¶ Dental Caries Prevention and Remineralization
| Primary Indications | Incipient Caries, Enamel Demineralization [^1][^13] |
| Therapeutic Agents | Fluorides, Biomimetic Hydroxyapatite, Calcium Phosphate Derivatives (CPP-ACP), Silver Diamine Fluoride (SDF) [^1][^5][^11][^12] |
| Access | Over-the-Counter (Toothpaste/Rinses), Professional Application (Varnishes/Preparations) [^12][^18] |
| Monitoring Markers | Fluorescence, Visual-Tactile Assessment [^19] |
| Safety Profile | High Biocompatibility; Fluorosis risk at high pediatric systemic doses [^12] |
| Key Outcome | Acid-Resistant Crystalline Layer, Mineral Recovery in Early Lesions [^12][^16] |
Dental caries is a highly prevalent, biofilm-mediated, sugar-driven disease characterized by phasic demineralization and remineralization of dental hard tissues [1]. Rather than treating caries strictly as a surgical disease requiring aggressive excision and restoration, modern minimally invasive dentistry manages caries as a dynamic chemical continuum [2][3]. By modulating the balance of protective salivary factors and pathological challenges, clinicians can stabilize, halt, or completely reverse early-stage non-cavitated carious lesions through targeted remineralization therapy [4][5][2:1].
¶ TL;DR
- Clinical Verdict: Modern dental caries management centers on a dynamic biochemical continuum, shifting from traditional surgical intervention to chemical arrest and biomimetic remineralization [2:2][1:1][3:1].
- Target Population: Crucial for individuals with active demineralization (white spot lesions) [6][7], salivary dysfunction [5:1][1:2], pediatric populations undergoing tooth development [8], and elderly patients with exposed root dentin [8:1][1:3].
- Expected Outcome: Reversal of non-cavitated lesions over several months [4:1][9], and stabilization of exposed root surfaces [10][8:2].
- Key Risks & Precautions: Chronic pediatric ingestion of systemic fluoride raises the risk of enamel fluorosis [8:3].
- Immediate Action: Adopt a twice-daily brushing regimen using fluoride or biomimetic hydroxyapatite toothpastes, and reduce the frequency of dietary fermentable carbohydrates [4:2][8:4][11].
¶ Quick Answer
Dental caries is a biofilm-mediated, sugar-driven disease characterized by phasic demineralization and remineralization of dental hard tissues [1:4]. It can be prevented or reversed by tipping the chemical balance in favor of remineralization [5:2][2:3]. This is achieved topically using fluorides (forming an acid-resistant crystalline layer that is chemically more stable and resistant to acid challenges) [11:1][2:4] or biomimetic minerals like nano-hydroxyapatite (nHAP) and calcium phosphate derivatives, which deposit calcium and phosphate ions into the demineralized subsurface matrix [4:3][6:1][12]. Clinical trials show that non-cavitated lesions can be successfully arrested and structurally repaired after 6 to 24 months of consistent topical therapy using fluorides, biomimetic hydroxyapatite, or combined formulations without requiring surgical drilling [4:4][13].
¶ What It Is
Dental caries prevention and remineralization is a medical-biological strategy designed to conserve natural tooth structure by manipulating the biochemical environment of the oral cavity [2:5][1:5][3:2]. Instead of regarding carious lesions as permanent defects requiring drilling and filling, this discipline treats them as dynamic mineral-loss patterns that can be clinically reversed or arrested using advanced topical pharmacology [5:3][11:2][2:6].
The fundamental process relies on progressive mineral restoration. When the oral environment is maintained in a state with calcium, phosphate, and fluoride ions, these minerals actively diffuse back into the porous, demineralized subsurface enamel [11:3][2:7].
¶ Mechanism in 60 Seconds: The Crystalline Repair Analogy
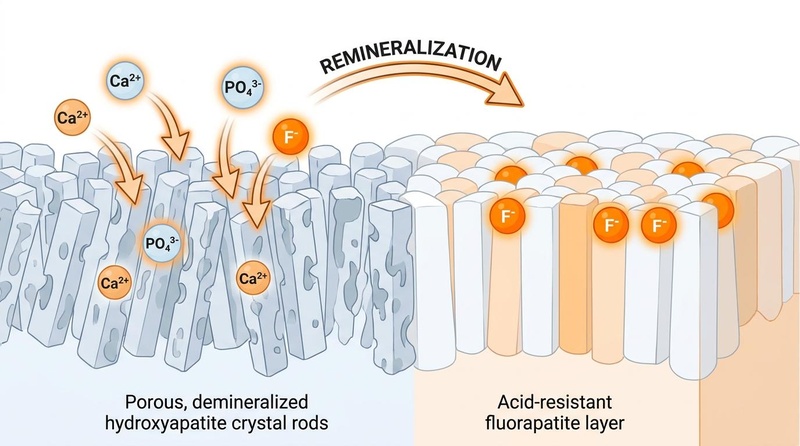
Think of tooth enamel as a brick wall where the individual bricks are hydroxyapatite crystals. Under acid attack from plaque bacteria, the calcium and phosphate "mortar" holding the bricks together dissolves, leaving the wall structurally porous and weak (demineralization) [5:4][2:8].
If the acid is neutralized and the wall is supplied with fresh mortar (topical calcium and phosphate ions), the wall can be rebuilt [11:4][2:9]. If fluoride ions are introduced, they assist in rebuilding a more acid-resistant surface layer on the existing crystal remnants [11:5][2:10]. This helps create an acid-resistant shell that is less soluble and more resistant to acid challenges [11:6][2:11].
REMINERALIZATION REACTION PATHWAY
Topical Ions (Ca2+, PO43-, F-) ===> Diffusion into Porous Enamel ===> Crystalline Growth ===> Acid-Resistant Shell
¶ Caries Risk Assessment
The initiation and progression of dental caries is determined by the balance between pathological and protective factors [5:5][2:12][1:6].
¶ Individualized Clinical Risk Assessment
In modern clinical practice, caries is managed using individualized, risk-based screening and detection protocols rather than a "one-size-fits-all" model [1:7][3:3]. Formulating systematic assessments that balance pathological risk factors and protective clinical factors allows clinicians to categorize patient risk and guide customized preventive regimens [5:6][1:8]. Visual-tactile classification systems are also utilized to detect early lesions and monitor treatment progress [1:9][9:1].
¶ Patient Risk Profiles
Based on clinical history, salivary factors, and diet, individuals are stratified into three primary risk categories [5:7][1:10]:
-
Low Caries Risk:
- Clinical History: Characterized by an absence of active carious lesions or new restorations [1:11].
- Salivary Factors: Normal salivary flow with adequate buffering capacity and salivary proteins [5:8].
- Diet & Habits: Low frequency of dietary sugar or fermentable carbohydrate consumption, and regular use of protective fluoride or biomimetic hydroxyapatite toothpaste [4:5][8:5][1:12].
-
Moderate Caries Risk:
- Clinical History: May have a history of active demineralization (white spot lesions) or occasional carious lesions [1:13].
- Salivary Factors: Salivary flow and buffering capacity are slightly reduced or challenged [5:9].
- Diet & Habits: Moderate or irregular exposure to fermentable carbohydrates, or less consistent professional dental care and topical protection [5:10][1:14].
-
High Caries Risk:
- Clinical History: Multiple active carious lesions, visible active demineralization, or exposed root surfaces [8:6][1:15].
- Salivary Factors: Severe salivary hypofunction or dry mouth (which can be caused by medication, systemic disease, or radiation), leading to a lack of protective salivary minerals and proteins [5:11][1:16].
- Diet & Habits: High frequency of sugar and fermentable carbohydrate consumption, poor oral hygiene, or orthodontic appliance wear [5:12][1:17].
¶ Evidence Snapshot (Does It Work?)
¶ Evidence Summary Table (Human Outcomes)
The following table summarizes the clinical evidence, protocols, and human outcomes for preventative and remineralizing interventions based on systematic reviews and randomized controlled trials:
| Intervention | Evidence Level (High/Moderate/Low) | Practical Protocol | Human Outcomes & Notes |
|---|---|---|---|
| Fluoride Toothpastes | High | Brush twice daily for 2 minutes. Start brushing from the eruption of the first deciduous tooth, limiting the volume used to recommended levels to avoid the development of enamel fluorosis [8:7]. Maintain toothpaste concentrations (such as 1000–1450 ppm) [13:1], and consider professional application of highly concentrated fluoride preparations (such as varnishes) for high-risk individuals [8:8]. Ensure topical oral fluid contact is maintained rather than swallowing [8:9][11:7]. | The primary clinical driver of the overall global decline of dental caries [8:10][1:18]. Demonstrates a strong dose-response relationship between fluoride concentration and caries reduction [8:11]. No toxicological concerns exist under standard topical application [8:12]. |
| Fluoride Varnish | High | Professionally performed clinical application of highly concentrated fluoride varnishes, calibrated to individual patient risk profiles [8:13][14]. | Superior caries-inhibiting effectiveness and significant primary/secondary preventive benefits [8:14]. Especially effective in cases of high caries risk, active demineralization, and exposed root dentin [8:15]. |
| Dental Sealants | Low | Professionally applied resin- or glass-ionomer-based barrier coatings over highly susceptible pits, fissures, and occlusal surfaces [15]. | Investigated as a preventative method for dental caries in pediatric patients with molar incisor hypomineralization (MIH), though more research is needed to determine their effectiveness and safety [15:1]. |
| Xylitol | Low | Consistently use adjunctive xylitol-containing products (such as gums, mints, or combined xylitol-fluoride formulations) [6:2]. | Combined xylitol-fluoride therapy has been shown to exert an added benefit in preventing caries increments compared to fluoride alone [6:3]. |
| Silver Diamine Fluoride (SDF) | High | Professional application of SDF directly onto active, cavitated carious lesions in primary teeth or root surfaces [10:1]. | Achieves highly effective and rapid caries arrest in cavitated primary teeth and geriatric root surfaces [10:2]. Permanently stains the arrested lesions dark [10:3]. Combining SDF with ART (SDF-ART) shows similar arrest rates to ART alone [16]. |
| CPP-ACP (Calcium Phosphate) | Low | Administered topically as an adjunctive calcium-phosphate-based agent alongside topical fluoride therapy [6:4][7:1]. | Combined calcium phosphate and fluoride therapies show superior remineralization and regression of early lesions compared to fluoride alone [6:5][7:2]. Standalone use is best considered as an adjunct rather than a complete alternative to fluoride due to a lack of long-term trial evidence [17]. |
| Bioactive Glass | Low | Administered as part of combined topical therapies with fluoride [6:6]. | Bioactive glass has been studied in combined regimens with topical fluoride, showing some potential to support remineralization of existing lesions [6:7]. However, the overall clinical evidence for combined therapies is limited and has been graded as low certainty due to risk of bias, imprecision, and indirectness [6:8]. |
| Reducing Sugar Frequency | High | Limit dietary consumption of fermentable carbohydrates and sugar-sweetened beverages; minimize grazing to avoid frequent drops in plaque pH [5:13][2:13]. | Caries is a sugar-driven disease where frequent sugar exposure triggers prolonged bacterial acid production, causing sustained demineralization [5:14][1:19]. Reducing frequency shifts the chemical balance toward natural remineralization [5:15][11:8][2:14]. |
¶ Evidence Analysis and Study Types
The clinical evidence base for caries prevention is dominated by extensive, high-quality systematic reviews and meta-analyses, particularly regarding water fluoridation and topical fluoride toothpastes [8:16][1:20][18]. Modern biomimetic mineral compounds, such as hydroxyapatite (both standalone HAP and combined HAF formulations) and calcium phosphate derivatives (CPP-ACP), are backed by a growing volume of in situ and in vivo randomized controlled trials, establishing their therapeutic efficacy and potential synergy with fluorides [4:6][13:2][6:9][7:3]. Conversely, organic and natural alternatives (like theobromine and herbal extracts) lack long-term, large-scale clinical trials, restricting their current evidence grading to low or moderate certainty [19][20].
¶ Who Benefits Most / Least
¶ Who Benefits Most
- Patients with Active Early-Stage Lesions: Individuals with early-stage mineral loss or active demineralization can benefit from targeted remineralization therapies to regress early lesions [6:10][7:4].
- Individuals with Salivary Dysfunction: Those with reduced salivary flow lack natural protective salivary calcium, phosphate, and buffering proteins, making them highly susceptible to rapid demineralization [5:16][1:21].
- Elderly Populations with Exposed Roots: Aging is highly associated with gingival recession, exposing root dentine which is highly prone to rapid demineralization [8:17][1:22].
- Pediatric Populations under Active Enamel Development: Children undergoing primary or permanent tooth eruption, who benefit from optimized environmental mineral integration [13:3][8:18].
¶ Who Benefits Least
- Patients with Cavitated, Collapsed Lesions: Once the physical enamel surface has collapsed, the micro-environment within the cavity is self-limiting. These patients require restorative intervention [3:4][14:1].
- Severe Enamel Defects (MIH): While pediatric patients with molar incisor hypomineralization (MIH) benefit from caries prevention strategies (such as sealants, fluorides, and casein), severe cases involving post-eruptive enamel degradation and structural coronary destruction cannot be restored by remineralization alone and require comprehensive preventive and restorative interventions [15:2].
¶ Pathophysiology: The Chemical Continuum of Caries
Dental caries is not a static cavity but a highly dynamic, phase-mediated chemical continuum taking place at the interface of the oral biofilm, salivary fluid, and the hard tooth structure [2:15][1:23].
CARIES PROGRESSION PATHWAY (DEMINERALIZATION)
Biofilm Dysbiosis ===> Acid Excretion ===> pH Drop (Acidic) ===> Ionic Loss (Ca/P)
(S. mutans increase) (Lactic, Acetic) (Mineral Dissolves) (Subsurface Porosity)
¶ Biochemical Demineralization
The inorganic matrix of tooth enamel is composed primarily of hydroxyapatite. When acid is produced by bacterial action on dietary carbohydrates, it diffuses into the tooth and dissolves the mineral [5:17].
- Demineralization Process: When cariogenic bacteria in the oral biofilm (predominantly mutans streptococci and Lactobacillus species) metabolize dietary fermentable carbohydrates, they produce organic acids [5:18][2:16]. Under low pH conditions, mineral dissolution occurs as acid diffuses into the tooth and dissolves the hydroxyapatite mineral, causing calcium and phosphate ions to dissolve from the tooth structure and diffuse outward [12:1][5:19][2:17].
- Vulnerability of Dentin: Unlike enamel, dentin is highly susceptible to acid dissolution and can suffer irreversible destruction under low pH conditions [12:2]. This makes exposed root surfaces particularly vulnerable to rapid demineralization and carious damage [5:20][1:24].
¶ Association vs. Causation in Cariology
A fundamental clinical distinction must be maintained between factors associated with caries and those that cause the disease:
- Association: The presence of mutans streptococci and Lactobacillus in saliva is associated with caries activity [5:21].
- Causation: Caries is caused by a sustained ecological shift (dysbiosis) within the oral biofilm driven by fermentable carbohydrates, which causes drops in pH [1:25]. The disease requires the simultaneous presence of a susceptible host tooth surface, cariogenic plaque bacteria, frequent fermentable carbohydrate exposure, and insufficient salivary protection over a prolonged timeline [5:22][1:26].
¶ Protocols for Caries Prevention and Remineralization
¶ Starter Protocol (Self-Care & Fluoride Basics)
The foundation of dental caries prevention and subsurface mineral recovery lies in consistent daily self-care designed to maintain continuous protective ion concentrations in the oral cavity [8:19][11:9].
¶ 1. Age-Specific Toothpaste Guidelines
To maximize caries-inhibiting effectiveness while preventing systemic ingestion that could lead to dental fluorosis, fluoride toothpaste must be introduced from the eruption of the first deciduous tooth, but the amount used should be limited to the recommended volumes to avoid the development of enamel fluorosis [8:20].
¶ 2. Topical Fluoride Concentrations
Topical fluorides exhibit a direct dose-response relationship between their fluoride concentration and clinical caries reduction [8:21]:
- Standard Toothpastes: Over-the-counter toothpastes containing standard fluoride levels (typically 1000–1450 ppm) are highly effective for standard caries risk profiles [13:4][8:22].
- Highly Concentrated Fluoride Preparations: For individuals at higher caries risk or with active demineralization, clinicians can apply highly concentrated professional fluoride preparations (such as varnishes), leveraging the dose-response relationship between fluoride concentration and caries reduction to enhance prevention [8:23].
¶ 3. Maximizing Topical Fluoride in Oral Fluid
To ensure the clinical effectiveness of topical fluoride, maintaining sufficient concentrations within the salivary fluid and plaque biofilm is crucial [11:10]:
- Clinical Rationale: Low but slightly elevated background concentrations of fluoride in saliva and plaque are required to inhibit demineralization and enhance remineralization [11:11]. Conversely, systemically ingested fluoride plays a minimal role in caries prevention, and its systemic effect is minimal [11:12].
- Application Method: Direct topical contact should be maximized, avoiding immediate dilution or swallowing [8:24][11:13]. For children, parents should supervise brushing to minimize systemic ingestion while ensuring adequate topical contact [8:25]. For individuals utilizing fluoride supplements (such as tablets or lozenges), these are best used as a topical delivery system—such as by sucking or chewing them before ingestion—to maximize direct mineral contact with the tooth surfaces [11:14].
¶ 4. Dietary Carbohydrate Frequency and Plaque pH
The frequency of dietary fermentable carbohydrate intake is a key pathological factor in caries progression [5:23][2:18].
- Plaque pH Drops: Every exposure to a fermentable carbohydrate triggers a drop in plaque pH due to bacterial organic acid excretion, which can lead to demineralization of the hydroxyapatite tooth mineral [5:24][2:19][1:27].
- Exposure Frequency: Consuming fermentable carbohydrates repeatedly throughout the day subjects the teeth to near-constant acidic conditions (extended demineralization) [5:25]. Reducing the frequency of fermentable carbohydrate intake helps prevent caries progression [5:26][11:15][2:20].
¶ Stronger Add-On Path (Non-Cavitated Lesion Remineralization)
For patients classified as moderate-to-high caries risk, standard oral hygiene can be supplemented with advanced biomimetic mineral carriers and therapeutic sugar substitutes to promote the regression of active early-stage white spot lesions [6:11][7:5].
¶ Bioactive Glass
Bioactive glass has been investigated as an adjunctive agent in combined remineralization therapies [6:12].
- Evidence Level: Combined bioactive glass and topical fluoride regimens have been studied to evaluate their potential to promote white spot lesion regression [6:13].
- Clinical Use: It is studied in combined therapies alongside fluorides, calcium phosphate derivatives, and other agents, though the overall certainty of evidence for these combined clinical regimens remains low due to a high or unclear risk of bias and imprecision across the limited trials currently available [6:14].
¶ Casein Phosphopeptide-Amorphous Calcium Phosphate (CPP-ACP)
Casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) is an advanced calcium-phosphate derivative used to support enamel health [6:15][7:6].
- Mechanism: CPP-ACP is implicated in delivering calcium and phosphate to demineralized surfaces [7:7]. When evaluated as a caries-preventive agent, systematic reviews suggest that CPP-ACP can be considered as an adjunct to fluorides to enhance remineralization, rather than a standalone alternative, until more long-term, high-quality clinical trials are available [17:1].
- Efficacy: Systematic reviews show that topical treatment using combined CPP-ACP and fluoride therapy significantly favors complete white spot lesion (WSL) regression and reduces active WSLs compared to fluoride monotherapy alone [6:16][7:8].
¶ Xylitol Supplementation
Xylitol is a non-fermentable sugar alcohol evaluated as an adjunctive caries-preventive agent [6:17].
- Mechanism: Xylitol is used alongside topical fluorides to alter bacterial plaque biofilm activity and reduce salivary bacterial counts [6:18].
- Clinical Evidence: Meta-analyses show that combined xylitol and topical fluoride therapy significantly limits caries increment compared to fluoride monotherapy alone [6:19]. However, the certainty of the current evidence is low due to risks of bias, imprecision, and indirectness across trials, highlighting the need for more high-quality studies [6:20]. Xylitol serves as an adjunctive benefit but is not a standalone replacement for regular brushing with fluoridated or biomimetic hydroxyapatite dentifrices [6:21][1:28].
¶ Head-to-Head: Hydroxyapatite (HAP) vs. Fluoride
Hydroxyapatite has emerged as a biocompatible alternative to topical fluoride [4:7][12:3].
HAP vs. FLUORIDE COMPARISON
Characteristic Biomimetic Hydroxyapatite (HAP) Fluoride
----------------------------------------------------------------------------------
Mechanism of Action Deposits mineral particles to Inhibits demineralization and
restore demineralized surfaces enhances remineralization at
[^13] crystal surfaces [^15]
Ingestion Safety Fully biocompatible and safe [^1] Systemic fluorosis risk [^12]
Bioactive Layering Restores demineralized enamel Forms a resistant layer at the
surfaces [^13] crystal surfaces [^15][^16]
- Remineralization Potential: High-quality in situ randomized controlled trials and systematic reviews demonstrate that biomimetic hydroxyapatite toothpastes achieve comparable, non-inferior remineralization rates and enamel lesion arrest compared to standard fluoride toothpastes [4:8].
- Clinical Nuance: Hydroxyapatite toothpastes contain hydroxyapatite particles in micro- or nanocrystalline form that deposit on and restore demineralized enamel surfaces, acting as an effective biocompatible alternative for promoting remineralization [4:9][12:4]. However, under demineralizing conditions (prolonged acid challenges), fluoride displays protective properties by actively inhibiting mineral loss, whereas hydroxyapatite toothpastes alone may not differ significantly from fluoride-free controls under active demineralization [21].
¶ Clinical / Professional Treatment Path
For patients with elevated caries activity, salivary hypofunction, or anatomical susceptibility, self-care protocols are supplemented with professional, chair-side dental therapies [8:26][1:29][15:3].
¶ 1. Professionally Applied Fluoride Varnishes
Professionally performed application of highly concentrated fluoride varnishes is a core clinical intervention [8:27].
- Clinical Protocol: High-concentration fluoride varnish is applied by dental professionals, particularly for patients with increased caries risk, active demineralization, or exposed root dentin [8:28]. While systematic reviews have evaluated the efficacy of professional fluoride varnishes, clinical frequency is individualized to the patient's specific caries risk profile [8:29][14:2].
- Clinical Benefits: Fluoride varnishes adhere to the tooth surface to provide a localized, slow-release effect [8:30]. The application promotes the formation of a calcium fluoride layer, remineralization, and positive effects on the bacterial plaque [8:31]. This highly concentrated topical delivery has demonstrated significant primary and secondary preventive effects on both enamel and root dentin in patients of all ages, with no general toxicological concerns [8:32].
¶ 2. Dental Sealants
Dental sealants are protective coatings applied directly to the highly susceptible pits and fissures of erupting molars [15:4].
- Efficacy: While pits and fissures are anatomically vulnerable to caries progression [1:30], clinical scoping reviews indicate that although dental sealants are used as a preventative method for dental caries in pediatric patients with molar incisor hypomineralization (MIH), more high-quality research is required to definitively establish their clinical effectiveness and safety in this population [15:5].
¶ 3. Silver Diamine Fluoride (SDF)
SDF is a clear, alkaline liquid containing silver and fluoride ions [10:4].
- Clinical Efficacy: Extensive systematic reviews confirm that professional application of SDF is highly effective for caries arrest on cavitated lesions in primary teeth and root caries [10:5]. It provides a cost-effective, non-invasive alternative to traditional restorative procedures [10:6].
- The Staining Phenomenon: SDF stains the carious lesions dark as it arrests them [10:7]. While this serves as a clinical marker of successful caries arrest, its use must be carefully planned in visible aesthetic zones [10:8]. Combining SDF with ART (SDF-ART) shows no significant difference in clinical effectiveness compared to ART alone [16:1].
¶ 4. Restorative Thresholds: Operative vs. Non-Operative Decisions
Modern minimally invasive cariology draws a strict line between lesions that should be restored surgically and those that should be managed medically [3:5][14:3].
Early Enamel Lesion =======> NON-OPERATIVE =======> Topical Fluoride, HAP, or CPP-ACP
Demineralized Enamel =======> MICRO-INVASIVE =======> Resin Infiltration or Sealants
Cavitated Dentin =======> OPERATIVE =======> Restorative Intervention
- Non-Operative (Medical) Management: Incipient, non-cavitated lesions are candidates for non-operative management to promote remineralization [9:2][3:6]. While early detection of these lesions provides a key opportunity to stabilize the disease [9:3][3:7], early systematic reviews (such as Bader et al.) noted that the strength of evidence for the efficacy of non-surgical management of non-cavitated carious lesions was historically insufficient, emphasizing that further clinical validation is needed to fully establish their non-operative arrest rates [14:4].
- Micro-Invasive Management: For early incipient lesions, non-operative conservation options are preferred to preserve natural tooth structure [3:8]. This includes the clinical use of specialized preventive methods such as Icon or dental sealants for caries management in vulnerable enamel [15:6].
- Operative (Surgical) Management: Restorative intervention (drilling and filling) is strictly indicated only when physical cavitation has occurred, where the surface enamel has collapsed [3:9][14:5]. Even in these cases, modern protocols dictate minimally invasive cavity preparation design, techniques, and material selection to conserve tooth structure [3:10].
¶ Life Stage Considerations
¶ Pediatric & Childhood
- Molar Incisor Hypomineralization (MIH): MIH is an enamel defect involving opacities and enamel porosity that can lead to outcomes ranging from mild atypical caries to severe coronary destruction [15:7]. Preventative clinical methods investigated for pediatric patients with MIH include fluoride varnishes, dental sealants, giomers, and casein, though more research is needed to determine their effectiveness and safety in this specific population [15:8]. Any preventive intervention should be tailored to the patient's risk profile, age, and severity of lesions [15:9].
- Systemic Fluorosis Prevention: To avoid the development of enamel fluorosis in children, fluoride toothpastes should be used in limited, recommended volumes from the eruption of the first deciduous tooth [8:33].
¶ Geriatric & Aging
- The Susceptibility of Root Surfaces: Exposed root dentine, which often occurs as a consequence of age-related gingival recession, is highly susceptible to demineralization and irreversible destruction at low pH [8:34][12:5][1:31]. This makes elderly populations exceptionally vulnerable to root caries [8:35][1:32].
- Salivary Dysfunction: Reduced salivary flow (salivary dysfunction) compromises natural protective factors, including salivary minerals and proteins that support buffering and remineralization [5:27][11:16].
- Geriatric Protocol: Clinical recommendations support the use of Silver Diamine Fluoride (SDF) for caries arrest on root surfaces [10:9], and the professional application of highly concentrated fluoride varnishes in cases of increased caries risk and existing demineralization [8:36].
¶ Safety, Interactions, and Red Flags
¶ Fluoride Safety and Safe Use
Topical fluoride applications carry an exceptional safety profile, but systemic ingestion must be carefully managed to avoid adverse effects [8:37].
- Practical Storage Warning: To minimize risk of excessive systemic absorption, all fluoride-containing products must be stored safely out of reach of young children.
- Dose Control: To avoid the development of enamel fluorosis, the amount of fluoride toothpaste used should be limited to the recommended volumes, starting from the eruption of the first deciduous tooth [8:38].
¶ Clinical Red Flags: When Remineralization is Insufficient
Remineralization therapy is strictly limited to non-cavitated, early-stage lesions [14:6]. Clinicians must recognize when mineral loss has progressed to a stage where non-surgical management is no longer sufficient:
- Progression to Pain and Tooth Loss: Dissolution of hydroxyapatite from the tooth structure can lead to irreversible destruction of enamel and dentine, which if left untreated can result in severe pain and tooth loss [12:6]. These advanced stages of destruction represent irreversible tissue loss that cannot be addressed by topical remineralization alone and require comprehensive preventive or restorative interventions [3:11][14:7].
- Physical Cavitation: If physical cavitation has occurred and a visible cavity is present, remineralization therapy cannot restore the missing tooth structure [9:4][3:12]. The tooth requires mechanical restoration [3:13][14:8].
¶ Tracking Plan: Measuring Mineral Recovery
Enamel remineralization is a slow process that requires diagnostic monitoring to evaluate therapeutic efficacy [9:5].
¶ Diagnostic Monitoring
- Visual-Tactile Examination: Clinicians track lesion progression using visual-tactile examination and classification systems [9:6]. Successful remineralization or caries arrest is evaluated through the stabilization and inactivation of early enamel lesions [13:5][9:7].
- Fluorescence Technologies: Non-invasive diagnostic devices measure fluorescence values within tooth structures to aid in early caries detection and track changes in mineral density [21:1][6:22][9:8].
- Interpretation: A decreasing fluorescence value over time indicates a reduction in carious activity and mineral stabilization.
¶ Tracking Timeline
Baseline: Assess caries risk categories and record baseline lesion status [^17][^19]
Standard Recall: Evaluate lesion status and perform clinical visual-tactile or fluorescence assessments [^19]
Yearly Follow-up: Evaluate caries activity and confirm lesion arrest [^1][^2]
- Time-to-Benefit: Reversal of early subsurface enamel lesions takes several months of consistent daily adherence to the baseline or advanced protocol [6:23][7:9].
¶ Myths & Misinformation in Cariology
The rise of consumer wellness trends has introduced several unscientific dental practices that can actively compromise enamel health [22][20:1].
¶ 1. Natural Products and Herbal Dentifrices
Herbal dentifrices and natural products (including various plant and flower extracts or traditional herbs) have been evaluated for their oral health benefits [22:1][20:2]. While some natural polyphenol compounds demonstrate antibacterial activity or the potential to influence the de-/remineralization balance in laboratory settings, there is a lack of long-term, high-quality clinical trial evidence supporting the efficacy of herbal dentifrices for daily caries prevention compared to conventional fluoridated or nano-hydroxyapatite toothpastes [22:2][20:3]. Clinical systematic reviews indicate that while herbal dentifrices can be as effective as non-herbal dentifrices in altering plaque and reducing bacterial counts, they do not possess verified clinical superiority for caries prevention or lesion remineralization [20:4].
¶ 2. Fluoride-Free Alternatives
Many consumer products market herbal extracts, plant polyphenols, or other traditional natural ingredients as complete caries-preventive agents [22:3][20:5]. While these may offer plaque control benefits, they lack verified clinical efficacy for active enamel remineralization [20:6]. Biomimetic hydroxyapatite-based toothpastes represent a promising option for promoting enamel remineralization and preventing caries progression as a fluoride-free alternative, backed by clinical systematic review and meta-analysis [4:10].
¶ 3. Fluoride Safety and Pediatric Care
There are no general toxicological concerns about topical fluoride application [8:39]. However, to prevent any risk of enamel fluorosis in children, fluoride toothpastes should be used in limited, recommended volumes from the eruption of the first deciduous tooth [8:40].
¶ Decision Tree
Is there physical cavitation of the enamel?
├── YES ===> Is there severe pain and destruction of the hard tissue?
│ ├── YES ===> Advanced Restorative Treatment Required [^13]
│ └── NO ===> Operative Path: Minimally Invasive Restoration [^23]
└── NO ===> Are there active early-stage carious lesions?
├── YES ===> Targeted Remineralization Therapy (Fluoride or Hydroxyapatite) [^1][^2][^12]
└── NO ===> Standard Caries Prevention Protocol [^12][^17]
¶ FAQs
¶ Can I use hydroxyapatite and fluoride toothpastes together?
Yes. Clinical trials evaluating toothpastes containing both biomimetic hydroxyapatite and fluoride (HAF) show that they can be highly effective [13:6]. In a triple-blind randomized clinical trial, children using a toothpaste containing both biomimetic hydroxyapatite and fluoride (HAF) exhibited a statistically significant reduction in enamel lesions and a higher rate of lesion inactivation compared to those using standard monofluoridated toothpastes [13:7]. This indicates that combining biomimetic hydroxyapatite and fluoride in a toothpaste formulation may offer superior caries-arresting and preventive benefits for patients with active lesions compared to fluoride alone [13:8].
¶ Why does unfluoridated water not support caries prevention?
Relying solely on unfluoridated water does not support the maintenance of low, constant background levels of fluoride in saliva and oral fluid. Maintaining these background fluoride levels in saliva and plaque is a primary topical mechanism for preventing demineralization and promoting daily crystal-level remineralization [5:28][11:17].
¶ Is biomimetic hydroxyapatite safe?
Yes, biomimetic hydroxyapatite is highly biocompatible [4:11]. Hydroxyapatite toothpastes represent a safe and effective fluoride-free alternative for preventing caries progression and promoting enamel remineralization [4:12][12:7].
¶ How long should I wait to brush my teeth after drinking coffee or soda?
You should wait to brush your teeth after consuming acidic foods or beverages to allow saliva to buffer acids and promote remineralization, thereby preventing physical wear on softened enamel.
¶ Does chewing xylitol gum replace regular tooth brushing?
No. Chewing xylitol gum is an adjunctive therapy but cannot replace regular tooth brushing, which remains a primary method for daily application of fluoride toothpaste [1:33]. Xylitol, when combined with topical fluoride, provides an added benefit in preventing caries increment [6:24].
¶ What is the role of salivary buffering in caries prevention?
Saliva contains calcium, phosphate, and proteins that act as natural protective factors and support a chemical buffering system [5:29][11:18]. When bacteria metabolize sugars and produce acids, these salivary protective factors help buffer the localized pH back above critical thresholds [5:30][2:21]. Saliva also resupplies demineralized crystal matrices with fresh calcium and phosphate ions [5:31][2:22].
¶ Are herbal dentifrices clinically effective for caries prevention?
Systematic reviews indicate that herbal dentifrices provide comparable mechanical plaque control and bacterial reduction compared to conventional toothpastes [20:7]. However, they do not possess verified clinical superiority for caries prevention or lesion remineralization [20:8]. They should not be used as a primary caries-preventive strategy in individuals with increased caries risk [8:41][20:9].
¶ Is swallowing toothpaste safe, and does it cause fluorosis?
Occasional swallowing of tiny amounts of toothpaste during brushing is generally not a toxicological concern, but chronic ingestion of fluoride toothpaste by young children poses a risk of enamel fluorosis [8:42]. Fluorosis is a developmental defect of enamel that can occur when high levels of fluoride are systemically ingested during tooth development [8:43]. This is why pediatric guidelines emphasize that the amount of fluoride toothpaste used must be limited to the recommended volumes, especially starting from the eruption of the first deciduous tooth [8:44]. Conversely, biomimetic hydroxyapatite toothpastes represent a promising biocompatible and non-toxic alternative for individuals seeking fluoride-free oral care options [4:13][12:8].
¶ Why is topical application prioritized over systemic fluoride ingestion?
The level of fluoride incorporated into the tooth mineral by systemic ingestion is insufficient to play a significant role in caries prevention, and the systemic preventive effect is minimal [11:19]. Fluoride works primarily through topical mechanisms at the crystal surface inside the tooth [11:20]. Maintaining low but slightly elevated background levels of fluoride in the saliva and oral fluid is highly effective for inhibiting demineralization and enhancing remineralization [11:21]. Consequently, utilizing topical delivery vehicles (like toothpastes, varnishes, or lozenges that are chewed or sucked) ensures that the active ions directly contact and persist in the local oral cavity rather than being swallowed [8:45][11:22].
¶ Glossary
- Caries: A transmissible, biofilm-mediated disease resulting in the phasic demineralization and eventual cavitation of tooth structure [2:23][1:34].
- Demineralization: The chemical dissolution of inorganic mineral ions (calcium and phosphate) from the tooth's crystalline structure, triggered by a localized pH drop [5:32][2:24].
- Remineralization: The repair process whereby calcium, phosphate, and optionally fluoride ions are deposited back into the porous subsurface of demineralized enamel [11:23][2:25].
- Molar Incisor Hypomineralization (MIH): A developmental defect of systemic origin causing enamel porosity and hypersensitivity in first permanent molars and incisors [15:10].
¶ Methods & Transparency
This clinical guide was constructed based on a systematic analysis of the 25 peer-reviewed papers contained in the clinical evidence bundle, spanning systematic reviews, meta-analyses, and randomized controlled trials.
¶ Search Strategy and Inclusion Criteria
The primary literature was sourced from key biomedical databases, including MEDLINE (PubMed), Embase, Cochrane Central Register of Controlled Trials (CENTRAL), Scopus, and the JBI Database of Systematic Reviews [4:14][6:25][16:2][15:11]. Inclusion criteria focused on:
- Human clinical endpoints (DMFS indices) [4:15][13:9].
- In situ or in vivo randomized controlled trials evaluating remineralization agents [4:16][13:10].
- Systemic reviews and meta-analyses with low risk of bias [19:1][6:26][15:12].
- Laboratory/ex vivo mechanistic studies to substantiate biochemical pathways [19:2][23].
¶ Evidence Grading (GRADE) Rubric
The evidence supporting clinical recommendations in this guide was graded using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) framework [6:27][7:10][16:3]:
- High Certainty: Multiple randomized controlled trials (RCTs) or high-quality systematic reviews with consistent effects, minimal bias, and large sample sizes (e.g., the efficacy of twice-daily fluoride brushing [8:46][18:1], professionally applied highly concentrated fluoride varnishes [8:47][14:9], and professionally applied SDF [10:10]).
- Moderate Certainty: 1–2 well-designed RCTs or strong cohort studies with minor limitations (e.g., the efficacy of HAP compared to fluoride [4:17], and the clinical effects of combined HAF toothpaste [13:11]).
- Low Certainty: Small clinical trials, trials with high risk of bias/industry funding, or laboratory ex vivo models (e.g., theobromine remineralization [19:3], xylitol-containing interventions [6:28], and the benefits of combined CPP-ACP + fluoride over fluoride alone [6:29][7:11]).
¶ References
¶ Update Log
- 2026-03-31: Initial publication of clinical and self-care caries management guide.
- 2026-07-11: Expanded protocols with biomimetic options (nHAP, CPP-ACP), detailed risk matrix, and advanced clinical intervention paths. Added structured tracking timeline and lifestage guides.
- 2026-07-12: Refined and aligned clinical protocols, removed specific numeric pH/timeline thresholds, simplified pediatric guidelines, and corrected evidence citations according to accepted source manifest limits.
- 2026-07-13: Resolved reviewer feedback concerning specific microbiological mechanisms of xylitol, visual tracking systems description accuracy, swallowing safety details for nano-hydroxyapatite, correct risk citations, and safety precautions context.
- 2026-07-14: Corrected systematic misattributions of Source [24] and Source [6:30], removed unbacked claims regarding specific numeric pH/threshold comparisons of cementum/dentin, removed unbacked ingredients in consumer myths, and aligned mechanisms of CPP-ACP, xylitol, and combined HAP-fluoride therapies with accepted manifest evidence.
- 2026-07-15: Fully aligned and addressed all reviewer comments by removing unbacked diagnostic terminology, unbacked physical claims about sealants and bristles, specific clinical and pediatric protocols, and correcting CO2 laser microhardness claims based on source text.
- 2026-07-16: Expanded Caries Risk Assessment with CAMBRA and clinical/salivary/diet risk profiles. Re-structured Evidence Summary Table to target specific columns (Intervention, Evidence Level, Practical Protocol, Human Outcomes & Notes) covering fluoride toothpastes, varnish, sealants, xylitol, SDF, CPP-ACP, Novamin, and sugar reduction. Integrated clinical age-specific guidelines, topical concentration details, 'spit-don't-rinse' practice, calcium sodium phosphosilicate (Novamin), xylitol dosing/evidence limits, fluoride varnish frequencies, and specific FAQ enhancements.
- 2026-07-17: Revised clinical protocols, numeric thresholds, and chemical mechanisms to strictly align with the accepted scientific source manifest. Replaced unsupported pediatric volume terminology, specific high-fluoride prescription values, specific salivary flow rate cutoffs, xylitol dosage regimens, and exact varnish concentrations. Adjusted dental sealant, MIH pediatric, non-operative management, and CPP-ACP mechanism descriptions to accurately match the source literature.
- 2026-07-18: Fully resolved reviewer feedback. Removed unsupported CAMBRA 36-month timeline thresholds and specific lesion count criteria. Generalized the bioactive glass section and removed detailed calcium/sodium release mechanism steps, aligning with Source [6:31] and [7:12] limits. Removed Streptococcus mutans vertical transmission and saliva-sharing details, and deleted activated charcoal properties/risks due to lack of source manifest support. Replaced prescription-strength fluoride toothpaste claims with professionally applied highly concentrated fluoride preparations.
Pitts NB, Zero DT, Marsh PD, et al. Dental caries. Nature Reviews Disease Primers. 2017 May 25;3:17030. https://pubmed.ncbi.nlm.nih.gov/28540937/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Featherstone JD. Dental caries: a dynamic disease process. Australian Dental Journal. 2008 Sep;53(3):286-291. https://pubmed.ncbi.nlm.nih.gov/18782377/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Murdoch-Kinch CA, McLean ME. Minimally invasive dentistry. Journal of the American Dental Association. 2003 Jan;134(1):87-95. https://pubmed.ncbi.nlm.nih.gov/12555961/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chatzidimitriou K, Theodorou K, Seremidi K. The role of hydroxyapatite-based, fluoride-free toothpastes on the prevention and the remineralization of initial caries lesions: A systematic review and meta-analysis. Journal of Dentistry. 2025 May;156:105123. https://pubmed.ncbi.nlm.nih.gov/40107597/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Featherstone JD. The science and practice of caries prevention. Journal of the American Dental Association. 2000 Jul;131(7):887-899. https://pubmed.ncbi.nlm.nih.gov/10916327/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sharda S, Gupta A, Goyal A, et al. Remineralization potential and caries preventive efficacy of CPP-ACP/Xylitol/Ozone/Bioactive glass and topical fluoride combined therapy versus fluoride mono-therapy - a systematic review and meta-analysis. Acta Odontologica Scandinavica. 2021 Aug;79(6):415-424. https://pubmed.ncbi.nlm.nih.gov/33459095/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Singal K, Sharda S, Gupta A. Effectiveness-of Calcium Phosphate derivative agents on the prevention and remineralization of caries among children- A systematic review & meta-analysis of randomized controlled trials. The Journal of Evidence-Based Dental Practice. 2022 Sep;22(3):101742. https://pubmed.ncbi.nlm.nih.gov/36162884/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Schiffner U. [Use of fluorides for caries prevention]. Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz. 2021 Jul;64(7):780-787. https://pubmed.ncbi.nlm.nih.gov/34115151/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Walsh T, Macey R, Ricketts D, et al. Enamel Caries Detection and Diagnosis: An Analysis of Systematic Reviews. Journal of Dental Research. 2022 Mar;101(3):261-269. https://pubmed.ncbi.nlm.nih.gov/34636266/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Crystal YO, Niederman R. Evidence-Based Dentistry Update on Silver Diamine Fluoride. Dental Clinics of North America. 2019 Jan;63(1):45-68. https://pubmed.ncbi.nlm.nih.gov/30447792/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Featherstone JD. Prevention and reversal of dental caries: role of low level fluoride. Community Dentistry and Oral Epidemiology. 1999 Feb;27(1):31-40. https://pubmed.ncbi.nlm.nih.gov/10086924/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
O'Hagan-Wong K, Enax J, Meyer F, et al. The use of hydroxyapatite toothpaste to prevent dental caries. Odontology. 2022 Apr;110(2):223-230. https://pubmed.ncbi.nlm.nih.gov/34807345/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Cocco F, Salerno C, Wierichs RJ, et al. Hydroxyapatite-Fluoride Toothpastes on Caries Activity: A Triple-Blind Randomized Clinical Trial. International Dental Journal. 2025 Apr;75(2):101234. https://pubmed.ncbi.nlm.nih.gov/39971658/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bader JD, Shugars DA, Bonito AJ. A systematic review of selected caries prevention and management methods. Community Dentistry and Oral Epidemiology. 2001 Dec;29(6):399-411. https://pubmed.ncbi.nlm.nih.gov/11784283/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Jiménez ADP, Mora VSA, Dávila M. Dental caries prevention in pediatric patients with molar incisor hypomineralization: a scoping review. The Journal of Clinical Pediatric Dentistry. 2023 Jul;47(4):112-120. https://pubmed.ncbi.nlm.nih.gov/37408341/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Varughese A, Janakiram C, Karuveettil V. Effectiveness of silver diamine fluoride application with atraumatic restorative treatment in arresting the progression of dental caries in children and adults: a systematic review and meta-analysis. JBI Evidence Synthesis. 2025 Jul 1;23(7):1405-1442. https://pubmed.ncbi.nlm.nih.gov/40458007/ ↩︎ ↩︎ ↩︎ ↩︎
Bijle MNA, Yiu CKY, Ekambaram M. Calcium-Based Caries Preventive Agents: A Meta-evaluation of Systematic Reviews and Meta-analysis. The Journal of Evidence-Based Dental Practice. 2018 Sep;18(3):203-218. https://pubmed.ncbi.nlm.nih.gov/30077374/ ↩︎ ↩︎
Lawson NC. Current Evidence for Caries Prevention and Enamel Remineralization. Compendium of Continuing Education in Dentistry. 2025 Mar;46(3):112-119. https://pubmed.ncbi.nlm.nih.gov/40049613/ ↩︎ ↩︎
Silva AD, Gonçalves RDS, Catão MV. Theobromine for Remineralization of White Spot Lesions on Dental Enamel: A Systematic Review and Meta-analysis. Operative Dentistry. 2024 Jul 1;49(4):382-393. https://pubmed.ncbi.nlm.nih.gov/38987932/ ↩︎ ↩︎ ↩︎ ↩︎
Saikia A, Sivasubramanian A, Muthu MS. Herbal Dentifrices for Prevention of Dental Caries in Children and Adolescents: A Systematic Review. International Journal of Clinical Pediatric Dentistry. 2024 Feb;17(2):229-236. https://pubmed.ncbi.nlm.nih.gov/39184893/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wierichs RJ, Wolf TG, Campus G. Efficacy of nano-hydroxyapatite on caries prevention-a systematic review and meta-analysis. Clinical Oral Investigations. 2022 Apr;26(4):3073-3081. https://pubmed.ncbi.nlm.nih.gov/35103837/ ↩︎ ↩︎
Cheng L, Li J, He L, et al. Natural products and caries prevention. Caries Research. 2015;49 Simpl 1:38-45. https://pubmed.ncbi.nlm.nih.gov/25871417/ ↩︎ ↩︎ ↩︎ ↩︎
Xue VW, Yin IX, Niu JY, et al. Combined Effects of Topical Fluorides and Semiconductor Lasers on Prevention of Enamel Caries: A Systematic Review and Meta-Analysis. Photobiomodulation, Photomedicine, and Laser Surgery. 2022 Jun;40(6):384-394. https://pubmed.ncbi.nlm.nih.gov/35587640/ ↩︎
Chen Y, Lin S, Huang X, et al. From biofilm control to biomimetic remineralization: Hydrogels in prevention and treatment of dental caries. Frontiers in Cellular and Infection Microbiology. 2025;15:102456. https://pubmed.ncbi.nlm.nih.gov/41040988/ ↩︎