it is a poor direct surrogate for the physical, structural properties of the central arterial wall compared to direct PWV measurements [19:8][3:17].
¶ Key Specs
Evaluating arterial stiffness in clinical practice and clinical trials relies on specific diagnostic modalities, each with distinct technological designs, measurement sites, and clinical parameters [21][22].
| Modality / Spec | Carotid-Femoral PWV (cfPWV) | Brachial-Ankle PWV (baPWV) | Augmentation Index (AIx) | Ambulatory Arterial Stiffness Index (AASI) |
|---|---|---|---|---|
| Vascular Segment Assessed | Central aorta (elastic) [1:2][21:1] | Central aorta + peripheral muscular arteries [8:4][21:2] | Systemic wave reflection sites [3:18][19:9] | Indirect estimate of systemic arterial tree [23][24] |
| Technological Method | Applanation tonometry or piezoelectric sensors [22:1] | Four-extremity blood pressure cuffs (oscillometric) [7:1][21:3] | Radial tonometry and generalized transfer function [3:19][22:2] | 24-hour ambulatory blood pressure monitoring (ABPM) [23:1][24:1] |
| Path Length / Distance | 80% of direct carotid-to-femoral distance [1:3][22:3] | Automated estimation [21:4] | Reconstructed central pressure waveform [3:20] | Not applicable (slope-derived) [23:2] |
| Primary Output Metric | Velocity in meters per second (m/s) [1:4] | Velocity in centimeters per second (cm/s) or m/s [16:1] | Percentage ratio of augmented pressure (%) [19:10] | Unitless index value (range: 0 to 1) [23:3][24:2] |
| Prognostic Value | Cardiovascular events, stroke, and mortality [4:4][5:3] | Incident hypertension, target organ damage, cognitive decline [12:1][25][17:1] | Vascular aging, left ventricular load, vasodilator efficacy [3:21][10:3] | Stroke and cardiovascular mortality prediction [23:4][24:3] |
| Ease of Clinical Use | Moderate (requires specialized operator training) [21:5] | High (fully automated, minimal operator bias) [21:6] | Moderate (requires stable waveforms) [22:4] | High (readily calculated from standard 24-hr ABPM) [23:5] |
¶ 1. Carotid-Femoral PWV (cfPWV)
Carotid-femoral PWV is the clinical reference standard ("gold standard") for central arterial stiffness assessment [1:5][21:7]. It utilizes applanation tonometry or transcutaneous transducers to record the pulse pressure waveform at the common carotid artery and the common femoral artery [1:6][22:5]. The transit time () of the pulse wave is calculated between these two sites (typically utilizing the intersecting tangent method to identify the waveform foot) [22:6].
The distance () between the recording sites must be measured precisely. The international consensus guidelines recommend using 80% of the direct straight-line distance between the carotid and femoral measurement sites as the most accurate estimate of true aortic path length to prevent systematic overestimation of velocity [1:7][22:7]:
Because it measures the central aortic pathway, cfPWV directly reflects central vascular aging and exhibits the strongest, most consistent predictive value for long-term clinical events [1:8][4:5].
¶ 2. Brachial-Ankle PWV (baPWV)
Brachial-ankle PWV is a simplified, highly reproducible automated alternative widely used in East Asian clinical and screening settings [21:8][26]. It utilizes four pneumatically inflated blood pressure cuffs wrapped around the bilateral upper arms (brachial artery) and ankles (posterior tibial and dorsalis pedis arteries) [7:2][21:9]. The system simultaneously monitors the volume pressure waveforms at all four extremities, calculating transit times automatically [7:3][21:10].
Unlike cfPWV, the baPWV pathway encompasses both central elastic segments (aorta) and peripheral muscular segments (upper arm and leg arteries) [8:5][21:11]. In terms of path length calculation, baPWV distance is automated [21:12]. This peripheral inclusion has distinct clinical implications [26:1]:
- Higher Absolute Values: Because muscular arteries are intrinsically stiffer than elastic central arteries, baPWV yields systematically higher absolute values than cfPWV, with a pooled mean difference of 5.03 m/s (95% CI: 4.34 to 5.72 m/s) [26:2].
- Strong Correlation: Despite measuring different segments, baPWV and cfPWV are strongly correlated (, 95% CI: 0.61 to 0.74) [26:3].
- Target Organ Damage Correlation: baPWV and cfPWV show similar, robust correlations with indices of subclinical Target Organ Damage (TOD), such as left ventricular mass index (LVMI), carotid intima-media thickness (cIMT), and urine albumin-to-creatinine ratio (UACR) [26:4].
¶ 3. Ambulatory Arterial Stiffness Index (AASI)
The Ambulatory Arterial Stiffness Index is a novel parameter calculated from 24-hour ambulatory blood pressure monitoring (ABPM) [23:6][24:4]. It is derived from the regression slope of diastolic blood pressure on systolic blood pressure over a 24-hour recording period [23:7]. The index is defined as:
As the arterial system becomes stiffer, the dynamic relationship between systolic and diastolic pressure changes, resulting in a flatter regression slope and a higher AASI (approaching 1.0) [23:8]. While AASI is a strong, independent predictor of fatal stroke and cardiovascular mortality, it is not interchangeable with cfPWV or AIx [23:9][24:5]. Clinical trials demonstrate that once age is adjusted for, the correlations between AASI, cfPWV, and AIx are entirely negated, demonstrating that they reflect different physiological properties of the arterial tree [24:6].
¶ Protocols
¶ Standardized Measurement Conditions
To ensure reproducible measurements and prevent transient hemodynamic fluctuations from confounding the clinical assessment, clinicians must strictly adhere to the following standardization protocols [1:9][2:2]:
- Resting State: The patient should remain in a quiet, resting state in a supine position prior to taking measurements to ensure standard hemodynamics [1:10][2:3].
- Stimulant and Food Avoidance: Patients should avoid vasoactive stimulants (such as caffeine or nicotine) and heavy meals before the procedure as recommended by standard protocols [2:4][9:2].
- Restrained Communication: Speaking or moving during the resting period and the measurement process is strictly prohibited to avoid sympathetic activation [1:11][2:5].
- Bladder Status: The patient should empty their bladder prior to the rest period, as a full bladder can elevate sympathetic tone and blood pressure.
- Therapeutic Record: All concurrent vasoactive or cardiovascular therapies (such as statins or vasodilators) should be documented, alongside the exact timing of their last dose, as they directly alter vascular tone and wave reflection dynamics [10:4][3:22][9:3].
¶ Blood Pressure Confounding and Calibration
Blood pressure is the most critical confounding variable in any arterial stiffness measurement [8:6][21:13]. Because arteries are viscoelastic tubes, an acute elevation in blood pressure stretches the elastic fibers in the arterial wall [3:23][9:4]. This passive distension transfers the mechanical stress of the pulse wave from highly compliant elastin fibers to extremely stiff collagen fibers [3:24][9:5].
As a direct physiological consequence, an acute increase in mean arterial pressure (MAP) will passively increase PWV, even in the complete absence of any structural changes in the vascular wall [8:7][21:14][9:6]. Therefore, clinicians must follow these calibration rules [1:12][2:6]:
- Same-Day Blood Pressure Recording: Peripheral blood pressure (systolic, diastolic, and calculated MAP) must be recorded on the same day as the PWV measurement using a validated, calibrated device [1:13][2:7].
- Hemodynamic Normalization: When evaluating longitudinal changes or comparing clinical cohorts, PWV values must be statistically adjusted for MAP to ensure that any observed changes reflect true vascular reverse-remodeling rather than a passive shift along the pressure-area curve [8:8][9:7].
¶ Algorithm and Device Discrepancies
Different commercial devices utilize varying hardware designs and transit-time detection algorithms, which can introduce systematic discrepancies in PWV calculations [22:8]:
- Tonometric vs. Oscillometric Devices: Applanation tonometry devices (e.g., SphygmoCor) require manual operator skill to capture high-quality pressure waveforms, introducing potential operator bias [22:9]. Oscillometric cuff-based devices (e.g., Vicorder, Mobil-O-Graph) are automated but rely on proprietary volume-displacement algorithms that can yield slightly different absolute transit times [22:10].
- Transit-Time Algorithms: Waveform foot detection algorithms differ. Most high-adherence validation devices utilize the intersecting tangent method (defining the foot of the wave by the intersection of a baseline tangent and a systolic upstroke tangent) [22:11]. These transit-time algorithms are not mathematically identical across all commercial systems, which can result in small, systematic differences in calculated transit times [22:12].
To maintain clinical validity, longitudinal monitoring of a single patient must be performed using the exact same device, operator technique, and transit-time algorithm [22:13][9:8].
¶ Evidence
¶ Confounding Effects of Age and Blood Pressure
Aging and chronic blood pressure elevation are the two primary drivers of arterial stiffening [8:9]. In healthy pediatric populations, central arterial stiffness progresses predictably, with a normal rate of cfPWV progression of 0.12 m/s per year of age (95% CI: 0.07 to 0.16 m/s) [27].
With advancing age in adults, this progression accelerates as elastin fibers undergo structural fatigue and breakdown [3:25][28]. Because chronic hypertension exposes the arterial wall to persistent circumferential stress, it dramatically accelerates this structural remodeling [3:26][29]. High-quality community cohorts show that elevated cfPWV is the most prevalent form of Hypertension-Mediated Organ Damage (HMOD), occurring in 40% to 60% of hypertensive individuals, whereas peripheral damage (such as a low ankle-brachial index) occurs in less than 5% [29:1].
¶ Incremental Risk Prediction & Clinical Guidelines
Carotid-femoral PWV is not merely a marker of vascular age; it provides significant incremental prognostic information regarding future clinical events beyond traditional risk calculators like the Framingham Risk Score [5:4][29:2]:
- Quantitative Risk Scaling: A systematic meta-analysis of prospective trials demonstrates that a 1 m/s increase in cfPWV is associated with a 12% increase in risk for total cardiovascular events (RR 1.12, 95% CI: 1.07-1.18) and a 9% increase in cardiovascular mortality (RR 1.09, 95% CI: 1.04-1.14) [4:6].
- High-Risk Target Populations: The predictive value of elevated central arterial stiffness is significantly higher in individuals with higher baseline disease risk, such as those with pre-existing coronary artery disease or end-stage renal disease [4:7].
- Moderate Blood Pressure Utility: The clinical utility of cfPWV is highly pronounced in patients with "moderate" or borderline blood pressure (120–159 / 80–99 mmHg), where standard cardiovascular risk scores frequently fail to identify those who would benefit most from early treatment [5:5]. Adding cfPWV to traditional models significantly improves the discrimination C-index (change of 0.0048, p=0.041), and simulation models indicate that cfPWV-guided treatment in this population could reduce clinical event rates [5:6].
¶ Guideline-Defined Cutoffs vs. Consumer Metrics
In clinical medicine, established guidelines define specific, validated thresholds to identify patients at high risk who require aggressive cardiovascular management:
- Central cfPWV Gold Standard Cutoff: The international consensus document establishes a threshold of 10.0 m/s to define high cardiovascular risk and significant subclinical target organ damage [1:14][20:1]. In specific populations, localized risk associations have been refined; for instance, in hypertensive Chinese cohorts, elevated cfPWV is significantly correlated with a high risk of developing atherosclerotic cardiovascular disease (ASCVD ≥ 10%), serving as an effective clinical predictor [30].
- Peripheral baPWV Cutoffs: In Japanese clinical guidelines, clear risk-stratification categories are defined for baPWV [31]:
- Low Risk:
< 14.0 m/s(representing normal vascular function). - Medium Risk:
14.0 to 18.0 m/s(indicating intermediate arterial stiffening). - High Risk:
≥ 18.0 m/s(strongly associated with advanced target organ damage and future coronary events).
- Low Risk:
In stark contrast, consumer health wearables (such as smart scales, rings, or watches) utilize photoplethysmography (PPG) sensors at the finger or wrist to calculate proprietary, non-standardized scores, such as "Vascular Age" or "Vessel Health Indices." These consumer metrics:
- Lack Peer-Reviewed Validation: There is zero high-tier clinical evidence establishing a correlation between these consumer scores and hard cardiovascular outcomes, such as stroke, myocardial infarction, or mortality.
- Confounding Algorithms: They rely on proprietary mathematical models that are highly sensitive to superficial skin blood flow, ambient temperature, and motion artifacts.
- No Central Assessment: They cannot directly measure central aorta stiffness (the actual site of elastic buffering), making them poor surrogates for medical-grade cfPWV.
¶ Therapeutic Reverse-Remodeling vs. Passive Pressure Drop
Evaluating the success of an intervention (such as lifestyle modification or pharmacotherapy) using repeated PWV measurements requires understanding the physiological limits of vascular reverse-remodeling [8:10][9:9].
Vascular Response to Therapy:
[Therapeutic Intervention]
/ \
v v
[Acute Vasodilation] [Structural Reverse-Remodeling]
- Immediate (minutes) - Slow (months/years)
- Passive pressure drop - Degradation of stiff collagen cross-links
- Lowers PWV passively - Rebuilding of elastic elastin matrix
- Falsely infers cure - Represents true vascular rejuvenation
While certain medications (specifically angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, and statins) and lifestyle interventions are proven to reduce PWV, a reduction in PWV does not automatically translate to a proportional reduction in long-term cardiovascular risk or structural cure [8:11][9:10]:
- The Passive Pressure Confound: Most drugs that lower arterial stiffness do so primarily by lowering mean arterial pressure, which reduces vascular smooth muscle tone and passively drops PWV immediately [3:27][9:11]. This functional, pressure-dependent improvement occurs within minutes to hours, but does not reflect any structural healing of the vessel wall [8:12][9:12].
- The Structural Remodeling Lag: True structural reverse-remodeling—characterized by the actual clearing of advanced glycation end-products (AGEs), degradation of pathologic collagen cross-links, and the re-deposition of functional elastin—occurs extremely slowly over months or years [3:28][9:13].
Therefore, serial monitoring must be interpreted with extreme caution: a short-term reduction in PWV must not be falsely extrapolated to assume true biological vascular rejuvenation or a complete reversal of cardiovascular risk, unless the improvement persists after adjusting for mean arterial pressure over a long-term follow-up [8:13][9:14].
¶ Pathological and Lifestyle Impacts
Arterial stiffness is accelerated by cardiometabolic diseases and chronic inflammation, but can be mitigated by specific lifestyle and nutritional interventions:
- Prediabetes and Diabetes: The chronic inflammatory state and hyperglycemia associated with prediabetes and diabetes mellitus cause accelerated deposition of advanced glycation end-products in the arterial wall [6:2]. Meta-analyses show that aortic stiffness (cfPWV) progresses significantly during the prediabetic stage and is severely elevated in patients with frank diabetes [6:3].
- Metabolic Syndrome: In patients with metabolic syndrome, the clustering of visceral obesity, insulin resistance, and dyslipidemia accelerates baPWV [7:4]. This systemic stiffening is clinically linked to cognitive decline, with higher baPWV acting as a strong, independent predictor of impaired working memory and executive dysfunction in older adults with metabolic syndrome [17:2].
- Chronic Inflammatory Lung Disease: Patients with COPD and severe asthma exhibit significantly elevated arterial stiffness (baPWV and central aortic PWV) [16:2][32]. Spirometry metrics (such as FEV1) are powerful, independent predictors of the severity of arterial stiffness in these patient populations [16:3].
- Nutritional and Dietary Interventions: Lifestyle modifications show direct vascular benefits. A systematic review and meta-analysis demonstrated that healthy individuals following a vegetarian diet have significantly lower central arterial stiffness, with a cfPWV mean difference of -0.43 m/s and reduced carotid intima-media thickness compared to omnivores [13:1].
- Physical Activity vs. Sedentary Behavior: Time spent in light physical activity (r = -0.16) and moderate-to-vigorous physical activity (r = -0.16) is associated with lower cfPWV, whereas sedentary behavior is positively associated with increased stiffness (r = 0.23, p<0.01) [15:1]. Habitual exercise acts to preserve vascular compliance and slow arterial aging, even in asymptomatic populations [14:1].
- Targeted Interventions: Highly purified omega-3 fatty acids, specifically high-purity EPA (1,800 mg/day for 6 months) sequentially administered to a subgroup of 21 patients (from a larger cohort of 191 on a fish-based diet), significantly reduced baPWV and increased the plasma EPA/AA ratio [11:2].
¶ Safety
¶ Clinical Contraindications
While PWV is a non-invasive, safe, and low-risk procedure, specific physiological conditions act as absolute or relative contraindications because they alter central hemodynamics or prevent the device algorithms from obtaining valid data [21:15][22:14]:
- Severe Cardiac Arrhythmias (e.g., Atrial Fibrillation, Frequent PVCs): Standard tonometric and oscillometric PWV devices rely on stable, sequential cardiac cycles to identify the "foot" of the pulse wave and calculate a reliable transit time [22:15]. In patients with atrial fibrillation or frequent ectopic beats, the extreme beat-to-beat variability in stroke volume, pulse amplitude, and cycle length makes accurate mathematical calculation of transit time impossible, resulting in highly erroneous values [22:16][9:15].
- Severe Peripheral Artery Disease (PAD) of the Lower Extremities: For brachial-ankle PWV (baPWV), the presence of severe peripheral artery disease can severely confound measurement accuracy [7:5][21:16]. Severe arterial stenosis in the lower limbs dampens the pulse volume waveform, delays the arrival of the pulse wave at the ankle, and produces inaccurate baPWV measurements that do not reflect central aortic stiffness [21:17].
- Recent Extremity Surgery or Arterial Shunts: Inflation of blood pressure cuffs on limbs with active vascular access shunts (for hemodialysis), deep vein thrombosis, or recent vascular surgery is contraindicated [21:18].
¶ Clinical Framework: Screening, Diagnosis, Monitoring & Consumer Extrapolation
To maintain professional clinical standards, clinicians and practitioners must distinguish between the varying roles of PWV in different medical and wellness contexts:
- Screening (Vascular Risk Profiling): PWV is highly validated for screening asymptomatic, high-risk populations (such as hypertensive, diabetic, or geriatric patients) to detect early, subclinical Target Organ Damage (HMOD) [29:3][19:11]. Identifying elevated stiffness allows for aggressive primary prevention before clinical events occur [5:7].
- Diagnosis (Not a Standalone Diagnostic): PWV is not a primary diagnostic tool for specific clinical pathologies. For instance, an elevated cfPWV of 11.5 m/s cannot diagnose coronary artery disease, renal stenosis, or structural heart disease on its own [1:15][21:19]. It is a functional physiological parameter that must be integrated with anatomical and clinical diagnostic modalities [1:16].
- Monitoring (Therapeutic Tracking): Serial measurement of PWV can be utilized to monitor systemic vascular response to antihypertensive or lifestyle therapies over time [9:16]. However, clinicians must interpret changes cautiously, ensuring that blood pressure is calibrated and normalized on the day of the test to avoid mistaking a passive pressure drop for true vascular healing [8:14][9:17].
- Consumer Extrapolation (The "Longevity Age" Trap): Wellness coaches and longevity enthusiasts frequently extrapolate transient changes in consumer-grade vascular metrics to claim a reversal of biological age or systemic rejuvenation. This practice represents a severe clinical error. Extrapolating a structural cure or vascular rejuvenation from short-term, pressure-dependent fluctuations in PWV is medically invalid and lacks high-tier supportive evidence [8:15][9:18].
¶ Appropriate Clinical Follow-Up
High PWV Detected (cfPWV > 10 m/s or baPWV > 18 m/s)
│
▼
[Systemic Organ Damage Evaluation]
├───────────────────────────┐
▼ ▼
[Renal Assessment] [Cardiometabolic Screening]
- Microalbuminuria test - Same-day blood pressure check
- Urine Albumin-to-Creatinine - Fasting glucose & HbA1c
- Lipid panel & EPA/AA ratio
│ │
└─────────────┬─────────────┘
▼
[Therapeutic Optimization]
- Initiate/optimize RAS inhibitors (ACEi/ARBs)
- Optimize statin therapy
- Support physical activity & dietary changes
When a standardized medical-grade measurement detects elevated arterial stiffness (e.g., cfPWV > 10 m/s or baPWV > 18 m/s), a structured clinical workup is required [1:17][31:1]:
- Evaluate for Subclinical Target Organ Damage: Because elevated arterial stiffness directly exposes peripheral microvascular beds to high pressure, clinicians should immediately check for microalbuminuria [25:1]. Baseline baPWV is a powerful, independent predictor of the development of future microalbuminuria in patients with essential hypertension; therefore, checking the Urine Albumin-to-Creatinine Ratio (UACR) is mandatory [25:2][26:5].
- Cardiometabolic Risk Screening: Patients must undergo comprehensive screening for silent risk factors, including same-day blood pressure check, fasting blood glucose and HbA1c (to rule out prediabetes and diabetes) [6:4], lipid panels [10:5], and plasma EPA/AA ratios [11:3].
- Optimize Therapeutic Interventions: Clinicians should optimize medical and lifestyle therapies to reduce central aortic pressures. This includes initiating or adjusting renin-angiotensin-system (RAS) inhibitors (ACE inhibitors or angiotensin receptor blockers), which act on peripheral muscular arteries to reduce wave reflection amplitude and lower central systolic pressure independently of brachial blood pressure [3:29]. Statin therapy should be optimized to reduce aortic wave reflection [10:6], and targeted lifestyle support (such as aerobic exercise and a balanced vegetarian or fish-rich diet) should be prescribed [13:2][14:2][11:4].
¶ FAQ
¶ What is the clinical gold standard for measuring arterial stiffness?
Carotid-femoral pulse-wave velocity (cfPWV) is the universally accepted gold standard. It directly measures the transit time of the pulse wave through the descending aorta, which is the most clinically relevant elastic vascular segment [1:18][21:20].
¶ How does brachial-ankle PWV (baPWV) differ from carotid-femoral PWV (cfPWV)?
While cfPWV measures central aortic stiffness, baPWV measures a combination of central and peripheral muscular arterial stiffness [8:16][21:21]. baPWV is simpler to perform because it uses automatic limb cuffs, but its values are systematically higher than cfPWV by an average of 5.03 m/s, meaning they are not directly interchangeable [26:6][21:22].
¶ Why is the Augmentation Index (AIx) considered limited for assessing arterial wall structure?
The Augmentation Index is a mathematical ratio of augmentation pressure to pulse pressure [19:12]. Because both of these pressures fluctuate dynamically with heart rate, height, and acute changes in peripheral vascular tone, a change in AIx may occur without any change in the structural stiffness of the arterial wall itself [19:13][3:30].
¶ Can you reverse arterial stiffness with diet and lifestyle?
Yes, clinical evidence shows that structural vascular aging can be slowed and functional stiffness improved [3:31][9:19]. Meta-analyses show that vegetarian diets are associated with significantly lower cfPWV (-0.43 m/s) [13:3], habitual physical activity reduces stiffness [14:3], and interventions like high-purity EPA (1,800 mg/day) and statin therapy can significantly improve arterial hemodynamics [11:5][10:7].
¶ How do acute blood pressure changes affect a PWV measurement?
Blood pressure is a major confounding determinant of PWV [8:17]. An acute increase in blood pressure stretches the arterial wall, transferring mechanical load from compliant elastin to stiff collagen fibers, passively increasing PWV [3:32][9:20]. To evaluate true structural stiffness, measurements must be standardized to a resting state, and blood pressure must be measured on the same day [1:19][9:21].
¶ Are consumer-grade "vascular age" scores on smart devices accurate?
No. Consumer-grade devices calculate proprietary, non-standardized vascular scores using PPG sensors at the wrist or finger. These consumer metrics lack rigorous peer-reviewed clinical validation, are highly sensitive to motion and temperature artifacts, and cannot measure the central aorta. They should never be used as a substitute for medical-grade cfPWV or baPWV assessments.
¶ References
Van Bortel LM, Laurent S, Boutouyrie P, et al. Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity. Journal of Hypertension. 2012;30(3):445-448. https://pubmed.ncbi.nlm.nih.gov/22278144/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Townsend RR. Arterial Stiffness: Recommendations and Standardization. Pulse (Basel). 2017;4(Suppl 1):3-7. https://pubmed.ncbi.nlm.nih.gov/28275588/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Nichols WW. Clinical measurement of arterial stiffness obtained from noninvasive pressure waveforms. American Journal of Hypertension. 2005;18(1 Pt 1):3-10. https://pubmed.ncbi.nlm.nih.gov/15683725/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zhong Q, Hu MJ, Cui YJ, et al. Carotid-Femoral Pulse Wave Velocity in the Prediction of Cardiovascular Events and Mortality: An Updated Systematic Review and Meta-Analysis. Angiology. 2018;69(7):617-626. https://pubmed.ncbi.nlm.nih.gov/29172654/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Pavey H, Wood A, McEniery CM, et al. Association between carotid-femoral pulse wave velocity and cardiovascular disease in individuals with moderate blood pressure: a systematic review and individual participant meta-analysis. BMJ Open. 2025;15(12):e084321. https://pubmed.ncbi.nlm.nih.gov/41401986/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Liang X, Li D, Wang Z. Aortic Stiffness Measured by Carotid Femoral-Pulse Wave Velocity at Different Stages of Normal Glucose, Prediabetes, and Diabetes Mellitus: A Systematic Review and Meta-Analysis. Reviews in Cardiovascular Medicine. 2024;25(9):312. https://pubmed.ncbi.nlm.nih.gov/39355589/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Tsubakimoto A, Saito I, Mannami T. Impact of metabolic syndrome on brachial-ankle pulse wave velocity in Japanese. Hypertension Research. 2006;29(1):29-37. https://pubmed.ncbi.nlm.nih.gov/16715651/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Tomiyama H, Yamashina A. [Pulse wave velocity]. Rinsho Byori. 2004;52(8):665-672. https://pubmed.ncbi.nlm.nih.gov/15478622/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kim HL. The Value of Serial Measurement of Arterial Stiffness in Cardiovascular Disease. Reviews in Cardiovascular Medicine. 2024;25(1):32. https://pubmed.ncbi.nlm.nih.gov/39077652/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sahebkar A, Pećin I, Tedeschi-Reiner E, et al. Effects of statin therapy on augmentation index as a measure of arterial stiffness: A systematic review and meta-analysis. International Journal of Cardiology. 2016;212:272-278. https://pubmed.ncbi.nlm.nih.gov/27038725/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Fukuoka Y, Nuruki N, Amiya S, et al. Effects of a fish-based diet and administration of pure eicosapentaenoic acid on brachial-ankle pulse wave velocity in patients with cardiovascular risk factors. Journal of Cardiology. 2014;63(3):215-221. https://pubmed.ncbi.nlm.nih.gov/24080436/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lee SJ, Avolio A, Seo DC, et al. Relationship Between Brachial-Ankle Pulse Wave Velocity and Incident Hypertension According to 2017 ACC/AHA High Blood Pressure Guidelines. Journal of the American Heart Association. 2019;8(16):e013019. https://pubmed.ncbi.nlm.nih.gov/31412746/ ↩︎ ↩︎
Saz-Lara A, Battino M, Del Saz Lara A, et al. Differences in carotid to femoral pulse wave velocity and carotid intima media thickness between vegetarian and omnivorous diets in healthy subjects: a systematic review and meta-analysis. Food & Function. 2024;15(3):1214-1225. https://pubmed.ncbi.nlm.nih.gov/38230750/ ↩︎ ↩︎ ↩︎ ↩︎
Lear R, Metcalf B, Brailey G, et al. Associations of habitual physical activity and carotid-femoral pulse wave velocity; a systematic review and meta-analysis of observational studies. PLoS One. 2023;18(3):e0283421. https://pubmed.ncbi.nlm.nih.gov/37023122/ ↩︎ ↩︎ ↩︎ ↩︎
Germano-Soares AH, Andrade-Lima A, Menêses AL, et al. Association of time spent in physical activities and sedentary behaviors with carotid-femoral pulse wave velocity: A systematic review and meta-analysis. Atherosclerosis. 2018;269:211-218. https://pubmed.ncbi.nlm.nih.gov/29407596/ ↩︎ ↩︎
Chen R, He W, Zhang K, et al. Airflow obstruction was associated with elevation of brachial-ankle pulse wave velocity but not ankle-brachial index in aged patients with chronic obstructive pulmonary disease. Atherosclerosis. 2015;242(1):121-125. https://pubmed.ncbi.nlm.nih.gov/26188536/ ↩︎ ↩︎ ↩︎ ↩︎
Gosalia J, Montgomery PS, Zhang S, et al. Increased pulse wave velocity is related to impaired working memory and executive function in older adults with metabolic syndrome. GeroScience. 2022;44(6):3211-3221. https://pubmed.ncbi.nlm.nih.gov/35980564/ ↩︎ ↩︎ ↩︎
Dogdus M, Akhan O, Ozyasar M, et al. Evaluation of Arterial Stiffness Using Pulse Wave Velocity and Augmentation Index in Patients with Chronic Venous Insufficiency. International Journal of Vascular Medicine. 2018;2018:7290135. https://pubmed.ncbi.nlm.nih.gov/30631600/ ↩︎
Cheng LT, Tang LJ, Cheng L, et al. Limitation of the augmentation index for evaluating arterial stiffness. Hypertension Research. 2007;30(8):723-731. https://pubmed.ncbi.nlm.nih.gov/17917319/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Anastasio F, Testa M, Ferreri C, et al. The Analysis of Arterial Stiffness in Heart Failure Patients: The Prognostic Role of Pulse Wave Velocity, Augmentation Index and Stiffness Index. Journal of Clinical Medicine. 2022;11(12):3501. https://pubmed.ncbi.nlm.nih.gov/35743576/ ↩︎ ↩︎
Sugawara J, Tanaka H. Brachial-Ankle Pulse Wave Velocity: Myths, Misconceptions, and Realities. Pulse (Basel). 2015;3(2):106-113. https://pubmed.ncbi.nlm.nih.gov/26587459/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Milan A, Zocaro G, Leone D, et al. Current assessment of pulse wave velocity: comprehensive review of validation studies. Journal of Hypertension. 2019;37(8):1547-1557. https://pubmed.ncbi.nlm.nih.gov/30882597/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Li Y, Dolan E, Wang JG, et al. Ambulatory arterial stiffness index: determinants and outcome. Blood Pressure Monitoring. 2006;11(2):107-110. https://pubmed.ncbi.nlm.nih.gov/16534414/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Jerrard-Dunne P, Mahmud A, Feely J, et al. Ambulatory arterial stiffness index, pulse wave velocity and augmentation index--interchangeable or mutually exclusive measures? Journal of Hypertension. 2008;26(3):435-440. https://pubmed.ncbi.nlm.nih.gov/18300865/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Munakata M, Miura Y, Yoshinaga K. Higher brachial-ankle pulse wave velocity as an independent risk factor for future microalbuminuria in patients with essential hypertension: the J-TOPP study. Journal of Hypertension. 2009;27(7):1466-1471. https://pubmed.ncbi.nlm.nih.gov/19412131/ ↩︎ ↩︎ ↩︎
Kyriakoulis KG, Chatzopoulos M, Komnianou A, et al. Brachial-ankle versus carotid-femoral pulse wave velocity: a systematic review and meta-analysis. Journal of Hypertension. 2025;43(11):1-10. https://pubmed.ncbi.nlm.nih.gov/40986695/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Stoner L, Kucharska-Newton A, Meyer ML, et al. Cardiometabolic Health and Carotid-Femoral Pulse Wave Velocity in Children: A Systematic Review and Meta-Regression. The Journal of Pediatrics. 2020;218:207-213. https://pubmed.ncbi.nlm.nih.gov/31810627/ ↩︎
Zhang Y, Agnoletti D, Xu Y. Carotid-femoral pulse wave velocity in the elderly. Journal of Hypertension. 2014;32(8):1551-1556. https://pubmed.ncbi.nlm.nih.gov/24721930/ ↩︎
Vasan RS, Song RJ, Xanthakis V. Hypertension-Mediated Organ Damage: Prevalence, Correlates, and Prognosis in the Community. Hypertension. 2022;79(3):505-515. https://pubmed.ncbi.nlm.nih.gov/35138872/ ↩︎ ↩︎ ↩︎ ↩︎
Chang G, Hu Y, Ge Q. Arterial Stiffness as a Predictor of the Index of Atherosclerotic Cardiovascular Disease in Hypertensive Patients. International Journal of Environmental Research and Public Health. 2023;20(4):2841. https://pubmed.ncbi.nlm.nih.gov/36833532/ ↩︎
Kabutoya T, Kario K. Comparative Assessment of Cutoffs for the Cardio-Ankle Vascular Index and Brachial-Ankle Pulse Wave Velocity in a Nationwide Registry: A Cardiovascular Prognostic Coupling Study. Pulse (Basel). 2019;6(3-4):158-163. https://pubmed.ncbi.nlm.nih.gov/31049312/ ↩︎ ↩︎
Karoli NA, Zarmanbetova OT, Rebrov AP. [Clinical and diagnostical value of 24-hour arterial stiffness monitoring in patients with bronchial asthma]. Terapevticheskii Arkhiv. 2020;92(4):21-27. https://pubmed.ncbi.nlm.nih.gov/32598790/ ↩︎