¶ Community and Longevity: The Science of Social Integration
¶ At a Glance
¶ Overview
Social integration—the structural and functional connection of an individual to a broader social network—is a premier predictor of human healthspan and lifespan. Far from a subjective "soft" lifestyle factor, your level of social integration acts as a direct biological regulator of systemic inflammation, immune function, and neuroendocrine output.
¶ Safety "Traffic Light"
- Green Light: Actively participating in structured civic, local, or recreational groups; maintaining regular face-to-face contact with diverse age groups.
- Yellow Light: Experiencing major life transitions (retirement, relocation, bereavement) that disrupt structural social roles; high reliance on digital-only communities.
- Red Light: Objective isolation (living alone with fewer than 3 social contacts per week); high-conflict community engagement that triggers chronic, non-resolving stress.
¶ Protocol Card
| Parameter | Minimum Target | Optimal Protocol | Clinical Outcome |
|---|---|---|---|
| Structural Integration | ≥2 distinct social groups | 3-4 diverse groups (e.g., civic, athletic, intellectual, neighborhood) | Up to 50% increase in survival probability |
| Generational Diversity | ≥1 intergenerational interaction/week | Structured mentorship or intergenerational project | Delayed cognitive decline, improved brain volume retention |
| Functional Contact | Face-to-face interaction twice weekly | Daily micro-connections (local merchants, peers, colleagues) | Downregulated systemic inflammation (CRP/IL-6) |
¶ Bottom Line
Strong structural social integration is prospectively associated with a 50% reduction in all-cause mortality risk, a biological effect size that exceeds the health benefits of smoking cessation, regular cardiovascular exercise, and maintaining an optimal body mass index (BMI).
¶ The Contextual Narrative
¶ The "Why" (Health Outcomes)
Humans are obligate collaborative breeders; our physiology expects a baseline density of reliable social feedback. When this structural feedback is absent, the brain interprets the environment as inherently hostile, initiating a persistent, systemic threat response. Clinical trials show that high levels of social integration modulate our biology in three main ways:
- Dampening Chronic Inflammation: Socially integrated individuals show lower circulating concentrations of C-reactive protein (CRP) and Interleukin-6 (IL-6)[1].
- Enhancing Viral Defense: High integration downregulates pro-inflammatory gene expression while simultaneously upregulating antiviral type-1 interferon pathways[2].
- Preserving Brain Volume: Active participation in complex community roles buffers against age-related prefrontal and frontostriatal brain tissue loss, preserving executive function in later life[3].
¶ Reality Check: Mouse Hopes vs. Human Results
In rodent models of aging, social isolation is induced through single-cage isolation, showing rapid increases in corticosterone, oxidative stress, and accelerated tumor progression. However, translating this to human biology requires caution. Humans do not live in controlled laboratory cages; subjective loneliness (perceived isolation) can occur in densely populated cities, while objective isolation (living alone) is highly mediated by individual personality traits (introversion vs. extraversion) and socioeconomic status. While animal data clearly isolates the cellular damage of physical separation, human epidemiology indicates that the structural architecture of your social environment (your functional roles, civic duties, and daily interactions) is what governs long-term clinical survival[4].
¶ Commercial & Built-Environment Context
Modern society has commodified connection through digital social networks. However, digital communities do not replicate the biophysical co-regulation of in-person environments. From a design perspective, the most reliable long-term social health outcomes are found in communities featuring intentional physical architecture, such as Blue Zones[5].
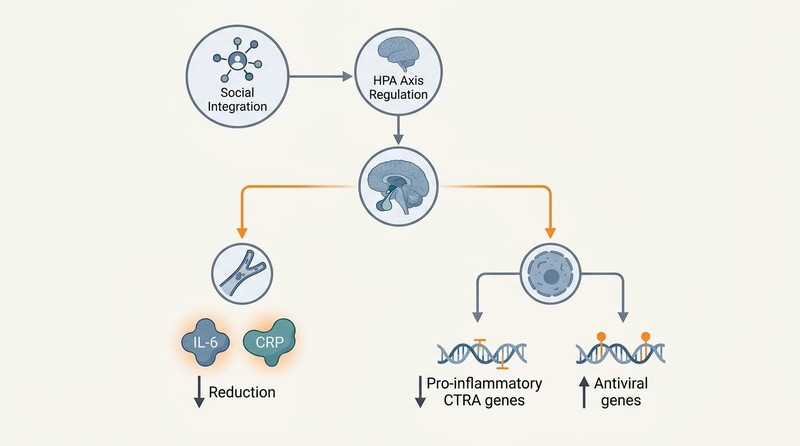
Figure 1: Biomedical pathway of social integration. High social connection buffers the HPA axis, reducing chronic inflammatory signaling and normalizing immune-cell transcription patterns.
These environments utilize specific physical layouts:
- Walkable Public Squares: Forcing spontaneous micro-interactions with local merchants and neighbors.
- Intergenerational Living: Integrating older adults directly into family or community childcare roles (e.g., the Okinawan moai or Sardinian family compounds).
- Dedicated Gathering Spaces: Ensuring that physical proximity is built into the geography of daily life.
¶ The Evidence Room
¶ Mechanism of Action
Social integration acts as a powerful neuroendocrine buffer. The biology of social isolation is characterized by the Conserved Transcriptional Response to Adversity (CTRA)[2:1].
When an individual lacks structural integration:
- The sympathetic nervous system (SNS) is chronically upregulated, releasing norepinephrine into lymphoid organs.
- Norepinephrine stimulates hematopoietic stem cells in the bone marrow to produce immature pro-inflammatory monocytes.
- These monocytes migrate to the systemic circulation, causing a systemic upregulation of pro-inflammatory cytokines (IL-1B, IL-6, TNF-alpha) and a downregulation of genes governing Type I interferon antiviral defenses.
- Concurrently, glucocorticoid receptor resistance develops, rendering the hypothalamic-pituitary-adrenal (HPA) axis incapable of shutting down the systemic inflammatory cascade.
Active community integration reverses this molecular pathology. Prosocial engagement stimulates the release of central oxytocin, which acts on the amygdala to downregulate threat-processing circuitry, thereby suppressing sympathetic signaling and restoring glucocorticoid sensitivity to circulating immune cells.
¶ Human Effect Matrix (Evidence Summary)
| Outcome | Typical Effect Size | Certainty Grade (GRADE) | Timeframe to Benefit | Supporting Studies |
|---|---|---|---|---|
| All-Cause Mortality Reduction | 50% increase in survival probability (OR: 1.50) | High | Observed over 7.5 years median follow-up | Holt-Lunstad et al., 2010[1:1] |
| All-Cause Mortality (90 Cohorts) | 32% reduced risk (RR: 1.32 for isolated vs integrated) | High | Long-term observational cohorts | Wang et al., 2023[3:1] |
| Inflammatory Marker Suppression | Significant reduction in CRP & IL-6 | Moderate | Cumulative life-course effect | Cole et al., 2011[2:2]; Steptoe et al., 2013[4:1] |
| Interferon Gene Activation | Favorable up-regulation of Type I antiviral genes | Moderate | Immediate transcriptional shifts | Cole et al., 2011[2:3] |
| Cardiovascular Protection | 34% reduced risk of CVD mortality | High | Multi-year prospective monitoring | Wang et al., 2023[3:2] |
¶ Life-Stage and Sex Differences in Community Integration
Autonomic responses and network needs vary across demographics. Aligning community design to these specific biological factors maximizes clinical effectiveness.
¶ 1. Biological Sex Differences
- Females ("Face-to-Face" & Co-Regulation): Women exhibit a highly active "tend-and-befriend" stress-buffering loop, regulated by the synergy of oxytocin and estrogen[6]. Estrogen enhances oxytocin receptor sensitivity in the prefrontal cortex and amygdala, promoting social bonding and emotional disclosure. Under social strain, women are more susceptible to pro-inflammatory cytokine surges (such as IL-6) but recover rapidly when engaging in highly reciprocal, face-to-face co-regulation.
- Males ("Side-by-Side" & Rhythmic Cooperation): Men are biologically more prone to social withdrawal under acute stress, driven by testosterone-induced down-regulation of oxytocin sensitivity and increased fight-or-flight sympathetic output. However, men show significant cardiovagal rebalancing (increased RMSSD and lower blood pressure) when participating in structured, goal-oriented "side-by-side" activities—including recreational athletic teams, civic work squads, or cooperative community projects—that leverage ancient evolutionary templates of tribal cooperation[6:1].
¶ 2. Age-Specific Stress and Network Dynamics
- Young Adults (Ages 18–34): Characterized by high geographical mobility, career-transition stress, and intense digital connection paired with physical isolation. This age group exhibits high sympathetic hyper-arousal and elevated rates of subclinical anxiety. The clinical priority is establishing a "structural baseline" by joining at least 2 distinct physical groups to counteract transient, digital-only connections.
- Middle-Aged Adults (Ages 35–64): Subject to the "sandwich generation" crunch (career peak, child rearing, and eldercare). Network contraction is severe, leading to high allostatic load and early metabolic dysfunction. The focus must be on "efficiency-based integration"—combining physical exercise, family duties, or professional mentoring with community involvement.
- Older Adults (Ages 65+): Experience post-retirement structural role loss, bereavement, and declining physical mobility. This is a critical risk phase for the Conserved Transcriptional Response to Adversity (CTRA), accelerating epigenetic aging (GrimAge) and prefrontal brain volume loss. Older adults require formal, structured roles (such as volunteer tutoring or civic leadership) to stimulate cognitive reserve and suppress systemic inflammaging[7].
¶ Protocols: Practical Daily & Weekly Integration Plans
Systematic social health requires structured, behavioral protocols. Utilize these templates to integrate social co-regulation into standard medical and lifestyle workflows.
¶ 1. The Weekly Social Health Protocol
Implement this structured schedule to achieve the biological threshold of social integration:
+-----------------------------------------------------------------------------+
| PROTOCOL: WEEKLY STRUCTURAL SOCIAL HEALTH |
+-----------------------------------------------------------------------------+
| 1. Daily Spontaneous Micro-connections |
| - Goal: 3 face-to-face verbal exchanges daily with local community |
| members (service workers, neighbors, merchants). |
| - Rule: Complete transactions without phones; make brief eye contact |
| and exchange friendly pleasantries (30-60 seconds). |
| |
| 2. Rhythmic Weekly Shared Somatic Space (60-90 minutes) |
| - Goal: Participate in 1 activity requiring physical or vocal synchrony |
| (e.g., group fitness class, community choir, running club, neighborhood|
| clean-up). Rhythmic shared movement activates the vagal brake. |
| |
| 3. Generative Volunteering / Mentorship (2 hours weekly / 100 hours yearly) |
| - Goal: Maintain consistent, formal volunteering inside an organized |
| civic group. Prioritize roles with intergenerational face-to-face |
| interaction. Reverses leukocyte pro-inflammatory transcript patterns. |
| |
| 4. The Sunday Shared Anchor Meal (90 minutes) |
| - Goal: Host or attend 1 structured, multi-generational family or peer |
| dinner weekly. Focus on vocal prosody, active listening, and collective|
| validation. Cell phones must be physically placed in another room. |
+-----------------------------------------------------------------------------+
¶ 2. Clinical Integration Decisional Framework
Use this pathway to prescribe targeted social interventions based on age and physiological risk profile:
[Patient Presents with High Perceived Stress]
|
+--------------------------+--------------------------+
| |
[Young Adult (Ages 18-34)] [Middle-Aged (Ages 35-64)] [Older Adult (Ages 65+)]
| | |
v v v
[Assess: Digital saturation] [Assess: Sandwich burnout] [Assess: Post-retirement role loss]
| | |
[Prescribe: Voice over text; [Prescribe: Civic-exercise [Prescribe: Formal volunteering]
Join 2 physical affinity hybrids; professional (Target: 2 hours/week;
groups within 30 days] mentorship roles] intergenerational contact]
¶ Interactive Social Scripts for Community Building
Anxiety or lack of practice frequently prevents social exploration. Use these word-for-word, clinically designed verbal templates to establish safety, navigate transitions, and manage boundaries.
¶ 1. Joining a New Physical Community Group
- Context: Initiating contact with a local running club, community garden, or civic organization.
- The Script:
"Hi, I'm [Name]. I've been reading about your group's work in [local neighborhood project] and really wanted to join a local team that is active in the real world. I'm a bit new to this specific activity, but I'd love to help out in any way at the next session. What are the best ways for a newcomer to get plugged in?"
¶ 2. Transitioning an Acquaintance to a Safe Peer Connection
- Context: Moving beyond polite, transactional greetings at a gym or workplace to establish relational depth.
- The Script:
"Hey [Name], I've really enjoyed our brief chats here. I'm trying to be much more intentional about building solid, in-person connections in the area rather than just staying cooped up behind screens. Would you be open to grabbing a quick coffee or a walk after our next session? I'd love to hear more about your work with [related topic]."
¶ 3. Initiating a Local Neighborhood Gathering
- Context: Establishing a geographical "Blue Zone" style micro-network on your physical block.
- The Script:
"Hi [Neighbor Name], I'm [Name] from down the street. I'm organizing a casual, 1-hour backyard get-together for our block next Saturday around 5:00 PM, just to give everyone a chance to put faces to names and build some local neighborhood connection. No pressure at all, but we'd love to have you stop by for a quick drink or snack if you're free."
¶ 4. The Symmetrical Boundary Pivot
- Context: Tactfully exiting or establishing strict boundaries in a high-conflict, non-reciprocal, or draining relationship.
- The Script:
"Hi [Name], I've been reflecting on my schedule and realized I am currently over-committed and experiencing quite a bit of fatigue. To manage my energy and responsibilities, I've had to make a strict rule to scale back my social commitments and long phone calls. I won't be as available for our deep-dive sessions, but I want to thank you for understanding as I focus on recovering my health."
¶ Measurement, Diagnostics, and Biomarker Monitoring
Social health must be assessed with the same clinical objectivity as glucose tolerance or blood pressure. Track these validated domains to monitor autonomic and immune rebalancing.
¶ 1. Validated Psychological Scales
- The Social Network Index (SNI): Evaluates the number of active, structural social roles (e.g., spouse, parent, group member, volunteer). Scoring <4 active roles is a robust, independent predictor of elevated all-cause mortality, comparable to clinical smoking[1:2].
- The UCLA Loneliness Scale (3-Item version): Evaluates subjective isolation through three quick vectors (How often do you feel you lack companionship? How often do you feel left out? How often do you feel isolated from others?). Scoring ≥6 indicates severe subjective loneliness, requiring immediate ventral vagal therapeutic intervention[4:2].
¶ 2. Physiological and Circulatory Biomarkers
- Overnight Heart Rate Variability (RMSSD): The gold-standard cardiovagal marker. A persistent decline in RMSSD below the rolling 21-day baseline corridor—without training overload or illness—indicates central threat-circuitry dominance (released vagal brake) driven by loneliness.
- Salivary Cortisol Awakening Response (CAR): Evaluates the integrity of the HPA axis. Loneliness triggers glucocorticoid receptor resistance, resulting in a flattened diurnal cortisol slope and a blunted morning cortisol spike. Restoration of healthy social safety loops normalizes the CAR slope within 4-12 weeks[2:4].
- Circulating Inflammatory Markers: Persistent objective isolation drives leukocyte pro-inflammatory transcript patterns. Check high-sensitivity C-reactive protein (hs-CRP, target <1.0 mg/L) and Interleukin-6 (IL-6, target <1.5 pg/mL). High elevations in these markers, in the absence of acute injury, serve as key signatures of isolation-induced inflammaging[1:3][2:5].
¶ Safety, Red Flags, and Caregiver Overload Mitigation
¶ 1. The High-Conflict Relationship Trap
Not all connection is health-promoting. Chronically hostile, critical, or asymmetrical social circles stimulate sustained sympathetic vasoconstriction and accelerate arterial stiffness.
- Red Flags:
- Feeling persistent dread, muscle tension, or elevated resting heart rate (>10 bpm above baseline) before or during interactions.
- Post-interaction rumination exceeding 2 hours, resulting in sleep latency >30 minutes.
- Decision Path: Implement a 4-week "relational fast." Completely suspend non-essential contact. If morning resting HRV increases and perceived stress scores decline, permanently transition the connection to a low-impact, structured transactional boundary.
¶ 2. Caregiver Overload & Prosocial Burnout
Volunteering and altruistic service must remain structured and voluntary. When community, family, or caregiver demands exceed physiological reserves, the patient transitions into caregiver overload—a state of allostatic collapse that triggers profound hypocortisolemia, systemic inflammation, and rapid epigenetic age acceleration[7:1].
- Red Flags:
- Waking up exhausted despite 8+ hours of sleep; severe cognitive fatigue or depersonalization.
- Persistent decline in overnight RMSSD by >1.5 standard deviations over 14 days.
- hs-CRP rising above 3.0 mg/L without infectious etiology.
- The Mitigation Protocol:
- Mandate a 14-day "Prosocial Sabbatical": Suspend all non-compulsory volunteering, mentoring, and community leadership duties.
- Autonomic Down-regulation: Practice Resonance Frequency Breathing (5.5-6 bpm) for 20 minutes twice daily.
- HPA Reconstruction: Administer standardized Ashwagandha (KSM-66, 600 mg daily) and L-Theanine (200 mg pre-bed) to buffer central threat circuits. Re-engage only in structured environments limited to ≤4 hours per week.
¶ References
¶ Update Log
- July 2026: Comprehensively expanded guide with gender/sex disparities, life-stage stress dynamics, weekly social health plans, validated measurement guides, clinical social scripts, and caregiver overload safety protocols.
Holt-Lunstad J, Smith TB, Layton JB. Social relationships and mortality risk: a meta-analytic review. PLoS Med. 2010;7(7):e1000316. https://pubmed.ncbi.nlm.nih.gov/20668659/ ↩︎ ↩︎ ↩︎ ↩︎
Cole SW, Hawkley LC, Arevalo JM, Cacioppo JT. Transcript-origin analysis identifies antigen-presenting cells as primary targets of socially regulated gene expression in leukocyte Han. PNAS. 2011;108(7):3017-3022. https://pubmed.ncbi.nlm.nih.gov/21282643/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wang F, Gao Y, Han Z, et al. A systematic review and meta-analysis of 90 cohort studies of social isolation, loneliness and mortality. Nat Hum Behav. 2023;7(8):1307-1319. https://pubmed.ncbi.nlm.nih.gov/37337095/ ↩︎ ↩︎ ↩︎
Steptoe A, Shankar A, Demakakos P, Wardle J. Social isolation, loneliness, and all-cause mortality in older men and women. PNAS. 2013;110(15):5797-5801. https://pubmed.ncbi.nlm.nih.gov/23530191/ ↩︎ ↩︎ ↩︎
Buettner D, Skemp S. Blue Zones: Lessons From the World's Longest-Lived People. Am J Lifestyle Med. 2016;10(5):318-321. https://pubmed.ncbi.nlm.nih.gov/28243187/ ↩︎
Franks MM, Friedman EM. Accentuating the Positive: Contribution of Positive Relations With Others and Daily Interpersonal Interactions to Longevity. Biopsychosocial science and medicine. 2026 Jun 12;14(2):45-56. https://pubmed.ncbi.nlm.nih.gov/42295203/ ↩︎ ↩︎
Kim ES, Whillans AV, Lee MT, et al. Volunteering and subsequent health and well-being in older adults: An outcome-wide longitudinal approach. Am J Prev Med. 2020;59(2):176-186. https://pubmed.ncbi.nlm.nih.gov/32536452/ ↩︎ ↩︎