¶ Coronary Artery Calcium Scoring
| Indication | Cardiovascular Risk Stratification |
| Access | Clinician referral or self-pay, depending on region |
| Repeat testing | Individualized; often unnecessary once management is established |
| Safety Profile | Low-dose radiation (~1 mSv) |
| Key Marker | Agatston Calcium Score |
| Est. Cost | $100-$400 out-of-pocket |
Coronary artery calcium (CAC) scoring is a non-contrast, electrocardiogram-gated computed tomography (CT) scan that detects and quantifies calcified plaque in the coronary arteries. It is a risk marker—not a direct test of blood-flow obstruction—and can help an asymptomatic adult and clinician refine a primary-prevention decision when conventional risk assessment leaves meaningful uncertainty.
¶ At a glance
- What people use it for: Refining cardiovascular risk when an asymptomatic adult and clinician remain uncertain about the value of preventive treatment after considering standard risk factors.
- Does it work? Yes for risk prediction and reclassification: large cohorts show that CAC adds prognostic information beyond conventional risk factors [1][2]. Whether a CAC-guided strategy itself reduces cardiovascular events more than standard care remains uncertain.
- Key risks: Ionizing radiation, incidental findings and follow-up cascades, cost, anxiety, and false reassurance from a score of zero [3][4].
- Verdict: Most useful as a selective shared-decision tool, commonly in borderline- or intermediate-risk asymptomatic adults. It is not a rule-out test for active symptoms and is usually unnecessary when treatment decisions are already clear [5][6].
¶ Mechanism
¶ Scan Technique
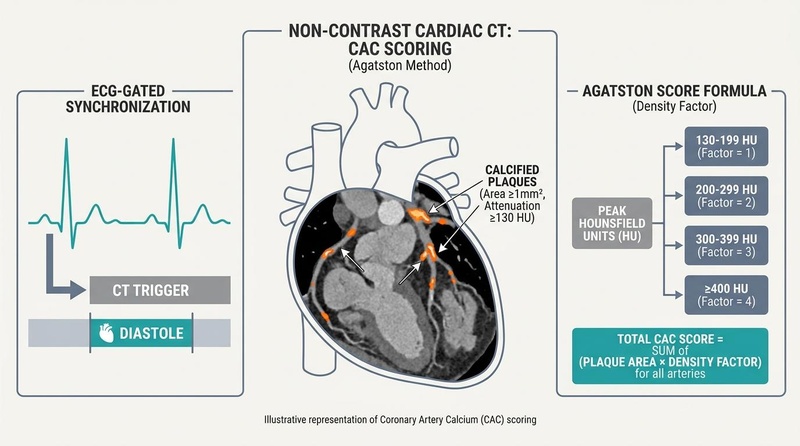
Coronary artery calcium scoring employs a fast, non-contrast chest CT scanner. Because the coronary arteries undergo rapid motion during the cardiac cycle, the acquisition is synchronized with the patient's electrocardiogram (ECG gating). ECG gating ensures that images are captured exclusively during a specific phase of the cardiac cycle—typically mid-to-late diastole when cardiac motion is minimized. This synchronization prevents motion artifacts that could blur the arterial wall, ensuring precise identification and volumetric rendering of calcified lesions.
¶ Pathophysiology of Vascular Calcification
Vascular calcification is not a passive process of mineral precipitation, but an active, highly regulated biological response to chronic vascular injury and atherogenesis, mimicking bone osteogenesis. The process begins with the retention of apolipoprotein B-containing lipoproteins (such as ApoB and Lp(a)) in the subendothelial space, which initiates a cascade of endothelial dysfunction, inflammatory cellular infiltration, and lipid accumulation.
Within the expanding lipid core of the plaque, macrophages, foam cells, and vascular smooth muscle cells (VSMCs) undergo necrosis and apoptosis. The resulting apoptotic bodies and microvesicles act as nucleating centers for calcium phosphate crystals (hydroxyapatite). As inflammation persists, VSMCs undergo an osteogenic phenotypic switch, expressing bone-related proteins (such as osteocalcin and RUNX2) that actively drive the formation of macroscopic, structured calcium sheets within the plaque's intima [7] [8].
While calcified plaque is often considered a late-stage stabilizing mechanism—representing "healed" or "stabilized" plaque that is less prone to acute rupture compared to lipid-rich, thin-cap fibroatheromas—its presence is a direct surrogate marker for the patient's total subclinical atherosclerotic burden. Accelerated coronary calcification is strongly associated with systemic inflammatory states, as observed in autoimmune conditions like ANCA-associated vasculitis [9], metabolic disturbances such as hyperuricemia [10], and chronic hypertensive states [7:1].
Furthermore, subclinical coronary calcification is closely correlated with future systemic inflammatory conditions, reflecting the tight biological link between vascular plaque burden and systemic immune activation [2:1].
¶ Key Specs
¶ Agatston Scoring Methodology
The standard metric for quantifying coronary calcium is the Agatston score, developed by Arthur Agatston in 1990. Plaque is defined as an area of attenuation of at least 130 Hounsfield Units (HU) spanning a minimum of 1 mm² (corresponding to at least 2-3 contiguous pixels on a standard CT slice). The Agatston score is calculated by multiplying the area of each calcified lesion by a density factor derived from the maximum attenuation of that lesion:
- 130–199 HU: Density factor of 1
- 200–299 HU: Density factor of 2
- 300–399 HU: Density factor of 3
- ≥400 HU: Density factor of 4
The scores of all calcified plaques across the major coronary arteries—Left Main (LM), Left Anterior Descending (LAD), Left Circumflex (LCX), and Right Coronary Artery (RCA)—are summed to generate the total Agatston score.
While the Agatston score remains the gold standard, alternative scoring systems exist. For example, the Weston Score is a visual assessment technique utilized primarily on non-gated chest CT scans, providing a semi-quantitative evaluation that is highly useful in specialized cohorts, such as patients with End-Stage Renal Disease (ESRD) or those undergoing noncardiac thoracic imaging [11].
¶ Interpretation of Agatston Scores
Common descriptive bands are shown below. They support discussion but do not prescribe treatment by themselves:
| Agatston Score | Risk Category | Clinical Implications |
|---|---|---|
| 0 | No calcified plaque detected | Often lowers estimated near-term risk, but does not exclude non-calcified plaque or override major risk enhancers, symptoms, or established disease [5:1][12]. |
| 1–10 | Minimal calcified plaque | Confirms some calcified atherosclerosis; interpret with age, sex, overall risk, and preferences [12:1]. |
| 11–100 | Mild calcified plaque | Can move a prevention discussion toward treatment in some people, but the decision remains individualized [12:2]. |
| 101–400 | Moderate calcified plaque | Indicates a higher plaque burden and generally strengthens the case for comprehensive risk-factor management [12:3]. |
| >400 | Extensive calcified plaque | Associated with high event risk and warrants timely clinician review of the complete cardiovascular-risk picture [12:4][13]. |
¶ Absolute Scores vs. Percentiles
Relying solely on absolute Agatston scores can be misleading because coronary calcification naturally increases with age and is significantly more prevalent in men than women. Therefore, absolute scores must always be contextualized using demographic-specific percentiles (such as those from the MESA database).
Percentiles can show whether a burden is unusually high for age and sex, but they do not turn the scan into a biological-age measurement and do not replace absolute risk. A high percentile can strengthen concern in a younger person even when the absolute score is modest [1:1][14].
The utility of using these percentiles is particularly critical in refining cardiovascular risk for diverse or historically underrepresented cohorts, such as South Asian adults, who often exhibit accelerated, premature patterns of subclinical plaque [15].
¶ Protocols
¶ Clinical Indications & Shared Decision-Making
The primary, guideline-supported indication for CAC scoring is in asymptomatic adults aged 40 to 75 who are at intermediate clinical risk (estimated 10-year ASCVD risk between 7.5% and 20%) based on traditional risk engines (such as the Pooled Cohort Equations) [5:2]. Within this cohort, CAC serves as a powerful "tie-breaker" or "decision-aid" during shared decision-making regarding lifelong lipid-lowering therapy.
¶ Repeat scanning
A repeat scan should be ordered only when the result is likely to change a future decision. Suggested intervals after a zero score vary with baseline risk, age, and guideline; they are not a universal 3-to-5-year schedule [3:1]. Once an elevated score has already changed management, serial scanning often adds little because treatment can alter plaque composition and calcium density without making score progression a valid treatment target [12:5][3:2].
¶ Inappropriate Clinical Scenarios
According to clinical cohort studies and "Choosing Wisely" guidelines, CAC scoring is frequently overutilized in inappropriate clinical scenarios. Specifically:
- It should not be performed in patients with known, established coronary artery disease (e.g., prior myocardial infarction, coronary artery bypass grafting, or percutaneous coronary intervention), as the clinical utility of risk-stratification is already obsolete [6:1].
- It usually adds little when a prevention decision is already clear from established disease or a very high-risk condition, although individual exceptions exist [5:3][12:6].
- It should not be used to dismiss chest pain, exertional breathlessness, syncope, or other possible ischemic symptoms. Those symptoms require prompt clinical assessment, with the diagnostic pathway chosen from the full presentation [5:4][6:2].
¶ Evidence
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Risk Reclassification | High | High | Multiple large cohorts | CAC can move selected people above or below conventional treatment-decision thresholds [1:2][16]. | |
| Cardiovascular-event prediction | High | High | Multiple large cohorts | Greater CAC burden is consistently associated with higher future event risk beyond standard risk factors [17][18][19]. | |
| CAC-guided care reducing events | Low | Low | Limited randomized evidence | Risk prediction is established, but direct evidence that scanning-guided care improves hard outcomes over standard assessment remains limited [20]. | |
| Statins and CAC progression | Moderate | Moderate | Mixed studies | Score or density can rise during effective therapy, so serial CAC is not a treatment-response target [12:7]. | |
| Vitamin K2 on CAC Progression | Moderate | Moderate | 1 RCT | Two years of Menaquinone-7 supplementation did not halt or slow CAC progression compared to placebo [21]. | |
| High Exercise Volume on CAC | Moderate | Low | Systematic Review | Extreme exercise volume may accelerate coronary calcification, though this is likely a benign plaque-stabilizing phenotype [22]. | |
| Lipoprotein(a) and CAC | High | High | Cohort Studies | Elevated Lp(a) is independently associated with higher CAC burden and carotid atherosclerosis [23][8:1]. |
- *Effect: Compact renderer encoding (preferred when using custom tags):
<effect e="[dir][mag][impact]"></effect>wheredir=u|d|e|q,mag=0|1|2|3,impact=p|n|x. Examples:↓↓ (p)-><effect e="d2p"></effect>,= (x)-><effect e="e0x"></effect>,?-><effect e="q0x"></effect>. - **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- ***Trials: Number of RCTs or total trials informing this outcome (shows evidence depth at a glance)
¶ Risk Reclassification & Cohort Evidence
Large longitudinal cohorts, including MESA and ARIC, show that CAC can improve cardiovascular-risk classification [1:3][2:2].
Among people near a treatment-decision threshold, a score of zero can lower estimated risk and may support deferral in selected cases after major risk enhancers are considered. It does not make deferral universally safe [5:5][16:1].
Conversely, unexpectedly high CAC can move a person toward a more intensive prevention discussion [16:2][19:1].
Furthermore, advancements in artificial intelligence have allowed integration of automated scoring models. Novel approaches, such as ECG-based deep learning or deep learning-derived pericardial adipose tissue quantification on cardiac CT, demonstrate incremental prognostic value, predicting future cardiovascular events even beyond the standard Agatston score [16:3] [24].
While serial measurements are sometimes utilized to monitor disease course, clinical registry data suggests that tracking the progression of coronary artery calcium over time provides limited incremental prognostic value for predicting future major adverse cardiovascular events once baseline risk has been established and preventive therapy is initiated [18:1] [25].
However, it is critical to note that while CAC is an outstanding risk marker, randomized controlled trial evidence explicitly demonstrating that CAC-guided treatment directly reduces clinical events compared to standard-of-care risk algorithms is still an evolving area of research [20:1].
¶ Opportunistic Screening on Non-Gated CT
A rapidly emerging clinical strategy is the opportunistic detection of CAC on non-ECG-gated chest CT scans performed for noncardiac indications (such as lung cancer screening, evaluation of pneumonia, or chronic obstructive pulmonary disease [COPD]). Approximately 19 million non-gated chest CT scans are performed annually in the United States alone.
While non-gated scans do not have the high temporal resolution of cardiac CTs, they are highly capable of detecting visual or semi-quantitative coronary calcification [26] [27].
Clinical trials, such as the ENCORES study, show that opportunistic detection of nongated CAC is highly predictive of operative risk in patients undergoing noncardiac surgeries [28].
Similarly, visual ordinal CAC scores on non-gated scans serve as strong independent predictors of all-cause mortality following severe COPD exacerbations [29], and AI-driven automated algorithms are increasingly utilized to semi-quantitate CAC as a clinically actionable "incidentaloma" without exposing patients to additional radiation, time, or out-of-pocket costs [26:1] [27:1] [30].
¶ Safety
¶ The Limitations of the Zero Score
A CAC score of zero is often reassuring in an appropriately selected asymptomatic adult, but it does not exclude non-calcified plaque and does not reduce risk to zero.
Non-calcified plaque can be present before calcium becomes detectable, particularly in younger people. Plaque risk depends on multiple features; "soft" is not synonymous with rupture-prone [14:1].
Therefore, a zero score must not be used to dismiss chest pain, exertional breathlessness, syncope, or other possible ischemic symptoms. Seek prompt medical assessment; a clinician should select any further testing from the symptoms, examination, and pre-test probability [5:6][6:3].
¶ Radiation Exposure
A modern ECG-gated CAC scan often delivers an effective dose around 1 millisievert (mSv), but dose varies with the scanner, protocol, and body size [3:3]. This is ionizing radiation, so the exposure should be justified by a reasonable chance that the result will change care. Comparisons with chest X-rays or mammography can mislead because those examinations and dose estimates vary.
¶ Incidental Findings & Downstream Cascades
The scan can reveal noncardiac incidental findings, such as pulmonary nodules or mediastinal abnormalities. Some matter; many do not.
Follow-up can include repeat imaging, referrals, or invasive procedures, with added radiation, cost, anxiety, and procedural risk. The possibility of detecting an important finding must be weighed against this cascade risk [4:1][27:2].
¶ Access, Equity, and Socioeconomic Disparities
Coverage for asymptomatic screening is inconsistent, and some people must self-pay.
Advertised prices are often $100 to $400, but the total can differ by country, insurer, imaging center, interpretation fee, and follow-up. Self-pay requirements can worsen access disparities. Confirm the full price and whether the result is likely to change care before scheduling.
¶ Red Flags and Contraindications
- Pregnancy: Elective CAC screening is generally avoided during pregnancy because it uses ionizing radiation and offers no urgent screening benefit. Urgent symptoms require clinical assessment rather than a screening CAC scan.
- Relative Contraindications:
- Severe Tachyarrhythmias: Uncontrolled atrial fibrillation or severe sinus tachycardia can disrupt ECG gating, resulting in severe motion blurring that renders the scan uninterpretable (though newer, high-speed CT scanners can partially mitigate this).
- Inability to Comply with Breath-Hold Protocols: Patients must lie flat and hold their breath for 3 to 10 seconds. Inability to do so creates severe motion artifacts.
- Clinical Red Flag:
¶ Actionable Next Steps ("What to do with the result")
- If your CAC score is 0: Review the result together with smoking, diabetes, family history, lipids, blood pressure, age, and symptoms. Continue proven prevention habits. Whether medication can be deferred and whether another scan would ever help are individualized decisions [12:8][3:4].
- If your CAC score is above 0: Discuss the absolute score, age/sex context, total cardiovascular risk, and options for managing modifiable risk factors. The scan alone does not select a drug, dose, aspirin strategy, or LDL target [12:9][13:1].
- CRITICAL WARNING: Never alter, start, or stop any prescription medications (including statins, PCSK9 inhibitors, or aspirin) based on your scan result without direct, personalized guidance and a prescription from your managing healthcare provider.
¶ FAQ
¶ Can I lower or reverse my coronary calcium score?
CAC is not a treatment-response target. Scores often remain stable or rise, and effective therapy can change plaque composition or density without producing a lower Agatston score. Focus on reducing clinical risk rather than trying to "chase" the scan number.
¶ Does taking Vitamin K2 reduce coronary calcium?
It is not established as a treatment for CAC. In one two-year randomized trial, menaquinone-7 did not slow CAC progression versus placebo [^15]. Do not substitute a supplement for evidence-based cardiovascular-risk management.
¶ Is fasting required before the scan?
No. Fasting is not required because a CAC scan does not require the injection of intravenous contrast dye. You may eat, drink, and take your regular medications normally prior to the procedure.
¶ If I have a high exercise volume, will it affect my score?
Some observational studies report more CAC in high-volume endurance athletes, but selection, plaque composition, and clinical meaning remain uncertain [^19]. Do not assume an elevated score is harmless because you exercise; interpret it with a clinician and your full risk profile.
¶ References
Wang FM, Cainzos-Achirica M, Ballew SH. Defining Demographic-specific Coronary Artery Calcium Percentiles in the Population Aged ≥75: The ARIC Study and MESA. Circulation. Cardiovascular imaging. 2023. https://pubmed.ncbi.nlm.nih.gov/37655462/ ↩︎ ↩︎ ↩︎ ↩︎
Manning ES, Shroff GR, Jacobs DR. Subclinical coronary artery calcification is associated with future inflammatory conditions in the Multi-Ethnic Study of Atherosclerosis. American Journal of Preventive Cardiology. 2026. https://pubmed.ncbi.nlm.nih.gov/42291055/ ↩︎ ↩︎ ↩︎
Zheutlin AR, Chokshi AK, Wilkins JT. Coronary Artery Calcium Testing—Too Early, Too Late, Too Often. JAMA Cardiology. 2025. https://pubmed.ncbi.nlm.nih.gov/40042828/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Murphy SJ, Winchester DE. Prevalence of CAC Scoring in Patients With Known Coronary Artery Disease: A Cohort Study on Choosing Wisely. Journal of Evaluation in Clinical Practice. 2025. https://pubmed.ncbi.nlm.nih.gov/40581979/ ↩︎ ↩︎
Hussain B, Mahmood A, Flynn MG. Coronary Artery Calcium Scoring in Asymptomatic Patients. HCA Healthcare Journal of Medicine. 2023. https://pubmed.ncbi.nlm.nih.gov/37969852/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Murphy SJ, Winchester DE. Prevalence of CAC Scoring in Patients With Known Coronary Artery Disease: A Cohort Study on Choosing Wisely. Journal of Evaluation in Clinical Practice. 2025. https://pubmed.ncbi.nlm.nih.gov/40581979/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Özet Mİ, Acehan F, Kaygısız M. Serum asprosin levels as a subclinical atherosclerosis marker in patients with primary hypertension. BMC Cardiovascular Disorders. 2026. https://pubmed.ncbi.nlm.nih.gov/42277661/ ↩︎ ↩︎
Savides MT, Bhatia HS, Kuznetsova I. The Evolving Role of Coronary Artery Imaging in Assessing Cardiovascular Risk from Lipoprotein(a). Current Atherosclerosis Reports. 2026. https://pubmed.ncbi.nlm.nih.gov/42429866/ ↩︎ ↩︎
Hendrickson M, Parakh A, Weber B. Burden of coronary artery calcification in ANCA-associated vasculitis. RMD Open. 2025. https://pubmed.ncbi.nlm.nih.gov/39762122/ ↩︎
Zhong Z, Zhang F, Hu X. Correlation between hyperuricemia and coronary artery calcification. The Journal of International Medical Research. 2026. https://pubmed.ncbi.nlm.nih.gov/42178649/ ↩︎
Fu J, Liao J, Long L. The Weston Score in coronary artery calcification among patients with End-Stage Renal Disease. Journal of Cardiothoracic Surgery. 2026. https://pubmed.ncbi.nlm.nih.gov/42192461/ ↩︎
Soroosh GP, Tasdighi E, Adhikari R. Coronary artery calcium in 2023: Guidelines for LDL-C goals, non-statin therapies, and aspirin use. Progress in Cardiovascular Diseases. 2024. https://pubmed.ncbi.nlm.nih.gov/38754533/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Cainzos-Achirica M, Quispe R, Mszar R. Coronary Artery Calcium Score to Refine the Use of PCSK9i in Asymptomatic Individuals: A Multicohort Study. Journal of the American Heart Association. 2022. https://pubmed.ncbi.nlm.nih.gov/35943062/ ↩︎ ↩︎
Asif A, Bairey Merz CN, Gransar H. Differences of plaque burden measures on CCTA in younger men and women. American Journal of Preventive Cardiology. 2026. https://pubmed.ncbi.nlm.nih.gov/42403470/ ↩︎ ↩︎
Gami A, Bisht S, Satish P. The utility of coronary artery calcium scoring to enhance cardiovascular risk assessment for South Asian adults. Progress in Cardiovascular Diseases. 2024. https://pubmed.ncbi.nlm.nih.gov/38723928/ ↩︎
Han C, You SC, Lee HC. Electrocardiogram-based deep learning score for coronary artery calcification reclassifies cardiovascular risk and identifies screening candidates. BMC Medical Informatics and Decision Making. 2026. https://pubmed.ncbi.nlm.nih.gov/41723484/ ↩︎ ↩︎ ↩︎ ↩︎
Anderson JL, Knight S, Dong L. Coronary Calcium Is Elevated in Patients with Myocardial Infarction without Standard Modifiable Risk Factors. Journal of Clinical Medicine. 2024. https://pubmed.ncbi.nlm.nih.gov/38731098/ ↩︎
He JM, Wang YC, Chang KC. Serial Coronary Artery Calcium Progression and Risk of Major Adverse Cardiovascular Events in an Asian Cohort. Journal of Clinical Medicine. 2026. https://pubmed.ncbi.nlm.nih.gov/42355820/ ↩︎ ↩︎
Raman E, Sailaxmi AK, Amaravadhi AR. Coronary artery calcium scoring for cardiovascular risk stratification: A prospective cohort study. Bioinformation. 2026. https://pubmed.ncbi.nlm.nih.gov/42282419/ ↩︎ ↩︎
Venkataraman P, Neil AL, Mitchell GK. The cost-effectiveness of coronary calcium score-guided statin therapy initiation for Australians with family histories of premature coronary artery disease. The Medical Journal of Australia. 2023. https://pubmed.ncbi.nlm.nih.gov/36841547/ ↩︎ ↩︎
Vossen LM, de Leeuw PW, Schurgers LJ. Two Years of Menaquinone-7 Supplementation and Coronary Artery Calcification: A Randomized Clinical Trial. JAMA Cardiology. 2026. https://pubmed.ncbi.nlm.nih.gov/42268593/ ↩︎
Ellingson CJ, Singh J, Shafiq MA. Exercise Volume and Coronary Artery Calcification: A Systematic Review. CJC Open. 2026. https://pubmed.ncbi.nlm.nih.gov/42007192/ ↩︎
Matta A, Ferrières D, Cougoul P. Association of advanced coronary artery calcification assessed by coronary artery calcium scoring with lipoprotein (a) and carotid atherosclerosis in asymptomatic patients. Nutrition, Metabolism, and Cardiovascular Diseases. 2026. https://pubmed.ncbi.nlm.nih.gov/42120211/ ↩︎
Esmaeili Z, Medina-Inojosa JR, Mahmoudi E. Deep learning-derived pericardial adipose tissue by electrocardiogram-gated cardiac computed tomography predicts cardiovascular events beyond coronary calcium score. American Journal of Preventive Cardiology. 2026. https://pubmed.ncbi.nlm.nih.gov/42291032/ ↩︎
Glidden MD, Sirasapalli SK, Yoder M. Incremental prognostic value of coronary artery calcium progression within a large community-benefit calcium score registry. American Journal of Preventive Cardiology. 2026. https://pubmed.ncbi.nlm.nih.gov/42291041/ ↩︎
Malik RF, Sun KJ, Azadi JR. Opportunistic Screening for Coronary Artery Disease: An Untapped Population Health Resource. Journal of the American College of Radiology. 2024. https://pubmed.ncbi.nlm.nih.gov/38382860/ ↩︎ ↩︎
Grant JK, Bokhari A, Manoharan A. Overcoming barriers to implementation: Improving incidental coronary calcium reporting on non-EKG gated chest CT scans. Journal of Clinical Lipidology. 2024. https://pubmed.ncbi.nlm.nih.gov/38908969/ ↩︎ ↩︎ ↩︎
Choi DY, Hayes D, Maidman SD. Existing Nongated CT Coronary Calcium Predicts Operative Risk in Patients Undergoing Noncardiac Surgeries (ENCORES). Circulation. 2023. https://pubmed.ncbi.nlm.nih.gov/37732454/ ↩︎
Xu H, Yew MS. Visual Ordinal Coronary Artery Calcium Score from Non-Gated Chest CT Predicts Mortality After Severe Chronic Obstructive Pulmonary Disease Exacerbation. International Journal of Chronic Obstructive Pulmonary Disease. 2023. https://pubmed.ncbi.nlm.nih.gov/38164410/ ↩︎
Kerndt CC, Chopra R, Weber P. Using Artificial Intelligence to Semi-Quantitate Coronary Calcium as an 'Incidentaloma' on Non-Gated, Non-Contrast CT Scans, A Single-Center Descriptive Study in West Michigan. Spartan Medical Research Journal. 2023. https://pubmed.ncbi.nlm.nih.gov/38084339/ ↩︎