¶ Bile Acid Malabsorption
| Alternative Name | Bile Acid Diarrhea (BAD) |
| Primary Marker | SeHCAT retention, Serum C4, Serum FGF19, Fecal Bile Acids |
| Primary Therapy | Bile acid binders (e.g., Colesevelam, Cholestyramine), Ultra-low-fat diet |
| Access | Rx (binders), OTC / Lifestyle (diet) |
| Safety Risk | Fat-soluble vitamin deficiencies (A, D, E, K), Drug-binding interactions, Hyperoxaluria |
| Key Marker to Monitor | Triglycerides, Vitamins A/D/E/K, Prothrombin time (INR) |
Bile Acid Malabsorption (BAM), also clinically termed Bile Acid Diarrhea (BAD), is a chronic gastrointestinal disorder characterized by the failure of the terminal ileum to reabsorb bile acids. This failure allows excessive quantities of bile acids to spill into the colon, where they act as potent secretagogues, driving water and electrolyte secretion, accelerating colonic transit, and manifesting as chronic, debilitating watery diarrhea [1], [2]. Often misdiagnosed as diarrhea-predominant Irritable Bowel Syndrome (IBS-D), BAM is a highly treatable underlying cause of chronic diarrhea that remains severely underdiagnosed due to geographic differences in diagnostic test availability and a general lack of clinical awareness [2:1], [3].
¶ At a glance
Key points (high-level summary)
- Efficacy of Intervention: First- and second-generation bile acid sequestrants (binders) yield clinical response rates of 70% to 90% depending on the subtype of BAM [1:1], [4].
- Key Limitation or Risk: Traditional binders (e.g., cholestyramine) suffer from poor compliance due to palatability, while all binders non-specifically bind other anionic medications and interfere with fat-soluble vitamin absorption (Vitamins A, D, E, K) [5], [6].
- The Verdict: Diagnostic screening using SeHCAT, C4, or FGF19 (or an empirical binder trial) is highly indicated for any patient with unexplained watery chronic diarrhea or refractory IBS-D, offering a rapid path to complete symptom resolution [2:2], [3:1], [7].
What people use it for
- Main goals: Resolution of chronic watery diarrhea, restoration of normal bowel habit consistency, management of post-cholecystectomy diarrhea, Crohn's-associated diarrhea, and refractory IBS-D symptoms [1:2], [2:3].
- Evidence quality: High for post-ileal resection (Type 1) and post-cholecystectomy (Type 3) BAM; Moderate-to-High for primary/idiopathic (Type 2) BAM [1:3], [4:1].
¶ What is it?
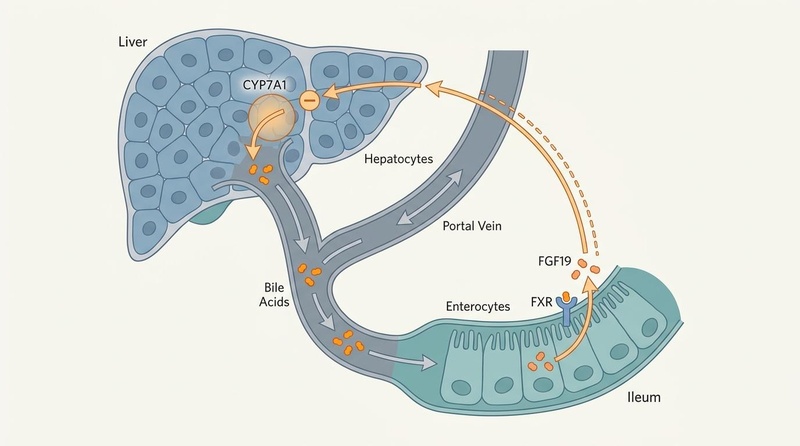
Bile acid malabsorption represents a disruption in the enterohepatic circulation of bile acids [2:4]. Under physiological conditions, the liver synthesizes approximately 0.5 grams of primary bile acids (cholic acid and chenodeoxycholic acid) daily from cholesterol via the rate-limiting enzyme cholesterol 7α-hydroxylase (CYP7A1) [8]. These bile acids are conjugated with glycine or taurine, stored in the gallbladder, and secreted into the duodenum following meal ingestion to assist in lipid emulsification and micelle formation [8:1].
Approximately 95% of bile acids are actively reabsorbed in the terminal ileum via the apical sodium-dependent bile acid transporter (ASBT) [1:4], [9]. They enter the portal circulation and return to the liver, completing the loop. The remaining 5% escape into the colon, where colonic bacteria deconjugate and dehydroxylate them into secondary bile acids (deoxycholic acid and lithocholic acid) before excretion [8:2].
When the reabsorption capacity of the terminal ileum is exceeded or compromised, a massive volume of bile acids enters the colon [2:5]. At colonic concentrations exceeding 1.5–3.0 mM, bile acids induce a secretory state by activating adenylate cyclase, increasing mucosal permeability, stimulating mucus secretion, and inducing high-amplitude propagating contractions (HAPCs) [1:5], [10]. The clinical result is chronic, urgent, often postprandial watery diarrhea.
+--------------------------------------------------------------+
| HEPATIC BILE ACID SYNTHESIS |
| Cholesterol --[CYP7A1]--> Bile Acids |
+--------------------------------------------------------------+
| (Secretion)
v
+--------------------------------------------------------------+
| SMALL INTESTINE |
| Lipid Emulsification & Digestion |
+--------------------------------------------------------------+
| (Active Transport via ASBT)
v
+--------------------+ +-------------------+
| TERMINAL ILEUM | --(Portal Vein)--> | LIVER |
| 95% Reabsorbed | <================== | Bile Acid Pool |
+--------------------+ +-------------------+
| (5% Escape) ^
| | (FGF19 Inhibition)
v |
+--------------------+ +-------------------+
| COLON | ===(Binds FXR)===> | FGF19 Pathway |
| Secretory Diarrhea | | Negative Feedback |
+--------------------+ +-------------------+
¶ The Three Subtypes of BAM
Gastroenterologists classify bile acid malabsorption into three distinct pathological phenotypes [1:6], [11]:
- Type 1 (Secondary to Ileal Dysfunction): Compromise of the terminal ileum due to structural disease, surgical resection, or localized mucosal damage [1:7], [11:1]. This is most frequently seen in patients with Crohn's Disease (active terminal ileitis), ileal resections (where resections >20 cm significantly impair ASBT capacity), radiation enteritis, or surgical bypass [1:8], [11:2].
- Type 2 (Primary / Idiopathic): Idiopathic overproduction of bile acids or defective feedback regulation in the absence of obvious ileal disease [1:9], [2:6]. This subtype is heavily linked to a defect in the intestinal hormone Fibroblast Growth Factor 19 (FGF19), which impairs the hepatic shut-off mechanism, leading to unchecked primary bile acid synthesis [9:1], [6:1].
- Type 3 (Secondary to Other Gastrointestinal Conditions): Altered gastrointestinal motility, anatomy, or luminal biochemistry [1:10], [11:3]. Key triggers include post-cholecystectomy diarrhea (the constant, unbuffered trickle of bile into the duodenum overloads the ileum) [2:7], Small Intestinal Bacterial Overgrowth (SIBO) (bacterial deconjugation of bile acids prematurely in the small intestine prevents active reabsorption) [12], celiac disease, chronic pancreatitis (impaired pancreatic bicarbonate secretion reduces luminal pH, causing bile acids to precipitate and escape reabsorption) [2:8], and microscopic colitis [13].
¶ Chronic Diarrhea and IBS-D Overlap
A substantial body of clinical trials and systematic reviews reveals that approximately 25% to 35% of patients meeting the Rome IV criteria for diarrhea-predominant Irritable Bowel Syndrome (IBS-D) actually suffer from underlying Bile Acid Malabsorption (primarily Type 2) [3:2], [7:1]. Because the symptoms are virtually indistinguishable—characterized by watery stools, urgent defecation, abdominal cramping, and bloating—millions of patients are mismanaged with general antidiarrheals or dietary restrictions (like low-FODMAP) when targeted bile acid binder therapy would resolve their condition [7:2], [14]. Clinical guidelines from United European Gastroenterology (UEG) and the European Society for Neurogastroenterology and Motility (ESNM) strongly advocate for diagnostic screening of BAM in all patients presenting with chronic diarrhea or refractory IBS-D [7:3].
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect | Consistency | Evidence quality | Trials | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Stool Frequency Reduction | High | High | >15 clinical studies, 1 Meta-analysis | Significant reduction in daily bowel movements (by 50% to 70%) across all BAM subtypes [4:2], [6:2]. | |
| Bowel Movement Urgency | High | Moderate-to-High | 8 prospective cohorts | Marked decrease in urgency and fecal incontinence scores within 4 to 7 days of initiation [4:3], [15]. | |
| Stool Consistency (Bristol Scale) | High | High | 1 Meta-analysis, 10 RCTs | Normalization of stool consistency from Bristol Type 6/7 (watery) to Bristol Type 3/4 (formed) [4:4], [6:3]. | |
| Quality of Life (QoL) Scores | High | Moderate | 6 cohort studies | Substantive improvement in overall daily functioning, social confidence, and travel anxiety [15:1]. | |
| Fat-Soluble Vitamin Status | Moderate | High | 5 observational studies | Potential long-term decline in lipophilic micronutrients over multi-year sequestrant therapy, requiring serial monitoring [5:1], [6:4]. | |
| Triglyceride Elevation | Moderate | Moderate | 4 clinical trials | Possible compensatory increase in hepatic VLDL synthesis, elevating serum triglycerides by 10% to 20% [16], [17]. |
¶ Mechanisms of Action
Understanding the cellular pathways of bile acid metabolism is critical to diagnosing and managing the condition. The entire cycle relies on precise receptor signaling, active mucosal transport, and endocrine negative feedback loops [2:9], [8:3].
¶ 1. Active Ileal Reabsorption (ASBT)
Active reabsorption is mediated by the Apical Sodium-Dependent Bile Acid Transporter (ASBT), located exclusively on the brush border membrane of enterocytes in the terminal ileum [2:10], [9:2]. ASBT is a cotransporter that couples the entry of two sodium ions with one bile acid molecule, driven by the sodium gradient generated by basolateral Na+/K+ ATPase [9:3]. Once inside the enterocyte, bile acids are transported across the cytoplasm by the ileal bile acid-binding protein (IBABP) and exported across the basolateral membrane into the portal vein by the organic solute transporter alpha/beta (OSTα/OSTβ) [9:4]. Physical damage to the ileal mucosa (e.g., Crohn's enteritis) or surgical removal of the terminal ileum directly strips the mucosal surface of ASBT, driving Type 1 BAM [1:11], [11:4].
¶ 2. The FXR-FGF19 Endocrine Feedback Loop
Under normal conditions, intracellular bile acids act as natural ligands for the Farnesoid X Receptor (FXR), a nuclear receptor highly expressed in ileal enterocytes [9:5], [6:5]. When bile acids bind to FXR, they induce the transcription and basolateral release of the peptide hormone Fibroblast Growth Factor 19 (FGF19) [9:6], [6:6].
FGF19 enters the portal circulation and travels to the liver, where it binds to a cell-surface receptor complex consisting of Fibroblast Growth Factor Receptor 4 (FGFR4) and the obligate co-receptor β-Klotho on hepatocytes [2:11], [9:7]. This binding initiates an intracellular signaling cascade (involving JNK and ERK1/2 pathways) that suppresses the transcription of the gene encoding CYP7A1 (cholesterol 7α-hydroxylase) [2:12], [8:4]. CYP7A1 is the rate-limiting enzyme in hepatic bile acid synthesis [8:5].
In Type 2 (Primary) BAM, this feedback loop is broken [9:8], [6:7]. Fasting serum levels of FGF19 are significantly reduced, and enterocytes fail to secrete adequate FGF19 in response to bile acid stimulation [9:9]. Consequently, the liver receives no inhibitory signal, resulting in a continuous, unchecked, massive overproduction of primary bile acids that completely overwhelms the normal reabsorption capacity of the ASBT, causing diarrhea [6:8].
¶ 3. Colonic Mucosal Action of Bile Acids
Once excessive bile acids enter the colon, they act as mechanical and biological detergents that alter mucosal function through multiple distinct pathways [1:12], [10:1]:
- Secretor Effect: Bile acids stimulate the colonic mucosa to secrete water and chloride ions. This is mediated by the intracellular accumulation of cyclic adenosine monophosphate (cAMP) and the activation of apical cystic fibrosis transmembrane conductance regulator (CFTR) chloride channels [10:2].
- Increased Permeability: At high concentrations, bile acids loosen tight junctions (occludin and zonula occludens-1), increasing paracellular permeability and driving passive fluid accumulation in the colonic lumen [2:13], [10:3].
- Motility Acceleration: Bile acids stimulate colonic mechanoreceptors and prompt mucosal mast cells to release histamine and 5-hydroxytryptamine (serotonin), triggering high-amplitude propagating contractions that clinically present as severe cramping and urgent defecation [2:14], [10:4].
¶ Diagnostic Evaluation
One of the greatest challenges in managing BAM is the high rate of misdiagnosis [2:15], [3:3]. Multiple diagnostic modalities exist, but their clinical utility and availability vary dramatically by global region [3:4], [7:4].
¶ Diagnostic Tests Comparison Table
| Diagnostic Test | Mechanism | Normal Reference Range | Sensitivity / Specificity | Geographic Availability | Clinical Advantages & Disadvantages |
|---|---|---|---|---|---|
| SeHCAT Scan | 7-day retention of a gamma-emitting synthetic bile acid analog (Se-HCAT) [18]. | >15% retention is normal [15:2]. | 95% / 93% [3:5]. | UK, Europe, Canada (Not FDA approved/US) [15:3]. | Gold Standard. Extremely accurate. Graduated classification of severity. Disadvantage: Requires nuclear medicine and two clinic visits 7 days apart [18:1]. |
| Serum C4 | LC-MS/MS measurement of 7α-hydroxy-4-cholesten-3-one, an intermediate of bile acid synthesis [19]. | <30 ng/mL (fasting morning draw) [3:6], [19:1]. | 90% / 85% [3:7]. | Globally available, expanding in US [3:8], [19:2]. | Simple venipuncture. Correlates well with hepatic overproduction. Disadvantage: Subject to diurnal variation; falsely elevated in liver disease or during binder therapy [19:3]. |
| Serum FGF19 | ELISA measurement of fasting circulating FGF19 hormone [6:9]. | >145 pg/mL is normal [6:10]. | 80% / 86% [6:11]. | Primarily research settings, expanding commercially [6:12]. | Direct assessment of the feedback pathophysiology in Type 2 BAM. Disadvantage: High diurnal fluctuation; overlap between normal and diseased populations [6:13]. |
| Fecal Bile Acids (48h/72h) | Stool collection with quantitative extraction of individual/total bile acids [20]. | <1000 µmol/72h (or <10% primary bile acids) [3:9], [20:1]. | 90% / 90% [3:10]. | United States (Mayo Clinic Laboratories, etc.) [3:11]. | US Gold Standard. Directly measures the chemical offending agent in stool. Disadvantage: Cumbersome and highly unpleasant 3-day stool collection [20:2]. |
| Empirical Binder Trial | Clinical therapeutic trial of a bile acid sequestrant (e.g., Cholestyramine) [7:5]. | Response defined as >50% reduction in stool frequency within 7–10 days [7:6]. | Diagnostic surrogate only; poor specificity [7:7]. | Globally available [7:8]. | Low cost, rapid, no specialized equipment. Disadvantage: Poor compliance can lead to false-negative diagnosis; does not differentiate pathology [7:9]. |
¶ The SeHCAT Scan: Graduated Severity
In countries where the Selenium-75-homocholic acid taurine (SeHCAT) scan is available, clinicians use the 7-day retention percentage to classify the severity of BAM, which strongly predicts the success of treatment [15:4], [18:2]:
- Severe BAM: <5% retention. Response rate to bile acid sequestrants is exceptionally high (>90%) [15:5].
- Moderate BAM: 5% to 10% retention. Response rate is approximately 70% to 80% [15:6].
- Mild BAM: 10% to 15% retention. Response rate is more variable (~50%), and dietary fat modification may play a larger role [15:7].
¶ Therapeutic Protocols & Management
Therapy is highly effective, aiming to sequester luminal bile acids before they reach the colon or, in emerging therapies, downregulate their hepatic synthesis [1:13], [4:5].
¶ 1. Pharmacological: Bile Acid Sequestrants
Bile acid sequestrants (binders) are positively charged anion-exchange resins that bind to the negatively charged carboxyl groups of bile acids in the small intestinal lumen, forming an insoluble complex that cannot be reabsorbed or stimulate the colonic mucosa, and is excreted harmlessly in feces [5:2].
¶ First-Generation Binders (Anion Exchange Resins)
- Cholestyramine (Questran):
- Form: Powder packets. Must be dissolved in water or juice.
- Dosing: Start with 4g (1 packet) once daily with a meal. Titrate upward by 4g increments weekly based on clinical response [5:3].
- Maintenance Dose: Usually 4g to 12g daily, split into 2–3 doses taken with major fat-containing meals [5:4].
- Limitations: Poor palatability (sandy, gritty texture), high rate of compliance failure (up to 40-50%), and significant risk of bloating, gas, and abdominal cramping [6:14].
- Colestipol (Colestid):
- Form: Powder packets or 1g tablets.
- Dosing: Start with 2g of powder or 2 tablets daily. Titrate upward to a maximum of 16g/day [5:5].
- Limitations: Large pill size can make swallowing difficult; intermediate tolerability.
¶ Second-Generation Binders (High-Affinity Polymeric Binders)
- Colesevelam (Welchol, Cholestagel):
- Form: 625mg tablets or oral suspension.
- Dosing: Start with 1.875g daily (3 tablets of 625mg, taken together with a fat-containing meal or split as 2 tablets with breakfast and 1 with dinner). Titrate upward to 3.75g daily (6 tablets) if clinical response is partial [5:6], [6:15].
- Why it is Preferred: Colesevelam possesses a molecular structure with multi-armed hydrophobic side chains, giving it an affinity for bile acids that is 4 to 6 times higher than cholestyramine. This allows for a lower pill burden, avoids gritty powders, and is associated with significantly fewer gastrointestinal side effects (e.g., bloating, constipation) [5:7], [6:16].
CLINICAL PROTOCOL CARD: PHARMACOLOGICAL TITRATION
- Baseline Labs: Screen fasting serum lipid panel (especially triglycerides) and serum Vitamins A, D, E, K, and prothrombin time (INR) [6:17], [17:1].
- Initiation: Start Colesevelam 1.875g (3 x 625mg tablets) daily, taken with the largest meal of the day [5:8].
- Titration: If response is partial after 7 days (Bristol Stool Form remaining >5), increase to 3.75g (6 tablets) daily (3 with breakfast, 3 with dinner) [5:9].
- Timing Rule: Ensure all other medications are taken at least 1 hour before or 4–6 hours after any bile acid sequestrant to prevent drug-binding malabsorption [5:10].
¶ 2. Dietary Interventions: The Low-Fat Protocol
Dietary lipid intake is the primary driver of gallbladder contraction and bile acid secretion [2:16]. Therefore, dietary fat restriction is highly synergistic with binder therapy and can occasionally resolve mild cases on its own [4:6].
- Ultra-Low-Fat Diet: Restricting total dietary fat to <40 grams per day (or <20% of total daily caloric intake) minimizes the total volume of bile acids circulating through the gastrointestinal tract [6:18].
- Fat Quality and Distribution: Avoid large boluses of fat in a single sitting. Distribute fat intake evenly across 4–5 small meals daily to prevent sudden gallbladder contraction from overwhelming the terminal ileum's remaining ASBT transport capacity.
- Medium-Chain Triglyceride (MCT) Substitution: In patients with severe Type 1 BAM (who have undergone extensive ileal resections and have a highly depleted bile acid pool, resulting in steatorrhea), standard dietary fats (LCTs) cannot be absorbed and will exacerbate diarrhea [2:17]. Clinicians should replace long-chain dietary fats with MCT oil (10–15g per meal), as MCTs are absorbed directly across the intestinal mucosa into the portal vein without requiring emulsification by bile acids or pancreatic lipase [11:5].
¶ 3. Emerging Medical Therapies
- GLP-1 Receptor Agonists (e.g., Liraglutide, Semaglutide): Emerging evidence has demonstrated that GLP-1 receptor agonists are highly effective for patients with severe, binder-refractory bile acid diarrhea [6:19], [14:1]. GLP-1 agonists slow gastric emptying, delay small bowel transit time, and possibly modulate the enterohepatic signaling loop [6:20]. In clinical case series, low-dose liraglutide (escalated from 0.6mg to 1.8mg subcutaneously daily) achieved complete clinical remission in patients who failed high-dose colesevelam, offering a novel therapeutic pathway [14:2].
- Farnesoid X Receptor (FXR) Agonists (e.g., Obeticholic Acid): By directly activating enterocyte FXR, these agents stimulate the physiological transcription and release of FGF19, downregulating hepatic CYP7A1 activity and restoring homeostatic control over bile acid synthesis [9:10], [6:21]. While highly elegant, their use is currently restricted by potential side effects, including severe pruritus (itching) and adverse lipid profile changes (elevated LDL-C) [6:22].
¶ Clinical Safety, Risk Mitigation & Monitoring
Bile acid sequestrants are non-systemic and generally safe, but their physical action in the intestinal lumen presents several clinical risks that require careful, long-term monitoring [5:11], [6:23].
CRITICAL CLINICAL WARNINGS
- Medication Malabsorption: Sequestrants bind non-specifically to anionic compounds. Taking thyroid hormone, statins, digoxin, warfarin, beta-blockers, or oral contraceptives simultaneously with a binder can result in severe treatment failure [5:12].
- Hypertriglyceridemia Risk: Binders can stimulate hepatic VLDL synthesis. In patients with high baseline triglycerides (>250 mg/dL), sequestrants can trigger severe hypertriglyceridemia, potentially causing acute pancreatitis [16:1], [17:2].
¶ 1. Serial Micronutrient Monitoring
Long-term bile acid malabsorption or the use of sequestrants impairs micellar solubilization of fat, leading to the malabsorption of lipophilic micronutrients [2:18], [5:13]. Clinicians should perform the following serial screens every 6 to 12 months [6:24]:
- Vitamin D3: Monitor 25-hydroxyvitamin D (target >30 ng/mL). Malabsorption can accelerate bone loss and osteopenia.
- Vitamin A: Monitor serum retinol levels.
- Vitamin E: Monitor serum alpha-tocopherol.
- Vitamin K1 and Coagulation: Monitor serum phytonadione or Prothrombin Time (INR). A rising INR indicates subclinical Vitamin K deficiency, which impairs the gamma-carboxylation of clotting factors II, VII, IX, and X.
- Folate and B12: Monitor periodically, as some studies show mild interference with folate absorption [5:14].
¶ 2. Enteric Hyperoxaluria and Kidney Stone Risk
In patients with significant ileal malabsorption (Type 1 BAM), unabsorbed fatty acids and bile acids enter the colon [2:19]. These lipids strongly bind to divalent calcium ions () in the colonic lumen, forming insoluble calcium soaps.
Under normal circumstances, luminal calcium binds to dietary oxalate, forming insoluble calcium oxalate that is excreted in stool. However, when calcium is consumed by unabsorbed fatty acids, dietary oxalate remains free and highly soluble. The colon absorbs this free oxalate rapidly (enteric hyperoxaluria) [2:20]. Once in the circulation, the kidneys excrete this excess oxalate, leading to calcium oxalate nephrolithiasis (kidney stones) and, in severe cases, oxalate nephropathy and renal failure.
Mitigation Protocol:
- Maintain aggressive hydration (>2.5 liters of water daily).
- Adhere strictly to a low-fat diet to prevent calcium soap formation.
- Supplement with oral calcium citrate (500–1000 mg taken with meals). The supplemental calcium binds free oxalate in the gut, forcing its excretion in feces and protecting the kidneys.
¶ 3. Red Flag Symptoms (Stop & Escalate)
While BAM is a functional-secretory disorder, patients presenting with chronic diarrhea must be screened for organic "red flags" that point to alternative diagnoses (such as colorectal cancer, severe inflammatory bowel disease, or systemic infections) [1:14], [13:1]:
- Unexplained weight loss (>5% of body weight within 6 months).
- Nocturnal diarrhea (diarrhea that awakens the patient from sleep, indicating an active secretory process independent of meals).
- Hematochezia (blood in the stool, melena, or occult blood).
- Unexplained fever or severe, persistent nocturnal sweats.
- Severe, localized abdominal pain (especially in the right lower quadrant, pointing to active Crohn's disease or appendiceal pathology).
- New-onset diarrhea in patients >50 years old without prior history of gastrointestinal dysfunction.
¶ Practical Decision-Path / Diagnostic Algorithm
Below is a clinical diagnostic algorithm designed to guide the management of chronic watery diarrhea and identify Bile Acid Malabsorption.
| Presenting Symptom | Clinical Action | Next Step / Diagnostic Decision |
|---|---|---|
| Watery Diarrhea (>4 weeks) | Screen for Red Flags [1:15]. | If Red Flags present, refer for urgent Colonoscopy/CT [13:2]. |
| No Red Flags Present | Review medical history [1:16]. | Check for prior ileal resection, Crohn's, or Cholecystectomy [2:21], [11:6]. |
| Prior Ileal Resection / Active Crohn's | Diagnose Type 1 BAM [11:7]. | Start low-dose Colesevelam and low-fat diet immediately [5:15]. |
| Prior Cholecystectomy | Suspect Type 3 BAM [2:22]. | Consider empirical trial of Colesevelam (1.875g/day) [5:16], [7:10]. |
| No Surgical History (Idiopathic) | Evaluate availability of diagnostic testing [3:12]. | Perform SeHCAT scan, Serum C4, or Fecal Bile Acids [3:13], [18:3]. |
| Testing Unavailable | Initiate Empirical Trial [7:11]. | Prescribe Cholestyramine (4g BID) or Colesevelam (1.875g BID) for 10 days [5:17]. |
| Positive Test / Symptom Resolution | Confirm BAM diagnosis [1:17], [15:8]. | Continue therapy, establish long-term micronutrient monitoring [6:25]. |
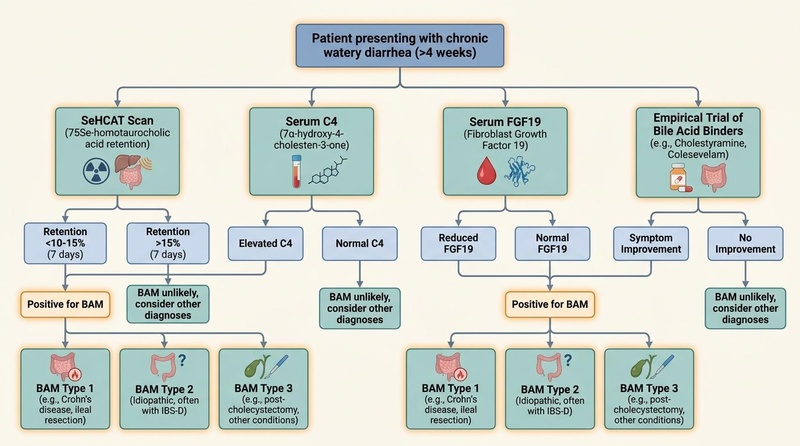
Figure 2: Comprehensive clinical flowchart illustrating the diagnostic pathways and therapeutic decisions for Bile Acid Malabsorption.
¶ Practical FAQ
How can I tell if my diarrhea is from BAM or regular IBS-D?
While symptoms overlap, BAM-induced diarrhea is classically watery, urgent, and highly postprandial (occurring shortly after eating fat-rich meals) [1:18], [2:23]. Unlike typical IBS-D, BAM diarrhea rarely alternates with constipation, is less likely to be triggered purely by psychological stress, and often persists even during fasting or during the night [2:24]. A positive response to a short trial of bile acid binders is a strong clinical indicator of BAM [7:12].
Can I treat BAM without prescription medications?
Yes, mild cases of BAM (often Type 3 post-cholecystectomy or mild Type 2) can be managed successfully with strict dietary fat restriction (<40g per day) [4:7], [6:26]. Eliminating high-fat triggers prevents the sudden release of large volumes of bile acids into the duodenum, allowing the remaining transport mechanisms in the ileum to successfully cope [2:25]. However, moderate-to-severe cases typically require a combination of diet and low-dose bile acid binders [6:27].
Why are bile acid binders so hard to tolerate, and what can I do about it?
First-generation binders like cholestyramine are insoluble resins that do not dissolve, creating a gritty, sandy mouthfeel that many patients find highly unpleasant, often leading to nausea [6:28]. Switching to colesevelam tablets avoids this issue completely [5:18]. If you must take cholestyramine, mixing the powder into thick liquids (like applesauce, yogurt, or pulpy orange juice) and chilling it before consumption can significantly improve palatability and adherence [5:19].
Will taking bile acid binders affect my other daily supplements or vitamins?
Yes, bile acid binders are highly non-specific and will physically bind to other supplements, fat-soluble vitamins, and medications [5:20]. To avoid malabsorption, you must take all other oral substances at least 1 hour before or 4 to 6 hours after your dose of bile acid binders [5:21]. Long-term use of binders also requires monitoring of fat-soluble vitamin levels (Vitamins A, D, E, K) and periodic supplementation [6:29].
Can SIBO cause bile acid malabsorption, and is it reversible?
Yes, SIBO is a well-established cause of Type 3 BAM [11:8], [12:1]. Excess bacteria in the small intestine prematurely deconjugate bile acids before they reach the terminal ileum [12:2]. Deconjugated bile acids cannot be recognized by the active ASBT transporters, preventing their reabsorption and causing them to spill into the colon [2:26], [12:3]. Once SIBO is successfully eradicated with targeted antibiotics (e.g., rifaximin), bile acid reabsorption typically normalizes completely, resolving the diarrhea [12:4].
¶ Glossary
- ASBT: Apical Sodium-Dependent Bile Acid Transporter; the key active transporter in the terminal ileum responsible for reabsorbing conjugated bile acids [9:11].
- CYP7A1: Cholesterol 7α-hydroxylase; the rate-limiting hepatic enzyme responsible for synthesizing primary bile acids from cholesterol [8:6].
- FGF19: Fibroblast Growth Factor 19; an enterocyte-derived peptide hormone that downregulates hepatic bile acid synthesis [6:30].
- FXR: Farnesoid X Receptor; a nuclear receptor activated by intracellular bile acids that triggers FGF19 expression [9:12].
- Enterohepatic Circulation: The highly efficient loop through which bile acids are synthesized in the liver, secreted into the intestine, reabsorbed in the ileum, and returned to the liver via the portal vein [8:7].
- SeHCAT: Selenium-75-homocholic acid taurine; a nuclear medicine scan used to measure fractional retention of a synthetic bile acid analog [18:4].
- Secretagogue: A substance that stimulates another substance to be secreted; in the colon, unabsorbed bile acids act as secretagogues for water and electrolytes [10:5].
¶ References
¶ Update Log
¶ March 2026
- Created comprehensive Bile Acid Malabsorption clinical guide.
- Integrated standard diagnostic pathways comparing SeHCAT, serum C4, serum FGF19, and fecal bile acid profiles.
- Established detailed first- and second-generation bile acid sequestrant dosing tables and low-fat dietary protocols.
- Documented clinical safety guidelines covering fat-soluble vitamin monitoring, medication binding timing, and hyperoxaluria management.
- Added professional-grade enterohepatic regulation and diagnostic algorithm illustrations.
Maqsood A, Fatima SK, Kumar S, et al. Primary Bile Acid Diarrhea: A Narrative Review of Pathophysiology, Diagnostic Challenges, and Emerging Therapeutic Strategies. Cureus. 2026;18(5):e108847. https://pubmed.ncbi.nlm.nih.gov/42291991/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Barbara G, Bellini M, Portincasa P, et al. Bile acid diarrhea in patients with chronic diarrhea. Current appraisal and recommendations for clinical practice. Digestive and Liver Disease. 2025;57(3):345-356. https://pubmed.ncbi.nlm.nih.gov/39827025/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Camilleri M. When and What to Test for Diarrhea: Focus on Stool Testing. The American Journal of Gastroenterology. 2025;120(4):512-523. https://pubmed.ncbi.nlm.nih.gov/39480027/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Dilmaghani S, BouSaba J, Lupianez-Merly C, et al. Meta-Analysis: Efficacy and Safety of Sequestrants for Bile Acid Diarrhoea. Alimentary Pharmacology & Therapeutics. 2025;62(12):1420-1432. https://pubmed.ncbi.nlm.nih.gov/41090475/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Patel P, John S. Cholestyramine Resin. StatPearls. 2026;12(1):30475562. https://pubmed.ncbi.nlm.nih.gov/30475562/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chinese Society of Gastroenterology, Chinese Medical Association. Chinese Expert Consensus on the Clinical Management of Bile Acid Diarrhea (2026 Version). Journal of Digestive Diseases. 2026;27(1):41757816. https://pubmed.ncbi.nlm.nih.gov/41757816/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Savarino E, Zingone F, Barberio B, et al. Functional bowel disorders with diarrhoea: Clinical guidelines of the United European Gastroenterology and European Society for Neurogastroenterology and Motility. United European Gastroenterology Journal. 2022;10(6):554-572. https://pubmed.ncbi.nlm.nih.gov/35695704/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Cheng Y, Zhang L, Zhang M, et al. Advances in research on the effects of bile acids and their receptors on intestinal function. Frontiers in Nutrition. 2026;13:42095223. https://pubmed.ncbi.nlm.nih.gov/42095223/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Winston JA. Bile Acid Dysregulation: Pathophysiology and Therapeutic Approaches to Bile Acid Diarrhea. The Veterinary Clinics of North America. Small Animal Practice. 2026;56(3):41876339. https://pubmed.ncbi.nlm.nih.gov/41876339/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wortmann E, Groll T, Strigli A, et al. Modulation of intestinal bile acids influences colonic mucosal responses. Scientific Reports. 2026;16(1):42236792. https://pubmed.ncbi.nlm.nih.gov/42236792/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Barkun AN, Love J, Gould M, et al. Bile acid malabsorption in chronic diarrhea: pathophysiology and treatment. Canadian Journal of Gastroenterology. 2013;27(11):653-659. https://pubmed.ncbi.nlm.nih.gov/24199211/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Furqan A, Sultan MT, Khalid MU, et al. Small Intestinal Bacterial Overgrowth: Microbiome Dysregulation, Gut-Brain Axis Disruption, and Systemic Consequences. Molecular Nutrition & Food Research. 2026;70(7):42378001. https://pubmed.ncbi.nlm.nih.gov/42378001/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Nielsen OH, Pardi DS. Diagnosis and Pharmacological Management of Microscopic Colitis in Geriatric Care. Drugs & Aging. 2024;41(2):112-124. https://pubmed.ncbi.nlm.nih.gov/38231321/ ↩︎ ↩︎ ↩︎
Borup C, Munck LK, Andersen NN, et al. Remission of Sequestrant-refractory Bile Acid Diarrhea in Patients on Liraglutide With Pragmatic Dose Escalation: A Case Series. Clinical Gastroenterology and Hepatology. 2026;24(1):40368130. https://pubmed.ncbi.nlm.nih.gov/40368130/ ↩︎ ↩︎ ↩︎
Damsgaard B, Dalby HR, Krogh K, et al. Long-term effect of medical treatment of diarrhoea in 377 patients with SeHCAT scan diagnosed bile acid malabsorption from 2003 to 2016; a retrospective study. Alimentary Pharmacology & Therapeutics. 2018;47(8):1077-1087. https://pubmed.ncbi.nlm.nih.gov/29368342/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Caldera F, Vattoth AL. Optimizing Bile Acid Diarrhea Treatment: The Importance of Triglyceride Screening Before Bile Acid Sequestrant Therapy. The American Journal of Gastroenterology. 2025;120(4):40208779. https://pubmed.ncbi.nlm.nih.gov/40208779/ ↩︎ ↩︎
Papadia FS, Karcz KW, Pasta A, et al. Chronic Liver Disease, Liver Damage and Liver Failure After Hypoabsorptive Bariatric Surgery: A Dose-Dependent Relationship and Multisystemic Consequences. European Journal of Clinical Investigation. 2026;56(6):42223079. https://pubmed.ncbi.nlm.nih.gov/42223079/ ↩︎ ↩︎ ↩︎
Baena García A, Partida Palma F, García Martínez S, et al. (75)Se-Homocholic acid taurine scintigraphy ((75)SeHCAT(®)), a standard benchmark test in bile acid malabsorption? Revista Española de Medicina Nuclear e Imagen Molecular. 2019;38(5):297-303. https://pubmed.ncbi.nlm.nih.gov/30745130/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Atkins JS, Keevil BG, Taylor AE, et al. Development and validation of a novel 7α-hydroxy-4-cholesten-3-one (C4) liquid chromatography tandem mass spectrometry method and its utility to assess pre-analytical stability. Clinical Chemistry and Laboratory Medicine. 2025;63(2):39097844. https://pubmed.ncbi.nlm.nih.gov/39097844/ ↩︎ ↩︎ ↩︎ ↩︎
Masetto A, Leber T, Frömel T, et al. Towards routine high-throughput analysis of fecal bile acids: validation of an enzymatic cycling method for the quantification of total bile acids in human stool samples on fully automated clinical chemistry analyzers. Clinical Chemistry and Laboratory Medicine. 2025;63(1):39840591. https://pubmed.ncbi.nlm.nih.gov/39840591/ ↩︎ ↩︎ ↩︎