¶ Bloating
| Condition Class | Functional Bowel Disorder (FBD) |
| Primary Types | Bloating (Subjective) vs Distension (Objective) |
| Diagnostic Criteria | Rome IV (Functional Bloating/Distension) |
| Key Bio-Mechanisms | Abdominophrenic Dyssynergia, Visceral Sensation |
| First-Line Therapy | Low-FODMAP Diet, Biofeedback, Motility Agents |
| Prevalence | 15–30% of the general population |
Abdominal bloating (the subjective sensation of increased intra-abdominal pressure, gas, or fullness) and abdominal distension (the objective, visible increase in abdominal girth) are exceptionally common gastrointestinal complaints. Rather than being merely a consequence of "excess gas," functional bloating and distension are complex clinical entities driven by visceral hypersensitivity, impaired intestinal gas transit, dysbiosis, and neuromuscular dysregulation of the abdominal wall.
¶ TL;DR
- Bloating vs. Distension: Bloating is a subjective sensory symptom; distension is an objective, visible expansion of the abdomen. They often overlap but have distinct pathophysiological mechanisms.
- Neuromuscular Dysregulation is Key: Chronic distension is frequently mediated by abdominophrenic dyssynergia (paradoxical descent of the diaphragm and relaxation of the anterior abdominal wall in response to normal gas volumes).
- Dietary FODMAP Restriction is First-Line: Restricting fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAPs) highly effectively reduces gas production and osmotic water retention in the lumen.
- Biofeedback Targets the Core Muscle Defect: Diaphragmatic breathing and wall-motion-guided biofeedback are highly effective clinical therapies for restoring correct abdominophrenic coordination.
- Look for Under-recognized Organic Causes: Rule out small intestinal bacterial overgrowth (SIBO), celiac disease, exocrine pancreatic insufficiency, and pelvic floor dyssynergia before diagnosing functional bloating.
¶ Quick Answer
The clinical management of functional abdominal bloating and distension requires differentiating between a subjective excess of gas (bloating) and a muscular coordination failure (distension). While bloating is primarily addressed by limiting dietary fermentation (the Low-FODMAP diet) and managing visceral hypersensitivity (low-dose tricyclic antidepressants), visible abdominal distension requires retraining the somatic abdominal musculature. The principal mechanism behind functional distension is abdominophrenic dyssynergia: when a normal volume of gas enters the gut, the patient’s diaphragm paradoxically contracts and descends, while the anterior abdominal wall muscles relax and protrude. Effective therapy for this muscular coordination failure utilizes thoracoabdominal biofeedback and diaphragmatic breathing to retrain somatic muscle patterns.
¶ What It Is
Functional Abdominal Bloating and Distension (FABD) is classified as a distinct functional bowel disorder under the Rome IV criteria. It is defined by recurrent episodes of bloating or visible distension occurring at least one day per week, with symptoms predominating over other functional gastrointestinal symptoms (such as pain or bowel habit changes), and a duration of at least six months.
- Subjective Bloating: A transient or persistent feeling of abdominal fullness, pressure, or trapped gas.
- Objective Distension: Measurable, visible abdominal protrusion that typically worsens as the day progresses (diurnal variation) and resolves or improves overnight.
¶ Mechanism in 60 Seconds
FABD is rarely caused by an absolute excess of intestinal gas volume. Instead, the pathology involves three primary drivers:
- Impaired Gas Transit: Slowed transit or pooling of normal gas volumes in the small and large intestines.
- Visceral Hypersensitivity: Over-responsiveness of gut sensory nerves, causing normal physiological volumes of intestinal gas or liquid to be perceived as severe bloating or pressure.
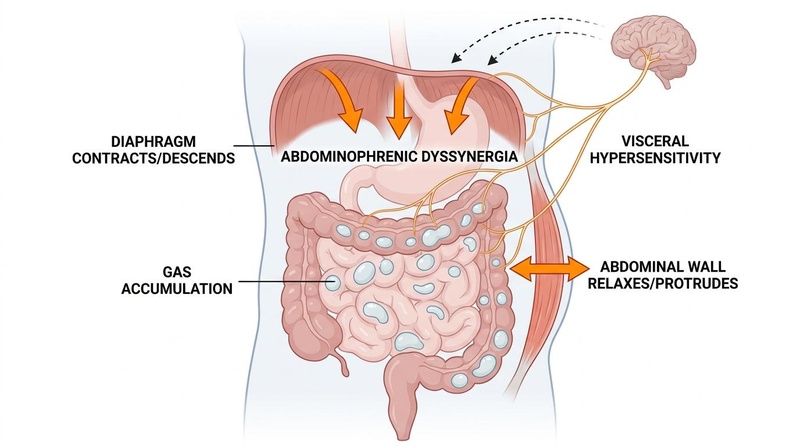
- Abdominophrenic Dyssynergia: A paradoxical reflex where the diaphragm contracts and moves downward, and the anterior abdominal wall muscles relax and protrude in response to gas, causing physical distension. In healthy individuals, the diaphragm normally relaxes (moves upward) and the abdominal wall contracts (pulls inward) to accommodate increased luminal volume without outward expansion.
¶ Does It Work? (Evidence Snapshot)
The efficacy of various therapeutic modalities in reducing functional bloating and objective abdominal distension has been quantified across multiple clinical trials.
¶ Primary Interventions for Functional Bloating & Distension
| Intervention | Primary Mechanism | Clinical Target | Expected Efficacy (Symptom Reduction) | Evidence Quality (GRADE) | Supported Study Count |
|---|---|---|---|---|---|
| Low-FODMAP Diet | Decreases osmotic fluid draw & colonic gas fermentation | Subjective Bloating & Gas Volume | 50–70% response rate (moderate-to-marked reduction) [1][2] | High | >30 RCTs, Meta-analyses |
| Thoracoabdominal Biofeedback | Retrains diaphragmatic ascent and anterior abdominal wall contraction | Visible Distension & Dyssynergia | reduction in visible abdominal girth [3] | Moderate-High | Multiple RCTs |
| Rifaximin | Suppresses gas-producing bacteria in the small bowel | Bloating (associated with IBS-D or SIBO) | 40% response rate (sustained benefit up to 10 weeks) [4] | Moderate-High | 3 Phase-III RCTs |
| Prokinetics (e.g., Prucalopride) | Accelerates colonic transit, preventing gas pooling | Bloating associated with constipation (IBS-C / CIC) | Significant decrease in daily bloating severity [5] | Moderate | >5 RCTs |
| Low-Dose Tricyclic Antidepressants | Neuromodulates visceral hypersensitivity pathways | Subjective Bloating / Pain | Significant reduction in subjective bloating scores [6] | Moderate | >10 RCTs |
| Simethicone | Coalesces gas bubbles to facilitate transit/elimination | Acute, transient gas/bloating | Mild, transient symptom relief (placebo-level in chronic FABD) [7] | Low | Multiple small trials |
¶ Who Benefits Most / Least
¶ Subgroup Variations
- Females: Females are disproportionately affected by FABD, reporting a 2-fold higher prevalence than males [8]. Progesterone fluctuations during the luteal phase delay gastrointestinal transit and increase visceral hypersensitivity, leading to cyclic exacerbations of bloating [9]. Females also exhibit a higher propensity for abdominophrenic dyssynergia, making them excellent candidates for biofeedback therapy.
- Patients with SIBO: Those presenting with hydrogen- or methane-producing SIBO experience profound gas production within 30–60 minutes of eating fermentable carbohydrates. These individuals benefit significantly from antimicrobial therapy (rifaximin) [4:1].
- Patients with Pelvic Floor Dysfunction: Individuals with pelvic floor dyssynergia (inability to relax the puborectalis muscle during defecation) experience severe retrograde fecal loading, leading to chronic colonic gas entrapment. These patients will not respond to simple dietary changes and require pelvic floor physical therapy.
¶ How to Try It: Actionable Protocols
¶ Step 1: Clinical Diagnosis & Rule-Outs
Confirm the patient meets the Rome IV criteria for Functional Bloating & Distension. To prevent diagnostic errors, exclude the following organic mimics:
- Celiac Disease: Check tTG-IgA and total IgA.
- Exocrine Pancreatic Insufficiency (EPI): Check fecal elastase ( indicates deficiency) [10].
- Active Gut Inflammation: Check fecal calprotectin ( to exclude IBD).
- SIBO: Perform a lactulose or glucose hydrogen-methane breath test [11].
¶ Step 2: First-Line Diet & Motility Baseline (4–6 Weeks)
If bloating is the predominant symptom (without severe visible distension):
- Low-FODMAP Diet:
- Soluble Fiber Addition:
- Introduce Partially Hydrolyzed Guar Gum (PHGG) at dissolved in water [12]. PHGG is highly water-soluble, slowly fermentable, and does not cause the rapid gas production associated with coarse bran.
- Alpha-Galactosidase Supplementation:
- For meals containing complex legumes or cruciferous vegetables, administer 300–600 units of oral alpha-galactosidase with the first bite to facilitate complex carbohydrate digestion.
¶ Step 3: Biofeedback Protocol for Visible Distension (Abdominophrenic Retraining)
If the patient exhibits visible, progressive daytime abdominal distension (indicative of abdominophrenic dyssynergia):

- Daily Diaphragmatic Breathing:
- Position the patient supine with one hand on the chest and one on the abdomen.
- Instruct the patient to inhale deeply through the nose for 4 seconds, ensuring only the abdomen rises (the chest must remain completely still, indicating diaphragmatic control).
- Exhale slowly through pursed lips for 6 seconds, pulling the abdominal wall gently inward.
- Perform this exercise for 10–15 minutes twice daily (specifically 20 minutes post-meals) to inhibit paradoxical diaphragmatic contraction.
- Clinical Biofeedback:
- Enroll the patient in a thoracoabdominal wall motion-guided biofeedback program using surface electromyography (EMG) or abdominal belt sensors [3:1][13]. This provides real-time visual feedback, teaching the patient to contract the intercostal/anterior abdominal muscles and relax the diaphragm during periods of fullness.
¶ Step 4: Pharmacological Escalation for Refractory Bloating
If symptoms persist despite dietary and biofeedback interventions:
- For Overlap with Constipation (IBS-C / CIC):
- Prucalopride (5-HT4 agonist): orally once daily at bedtime. This accelerates colonic transit, clearing trapped gas pockets [5:1].
- For Overlap with Diarrhea (IBS-D / SIBO):
- Rifaximin: orally three times daily for 14 days to suppress gas-producing hydrogen/methane microbiota [4:2].
- For Visceral Hypersensitivity:
- Low-dose Tricyclic Antidepressants (TCAs): Start Amitriptyline at orally at bedtime. Titrate up to if tolerated. (TCAs down-regulate gut-brain pain pathways and reduce subjective sensory bloating) [6:1].
¶ Safety, Interactions, Red Flags
¶ Who Should Avoid (Absolute Contraindications)
- Prucalopride: Contraindicated in patients with mechanical intestinal obstruction, bowel perforation, or severe inflammatory bowel disease.
- TCAs: Contraindicated in patients with a history of prolonged QT interval, severe cardiac arrhythmias, narrow-angle glaucoma, or severe urinary retention.
¶ Side Effects & Mitigation
- Prucalopride: Can cause transient headache, nausea, and abdominal cramping during the first 1–3 days of therapy. Mitigation: Start with a low dose of or for the first week before escalating to .
- TCAs: Drowsiness, dry mouth, and constipation. Mitigation: Administer strictly at bedtime. If constipation occurs, ensure adequate soluble fiber intake and hydration.
¶ "Red Flag" Symptoms (Invasive Pathology Screening)
Immediately suspend functional therapy and pursue diagnostic workup (e.g., CT scan, colonoscopy, gynecological ultrasound) if any of the following are detected:
- New-onset, progressive bloating in a postmenopausal female (highly indicative of ovarian cancer; requires immediate pelvic ultrasound and CA-125 serum marker evaluation) [7:1].
- Unintentional weight loss ( of body weight within 6 months).
- Early satiety or persistent vomiting.
- Iron deficiency anemia or occult blood in the stool.
- Persistent fever or night sweats.
- Ascites (fluid accumulation in the peritoneal cavity).
¶ Tracking & What “Good” Looks Like
¶ Objective Markers
- Abdominal Girth Measurement: Measured using a flexible tape measure at the level of the umbilicus at three specific times: immediately upon waking, 1 hour after lunch, and immediately before bedtime. Success is defined as maintaining a flat abdominal profile with of fluctuation throughout the day [14].
- Bowel Motility Markers: Achieving a consistent transit time of 12–36 hours (as assessed by a blue stool transit test or wireless motility capsule).
¶ Subjective Metrics
- Visual Analogue Scale (VAS) for Bloating: A 0–10 scale rating daily bloating severity. A clinically meaningful response is a -point reduction in average scores.
- Bowel satisfaction score: Tracked via daily log.
¶ Expected Timelines
- Low-FODMAP Diet: Reduction in subjective bloating and gas volume occurs within 7–14 days [1:2].
- Abdominophrenic Biofeedback: Reversal of paradoxical diaphragmatic descent and visible abdominal distension is typically achieved within 3–6 sessions of guided biofeedback combined with daily at-home practice [3:2].
- Prucalopride Therapy: Acceleration of colonic gas clearance is seen within 1 week of starting daily dosing.
¶ Common Mistakes & Myths
- The "Yogurt and Probiotics" Blunder: Patients often attempt to "cure" bloating by consuming high volumes of active-culture yogurt, kefir, or multi-strain probiotic capsules. Reality: In patients with impaired motility or SIBO, introducing highly active, fermentable dairy or massive doses of bacterial CFU () acts as "fuel for the fire," causing rapid gas production, severe distension, and worsened abdominal pain [11:1].
- The "Activated Charcoal" Fallacy: Many patients swallow high doses of activated charcoal capsules after meals to absorb gas. Reality: Systematic reviews have shown that activated charcoal is largely ineffective at binding intestinal gases (such as hydrogen and methane) in vivo, as these gases are rapidly absorbed into the bloodstream or passed before charcoal can exert any meaningful physical binding [7:2].
- The "Gluten Allergy" Misconception: Patients frequently assume that post-meal bloating is due to a non-celiac gluten sensitivity and eliminate gluten entirely. Reality: In the majority of these cases, the bloating is actually triggered by fructans—a highly fermentable oligosaccharide (FODMAP) found in wheat, barley, and rye—rather than the gluten protein itself [2:2].
¶ Decision Tree (Text-Based)
[Patient Presents with Chronic Abdominal Bloating / Distension]
|
Assess for "Red Flags" & Organic Mimics
(Postmenopausal female, weight loss, fever)
|
+-----------------------+-----------------------+
| |
[Red Flags Present] [No Red Flags Present]
| |
Pursue Pelvic Ultrasound, Determine Primary Phenotype
CA-125, CT Abdomen/Pelvis |
|
+-------------------------------+-------------------------------+
| |
[Subjective Bloating] [Visible Distension]
(Feeling of pressure, normal girth) (Visible protrusion, diurnal fluctuation)
| |
1. Low-FODMAP Diet 1. Diaphragmatic Breathing
2. Partially Hydrolyzed Guar Gum 2. Thoracoabdominal Biofeedback
3. Test for SIBO / Treat if positive 3. Optimize bowel transit (Prucalopride)
| |
+-------------------------------+-------------------------------+
|
[Persistent / Refractory Symptoms]
|
Initiate Visceral Neuromodulation
(Low-Dose TCA: Amitriptyline)
¶ Practical FAQ
Why does my bloating get significantly worse as the day goes on?
This classic diurnal pattern is driven by the gradual accumulation of intestinal gas and fluid from meals consumed throughout the day, combined with progressive muscle fatigue. As the day progresses, the anterior abdominal wall muscles tire, making them more susceptible to relaxing and protruding (abdominophrenic dyssynergia) in response to the normal mechanical load of digesting food.
Can food intolerances cause severe bloating without diarrhea?
Yes. Food intolerances, particularly those involving carbohydrate malabsorption (such as lactose, fructose, or sorbitol), do not always cause diarrhea. If the colon has a highly efficient water-absorption capacity, or if the predominant gut microbiota rapidly ferment the unabsorbed sugars into gases (hydrogen, carbon dioxide) rather than short-chain fatty acids, the patient will experience severe gas distension and bloating without any increase in stool liquid.
How does diaphragmatic breathing physically reduce abdominal distension?
When you perform diaphragmatic breathing, you consciously force the diaphragm to move upward during exhalation and regulate its downward travel during inhalation. This conscious motor control directly overrides the subconscious, paradoxical contraction of the diaphragm seen in abdominophrenic dyssynergia. By forcing the diaphragm upward, it expands the vertical capacity of the chest cavity, allowing the abdominal organs to move back into their correct anatomical position, which automatically pulls the protruding abdominal wall inward.
Is carbonated water bad for chronic bloating?
Yes. Carbonated beverages contain dissolved carbon dioxide gas (). When consumed, this gas is rapidly released in the stomach due to body temperature and stomach acid. While a portion of this gas is eliminated via eructation (belching), a significant volume passes through the pylorus into the small intestine. In patients with visceral hypersensitivity or impaired gas transit, this additional gas volume directly triggers luminal distension and severe subjective bloating.
Can SIBO cause bloating even if I eat a very clean, healthy diet?
Yes. In fact, patients with SIBO often report that eating a "clean, healthy" diet makes their bloating significantly worse. This is because standard healthy diets are exceptionally high in prebiotic fibers, raw vegetables, legumes, and fruits (which are rich in FODMAPs). If pathogenic bacteria have colonised the small intestine, they will rapidly ferment these high-quality prebiotic fibers, producing massive amounts of gas directly in the narrow lumen of the small bowel, causing intense pain and distension.
¶ Glossary
- Abdominophrenic Dyssynergia: A functional neuromuscular disorder characterized by paradoxical contraction (descent) of the diaphragm and simultaneous relaxation (protrusion) of the anterior abdominal wall muscles in response to luminal volume.
- Functional Abdominal Distension: An objective, measurable increase in abdominal girth that exhibits diurnal variation, typically absent in the morning and peak in the evening.
- Visceral Hypersensitivity: A state of heightened pain sensitivity in the internal organs, where normal physiological stretch, pressure, or chemical signals are processed by the central nervous system as painful or distressing.
- Thoracoabdominal Biofeedback: A clinical retraining therapy that uses physiological sensors to teach patients how to consciously coordinate diaphragmatic movement and abdominal wall contraction.
- Fructans: Polymers of fructose molecules found in wheat, onions, garlic, and artichokes, which cannot be digested by human enzymes and are rapidly fermented by colonic bacteria.
¶ Methods (Transparency)
This clinical guide is based on current consensus recommendations, clinical reviews, and randomized controlled trials evaluating functional bloating and distension up to July 2026.
- Search Strategy: Searched PubMed, Embase, and the Cochrane Library. Key search strings: "functional bloating", "abdominal distension", "abdominophrenic dyssynergia", "biofeedback distension", and "Low-FODMAP bloating".
- Inclusion Criteria: Guidelines from the European Society for Neurogastroenterology and Motility (ESNM), United European Gastroenterology (UEG), and the American Gastroenterological Association (AGA); randomized clinical trials evaluating biofeedback and dietary interventions.
- Evidence Grading: Interventions are evaluated and graded using the standard GRADE methodology.
¶ References
¶ Update Log
- July 2026: Comprehensively revised to integrate the European Consensus (ESNM/UEG) on functional bloating and abdominal distension, including updated biofeedback evidence.
- September 2023: Updated to include the AGA Clinical Practice Update recommendations for functional bloating.
Yang X, Shui X. Characteristics and clinical applicability of four dietary interventions for irritable bowel syndrome: A systematic review and meta-analysis. Clinical Nutrition. 2026;45(7):110-124. https://pubmed.ncbi.nlm.nih.gov/42160924/ ↩︎ ↩︎ ↩︎
Shiha MG, Buckle RL, Shaw CC, et al. Low FODMAP Diet versus Traditional Dietary Advice in Postprandial Functional Dyspepsia: A Randomized Clinical Trial. Clinical Gastroenterology and Hepatology. 2026;24(6):1220-1231. https://pubmed.ncbi.nlm.nih.gov/42297316/ ↩︎ ↩︎ ↩︎
Barba E, Livovsky DM, Accarino A, et al. Thoracoabdominal Wall Motion-Guided Biofeedback Treatment of Abdominal Distention: A Randomized Placebo-Controlled Trial. Gastroenterology. 2024;167(2):295-305. https://pubmed.ncbi.nlm.nih.gov/38467383/ ↩︎ ↩︎ ↩︎
Lacy BE, Pimentel M, Brenner DM, et al. ACG Clinical Guideline: Management of Irritable Bowel Syndrome. The American Journal of Gastroenterology. 2021;116(1):17-44. https://pubmed.ncbi.nlm.nih.gov/33315591/ ↩︎ ↩︎ ↩︎
Goyal O, Chowdhary R, Sehgal T, et al. Evolving prokinetic therapy: New targets and therapeutic opportunities in gastrointestinal motility disorders. World Journal of Gastrointestinal Pharmacology and Therapeutics. 2026;17(2):45-58. https://pubmed.ncbi.nlm.nih.gov/42273241/ ↩︎ ↩︎
Khasawneh M, Thakur ER, Goodoory VC, et al. Efficacy of gut-brain neuromodulators and brain-gut behaviour therapies for irritable bowel syndrome: systematic review and network meta-analysis. Gut. 2026;75(6):1122-1135. https://pubmed.ncbi.nlm.nih.gov/42362221/ ↩︎ ↩︎
Moshiree B, Drossman D, Shaukat A, et al. AGA Clinical Practice Update on Evaluation and Management of Belching, Abdominal Bloating, and Distention: Expert Review. Gastroenterology. 2023;165(3):791-800. https://pubmed.ncbi.nlm.nih.gov/37452811/ ↩︎ ↩︎ ↩︎
Melchior C, Hammer H, Bor S, et al. European Consensus on Functional Bloating and Abdominal Distension-An ESNM/UEG Recommendations for Clinical Management. United European Gastroenterology Journal. 2025;13(9):810-825. https://pubmed.ncbi.nlm.nih.gov/40844856/ ↩︎
Zadeh RGB, Roghani T, Gladin A, et al. Spinal-Related Musculoskeletal Determinants of Functional Abdominal Bloating and Distension: A Narrative Review. Health Science Reports. 2025;8(7):e2402. https://pubmed.ncbi.nlm.nih.gov/40636528/ ↩︎
Williams V, Funk S. Unique causes of exocrine pancreatic insufficiency: When to consider pancreatic enzyme supplementation: A narrative review. Nutrition in Clinical Practice. 2026;41(3):210-221. https://pubmed.ncbi.nlm.nih.gov/42319011/ ↩︎
Furqan A, Sultan MT, Khalid MU, et al. Small Intestinal Bacterial Overgrowth: Microbiome Dysregulation, Gut-Brain Axis Disruption, and Systemic Consequences. Molecular Nutrition & Food Research. 2026;70(7):e2500120. https://pubmed.ncbi.nlm.nih.gov/42378001/ ↩︎ ↩︎
Scarpellini E, Roselli F, Scarcella M, et al. Guar Gum, Partially Hydrolyzed Guar Gum, and Human Gut Health: A Narrative Review. Reviews on Recent Clinical Trials. 2026;21(2):98-107. https://pubmed.ncbi.nlm.nih.gov/42304914/ ↩︎
Damianos JA, Tomar SK, Azpiroz F. Abdominophrenic Dyssynergia: A Narrative Review. The American Journal of Gastroenterology. 2023;118(1):34-42. https://pubmed.ncbi.nlm.nih.gov/36191283/ ↩︎
Barba E, Burri E, Quiroga S, et al. Visible abdominal distension in functional gut disorders: Objective evaluation. Neurogastroenterology and Motility. 2023;35(2):e14498. https://pubmed.ncbi.nlm.nih.gov/36153798/ ↩︎