¶ Colorectal Cancer Screening
| Indication | Colorectal Neoplasia Detection & Prevention |
| Access | Clinician referral or primary care order |
| Dosing Sched | Modality-specific (1 to 10 years) |
| Safety Profile | Medium-Low |
| Key Marker | Fecal hemoglobin, dysplastic adenomas, colonic polyps |
| Est. Cost | $0-$4000 |
Colorectal cancer screening encompasses a diverse suite of non-invasive stool-based biomarker assays and direct optical visualization modalities designed to identify precancerous lesions and localized adenocarcinomas. Screening transitions a historically high-mortality malignancy into a highly preventable disease, with clinical evidence supporting its deployment in asymptomatic cohorts to reduce both cancer incidence and cause-specific mortality.
¶ At a Glance
- What people use it for: Detection of precancerous colorectal lesions (adenomas, sessile serrated polyps) and early-stage localized colorectal adenocarcinoma, transitioning what is often a high-mortality malignancy into a highly preventable disease [1][2].
- Does it work? Yes, though the degree of clinical benefit and real-world compliance varies by modality. While cohort and observational studies consistently support the effectiveness of screening in preventing colorectal cancer deaths, clinical trials continue to define exact long-term parameters for each approach.
- Colonoscopy (NordICC Trial): In the landmark NordICC trial, at 10-year follow-up, an invitation to a single screening colonoscopy significantly reduced the risk of colorectal cancer diagnosis (0.98% in the invited group vs. 1.20% in the usual-care group, RR 0.82; 95% CI, 0.70 to 0.93), but did not demonstrate a statistically significant reduction in colorectal cancer-related mortality (0.28% vs. 0.31%, RR 0.90; 95% CI, 0.64 to 1.16) [3]. Extended 13-year follow-up confirmed a significant reduction in colorectal cancer incidence (intention-to-screen RR 0.81 [95% CI, 0.71 to 0.90]; per-protocol RR 0.55 [95% CI, 0.33 to 0.81]), though the reduction in colorectal cancer-related mortality remained statistically non-significant (0.41% in the screening group vs. 0.47% in the no-screening group, RR 0.88; 95% CI, 0.68 to 1.08) [4].
- Fecal Immunochemical Test (FIT): Non-invasive stool-based screening programs utilizing the Fecal Immunochemical Test (FIT) are established as highly feasible and effective tools for population-based screening [1:1][5]. In the pragmatic COLONPREV trial, invitation to biennial FIT screening achieved higher screening participation and uptake compared to invitation to standard colonoscopy, confirming its feasibility in organized healthcare settings [6].
- Flexible Sigmoidoscopy: Other screening modalities, such as flexible sigmoidoscopy, have shown statistically significant reductions in colorectal cancer-specific mortality (24% reduction, RR 0.76; 95% CI, 0.70 to 0.82) and incidence (20% reduction, RR 0.80; 95% CI, 0.75 to 0.86) in large-scale randomized controlled trials [7].
- Key risks: Physical complications of invasive procedures (such as bleeding after polyp removal, with major bleeding occurring in 15 of 11,843 screened participants in the NordICC trial and no perforations or screening-related deaths reported within 30 days) and the varying sensitivities and specificities of different modalities [1:2][3:1].
- Verdict: Colorectal cancer screening is a highly effective clinical tool. Organized screening guidelines support starting at age 45 for average-risk individuals to optimize early detection and prevent disease progression [1:3][8]. High-risk genetic or inflammatory bowel disease cohorts should be referred to specialized surveillance pathways [9][10].
¶ Pathophysiology & Screening Modalities
¶ The Adenoma-Carcinoma Sequence
Most colorectal cancers develop through a multi-step process involving a series of histological, morphological, and genetic changes that accumulate over time [1:4][2:1]. This progression allows for the detection and removal of early-stage precancerous polyps before they become cancerous in average-risk individuals, leading to a substantial decrease in the incidence of colorectal cancer [1:5][2:2]. This developmental timeline provides a critical clinical opportunity for endoscopic detection and preventive polypectomy.
Most colon tumors develop through standard multistep histopathological progression [2:3]. Ongoing clinical and epidemiological research continues to investigate early-onset colorectal cancer, which has shown rising incidence and mortality in cohorts younger than 50 years, with the DIRECt international guidelines emphasizing the need for prompt risk stratification and symptom assessment in this cohort [11]. This progression can be influenced by chronic inflammatory pathways, particularly in patients with inflammatory bowel disease [9:1]. Colonic dysbiosis and bacterial toxins also play a role: the cycle inhibiting factor (CIF) toxin is associated with polyps or adenomas, and pks+ genetic elements appear to be predisposing factors for colorectal cancer, whereas Bacteroides fragilis toxin does not show an association with precancerous or cancerous lesions [12].
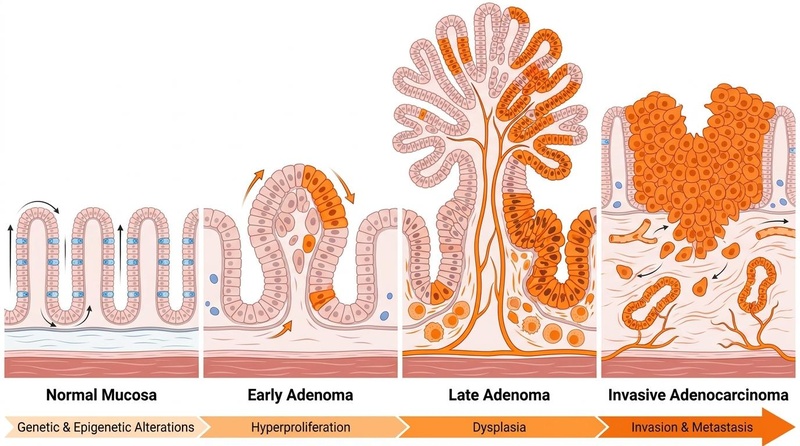
Figure 1: The Adenoma-Carcinoma Sequence. The progression of normal colorectal epithelium to invasive adenocarcinoma occurs over time, driven by sequential genetic alterations and histopathological progression.
¶ Non-Invasive Stool-Based Tests
Stool-based tests are performed at home, do not require direct endoscope insertion or prior bowel prep, and are designed to analyze stool samples for blood-derived biomarkers or neoplastic molecular elements.
- Fecal Immunochemical Test (FIT):
- Screening Interval: Every 1 to 2 years (fecal testing needs to be repeated every year or every other year as part of regular programmatic screening, and large-scale trials have demonstrated the feasibility of biennial screening) [1:6][6:1].
- Clinical Mechanism: Utilizes antibodies directed against human hemoglobin [5:1]. Dietary restrictions are not required prior to testing, as this modality does not cross-react with non-human hemoglobin or dietary components [1:7].
- Diagnostic Performance: A systematic review and meta-analysis of diagnostic accuracy for colorectal cancer (CRC) (Lee 2014) established that FIT has high overall diagnostic specificity (94% specificity) and moderate sensitivity (79% sensitivity) for detecting colorectal cancer in asymptomatic, average-risk adults, with diagnostic performance depending heavily on the specific assay cutoff value used for a positive test result [5:2].
- Follow-up Requirement: Any positive FIT result must be followed by a prompt diagnostic colonoscopy [6:2][13].
- Multi-Target Stool DNA (FIT-DNA or mt-sDNA, e.g., Cologuard):
- Screening Interval: Repeated at regular clinical intervals to detect molecular and genetic alterations associated with colorectal neoplasia progression [1:8][2:4].
- Clinical Mechanism: Combines a fecal immunochemical test with molecular assays to detect altered DNA biomarkers in the stool [1:9][2:5].
- Diagnostic Performance: Offers an alternative non-invasive screening method with distinct sensitivity and specificity profiles compared to standard FIT, designed to detect DNA biomarkers and molecular alterations associated with colorectal neoplasia [1:10][2:6].
- Follow-up Requirement: A positive FIT-DNA result must be followed by a diagnostic colonoscopy [1:11].
- Guaiac Fecal Occult Blood Test (gFOBT):
- Screening Interval: Every 1 to 2 years (fecal testing typically requires annual or biennial repetition to maintain clinical sensitivity) [1:12].
- Clinical Mechanism: An older chemical assay relying on the pseudoperoxidase activity of heme to turn guaiac-impregnated paper blue [1:13]. Unlike FIT, gFOBT is prone to interference from dietary pseudoperoxidases (e.g., red meat), vitamin C, and upper gastrointestinal bleeding, requiring dietary restrictions prior to testing [1:14].
- Diagnostic Performance & Follow-up: While randomized trials historically support gFOBT's capacity to reduce colorectal cancer mortality, clinical evidence and guidelines prefer FIT as a primary non-invasive option due to its high diagnostic specificity, lack of dietary constraints, and favorable performance characteristics [1:15][5:3][2:7]. A positive gFOBT necessitates immediate follow-up with diagnostic colonoscopy [1:16].
¶ Direct Visualization Modalities
Direct visualization modalities provide optical or radiographic evaluation of the colonic mucosa, enabling both diagnostic identification and immediate therapeutic intervention where applicable.
- Colonoscopy:
- Screening Interval: Endoscopic visualization is typically recommended at longer clinical intervals, with major randomized trials evaluating long-term outcomes at 10-year and 13-year points [3:2][4:1].
- Clinical Mechanism: Complete insertion of a flexible endoscope through the rectum to the cecum, enabling direct optical inspection of the entire colonic mucosa under conscious sedation or deep anesthesia [1:17]. Requires intensive dietary modification and oral osmotic or stimulant laxative preparation to clear all fecal matter [1:18].
- Diagnostic Performance: Standard direct visualization allows for immediate biopsy and therapeutic removal (polypectomy) of precancerous adenomas and serrated lesions [1:19][3:3]. In the NordICC trial, standard colonoscopy invitation significantly reduced long-term incidence of colorectal cancer at both 10-year follow-up (0.98% vs. 1.20%, RR 0.82; 95% CI, 0.70 to 0.93) [3:4] and 13-year follow-up (1.46% vs. 1.80%, RR 0.81 [95% CI, 0.71–0.90]) [4:2]. Efficacy can be optimized using high-definition systems or artificial intelligence (AI)-assisted computer-aided detection. In a multicenter randomized trial, AI-assisted colonoscopy significantly improved the overall adenoma detection rate (ADR) and advanced ADR compared to conventional colonoscopy [14].
- Follow-up Requirement: If findings are normal, the individual re-enters the screening pool in 10 years [1:20]. If polyps are detected and resected, follow-up is guided by post-polypectomy surveillance intervals (such as the US MSTF / ACS guidelines) [15].
- Flexible Sigmoidoscopy:
- Screening Interval: Endoscopy is typically recommended with longer clinical intervals, such as every 5 to 10 years [1:21].
- Clinical Mechanism: Endoscopic inspection of the distal colon (rectum, sigmoid, and descending colon) only, typically performed without sedation and requiring less intensive bowel prep than colonoscopy [1:22][7:1].
- Diagnostic Performance: A meta-analysis of four large randomized trials demonstrated that flexible sigmoidoscopy-based screening significantly reduced distal colorectal cancer incidence by 32% (RR 0.68) and distal cancer-specific mortality by 36% (RR 0.64), but had no significant protective effect on proximal colon lesions [7:2].
- Follow-up Requirement: Detection of an advanced adenoma (≥10 mm, high-grade dysplasia, or villous features) or multiple polyps during flexible sigmoidoscopy necessitates referral for a complete diagnostic colonoscopy to evaluate the proximal colon [1:23].
- Computed Tomography Colonography (CTC or Virtual Colonoscopy):
- Screening Interval: Performed at regular intervals as an alternative radiographic visualization option [2:8].
- Clinical Mechanism: Minimally invasive, radiographic (CT-based) examination of the entire colon following bowel preparation and mechanical insufflation of air or carbon dioxide to distend the bowel wall [1:24]. Generates high-resolution 2D and 3D mucosal reconstructions [1:25].
- Diagnostic Performance & Follow-up: Highly accurate for detecting larger polyps, but less sensitive for flat, serrated, or smaller lesions [1:26]. Requires subsequent follow-up with diagnostic colonoscopy if any positive findings or lesions are identified [1:27].
¶ Emerging Screening Modalities
Research continues into novel, minimally invasive modalities:
- Methylated SEPT9 Blood Test (Epi proColon): This FDA-approved blood-based screening test may serve to increase participation and adherence rates for colorectal cancer screening [16].
- Urinary Volatile Organic Compounds (VOCs): This paradigm analyzes gaseous chemical compounds in urine that are altered by metabolic shifts [17]. In a systematic review and meta-analysis of 16 studies, urinary VOCs demonstrated a strong potential to discriminate colorectal cancer from controls, presenting a completely non-invasive screening avenue [17:1].
¶ Eligibility & Screening Protocols
¶ Average-Risk Screening Guidelines
For average-risk individuals—defined as those without a personal history of colorectal neoplasia, inflammatory bowel disease, or hereditary colorectal cancer syndromes—guidelines emphasize starting screening early to optimize outcomes.
- Age of Initiation: Average-risk screening is initiated starting at age 45, which is supported by evidence of rising early-onset disease incidence and screening uptake evaluations in this younger cohort [1:28][8:1].
- Age to Discontinue: Routine screening is continued through age 75, after which the clinical utility of ongoing screening shifts based on individual comorbidities, prior screening history, and remaining life expectancy [1:29].
- Screening Modality Choice: A variety of screening options exist, including direct visualization methods and non-invasive stool-based tests [1:30]. The most effective screening test remains the one that is completed and adhered to by the patient [18].
¶ USPSTF (2021) Average-Risk Screening Guidelines
The primary, highly authoritative guidelines from the US Preventive Services Task Force (USPSTF) define a clear screening framework for asymptomatic individuals at average risk of colorectal cancer [1:31]:
- Age 45 to 49 years: Screening is recommended with moderate certainty to provide a moderate net benefit (Grade B recommendation) [1:32].
- Age 50 to 75 years: Screening is recommended with high certainty to provide a substantial net benefit (Grade A recommendation) [1:33].
- Age 76 to 85 years: Screening is offered selectively based on the patient's overall health, prior screening history, and individual preferences, as the net benefit is overall small (Grade C recommendation) [1:34].
¶ Modality Screening Intervals and Characteristics
Clinical options for colorectal cancer screening are characterized by distinct testing frequencies and evidence characteristics, with fecal testing requiring frequent repetition and endoscopy recommended at extended intervals [1:35].
| Modality Category | Specific Screening Modality | Interval Frequency [1:36][6:3][19] | Primary Clinical Endpoint / Performance [5:4][7:3] |
|---|---|---|---|
| Endoscopy | Colonoscopy | Every 10 years | Direct visualization of entire colon; enables immediate polypectomy and biopsy [3:5]. |
| Endoscopy | Flexible Sigmoidoscopy | Every 5 to 10 years | Direct visualization of distal colon; significantly reduces distal incidence and mortality [7:4]. |
| Fecal / Stool Test | Fecal Immunochemical Test (FIT) | Every 1 to 2 years | High diagnostic specificity (94%) and moderate sensitivity (79%) for colorectal cancer detection [5:5]. |
| Fecal / Stool Test | Guaiac Fecal Occult Blood Test (gFOBT) | Every 1 to 2 years | Chemical detection of heme; historically reduces mortality but susceptible to dietary interference [5:6]. |
¶ High-Risk & Hereditary Screening Pathways
Patients at elevated risk due to genetic, familial, or inflammatory conditions require specialized screening and surveillance protocols.
- Hereditary Syndromes (Lynch Syndrome & FAP): Individuals with hereditary colorectal cancer risk, such as Lynch syndrome or Familial Adenomatous Polyposis (FAP), undergo targeted risk-reducing interventions [10:1]. These clinical pathways incorporate specialized endoscopic surveillance, preventative surgery, and chemoprevention based on phenotypic and genetic diagnosis [10:2].
- Family History of Colorectal Cancer: A family history of colorectal cancer represents a major heritable risk factor [10:3]. Guidelines suggest that individuals with a significant family history of colorectal cancer should undergo earlier, more frequent colonoscopic screening compared to average-risk populations [10:4].
- Inflammatory Bowel Disease (IBD): Patients with long-standing colitis (ulcerative colitis or Crohn's disease) carry an increased risk of advanced colorectal neoplasia [9:2]. Key risk factors include extensive anatomical disease, severe histologic inflammation, and primary sclerosing cholangitis, with colonoscopic surveillance acting as a critical protective factor [9:3]. For surveillance, high-definition dye-based chromoendoscopy (HD-DCE) has demonstrated potential to detect more dysplastic lesions compared with standard high-definition white light endoscopy [20].
- Cystic Fibrosis (CF): Adult patients with cystic fibrosis have a significantly elevated risk of developing colorectal cancer compared to the general population, with organ transplant recipients experiencing an even greater risk under immunosuppressive therapy, necessitating specialized clinical attention and proactive screening strategies [21].
- Post-Resection Surveillance: Surveillance after surgical resection of colorectal cancer involves clearing synchronous neoplasia perioperatively, followed by a colonoscopy at 1 year, and then every 3 to 5 years if findings are normal [22].
¶ Benefits of Screening
The clinical value of colorectal cancer screening is demonstrated by its unique dual impact: detecting early-stage, curable malignancies and directly preventing cancer through the excision of precancerous polyps.
¶ Evidence from Large-Scale Randomized Trials
Large-scale randomized controlled trials (RCTs) provide high-certainty evidence for the clinical benefits of colorectal cancer screening.
- Non-Invasive Screening Efficacy: Stool-based tests, such as FIT, are widely implemented in population screening programs as highly feasible and effective tools [1:37][5:7]. Large-scale pragmatic studies, such as the COLONPREV trial, highlight that inviting populations to biennial FIT screening achieves significantly higher initial participation and uptake compared to inviting them to a single screening colonoscopy [6:4].
- The NordICC Trial (Colonoscopy):
- 10-Year Outcomes (Bretthauer 2022): In a population-based randomized trial involving healthy adults aged 55 to 64, an invitation to a single screening colonoscopy was compared to usual care [3:6]. In intention-to-screen analyses, the risk of being diagnosed with colorectal cancer at 10 years was significantly lower in the invited group, representing an 18% relative risk reduction (0.98% in the invited group vs. 1.20% in the usual-care group, RR 0.82; 95% confidence interval [CI], 0.70 to 0.93) [3:7]. However, there was no statistically significant difference in colorectal cancer-specific mortality (0.28% in the invited group vs. 0.31% in the usual-care group, RR 0.90; 95% CI, 0.64 to 1.16) or all-cause mortality (11.03% vs. 11.04%, RR 0.99; 95% CI, 0.96 to 1.04) at 10 years [3:8].
- 13-Year Outcomes (Kaminski 2026): Extended 13-year follow-up confirmed that a single colonoscopy screening significantly reduced colorectal cancer incidence, with intention-to-screen analysis showing a significant reduction in colorectal cancer risk (1.46% in the screening group vs. 1.80% in the no-screening group, RR 0.81 [95% CI, 0.71–0.90]) and per-protocol analysis demonstrating a 45% reduction in colorectal cancer risk (RR 0.55 [95% CI, 0.33–0.81]) [4:3]. However, the reduction in colorectal cancer-specific mortality remained statistically non-significant in both the intention-to-screen analysis (0.41% vs. 0.47%, RR 0.88; 95% CI, 0.68 to 1.08) and per-protocol analysis (RR 0.70; 95% CI, 0.26 to 1.25) [4:4].
- The COLONPREV Trial (FIT vs. Colonoscopy): This pragmatic, randomized, controlled trial across 15 tertiary hospitals in Spain assigned 57,404 healthy individuals aged 50–69 to receive an invitation for one-time colonoscopy or biennial faecal immunochemical test before invitation to screening [6:5]. In the intention-to-screen population, participation in any form of screening was higher among individuals invited to fecal immunochemical test screening than colonoscopy screening, demonstrating high feasibility and uptake [6:6].
- Flexible Sigmoidoscopy Trials: A meta-analysis of four large randomized trials demonstrated that flexible sigmoidoscopy-based screening significantly reduced both colorectal cancer incidence (20% reduction, RR 0.80) and cancer-specific mortality (24% reduction, RR 0.76) [7:5]. Efficacy was highly pronounced for distal colorectal cancer (incidence RR 0.68; mortality RR 0.64), whereas no significant effect was observed for proximal colon cancer [7:6].
¶ Harms & Clinical Uncertainties
A balanced clinical assessment requires understanding the physical, diagnostic, and systemic risks associated with screening interventions.
- Procedural Complications: Invasive procedures such as colonoscopy carry physical risks, including bleeding after polyp removal and other procedural injuries, though major complications remain relatively rare in large clinical trials [1:38][3:9].
- Diagnostic Limitations of Stool-Based Tests: Stool-based tests exhibit varying sensitivity and specificity [1:39][5:8]. Positive results are not diagnostic of cancer and require a follow-up diagnostic colonoscopy to investigate for lesions, which may expose the patient to further procedural risks [1:40].
- Uptake and Adherence Barriers: A significant proportion of eligible patients do not complete screening as recommended [1:41]. Screen participation can vary based on the specific screening tests offered, recruitment methods, and patient-level characteristics [23][24]. Behavioral interventions, including reminders, patient navigation, and targeted paper materials, can significantly increase screening uptake and participation [25].
- Shifting Benefit-to-Harm Ratio in Older Adults: As patients age, the risk-to-benefit ratio of ongoing screening begins to shift [1:42]. With increasing comorbidities and decreasing life expectancy, the future potential benefits of colorectal cancer prevention become less robust, while the risk for screening-related complications grows [1:43]. Consequently, rigid age cutoffs are insufficient, and screening decisions must be tailored to the individual's physiological health [1:44].
¶ Shared Decision Making
Colorectal cancer screening decisions in older cohorts require a transition from standard age-based mandates to individualized shared decision-making.
- Routine Stopping Point: Clinical consensus supports evaluating a stopping point around age 75, as the risk-to-benefit ratio of ongoing screening begins to shift with advanced age [1:45].
- Individualized Clinical Approach for Older Adults: Screening decisions for older cohorts should be individualized based on physiological age and shared clinical discussion rather than strict chronological limits [1:46]. Key considerations include:
- Comorbidities & Life Expectancy: As comorbidities increase and life expectancy decreases, the future preventative benefits of screening become less robust, and the risks of procedural complications grow [1:47].
- Prior Screening History: A patient's prior screening history significantly impacts their clinical trajectory, as those who have never been screened stand to benefit most, whereas consistently screened patients have a much lower likelihood of harboring advanced neoplasia [1:48].
¶ Clinical Red Flags
Screening protocols are strictly indicated for asymptomatic individuals. The presence of specific signs or symptoms shifts the clinical pathway from screening to immediate diagnostic evaluation [1:49][26].
- Diagnostic vs. Screening Pathways: Clinical evidence highlights a clear distinction between screening and diagnostic routes. Screening programs in asymptomatic average-risk populations significantly increase the likelihood of early-stage diagnosis compared to evaluating patients after symptoms have developed [13:1]. Patients who present after developing symptoms (such as hematochezia or changes in bowel habits) are more likely to have left-sided lesions and a more advanced stage at diagnosis, highlighting the prevention and early-detection benefits of organized screening [13:2].
- Red Flag Signs and Symptoms: Early-onset colorectal cancer (EOCRC) can present with red flag signs and symptoms that are frequently missed, leading to significant diagnostic delays [26:1]. Key clinical presentations include hematochezia, abdominal pain, and altered bowel habits, which necessitate urgent diagnostic follow-up [26:2].
¶ Evidence Summary Table (human outcomes)
| Outcome | Effect | Quality | Consistency | Trials | Notes |
|---|---|---|---|---|---|
| Colorectal Cancer Mortality (General Screening) | High | High | Systematic Reviews | Screening average-risk populations allows for early detection of precancerous lesions and localized colorectal adenocarcinoma, significantly reducing colorectal cancer-specific mortality across population-based programs [1:50][7:7]. | |
| Colorectal Cancer Incidence (Colonoscopy) | High | High | RCTs & Cohorts | In the NordICC trial, one-time screening colonoscopy invitation significantly reduced long-term incidence of colorectal cancer at both 10-year follow-up (0.98% vs. 1.20%, RR 0.82; 95% CI, 0.70 to 0.93) [3:10] and 13-year follow-up (1.46% vs. 1.80%, RR 0.81 [95% CI, 0.71–0.90]) [4:5]. | |
| Screening Participation and Uptake (FIT vs. Colonoscopy) | High | High | Pragmatic RCT | Stool-based testing utilizing FIT achieves significantly higher population participation and adherence rates compared to inviting individuals to a screening colonoscopy [6:7]. | |
| Distal Colorectal Cancer Mortality (Flexible Sigmoidoscopy) | High | High | 4 RCTs | Flexible sigmoidoscopy-based screening significantly reduced distal colorectal cancer mortality (RR 0.64), but showed no significant effect on proximal colon cancer mortality in a meta-analysis of randomized trials [7:8]. | |
| Distal Colorectal Cancer Incidence (Flexible Sigmoidoscopy) | High | High | 4 RCTs | Sigmoidoscopy screening significantly reduced distal colorectal cancer incidence (RR 0.68), with no significant effect on proximal colon cancer in a meta-analysis of randomized trials [7:9]. | |
| Diagnostic Accuracy for Colorectal Cancer (CRC) (Fecal Immunochemical Test - FIT) | High | High | 19 Studies | A systematic review (Lee 2014) showed FIT has moderate sensitivity (79% sensitivity) and high specificity (94% specificity) for colorectal cancer, with sensitivity improving at lower positive threshold cutoff values [5:9]. | |
| Diagnostic Yield of AI-Assisted Colonoscopy | Moderate | High | Multicenter RCT | AI-assisted colonoscopy significantly improved the overall adenoma detection rate (ADR) compared to conventional colonoscopy in a multicenter randomized trial (Xu 2023) [14:1]. |
- *Effect: Compact renderer encoding:
[direction][magnitude][impact]where direction isu(up),d(down),e(equal), orq(uncertain); magnitude is0to3; and impact isp(positive),n(negative), orx(neutral). - **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- ***Trials: Number of RCTs or total trials informing this outcome (shows evidence depth at a glance)
¶ Clinician-Discussion Checklist & Actionable Next Steps
¶ Pre-Procedure Checklist
- Assess Patient Risk Profile: Stratify the patient into average-risk or high-risk (family history, genetic syndrome, long-standing colitis, cystic fibrosis) to determine the appropriate age of initiation and modality [1:51][10:5][21:1].
- Review Modality Preferences: Utilize shared decision-making to compare the benefits and burdens of direct visualization (longer-interval endoscopy) vs. non-invasive repeated fecal testing (annual or biennial FIT) [1:52][6:8].
- Bowel Preparation Quality: Perform a high-quality baseline colonoscopy with excellent patient preparation and adequate endoscopist withdrawal time to minimize the risk of missed lesions [15:1].
¶ Post-Polypectomy & Post-Resection Surveillance Guidelines
Follow-up and surveillance intervals after colonoscopy and polypectomy are determined based on baseline pathological findings, specifically incorporating the number, size, and histological features of baseline polyps [15:2]. Under standard clinical risk-stratification models, individuals with low-risk baseline findings can safely undergo extended-interval surveillance [15:3]. Conversely, patients with high-risk baseline findings require more frequent, shorter-interval surveillance to mitigate the long-term risk of metachronous advanced neoplasia [15:4].
The US Multi-Society Task Force on Colorectal Cancer and the American Cancer Society (Winawer 2006) define risk-adapted surveillance intervals following a high-quality baseline colonoscopy with complete resection of all lesions [15:5]:
| Baseline Colonoscopy Finding | Recommended Surveillance Interval | Clinical Rationale & Risk Classification [15:6] |
|---|---|---|
| Normal colonoscopy (no polyps detected) | 10 years | Average-risk baseline; standard screening interval. |
| Hyperplastic polyps only | 10 years | Non-neoplastic lesions; managed similarly to average-risk screening. |
| 1–2 small (<10 mm) tubular adenomas (with low-grade dysplasia) | 5 to 10 years | Low-risk cohort; long-term risk is minimal. |
| 3 or more tubular adenomas | 3 years | High-risk cohort; higher adenoma burden. |
| Adenoma ≥10 mm in size | 3 years | High-risk cohort; large size is a key predictor of metachronous advanced neoplasia. |
| Adenoma with villous / tubulovillous features | 3 years | High-risk cohort; advanced histology indicates higher malignant potential. |
| Adenoma with high-grade dysplasia (HGD) | 3 years | High-risk cohort; severe cellular atypia indicates high oncogenic risk. |
¶ Colonoscopy Surveillance After Cancer Resection
For patients undergoing curative surgical resection of colorectal cancer, surveillance protocols are designed to detect local recurrence and metachronous lesions [22:1]:
| Surveillance Phase | Recommended Timing | Clinical Rationale [22:2] |
|---|---|---|
| Perioperative Clearance | Preoperatively (or 3 to 6 months postoperatively if obstructed) | To clear the colorectum of any synchronous neoplasia. |
| First Post-Resection Exam | 1 year after resection | Based on high incidence of metachronous second cancers in the first 2 years. |
| Second Post-Resection Exam | 3 years after the 1-year exam (if 1-year exam was normal) | Intermediate surveillance phase. |
| Subsequent Exams | Every 5 years (if previous exams were normal) | Long-term surveillance phase; shorter intervals if adenomas are found. |
¶ FAQ
¶ Is a positive FIT result a definitive diagnosis of colorectal cancer?
No. A positive fecal immunochemical test (FIT) indicates the presence of blood in the stool, which can be caused by benign conditions such as hemorrhoids, anal fissures, diverticular disease, or inflammatory bowel disease. However, because it is also a key biomarker for bleeding, a positive FIT requires a follow-up colonoscopy [^3].
¶ Why has the recommended age to start screening decreased from 50 to 45?
Epidemiological evidence shows rising trends in early-onset colorectal cancer (EOCRC). Modeling and clinical evaluations support starting screening at age 45 for average-risk individuals, as initiating screening at this age has been shown to yield a favorable balance of benefits and risks [^1][^21].
¶ Can virtual colonoscopy (CT colonography) replace standard colonoscopy?
CT colonography (virtual colonoscopy) represents an alternative diagnostic imaging technique for colorectal screening [^1]. However, standard colonoscopy provides direct optical inspection of the entire colonic mucosa and immediate therapeutic capacity for biopsy and polypectomy, making it a primary modality [^1], whereas any positive findings on a CT colonography require subsequent follow-up with diagnostic colonoscopy.
¶ How do the screening recommendations change for individuals with inflammatory bowel disease (IBD)?
Patients with long-standing colitis (such as [ulcerative colitis](/pages/ulcerative-colitis.md) or [Crohn's disease](/pages/crohns-disease.md)) have an increased risk of advanced colorectal neoplasia, requiring regular colonoscopic surveillance as a protective factor [^10]. Surveillance using high-definition dye-based chromoendoscopy (HD-DCE) has shown potential to detect more dysplastic lesions compared with standard high-definition white light endoscopy [^12].
¶ References
US Preventive Services Task Force. Screening for Colorectal Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2021. https://pubmed.ncbi.nlm.nih.gov/34003218 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Simon K. Colorectal cancer development and advances in screening. Clinical interventions in aging. 2016. https://pubmed.ncbi.nlm.nih.gov/27486317 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bretthauer M, Løberg M, Wieszczy P. Effect of Colonoscopy Screening on Risks of Colorectal Cancer and Related Death. NEJM. 2022. https://pubmed.ncbi.nlm.nih.gov/36214590 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kaminski MF, Kalager M, Løberg M. Long-term effects of colonoscopy screening on colorectal cancer incidence and mortality: a multicountry, population-based randomised controlled trial. Lancet. 2026. https://pubmed.ncbi.nlm.nih.gov/42102826 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lee JK, Liles EG, Bent S. Accuracy of fecal immunochemical tests for colorectal cancer: systematic review and meta-analysis. Annals of internal medicine. 2014. https://pubmed.ncbi.nlm.nih.gov/24658694 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Castells A, Quintero E, Bujanda L. Effect of invitation to colonoscopy versus faecal immunochemical test screening on colorectal cancer mortality (COLONPREV): a pragmatic, randomised, controlled, non-inferiority trial. Lancet. 2025. https://pubmed.ncbi.nlm.nih.gov/40158525 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zhang C, Liu L, Li J. Effect of flexible sigmoidoscopy-based screening on colorectal cancer incidence and mortality: an updated systematic review and meta-analysis of randomized controlled trials. Expert review of anticancer therapy. 2023. https://pubmed.ncbi.nlm.nih.gov/37542427 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chen KL, Mangione CM, Shih YT. Unmet social needs and colorectal cancer testing at 45-49 since the 2021 USPSTF recommendation. Journal of the National Cancer Institute. 2026. https://pubmed.ncbi.nlm.nih.gov/41206948 ↩︎ ↩︎
Wijnands AM, de Jong ME, Lutgens MWMD. Prognostic Factors for Advanced Colorectal Neoplasia in Inflammatory Bowel Disease: Systematic Review and Meta-analysis. Gastroenterology. 2021. https://pubmed.ncbi.nlm.nih.gov/33385426 ↩︎ ↩︎ ↩︎ ↩︎
Monahan KJ, Bradshaw N, Dolwani S. Guidelines for the management of hereditary colorectal cancer from the British Society of Gastroenterology (BSG)/Association of Coloproctology of Great Britain and Ireland (ACPGBI)/United Kingdom Cancer Genetics Group (UKCGG). Gut. 2020. https://pubmed.ncbi.nlm.nih.gov/31780574 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Cavestro GM, Mannucci A, Balaguer F. Delphi Initiative for Early-Onset Colorectal Cancer (DIRECt) International Management Guidelines. Clinical gastroenterology and hepatology. 2023. https://pubmed.ncbi.nlm.nih.gov/36549470 ↩︎
Piciocchi A, Germinario EAP, Garcia Etxebarria K. Association of Polygenic Risk Score and Bacterial Toxins at Screening Colonoscopy with Colorectal Cancer Progression: A Multicenter Case-Control Study. Toxins. 2021. https://pubmed.ncbi.nlm.nih.gov/34437440 ↩︎
Flynn DJ, Feuerstein JD. Colon cancer screening programs prevent cancer. World journal of gastroenterology. 2024. https://pubmed.ncbi.nlm.nih.gov/39563750 ↩︎ ↩︎ ↩︎
Xu H, Tang RSY, Lam TYT. Artificial Intelligence-Assisted Colonoscopy for Colorectal Cancer Screening: A Multicenter Randomized Controlled Trial. Clinical gastroenterology and hepatology. 2023. https://pubmed.ncbi.nlm.nih.gov/35863686 ↩︎ ↩︎
Winawer SJ, Zauber AG, Fletcher RD. Guidelines for colonoscopy surveillance after polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer and the American Cancer Society. Gastroenterology. 2006. https://pubmed.ncbi.nlm.nih.gov/16697750 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Issa IA, Noureddine M. Colorectal cancer screening: An updated review of the available options. World journal of gastroenterology. 2017. https://pubmed.ncbi.nlm.nih.gov/28811705 ↩︎
van Liere ELSA, van Dijk LJ, Bosch S. Urinary volatile organic compounds for colorectal cancer screening: A systematic review and meta-analysis. European journal of cancer. 2023. https://pubmed.ncbi.nlm.nih.gov/37030079 ↩︎ ↩︎
Han A, Maratt J, Kahi C. Colorectal Cancer Screening Decisions in the Opportunistic Setting. Gastrointestinal endoscopy clinics of North America. 2020. https://pubmed.ncbi.nlm.nih.gov/32439079 ↩︎
Bretthauer M, Wieszczy P, Løberg M. Estimated Lifetime Gained With Cancer Screening Tests: A Meta-Analysis of Randomized Clinical Trials. JAMA internal medicine. 2023. https://pubmed.ncbi.nlm.nih.gov/37639247 ↩︎
Sinopoulou V, Nigam GB, Gordon M. Comparative Efficacy and Safety of Endoscopic Modalities for Colorectal Cancer Screening in Inflammatory Bowel Disease: A Systematic Review and Network Meta-analysis. Clinical gastroenterology and hepatology. 2025. https://pubmed.ncbi.nlm.nih.gov/39675405 ↩︎
Hadjiliadis D, Khoruts A, Zauber AG. Cystic Fibrosis Colorectal Cancer Screening Consensus Recommendations. Gastroenterology. 2018. https://pubmed.ncbi.nlm.nih.gov/29289528 ↩︎ ↩︎
Rex DK, Kahi CJ, Levin B. Guidelines for colonoscopy surveillance after cancer resection: a consensus update by the American Cancer Society and the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2006. https://pubmed.ncbi.nlm.nih.gov/16697749 ↩︎ ↩︎ ↩︎
Bresalier RS. Colorectal Cancer Screening in a Changing World. Gastroenterology clinics of North America. 2022. https://pubmed.ncbi.nlm.nih.gov/36153111 ↩︎
Wu W, Huang J, Yang Y. Adherence to colonoscopy in cascade screening of colorectal cancer: A systematic review and meta-analysis. Journal of gastroenterology and hepatology. 2022. https://pubmed.ncbi.nlm.nih.gov/34907588 ↩︎
Tsipa A, O'Connor DB, Branley-Bell D. Promoting colorectal cancer screening: a systematic review and meta-analysis of randomised controlled trials of interventions to increase uptake. Health psychology review. 2021. https://pubmed.ncbi.nlm.nih.gov/32401175 ↩︎
Demb J, Kolb JM, Dounel J. Red Flag Signs and Symptoms for Patients With Early-Onset Colorectal Cancer: A Systematic Review and Meta-Analysis. JAMA network open. 2024. https://pubmed.ncbi.nlm.nih.gov/38787555 ↩︎ ↩︎ ↩︎