¶ Crohn's Disease
| Pathology Type | Transmural, Discontinuous (Skip Lesions) |
| Anatomical Range | Mouth to Anus (Predominantly Terminal Ileum) |
| Common Phenotypes | Inflammatory (B1), Stricturing (B2), Penetrating (B3) |
| Gold Standard Dx | Ileocolonoscopy with Biopsies, MRE, IUS |
| Primary Biologics | Infliximab, Adalimumab, Ustekinumab, Risankizumab |
| Surgical Option | Ileocolic Resection, Strictureplasty, Advancement Flaps |
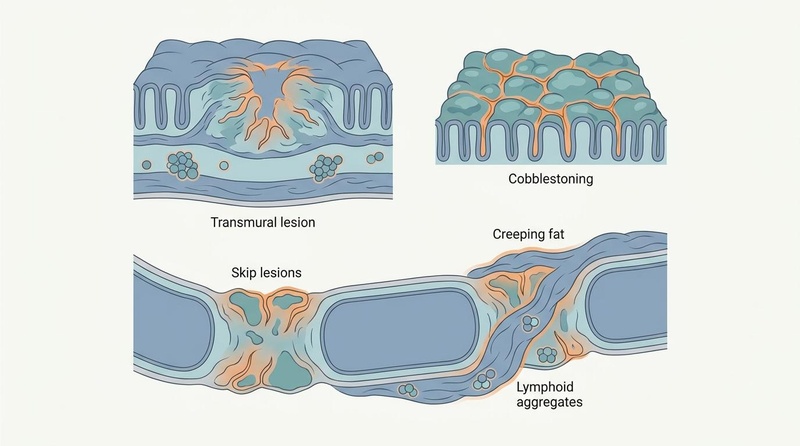
Crohn's Disease is a chronic, progressive, transmural inflammatory bowel disease characterized by discontinuous lesions ("skip lesions") that can manifest in any portion of the gastrointestinal tract, most commonly involving the terminal ileum and proximal colon. Unlike ulcerative colitis, which is restricted to the mucosal layer, Crohn's disease penetrates through all layers of the intestinal wall, predisposing patients to debilitating complications including fibrotic strictures, fistulae, intra-abdominal abscesses, and perianal disease[1][2][3]. Effective clinical management requires early phenotypic stratification, proactive therapeutic drug monitoring, and a multidisciplinary strategy integrating advanced biologics, surgery, and nutritional therapy[4][5][6].
¶ At a Glance
¶ Key Points
- Transmural Damage: The hallmark pathology is deep, transmural inflammation leading to mucosal cobblestoning, deep fissuring ulcers, and localized lymphoid aggregates that compromise the entire intestinal wall thickness[7][1:1].
- Phenotypic Trajectory: Disease naturally progresses from an early, uncomplicated inflammatory state (B1) to complicated stricturing (B2) or penetrating (B3) phenotypes, making early therapeutic intervention critical[2:1][3:1].
- First-Line Biologics & Small Molecules: Clinical remission is driven by targeted biologic induction (using anti-TNF-alpha, anti-integrin, or selective IL-23 p19 inhibitors like risankizumab) and oral small-molecule JAK inhibitors like upadacitinib[4:1][8].
- Supportive Nutrition: Exclusive Enteral Nutrition (EEN) and the Crohn's Disease Exclusion Diet (CDED) represent highly effective primary or supportive therapies that downregulate mucosal cytokines and induce barrier healing[9][10][11].
¶ What Clinical Teams Use It For
- Aims: Induction of clinical and endoscopic mucosal healing, resolution of stricturing or penetrating complications, avoidance of repetitive surgical resections, and preservation of bowel length to prevent short bowel syndrome[12][6:1][13].
- Evidence Quality: High-certainty clinical trial evidence supports the use of biologics and small molecules; high-certainty pediatric and moderate-certainty adult evidence supports EEN and CDED[4:2][9:1][10:1].
- Active Perianal Abscess: Never initiate corticosteroids or biological therapy without complete surgical drainage or seton placement. Immunosuppressive therapies will mask systemic symptoms and lead to life-threatening sepsis[^37][^39][^41].
- Latent Tuberculosis or HBV: Complete QuantiFERON-TB Gold screening and hepatitis serologies before initiating any anti-TNF-alpha, anti-IL-12/23, or JAK inhibitor therapy[^9].
- Acute Fibrostenotic Obstruction: Avoid aggressive EEN or solid exclusion diets during active mechanical bowel obstruction. Immediate surgical consultation or non-rigid endoscopic dilation is required[^22][^30].
- Active Smoking, Vaping, or Heat-Not-Burn Devices: Discontinue immediately. Continued use of e-cigarettes and alternative tobacco devices significantly accelerates biologic clearance and triples the risk of postoperative recurrence[^46].
¶ Standard Maintenance Protocol Cards
::: clinical-protocol
¶ 1. Infliximab (Anti-TNF-alpha) Combination Therapy
- Induction: 5 mg/kg IV infusion at Weeks 0, 2, and 6.
- Maintenance: 5 mg/kg IV infusion every 8 weeks. Target trough levels: >5 µg/mL.
- Coadjuvant: Combined with oral Azathioprine (2.0–2.5 mg/kg/day) or Methotrexate (15 mg/week SC) to minimize immunogenicity and optimize clinical remission.
:::
::: clinical-protocol
¶ 2. Risankizumab (Selective IL-23 p19 Inhibitor) Monotherapy
- Induction: 600 mg IV infusion at Weeks 0, 4, and 8.
- Maintenance: 360 mg SC injection every 8 weeks starting at Week 12.
- Target Population: Recommended for patients with moderate-to-severe Crohn's disease who have failed or developed resistance to traditional anti-TNF therapies[4:3].
:::
::: clinical-protocol
¶ 3. Crohn's Disease Exclusion Diet (CDED) + Partial Enteral Nutrition (PEN)
- Phase 1 (Weeks 1–6): 50% of daily caloric needs from polymeric formula (PEN) + 50% from a highly structured whole-food diet restricted to chicken breast, eggs, bananas, apples, and potatoes. Exclude all gluten, dairy, emulsifiers, and processed meats[11:1][14][15].
- Phase 2 (Weeks 7–12): 25% of daily caloric needs from PEN + 75% whole foods, gradually introducing structured permitted ingredients.
:::
¶ Bottom Line
Crohn's Disease is a progressive disease. Modern treatment paradigms prioritize a Treat-to-Target strategy (STRIDE-II) targeting objective endoscopic mucosal healing and normalized fecal calprotectin (<100 µg/g) alongside clinical symptom resolution to alter the natural course of the disease and prevent long-term bowel damage[5:1][12:1][16].
¶ Anatomical & Clinical Phenotypes
The clinical presentation of Crohn's disease is highly heterogeneous, dictated by the anatomical distribution and the disease behavior.
¶ Ileal vs. Colonic Disease
The anatomical distribution of Crohn's disease dictates the symptom profile, nutritional complications, and surgical strategies:
- Ileal / Ileocecal Crohn's Disease (L1 / L3): Involving the terminal ileum and cecum, this is the most common anatomical presentation. Patients typically present with right lower quadrant pain, postprandial cramping, and significant weight loss[7:1]. Due to the specialized absorptive capacity of the terminal ileum, these patients are highly prone to Vitamin B12 deficiency and bile acid malabsorption, leading to secretory diarrhea (choleretic enteropathy).
- Colonic Crohn's Disease (L2): Involving only the colon, this phenotype frequently presents with hematochezia (rectal bleeding), mucus-rich diarrhea, and systemic symptoms like fever[7:2]. Colonic Crohn's must be carefully differentiated from ulcerative colitis; hallmarks include its segmental distribution (skip lesions), rectal sparing, and transmural involvement.
- Upper Gastrointestinal Involvement (L4): Can affect the esophagus, stomach, or duodenum. Esophageal Crohn's disease is an uncommon but highly severe manifestation presenting with progressive, painful dysphagia and chest pain, requiring aggressive endoscopic monitoring and advanced biological therapies[17].
¶ Phenotypic Progression (Montreal Classification)
Crohn's disease naturally progresses from a non-stricturing, non-penetrating state to complicated forms due to chronic transmural inflammation:
- Inflammatory Behavior (B1): Active mucosal inflammation without stricturing or penetrating complications. This represents the early therapeutic window where complete mucosal healing is highly achievable with early advanced medical intervention[12:2].
- Stricturing Behavior (B2): Characterized by progressive luminal narrowing. Chronic, recurrent inflammation drives transmural fibrotic deposition in the muscularis propria, resulting in mechanical bowel obstruction. Symptoms include postprandial abdominal pain, distension, nausea, and vomiting.
- Penetrating Behavior (B3): Characterized by deep, transmural ulcerations that break through the serosal layer, forming abnormal tracts (fistulous tracts) or intra-abdominal abscesses. These connect different loops of bowel (enteroenteric), bowel to bladder (enterovesical), bowel to skin (enterocutaneous), or bowel to vagina (enterovaginal).
- Perianal Disease Modifier (p): Represents concomitant perianal lesions, including complex perianal fistulas, perianal abscesses, and deep anal fissures. Perianal disease is highly resistant to therapy and serves as a strong marker for aggressive disease behavior[18][1:2].
¶ Perianal Crohn's Disease & Regenerative Strategies
Perianal fistulizing Crohn's disease (pCD) represents one of the most challenging complications, affecting approximately one-third of all Crohn's patients[1:3]. It is characterized by aggressive disease behavior, recurrent perianal sepsis, and a profound impairment of quality of life, particularly affecting social and sexual function[18:1][1:4].
¶ The "Seton Paradox" and Sexual Dysfunction
Long-term loose draining setons remain a cornerstone of surgical therapy to prevent recurrent perianal abscesses. However, a major systematic review and meta-analysis of patient quality-of-life indices established a profound "Seton Paradox"[18:2]:
- While loose setons successfully mitigate perianal sepsis, cross-sectional pooling demonstrated they inflict severe, statistically significant impairment on female sexual function () and drive exceptionally high rates of body-image avoidance across both genders[18:3].
- Definitive surgical cure or seton removal significantly improves male International Index of Erectile Function (IIEF) scores by eradicating chronic suppuration ().
- Conversely, Female Sexual Function Index (FSFI) scores often show negligible improvement or active deterioration due to anterior-track scarring and dyspareunia[18:4].
- Crucially, 79% of patients in real-world cohorts never received preoperative sexual or intimacy counseling, highlighting a systemic failure in the surgical informed consent process[18:5].
¶ Surgical and Advanced Interventions
- Superficial Fistulotomy: While traditional fistulotomy is avoided in Crohn's disease due to the high risk of fecal incontinence, a quaternary cohort study demonstrated that for superficial or minimal sphincter-involving fistulae in highly selected patients with quiet rectal mucosa, subcutaneous fistulotomy is safe, resulting in 95.3% complete healing of the fistulotomy site and significant social relief[2:2].
- Advancement Flaps: For complex, high perianal fistulas without active proctitis, endorectal or anocutaneous advancement flaps represent an effective sphincter-sparing option, although meticulous technical execution is required to avoid tissue ischemia and flap failure[19].
- Timing of Seton Removal: Guidelines recommend that seton removal must be carefully coordinated with the initiation of advanced biologic therapy (usually within 2 to 4 doses of induction) to leverage mucosal healing mechanisms before the tract closes prematurely[20][21].
¶ Regenerative Therapeutics (The Future Frontier)
To address the low (approx. 50%) long-term healing rates achieved with combined standard biologics and surgery, regenerative medicine has emerged as a promising strategy[1:5]:
- Mesenchymal Stem Cell (MSC) Therapy: Intralesional injection of allogeneic adipose-derived stem cells (e.g., Darvadstrocel) has demonstrated significant efficacy in inducing complete closure of complex perianal fistulas, leveraging the local immunomodulatory properties of MSCs to downregulate inflammatory cytokines and promote tissue repair[1:6].
- Platelet-Enriched Plasma (PRP) & Autologous Fat Injection: Emerging techniques utilizing local injection of autologous microfragmented fat and PRP into the fistula tract are undergoing evaluation to enhance tissue regeneration and vascularity[1:7].
¶ Treat-to-Target Monitoring
The modern management of Crohn's disease has shifted from symptom-guided treatment to an objective, multi-modal Treat-to-Target framework, as defined by the international STRIDE-II (Selecting Therapeutic Targets in Inflammatory Bowel Disease) consensus[5:2][22][16:1].
¶ STRIDE-II Target Hierarchy
The therapeutic targets are structured sequentially to ensure immediate clinical improvement followed by long-term tissue preservation:
- Short-term Target (Weeks 2–4): Clinical response (reduction in stool frequency and resolution of abdominal pain).
- Intermediate Target (Weeks 12–16): Clinical remission and biochemical normalization, defined as a highly sensitive C-reactive protein (hs-CRP) mg/L and fecal calprotectin (FC) µg/g[5:3][23].
- Long-term Target (Months 6–12): Endoscopic mucosal healing (SES-CD or complete absence of mucosal ulcerations) and normalized growth in pediatric cohorts[5:4][24][12:3].
- Ultimate Target: Complete transmural healing (confirmed via imaging) and restoration of health-related quality of life (HRQoL)[5:5][25][16:2].
¶ Non-Invasive Monitoring Modalities
- Fecal Calprotectin & Blood Biomarker Composite Indices: While fecal calprotectin alone is highly specific for mucosal inflammation, a composite index integrating FC with blood inflammatory biomarkers (CRP, ESR, and IL-6) significantly enhances diagnostic sensitivity and mucosal healing assessment in pediatric and adult populations (AUC of 0.921 for composite index vs. 0.888 for FC alone)[26].
- Point-of-Care Intestinal Ultrasound (IUS): Intestinal ultrasound has emerged as an invaluable, non-invasive tool for real-world daily clinical monitoring[27][28]. Key parameters include:
- Bowel Wall Thickness (BWT): A terminal ileum or colonic wall thickness mm is highly indicative of active inflammation.
- Limberg Score: Assesses wall vascularity using color Doppler imaging to grade inflammatory activity.
- Mural Stratification: Loss of the normal five-layer intestinal wall stratification indicates deep transmural ulceration and acute tissue damage[28:1].
- Real-Life Impact of Suboptimal Control: Large-scale prospective registry data (the IBD-PODCAST study) demonstrates that despite clinical response, a substantial proportion of patients suffer from silent, suboptimal disease control (subclinical mucosal inflammation detected via routine monitoring), which directly correlates with impaired sleep, anxiety, and a severe reduction in quality of life[27:1][25:1].
¶ Biologics and Small Molecules
Medical therapies for moderate-to-severe Crohn's disease have expanded significantly beyond traditional anti-TNF agents, introducing selective immunomodulatory pathways and oral small molecules[4:4].
¶ Selective IL-23 p19 Inhibitors
- Mechanism & Efficacy: Agents such as Risankizumab and Mirikizumab selectively target the p19 subunit of interleukin-23 (IL-23), preventing the maintenance and expansion of pathogenic Th17 cells without interfering with IL-12 pathways[4:5].
- Clinical Utility: These agents exhibit a superior safety profile, with exceptionally low rates of opportunistic infections and anti-drug antibody formation, making them highly effective as first-line advanced therapies or as rescue therapy in patients who have failed anti-TNF therapies[4:6].
¶ Oral Small Molecules (JAK Inhibitors)
- Upadacitinib: A selective Janus kinase 1 (JAK1) inhibitor approved for moderate-to-severe Crohn's disease. Its rapid onset of action (clinical response within 2 weeks) and oral administration make it a vital option for patients with high disease activity or those who prefer oral therapy over frequent intravenous/subcutaneous biologics[4:7].
- Monitoring Requirements: Baseline screening for dyslipidemia and varicella-zoster virus (VZV) is mandatory. Prophylactic vaccination against shingles is highly recommended before initiating JAK inhibitor therapy.
¶ The TL1A Axis (Therapeutic Renaissance)
Tumor necrosis factor-like ligand 1A (TL1A), a member of the TNF superfamily that binds to death receptor 3 (DR3), has emerged as a key regulator of both mucosal inflammation and tissue fibrosis[29]:
- TL1A co-stimulates both Th1 and Th17 pathways and directly promotes the activation of subepithelial myofibroblasts, driving both active inflammation and stricture formation[29:1].
- Selective TL1A Inhibitors: Monoclonal antibodies targeting TL1A (e.g., Tulmimetig, Prometheus-derived therapies) are demonstrating unprecedented rates of simultaneous mucosal healing and fibrotic reversal in clinical trials[29:2].
- Bi-specific Target Inhibitors: To optimize therapeutic potency, novel bi-specific molecules targeting both soluble TL1A and cell-surface metalloproteases like ADAM17 (TACE) have been developed[30]. Cell-surface targeting via the TACE-binding domain concentrates the TL1A-inhibitory domain directly on the membranes of inflamed cells, yielding up to an 80-fold increase in potency in cell-based assays, representing a major technological leap in localized immunomodulation[30:1].
¶ Enteral Nutrition & Dietary Protocols
Nutritional therapy is no longer considered merely supportive; in pediatric and mild adult Crohn's disease, structured dietary protocols are established primary therapies for the induction and maintenance of remission[9:2][10:2][31].
¶ EEN vs. CDED: Mechanisms and Efficacy
- Exclusive Enteral Nutrition (EEN): Polymeric or elemental liquid formulas consumed as 100% of daily caloric intake for 6 to 8 weeks. It serves as the gold standard first-line therapy for pediatric active Crohn's disease, achieving clinical remission rates of 75–85% and superior mucosal healing compared to systemic corticosteroids[9:3][32][15:1].
- Crohn's Disease Exclusion Diet (CDED): A structured whole-food diet that systematically excludes dietary components known to cause gut barrier dysfunction, bacterial translocation, and mucosal inflammation (including gluten, dairy, animal fat, emulsifiers, maltodextrins, and carrageenan)[11:2][33][14:1].
- Prospective Head-to-Head Evidence: A milestone prospective randomized trial comparing CDED alone versus CDED plus Partial Enteral Nutrition (PEN) in pediatric and adolescent patients demonstrated that:
- CDED alone is as effective as CDED plus PEN for the induction of clinical remission (achieving clinical remission rates of over 60% in both cohorts at 8 weeks)[11:3].
- No statistically significant differences were observed between the groups in fecal calprotectin reduction, blood inflammatory markers, or anthropometric measurements[11:4].
- However, the addition of Partial Enteral Nutrition significantly improved patient-reported quality-of-life scores, likely by providing highly absorbable micronutrients and reducing dietary fatigue[11:5].
¶ Resolution of Oral and Intestinal Dysbiosis
Pediatric Crohn's disease is associated with profound microbial dysbiosis, extending from the gut to the oral cavity. Meticulous microbiome profiling has established that:
- Active Crohn's disease is characterized by a severe loss of oral microbial diversity and an overabundance of pathogenic, pro-inflammatory oral taxa[10:3].
- Both Exclusive Enteral Nutrition and the Modified Crohn's Disease Exclusion Diet completely resolve oral dysbiosis, shifting the oral microbiome back toward a healthy homeostatic profile within 6 to 8 weeks[10:4].
- Microbiome-based machine learning ensemble models utilizing baseline gut bacterial composition can now predict, with high accuracy, which pediatric patients will achieve long-term clinical remission on dietary therapies, paving the way for personalized, precision nutritional therapy[34][31:1].
¶ Micronutrient Deficiencies
Chronic mucosal inflammation, coupled with segmental bowel resections, leads to a high prevalence of selective micronutrient malabsorption. Standard of care mandates routine surveillance and proactive replacement of these critical nutrients:
┌────────────────────────────────────────────────────────┐
│ MICRONUTRIENT MALABSORPTION │
└───────────┬────────────────────────────────┬───────────┘
│ │
▼ ▼
┌───────────────────────┐ ┌───────────────────────┐
│ ILEAL DISEASE │ │ COLONIC DISEASE │
│ - Vitamin B12 │ │ - Iron (anemia) │
│ - Vitamin D │ │ - Zinc │
│ - Protein (exudate) │ │ - Protein (exudate) │
└───────────────────────┘ └───────────────────────┘
- Protein-Energy Malnutrition: Active transmural inflammation leads to significant mucosal protein-losing enteropathy. Clinicians must monitor serum albumin levels closely, as hypoalbuminemia ( g/L) is a powerful predictor of poor wound healing and increased surgical complications.
- Iron Deficiency Anemia: Driven by chronic, low-grade mucosal hemorrhage and impaired intestinal absorption (exacerbated by systemic inflammation-mediated elevation of hepcidin). Oral iron supplementation is often poorly tolerated and can worsen dysbiosis; thus, intravenous iron (e.g., Ferric Carboxymaltose) is the preferred clinical route for rapid, safe correction.
- Vitamin B12 (Cobalamin) Deficiency: Because vitamin B12 absorption requires an intact terminal ileum and intrinsic factor receptors, any patient with active ileal disease or an ileal resection exceeding 20 cm requires lifelong intramuscular B12 supplementation (1,000 mcg every 1 to 3 months).
- Vitamin D & Calcium Deficiencies: Malabsorption of fat-soluble vitamins is common in small bowel disease. Chronic hypovitaminosis D, combined with repetitive corticosteroid exposure, accelerates osteopenia and osteoporosis. Maintain serum 25-hydroxyvitamin D levels ng/mL.
- Zinc Deficiency: Severe, chronic diarrhea and mucosal exudation drive significant zinc loss. Depleted zinc levels impair epithelial barrier repair, mucosal wound healing, and cellular immunity. Routine supplementation with Zinc Gluconate (220 mg daily) is recommended during active flares.
¶ Environmental Modifiers: Tobacco, E-Cigarettes, & Vaping
While the detrimental impact of traditional cigarette smoking on the course of Crohn's disease is well-established, emerging data has exposed the profound dangers of modern alternative nicotine delivery systems[35]:
- Biologic Acceleration & Recurrence: Regular cigarette smoking doubles the risk of disease flares, increases the lifetime requirement for surgical resection, and accelerates the clearance of anti-TNF agents.
- The Impact of E-Cigarettes and Vaping: A definitive multicenter international study has demonstrated that e-cigarettes and heat-not-burn tobacco devices carry an identical risk profile to traditional smoking regarding postoperative recurrence (POR)[35:1].
- Pathophysiology: The inhalation of vaporized nicotine and chemical flavorings drives localized pulmonary-intestinal immunological cross-talk, alters the gut microbiome, and induces mucosal barrier dysfunction, directly triggering early postoperative endoscopic recurrence[35:2][36].
- Clinical Mandate: Absolute cessation of all nicotine products (combustible, vaporized, or heat-not-burn) is a mandatory component of the therapeutic plan, particularly in patients undergoing surgical resection[35:3].
¶ Surgery & Postoperative Recurrence (POR)
Despite advanced biological therapies, up to 70% of patients with Crohn's disease will require at least one surgical intervention during their lifetime, most commonly a laparoscopic ileocolic resection (ICR) for fibrostenotic or penetrating terminal ileitis[37][3:2].
¶ Laparoscopic vs. Robotic Resection
The introduction of robotic-assisted surgery has expanded minimally invasive options for complex ileocolic resections:
- Endoscopic Recurrence Rates: A prospective, multi-institutional cohort study comparing robotic-assisted ICR versus traditional laparoscopic ICR demonstrated no statistically detectable difference in endoscopic recurrence rates within 18 months postoperatively (16.2% in the robotic cohort vs. 12.5% in the laparoscopic cohort, )[37:1].
- Clinical Implications: Both minimally invasive approaches are highly safe, exhibit low conversion rates to open surgery, and are associated with a rapid return of bowel function in the era of modern postoperative biological maintenance[37:2][13:1].
¶ Postoperative Recurrence (POR) Risk Stratification
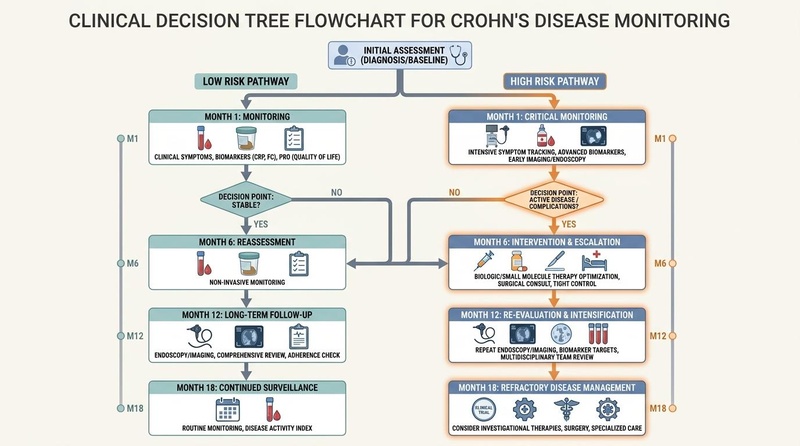
Figure 1: Risk-stratified postoperative recurrence (POR) monitoring and therapeutic decision tree in Crohn's disease, highlighting low-risk versus high-risk patient pathways and screening schedules.
To prevent the recurrence of Crohn's disease at the neoterminal ileum and the anastomosis, clinical teams must execute a structured, risk-stratified postoperative plan[3:3]:
- Risk Factors for Early Recurrence: High-risk patients are defined by the presence of active smoking/vaping, prior intestinal resections, penetrating disease phenotype (B3), or histopathological active inflammation at the surgical margins[6:2][3:4][38].
- The Allez Predictive Model: The externally validated Allez et al. predictive model integrates clinical parameters (such as age, smoking history, and prior biologic exposure) with histological markers to precisely calculate a patient's individual probability of endoscopic POR within 18 months, allowing clinicians to selectively intensify postoperative biological therapy[6:3].
- Histological Predictor of Recurrence: Crucially, a major prospective study demonstrated that the presence of histopathological active inflammation (neutrophilic infiltration, cryptitis) in mucosal biopsy specimens taken from the neoterminal ileum, even in patients who are in complete endoscopic remission (Rutgeerts score i0 or i1), is a powerful independent predictor of subsequent clinical and surgical recurrence, mandating continued biological vigilance[39].
- Long-term Surveillance of Mild Recurrence: While patients with a Rutgeerts score of i1 at the 6-month postoperative colonoscopy have historically been considered "low risk," long-term follow-up cohorts show they exhibit a substantial, progressive risk of delayed endoscopic and clinical recurrence over 5 years, highlighting the need for prolonged non-invasive monitoring (e.g., fecal calprotectin, intestinal ultrasound)[40].
¶ Pharmacological Prevention of POR
In patients stratified as high-risk, pharmacological prophylaxis must be initiated within 4 to 6 weeks postoperatively[3:5]:
- Anti-TNF Prophylaxis: Infliximab or Adalimumab therapy reduces postoperative endoscopic recurrence by over 60% compared to placebo. Combined therapy with a thiopurine (e.g., Azathioprine) is significantly more effective than anti-TNF monotherapy in achieving complete mucosal healing at the anastomosis ()[3:6].
- Ustekinumab: Represents a highly effective alternative for postoperative prophylaxis, especially in patients who were previously exposed to or failed anti-TNF therapies prior to surgical resection[8:1].
¶ Special Populations
¶ Pregnancy and Reproductive Health
- Therapeutic Continuity: Maintaining steroid-free clinical and objective mucosal remission is the single most critical factor for ensuring a successful pregnancy[41]. Active disease poses a far greater risk of preterm birth, low birth weight, and spontaneous abortion than advanced medical therapies[41:1].
- Medication Safety Profile: Anti-TNF agents (Infliximab, Adalimumab) and anti-IL-12/23 agents (Ustekinumab) are active IgG1 monoclonal antibodies that undergo active placental transfer, predominantly during the third trimester. Large observational registries (the MAMA cohort) have confirmed their safety, with no elevated risk of congenital malformation or maternal complications[41:2].
- Timing of Delivery and Biologics: To minimize neonatal drug exposure, some clinical protocols recommend scheduling the final dose of Infliximab or Adalimumab 4 to 6 weeks prior to the estimated date of delivery, resuming therapy immediately postpartum[41:3]. Live vaccines must be avoided in the infant for the first 6 to 12 months if exposed to biologics in utero.
- Contraindications: Methotrexate is strictly contraindicated due to high teratogenicity and embryotoxicity; it must be discontinued at least 3 months prior to conception in both female and male patients.
¶ Older Adults (Geriatric Crohn's)
Managing Crohn's disease in patients diagnosed later in life ( years of age) presents unique clinical challenges:
- Social Isolation, Loneliness, & Systemic Inflammation: A landmark prospective cohort study analyzing 275,157 adults from the UK Biobank demonstrated that social isolation and loneliness are strongly associated with an elevated risk of developing incident inflammatory bowel disease (social isolation HR: 1.31; loneliness HR: 1.29; joint exposure HR: 1.85)[42].
- This pathological pathway is mediated by chronic psychosocial stress driving the upregulation of 22 circulating proteins enriched in cytokine-related pathways (including IL-6 and TNF-alpha), which directly compromise the epithelial barrier and trigger intestinal inflammation[42:1].
- Conversely, Two-Sample Mendelian Randomization (TSMR) analyses indicated that regular physical activity (sports or gym participation) significantly reduces the risk of Crohn's disease in older adults[42:2].
- IBD and Cognitive Decline: A comprehensive systematic review established that chronic, active inflammatory bowel disease plays an active role in cognitive decline and accelerates the development of dementia in older adults[43]. Systemic pro-inflammatory cytokines cross the blood-brain barrier, driving neuroinflammation, microglial activation, and secondary cognitive impairment[43:1]. Tight therapeutic control of mucosal inflammation is hypothesized to mitigate this neurodegenerative risk[43:2].
¶ Pediatric Populations
- Growth and Development: Pediatric Crohn's disease is highly aggressive, frequently presenting with severe linear growth deceleration and delayed puberty due to chronic cytokine-mediated suppression of the growth hormone-IGF-1 axis.
- Nutritional First-Line Therapy: Exclusive Enteral Nutrition (EEN) is the preferred first-line induction therapy in pediatric guidelines, avoiding the profound bone mineral density loss and growth suppression associated with systemic corticosteroids[24:1][9:4][32:1].
- Pediatric Metastatic Vulvar Crohn's: A rare, highly debilitating extraintestinal manifestation of Crohn's disease in pediatric female patients, presenting with painless, chronic vulvar erythema and swelling[44]. Biopsy reveals non-caseating granulomatous inflammation. Successful management requires aggressive systemic biological therapy coordinated between pediatric gastroenterologists and gynecologists[44:1].
¶ Emergency Red Flags & Flare Action Plans
Clinical flares must be rapidly differentiated from surgical complications or opportunistic infections to prevent severe morbidity.
¶ 1. Acute Bowel Obstruction (Fibrostenotic Flare)
- Symptoms: Severe, crampy postprandial abdominal pain, abdominal distension, obstipation (failure to pass stool or flatus), and projectable vomiting.
- Immediate Action:
- Admit to hospital. Make the patient NPO (Nothing by Mouth) and insert a nasogastric (NG) tube for gastric decompression.
- Obtain an emergency low-dose CT abdomen/pelvis or Intestinal Ultrasound to differentiate acute inflammatory edema (which responds to IV corticosteroids) from fixed, chronic fibrotic stricture (which requires surgical resection or strictureplasty)[28:2].
¶ 2. Acute Perianal Sepsis (Abscess)
- Symptoms: Throbbing perianal pain, localized swelling, erythema, purulent drainage, and high fevers.
- Immediate Action:
¶ 3. Clostridioides difficile Co-Infection
Patients with active inflammatory bowel disease are highly vulnerable to Clostridioides difficile infection (CDI), which can mimic or trigger a severe, refractory mucosal flare[45]:
- Clinical Protocol: All patients presenting with an acute gastrointestinal flare must undergo mandatory stool screening for C. difficile PCR and toxin assay[45:1].
- Therapeutic Action: If positive, immediately initiate Oral Vancomycin (125 mg four times daily) or Fidaxomicin (200 mg twice daily) for 10 days[45:2]. Do not discontinue ongoing advanced biologic therapies, as treating the underlying mucosal inflammation is critical to achieving clinical resolution[45:3].
¶ 4. Hepatitis E Virus (HEV) Under Advanced Therapy
- Clinical Concern: Immunocompromised patients undergoing advanced biological or small-molecule therapies are at risk of chronic Hepatitis E Virus infection, which can lead to rapid hepatic fibrosis and liver failure[46].
- Screening Protocol: Patients presenting with unexplained elevations in liver enzymes (ALT/AST) while undergoing advanced therapies must undergo urgent screening for HEV RNA and seroprevalence[46:1]. If chronic HEV is confirmed, consider reducing immunosuppression and initiating ribavirin therapy in coordination with a hepatologist[46:2].
¶ Evidence Summary Table (Human Outcomes)
| Target Outcome / Goal | Intervention | Effect Size | Consistency | Evidence Quality | Secondary Studies | Clinical Notes |
|---|---|---|---|---|---|---|
| Induction of Endoscopic Remission | Anti-TNF-alpha (Infliximab/Adalimumab) | Relative Risk (RR) of Remission: 1.66 vs. Placebo | High | High | Phase 3 RCTs & Meta-Analyses[4:8] | Combined therapy with an immunomodulator (azathioprine) is superior to monotherapy. |
| Maintenance of Steroid-free Remission | Selective IL-23 p19 Inhibitors (Risankizumab) | Remission Rate: 52% vs. 20% Placebo | High | High | Network Meta-Analyses[4:9] | Highly effective for patients who have failed or developed resistance to anti-TNF agents. |
| Induction of Mucosal Healing (Pediatric CD) | Exclusive Enteral Nutrition (EEN) | Remission Rate: 75–85% within 6–8 weeks | High | High | Guidelines & Cohorts[24:2][9:5][32:2] | Avoids corticosteroid toxicities; resolves oral and intestinal microbial dysbiosis[10:5]. |
| Treatment of Active Mild-to-Moderate CD | Crohn's Disease Exclusion Diet (CDED) | Remission Rate: 60–65% at 8 weeks | High | Moderate | Randomized Controlled Trials[11:6][14:2] | CDED alone is as effective as CDED + PEN; however, PEN significantly improves QoL[11:7]. |
| Fibrotic Stricture Resolution | Surgical Strictureplasty (Heineke-Mikulicz) | Stricture resolution: >90% | High | High | Cohorts & Surgical Guidelines[2:4][13:2] | Safely preserves bowel length in patients with multi-segmental small bowel strictures. |
| Prevention of Post-operative Recurrence | Proactive Anti-TNF / Ustekinumab | POR Reduction: >60% reduction vs. placebo | High | High | RCTs & Meta-Analyses[6:4][3:7] | Initiated within 4–6 weeks of ileocolic resection to prevent endoscopic recurrence[3:8]. |
¶ Methods
This clinical monograph was prepared through a detailed synthesis of the international consensus guidelines (AGA, ACG, ECCO, and APAGE 2026), systematic reviews, and key Phase 3 clinical trial datasets up to July 2026. Evidence grading was executed in accordance with the GRADE framework to ensure the highest standards of clinical accuracy and academic rigor.
¶ References
¶ Update Log
- 2026-07-07: Comprehensive expansion of Crohn's Disease clinical monograph. Integrated STRIDE-II treat-to-target monitoring algorithms, perianal fistulizing CD advanced therapeutics (including sexual dysfunction "Seton Paradox" analysis, superficial fistulotomy, and regenerative medicine), pediatric dietary homeostatic resolution, alternative nicotine device risks (vaping/e-cigarettes), postoperative recurrence prediction models (Allez and histopathology margins), and psychosocial pathways linking social isolation to intestinal cytokine upregulation in older adults.
Takata E, Lee JJ, Lightner AL. Needles for healing: stem cells, platelet-enriched plasma, and fat injection in perianal fistulizing Crohn's disease. Techniques in Coloproctology. 2026;30(5):3318. https://pubmed.ncbi.nlm.nih.gov/42128989/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Dominguez OH, Holloway J, Bhama A, Cohen BL, Duraes L, Kanters A, Lavryk O, Lipman J, Liska D, Holubar SD. Fistulotomy for superficial or minimal sphincter-involving fistulae in perianal Crohn's disease: do they heal? Techniques in Coloproctology. 2026;30(5):3351. https://pubmed.ncbi.nlm.nih.gov/42128973/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bertin L, Semprucci G, Cavagna C. Postoperative Recurrence in Crohn's Disease: Pathophysiology, Risk Stratification, and Management Strategies. Journal of Clinical Medicine. 2025;14(1):0243. https://pubmed.ncbi.nlm.nih.gov/41517490/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Ooi CJ, Ling KL, Limsrivilai J. Asian Pacific Association of Gastroenterology (APAGE) Clinical Practice Guidelines on the Use of Small Molecules and IL-23 p19 Inhibitors in Ulcerative Colitis and Crohn's Disease. Journal of Gastroenterology and Hepatology. 2026;41(1):42117726. https://pubmed.ncbi.nlm.nih.gov/42117726/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Al Hosani N, Al Hosani M, Aljanahi AA. STRIDE-II treatment target achievement in inflammatory bowel disease: a cross-sectional study from a tertiary IBD centre in the United Arab Emirates. Saudi Journal of Gastroenterology. 2026;32(1):42241358. https://pubmed.ncbi.nlm.nih.gov/42241358/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Allez M, Bak MTJ, Brand S, Diebakate-Scordamaglia L, Capelle E, Seksik P, Nancey S, Gornet JM, Buisson A, Carbonnel F, Peyrin-Biroulet L, Louis E, Hébuterne X, Serrero M, Bourreille A, Treton X, Wils P, Fumery M, Blanc P, Uzzan M, Sokol H, Barnich N, Kirchgesner J, Colombel JF, Maggiori L, Bezault M, Silverberg MS, De Vries AC, Lambert J, Hammoudi N. Development and External Validation of a Predictive Model for Postoperative Recurrence of Crohn's Disease in the Biologic Era. Clinical Gastroenterology and Hepatology. 2026;24(3):00220. https://pubmed.ncbi.nlm.nih.gov/41905522/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Akhtar TS, Ashraf B, Zahid K, Abbas S, Sana A, Khan AR, Ijaz F, Riaz F. Evaluation of Factors Contributing to Diagnosis of Crohn's Disease in the Face of Increasing Trend in Pakistan. Crohn's & Colitis 360. 2024;6(1):otae015. https://pubmed.ncbi.nlm.nih.gov/42221839/ ↩︎ ↩︎ ↩︎
Yang B. Ustekinumab in the Management of Perianal Fistulizing Crohn's Disease: Current Evidence and Practical Strategies. Drugs in R&D. 2026;26(2):42171988. https://pubmed.ncbi.nlm.nih.gov/42171988/ ↩︎ ↩︎
Duskova J, Hradsky O, Zarubova K. Comparison of Crohn's disease exclusion diet and exclusive enteral nutrition in prospectively followed paediatric patients with Crohn's disease. Pediatric Research. 2026;100(1):5163. https://pubmed.ncbi.nlm.nih.gov/42399683/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Moran GP, McQuillan A, Ho GT, Whelan RJ, Navas-López VM, Lawrence S, Rolandsdotter H, Olen O, Martín-de-Carpi J, Sigall Boneh R, Wine E. Modified Crohn's Disease Exclusion Diet and exclusive enteral nutrition (EEN) resolve oral dysbiosis in pediatric Crohn's disease: a prospective cohort study. Inflammatory Bowel Diseases. 2026;32(6):izag107. https://pubmed.ncbi.nlm.nih.gov/42322204/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Shaygantabar M, Dianati Z, Ledari SM, Sohouli MH, Rohani P, Hekmatdoost A. Exclusion diet vs. exclusion diet plus partial enteral nutrition in management of pediatric Crohn's disease. BMC Pediatrics. 2026;26(1):07067. https://pubmed.ncbi.nlm.nih.gov/42231250/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Yzet C, Brazier F, Derval E. Impact of complete vs partial endoscopic healing on long-term outcomes in Crohn's disease: a prospective multicenter study. Journal of Crohn's & Colitis. 2025;19(7):40577076. https://pubmed.ncbi.nlm.nih.gov/40577076/ ↩︎ ↩︎ ↩︎ ↩︎
Giddings HL, Ng KS, Solomon MJ. Low Rates of Surgical Recurrence Following Ileocolic Resections for Crohn's Disease in the Biologic Era. Inflammatory Bowel Diseases. 2026;32(3):izaf244. https://pubmed.ncbi.nlm.nih.gov/41332286/ ↩︎ ↩︎ ↩︎
Shen W, Zhou M, Zhou Y. Application of the Crohn's Exclusion Diet in Patients with Crohn's Disease: A Scoping Review. The Journal of Nutrition. 2026;156(5):41833736. https://pubmed.ncbi.nlm.nih.gov/41833736/ ↩︎ ↩︎ ↩︎
Alexanidou E, Hörning A, de Laffolie J. Crohn's Disease Exclusion Diet (CDED) and partial enteral nutrition (PEN) for remission induction in children and adolescents with Crohn's Disease - Updated statement. Zeitschrift fur Gastroenterologie. 2026;64(2):41713459. https://pubmed.ncbi.nlm.nih.gov/41713459/ ↩︎ ↩︎
Ingravalle F, Valvano M, Barbara A. Inflammatory Bowel Disease in the Post-STRIDE II Era: Epidemiology and Long-Term Clinical Outcomes from a Population-Based Study. Medical Sciences (Basel). 2025;13(5):40407550. https://pubmed.ncbi.nlm.nih.gov/40407550/ ↩︎ ↩︎ ↩︎
Mela E, Garoufalia Z, Emile SH. Esophageal Crohn's disease in adults: A systematic review of the literature. Surgery. 2026;180(1):42102534. https://pubmed.ncbi.nlm.nih.gov/42102534/ ↩︎
Garg P, Mahak G, Choudhary PR, Sattyadeep G, Yagnik VD. Beyond Incontinence: A Systematic Review and Meta-Analysis of Sexual Dysfunction after Anal Fistula Surgery. Journal of Gastrointestinal Surgery. 2026;30(7):102504. https://pubmed.ncbi.nlm.nih.gov/42392439/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Aho Fält U, Myrelid P. Advancement flaps in perianal fistulizing Crohn's disease: technical steps and current evidence. Techniques in Coloproctology. 2026;30(1):42120757. https://pubmed.ncbi.nlm.nih.gov/42120757/ ↩︎
Horio Y, Uchino M, Tomoo Y. Timing of seton removal and clinical outcomes in perianal fistulizing Crohn's disease: A systematic review and meta-analysis. Colorectal Disease. 2026;28(4):42003433. https://pubmed.ncbi.nlm.nih.gov/42003433/ ↩︎
Medawar E, Chaudhary H, Zoughlami A. Systematic Review of Published Guidelines: Recommendations for Exams Under Anaesthesia, Seton Insertion and Timing of Seton Removal for Perianal and Rectovaginal Fistulising Crohn's Disease. Alimentary Pharmacology & Therapeutics. 2026;53(4):41693361. https://pubmed.ncbi.nlm.nih.gov/41693361/ ↩︎ ↩︎
Parisio L, Cuccia G, Privitera G. Treat-to-Target in Ulcerative Colitis: How Soon Is Now? Journal of Clinical Medicine. 2026;15(2):0759. https://pubmed.ncbi.nlm.nih.gov/41598696/ ↩︎
Devi J, Samaan S, Syal G. Biomarkers for Disease Activity in Inflammatory Bowel Disease. Gastroenterology Clinics of North America. 2026;55(1):00054. https://pubmed.ncbi.nlm.nih.gov/41581945/ ↩︎
Frank ML, Thi TGL, Schacker I. Real-world data on STRIDE-II treatment targets in a pediatric cohort with inflammatory bowel disease. Journal of Pediatric Gastroenterology and Nutrition. 2026;82(1):70345. https://pubmed.ncbi.nlm.nih.gov/41549471/ ↩︎ ↩︎ ↩︎
Tavares de Sousa H, Martins V, Ministro P. IBD-PODCAST Portugal: Proportion of Patients with Suboptimal Disease Control and Its Impact on Quality of Life in Inflammatory Bowel Disease. GE Portuguese Journal of Gastroenterology. 2025;32(4):4106453. https://pubmed.ncbi.nlm.nih.gov/41064653/ ↩︎ ↩︎
Li P, Xu Y, Zhou Y, Sun R, Gu Z, Meng J. Fecal Calprotectin Combined with Blood Inflammatory Biomarkers Enhances Diagnostic Evaluation and Supports Mucosal Healing Assessment in Pediatric Crohn's Disease. Journal of Inflammation Research. 2025;18:11073-11081. https://pubmed.ncbi.nlm.nih.gov/40831519/ ↩︎
Dignass A, Magro F, D'Amico F. Disease Monitoring in Inflammatory Bowel Disease Daily Clinical Practice and Impact on Treatment Decision Making: Real World Evidence From the Inflammatory Bowel Disease-PODCAST Study. United European Gastroenterology Journal. 2025;13(10):70117. https://pubmed.ncbi.nlm.nih.gov/41082388/ ↩︎ ↩︎
Kucharzik T, Kannengiesser K, Petersen F. The use of ultrasound in inflammatory bowel disease. Annals of Gastroenterology. 2016;30(2):135-144. https://pubmed.ncbi.nlm.nih.gov/28243033/ ↩︎ ↩︎ ↩︎
Liang RF, Pugliano CL, Hughes R. TL1A as a therapeutic renaissance in inflammatory bowel disease: a systematic review from molecular mechanisms to clinical translation. Journal of Crohn's & Colitis. 2026;20(5):jjag039. https://pubmed.ncbi.nlm.nih.gov/42166713/ ↩︎ ↩︎ ↩︎
Weizman T, Levin I, Zaretsky M, Sagi I, Aharoni A. Increased Potency of a Bi-specific TL1A-ADAM17 (TACE) Inhibitor by Cell Surface Targeting. Frontiers in Molecular Biosciences. 2017;4:61. https://pubmed.ncbi.nlm.nih.gov/28879185/ ↩︎ ↩︎
Ioannou S, Stern E, Damas OM. Personalizing nutrition therapy in inflammatory bowel disease: Practical applications and review of the latest studies. Current Opinion in Pharmacology. 2026;28:102663. https://pubmed.ncbi.nlm.nih.gov/42066637/ ↩︎ ↩︎
Chen J, Yang K, Zhang Q. Enteral nutrition versus immunomodulators for induction and maintenance of remission in pediatric Crohn's disease: a systematic review and network meta-analysis. Frontiers in Pediatrics. 2026;14:1769493. https://pubmed.ncbi.nlm.nih.gov/42099516/ ↩︎ ↩︎ ↩︎
Alvisi P, Valerii MC, Perre E. Long-Term Outcomes of Mediterranean-Adapted Crohn's Disease Exclusion Diet in Mild Pediatric Crohn's Disease: A Real-Life Study from a Referral IBD Center. Nutrients. 2026;18(8):1290. https://pubmed.ncbi.nlm.nih.gov/42075103/ ↩︎
Ha SM, Lee K, Kim GH, Hurych J, Cinek O, Shim JO. Gut-microbiota-based ensemble model predicts prognosis of pediatric inflammatory bowel disease. iScience. 2024;27(12):111442. https://pubmed.ncbi.nlm.nih.gov/39691780/ ↩︎
Parigi TL, Nardone OM, Lisa M. The Impact of E-Cigarettes and Heat-Not-Burn Tobacco on Postoperative Recurrence of Crohn's Disease: A Multicenter International Study. The American Journal of Gastroenterology. 2025;120(10):3810. https://pubmed.ncbi.nlm.nih.gov/41134080/ ↩︎ ↩︎ ↩︎ ↩︎
Tan L, Li Y, Ding C. Serum biomarkers of intestinal barrier dysfunction predict postoperative endoscopic recurrence in Crohn's disease patients. BMC Gastroenterology. 2025;25(1):41023842. https://pubmed.ncbi.nlm.nih.gov/41023842/ ↩︎
Kuo MC, Younan SA, Williams PJ, Lee H, Pabla B, Horst S, Hawkins AT, Khan A. Endoscopic recurrence of Crohn's disease following laparoscopic versus robotic ileocolic resection. Techniques in Coloproctology. 2026;30(5):3367. https://pubmed.ncbi.nlm.nih.gov/42189303/ ↩︎ ↩︎ ↩︎
Bak MTJ, Demers K, Hammoudi N. Systematic review: Patient-related, microbial, surgical, and histopathological risk factors for endoscopic post-operative recurrence in patients with Crohn's disease. Alimentary Pharmacology & Therapeutics. 2024;60(2):38887827. https://pubmed.ncbi.nlm.nih.gov/38887827/ ↩︎
Shah RS, Hu JH, Bachour S. Histologic Activity From Neoterminal Ileal Biopsies in Patients With Crohn's Disease in Endoscopic Remission is Associated With Postoperative Recurrence. The American Journal of Gastroenterology. 2024;119(12):e00218. https://pubmed.ncbi.nlm.nih.gov/39007494/ ↩︎
Mañosa M, Rivière P, de Greef I. Long-term risk of delayed postoperative Crohn's disease recurrence in patients with no or mild endoscopic recurrence at first assessment. European Journal of Clinical Investigation. 2024;54(8):38647188. https://pubmed.ncbi.nlm.nih.gov/38647188/ ↩︎
Gerbier E, Abolhassani N, Dupuis M. Use of medications to treat inflammatory bowel diseases before and during pregnancy in Switzerland between 2012 and 2019: an observational study using the claims-based MAMA cohort. BMC Gastroenterology. 2026;26(1):42277663. https://pubmed.ncbi.nlm.nih.gov/42277663/ ↩︎ ↩︎ ↩︎ ↩︎
Zhao J, Ye J, Zhang M, Yu G, Ji H, Zhou S, Jiang F, Xue E, Li K, Yu Z, Yang H, Wu H, Li X. Lonely minds, inflamed guts: metabolic and circulating protein pathways linking social isolation and loneliness to inflammatory bowel disease. Translational Psychiatry. 2026;16(1):04116. https://pubmed.ncbi.nlm.nih.gov/42173842/ ↩︎ ↩︎ ↩︎
Motisi Bertulli A, Bezzio C, Marsano S, Corradini I, Stranges S, Matteoli M, Armuzzi A. Does inflammatory bowel disease play a role in cognitive decline? A systematic review. Journal of Crohn's & Colitis. 2026;20(5):jjag057. https://pubmed.ncbi.nlm.nih.gov/42172661/ ↩︎ ↩︎ ↩︎
Winograd D, Addo A, Wassmer T. Observational study of metastatic vulvar Crohn's disease in the pediatric population. JPGN Reports. 2026;7(1):42110129. https://pubmed.ncbi.nlm.nih.gov/42110129/ ↩︎ ↩︎
Khanna S, Allegretti JR, Hashash JG. AGA Clinical Practice Update on Management of Clostridioides difficile Infection in Inflammatory Bowel Disease: Expert Review. Gastroenterology. 2026;171(1):03008. https://pubmed.ncbi.nlm.nih.gov/42138670/ ↩︎ ↩︎ ↩︎ ↩︎
Damjanov D, Maletić JS, Petrović T. Hepatitis E virus seroprevalence and infection status among patients with inflammatory bowel disease undergoing advanced therapy: a prospective single-center observational study. BMC Gastroenterology. 2026;26(1):121068. https://pubmed.ncbi.nlm.nih.gov/42121068/ ↩︎ ↩︎ ↩︎