¶ Continuous Glucose Monitoring
| Mechanism | Interstitial fluid glucose sensing |
| Key Spec | Mean Absolute Relative Difference (MARD) |
| Protocol | Continuous (10-14 day sensor life) |
| FDA Class | Class II / Class III |
| Entry Cost | $100 - $300 / month |
Continuous glucose monitoring (CGM) devices are wearable sensors that estimate glucose repeatedly throughout the day and night. They are established tools for diabetes management and are increasingly marketed to people without diabetes for metabolic feedback. Those are different use cases: accurate measurement does not by itself prove that consumer use improves health outcomes.
¶ At a glance
Key points
- Does it work? Yes, for diabetes management. CGMs improve glycemic control and reduce hypoglycemia in appropriate populations. In people without diabetes, studies show that CGM can describe glucose patterns, but evidence that routine use improves long-term clinical outcomes remains limited [1].
- Who needs it? Individuals with Type 1 diabetes, many with Type 2 diabetes (especially those on insulin), and patients with specific forms of hypoglycemia or glycogen storage diseases. Consumer use for "wellness" or metabolic tracking remains investigational.
- Verdict: An established and often important technology for diabetes care. Routine use in metabolically healthy people is an extrapolation with uncertain outcome benefit, added cost, and a risk of overinterpreting normal variation.
¶ Mechanism
¶ Interstitial Fluid vs. Blood Glucose
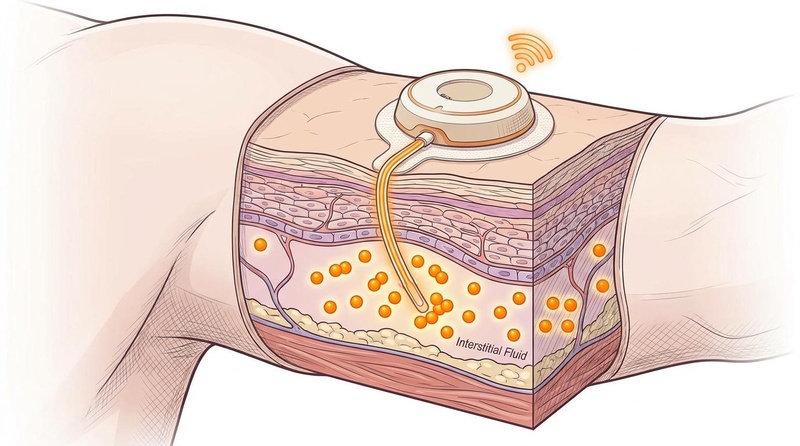
CGM sensors do not measure blood sugar directly. Instead, a tiny flexible filament sits just under the skin (subcutaneously) and measures glucose in the interstitial fluid (ISF)—the fluid surrounding the cells. Glucose moves from the blood vessels into the interstitial fluid, where it is oxidized by an enzyme on the sensor (typically glucose oxidase), generating an electrical current proportional to the glucose concentration [2].
¶ The Interstitial Lag
Because glucose must diffuse from the blood into the ISF, there is an inherent physiological delay, known as the interstitial lag. Blood glucose changes first, followed by ISF glucose several minutes later; the observed delay varies by device, physiology, and rate of change [3][4]. This matters most after eating, during exercise, and when glucose is rising or falling rapidly.
Newer predictive algorithms attempt to compensate for this lag mathematically, but users must understand that a CGM reading during a rapid spike or drop represents the past, not the immediate present [3:1].
¶ Key Specs: Accuracy and MARD
The gold standard metric for CGM accuracy is the Mean Absolute Relative Difference (MARD). It represents the average percentage error between the CGM reading and a simultaneous laboratory reference blood glucose value.
- A lower MARD indicates higher accuracy.
- Some current systems achieve study-level MARD values around 8% to 10%, but performance varies by device, population, glucose range, wear day, and comparator; a single MARD value does not describe every reading [5][2:1].
- Accuracy is often lower (higher MARD) in the first 24 hours of sensor wear, during hypoglycemia, and during rapid fluctuations [6].
¶ Indications & Established Clinical Uses
CGM is an established medical intervention with robust evidence guidelines for diabetes management.
- Type 1 Diabetes: Standard of care. CGMs are integrated into closed-loop insulin pump systems ("artificial pancreas"), drastically improving time-in-range and quality of life [7].
- Type 2 Diabetes: Strongly recommended by clinical guidelines for individuals on multiple daily insulin injections, and increasingly recognized as valuable for those on basal insulin or non-insulin therapies to improve glycemic control (HbA1c) [8][9].
- Glycogen Storage Diseases: Used to monitor and prevent severe hypoglycemia [10].
- Pregnancy: Used to manage hyperglycemia and gestational diabetes to improve maternal and fetal outcomes [11].
¶ Regulatory status is device-specific
In the United States, prescription CGMs have device-specific diabetes indications. The FDA has also cleared over-the-counter systems for adults aged 18 or older who do not use insulin, including people without diabetes who want to observe how diet and exercise relate to glucose. An OTC clearance confirms the device's intended use and safety controls; it does not establish that wellness use prevents diabetes or improves longevity. Some OTC systems are not designed to alert for dangerous hypoglycemia, so readers should follow the exact labeling of the product they use.
¶ Consumer Wellness & Non-Diabetic Use
The use of CGMs by individuals without diabetes has expanded through digital-health and wellness products. A systematic review found a growing body of observational and interventional research in non-diabetic populations, but heterogeneous studies and limited clinical endpoints do not establish that routine CGM use prevents future disease [1:1].
¶ Food and Exercise Experiments
People may use a short, predefined experiment to compare repeat responses to meals, sleep, or activity. Change one variable at a time, repeat the observation on more than one day, and treat the result as personal pattern-finding rather than a diagnosis. Exercise can temporarily raise or lower sensor glucose depending on intensity, timing, food, and medication [3:2]. There is no universal post-meal "spike" cutoff for a person without diabetes.
¶ Personalized Nutrition in Type 2 Diabetes
While the consumer focus is often on non-diabetic populations, the strongest evidence for CGM-guided dietary modifications (personalized nutrition) is found in individuals with Type 2 Diabetes. Scoping reviews indicate that integrating CGM data with personalized nutrition strategies can effectively guide dietary choices and improve time-in-range for these patients [12].
¶ What to Do with the Result (Interpretation)
Focusing on broad trends rather than hyper-fixating on single numbers is clinically prudent:
- Baseline stability: Observe fasting levels and overall baseline stability throughout the night.
- Pattern recognition: Look for repeatable trends rather than ranking foods from a single exposure. If you experiment, prefer changes that remain nutritionally balanced and sustainable [13].
- Confirm unexpected readings: Follow the device instructions when a reading does not match symptoms or when glucose is changing rapidly. Do not make medication or emergency-treatment decisions from a surprising consumer CGM value alone.
- Use validated diagnosis: A CGM trace does not diagnose prediabetes or diabetes. Discuss persistent concerns with a clinician, who can use validated blood tests and the full clinical context.
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Glycemic Control (HbA1c) | High | High | >20 RCTs | [Type 1 and Type 2 Diabetes; continuous use][9:1] | |
| Hypoglycemic Events | High | High | >10 RCTs | [Type 1 Diabetes; alerts and alarms integration][7:1] | |
| Quality of Life | Moderate | Moderate | >10 RCTs | [Patients with diabetes, reduction in fingersticks][9:2] | |
| Personalized Nutrition Guidance | Moderate | Moderate | Scoping Review | [Type 2 Diabetes; emerging use of CGM for dietary guidance][12:1] | |
| Long-term benefit in people without diabetes | Low | Low | Heterogeneous studies | CGM describes glucose patterns, but durable clinical-outcome benefit from routine wellness use is not established [1:2]. | |
| Access & Cost Effectiveness | High | Moderate | Multiple | [Type 2 Diabetes; cost-effectiveness recognized but disparities remain][14] |
¶ Safety, Limitations & Red Flags
While physically safe (complications are rare and mostly limited to skin irritation from the adhesive), the primary risks of CGM use in healthy populations are psychological and diagnostic [4:1].
¶ Accuracy Limitations and False Alarms
CGMs are least accurate during the first 24 hours ("sensor warmup") and when glucose is changing rapidly [2:2]. A healthy user might see a rapid dip to 60 mg/dL on their CGM and assume they are experiencing dangerous hypoglycemia, when in reality, the sensor is experiencing a "compression low" (caused by sleeping on the sensor and temporarily restricting interstitial fluid flow) or an algorithmic artifact [4:2].
¶ Psychological and disordered-eating considerations
Direct evidence that CGM causes disordered eating in healthy users is limited. Related evidence in diabetes populations nevertheless supports a cautious approach: a systematic review found orthorexia tendencies but limited evidence about their causes [15]; one small cross-sectional study found mixed results and no significant difference in orthorexia prevalence versus controls [16]; a single case report described restrictive eating driven by fear of CGM arrows [17]; and a review in type 2 diabetes reported both nutritional-awareness benefits and distressing or restrictive effects for some users [18]. These findings identify a plausible risk, not a known incidence or proof of causation in wellness users.
Pause the experiment and seek help from a clinician or eating-disorder-informed dietitian if the data causes anxiety, compulsive checking, avoidance of varied foods, rigid rules, or social withdrawal. A perfectly flat glucose line is neither required nor a sensible wellness target.
¶ Equity, Access, and Costs
CGMs represent a significant financial burden. Without insurance coverage (which is typically reserved for established diabetes diagnoses), out-of-pocket costs range from $100 to $300 per month for sensors, plus the cost of smartphone apps or subscription services. The growing consumer market for CGMs has sparked ethical debates about resource allocation, as supply chain shortages have occasionally impacted availability for insulin-dependent diabetic patients who rely on the technology for survival [14:1].
¶ References
"Continuous glucose monitoring in non-diabetic populations: a systematic review of observational and interventional studies with meta-analysis." PubMed. 2026. https://pubmed.ncbi.nlm.nih.gov/41588451/ ↩︎ ↩︎ ↩︎
"Calibration algorithms for continuous glucose monitoring systems based on interstitial fluid sensing." PubMed. 2024. https://pubmed.ncbi.nlm.nih.gov/38843770/ ↩︎ ↩︎ ↩︎
"Lag Time Remains with Newer Real-Time Continuous Glucose Monitoring Technology During Aerobic Exercise in Adults Living with Type 1 Diabetes." PubMed. 2019. https://pubmed.ncbi.nlm.nih.gov/31059282/ ↩︎ ↩︎ ↩︎
"Minimizing the impact of time lag variability on accuracy evaluation of continuous glucose monitoring systems." PubMed. 2013. https://pubmed.ncbi.nlm.nih.gov/23294784/ ↩︎ ↩︎ ↩︎
Zhang, T., et al. "Accuracy of Dexcom G6 Pro and G7 Continuous Glucose Monitors in Patients Treated with Maintenance Dialysis." PubMed. 2024. https://pubmed.ncbi.nlm.nih.gov/40824875/ ↩︎
"Continuous glucose monitoring system: Is it really accurate, safe and clinically useful?" PubMed. 2014. https://pubmed.ncbi.nlm.nih.gov/24843568/ ↩︎
"Continuous glucose monitoring considerations for the development of a closed-loop artificial pancreas system." PubMed. 2012. https://pubmed.ncbi.nlm.nih.gov/22226249/ ↩︎ ↩︎
"Evidence-based recommendations for the use of continuous glucose monitoring in type 2 diabetes: the Italian guidelines." PubMed. 2026. https://pubmed.ncbi.nlm.nih.gov/42207272/ ↩︎
"Does Continuous Glucose Monitoring Improve Glycemic Control and Quality of Life Among Adults With Type 2 Diabetes in Primary Care Settings? A Systematic Review and Meta-Analysis." PubMed. 2026. https://pubmed.ncbi.nlm.nih.gov/42206506/ ↩︎ ↩︎ ↩︎
"Continuous Glucose Monitoring in Glycogen Storage Diseases: A Systematic Review of Clinical Utility, Accuracy and Patient Outcomes." PubMed. 2026. https://pubmed.ncbi.nlm.nih.gov/42394382/ ↩︎
"The Role of Continuous Glucose Monitoring in Managing Hyperglycaemia First Detected in Pregnancy: A Narrative Review." PubMed. 2026. https://pubmed.ncbi.nlm.nih.gov/42310939/ ↩︎
"Continuous Glucose Monitoring and Personalized Nutrition in Type 2 Diabetes - A Scoping Review." PubMed. 2026. https://pubmed.ncbi.nlm.nih.gov/42394009/ ↩︎ ↩︎
"Bridging the Continuous Glucose Monitoring decision gap: from glycaemic variability data to actionable stability in diabetes care." PubMed. 2026. https://pubmed.ncbi.nlm.nih.gov/42290861/ ↩︎
"Continuous Glucose Monitoring in Type 2 Diabetes: Clinical Outcomes, Disparities in Access, and Cost-effectiveness." PubMed. 2026. https://pubmed.ncbi.nlm.nih.gov/42329523/ ↩︎ ↩︎
Grammatikopoulou MG, Gkiouras K, Polychronidou G. "Obsessed with Healthy Eating: A Systematic Review of Observational Studies Assessing Orthorexia Nervosa in Patients with Diabetes Mellitus." Nutrients. 2021. https://pubmed.ncbi.nlm.nih.gov/34836080/ ↩︎
Cosentino C, Rossi E, Pala L. "Orthorexia nervosa and type 1 diabetes: results of a cross-sectional study." Acta diabetologica. 2023. https://pubmed.ncbi.nlm.nih.gov/36806923/ ↩︎
Tahir M, Zahid A, Afzal S. "Trapped by the Arrows: Avoidant/Restrictive Food Intake Disorder and the Illusion of Control in Type 1 Diabetes Mellitus." Cureus. 2025. https://pubmed.ncbi.nlm.nih.gov/40630348/ ↩︎
Mackie S, Wallace T, Heath J. "The impact of glucose monitoring devices on relationships with food and eating behaviour for people with type 2 diabetes mellitus: A review of the literature." Diabetes & metabolic syndrome. 2026. https://pubmed.ncbi.nlm.nih.gov/41719841/ ↩︎