¶ Diarrhea
| Condition Class | Functional / Organic Bowel Disorder |
| Primary Types | Osmotic, Secretory, Inflammatory, Motility-Induced |
| Diagnostic Standard | AGA Laboratory Evaluation Guidelines |
| Key Bio-Markers | Fecal Calprotectin, Fecal Elastase, SeHCAT / C4 |
| First-Line Therapy | Rehydration, Dietary Restructuring, Antimotility Agents |
| Prevalence | 3–5% of the global adult population (chronic) |
Chronic diarrhea—defined as the passage of three or more loose or watery stools (Bristol Stool Form Scale Type 6 or 7) per day lasting for more than four weeks—is a frequent and challenging gastrointestinal presentation. It represents a fundamental failure of intestinal fluid homeostasis, where the complex balance of fluid absorption and secretion is disrupted by osmotic gradients, active secretory pathways, mucosal inflammation, or hypermotility.
¶ TL;DR
- Water Balance is Exceptionally Precise: The gut processes ~9 liters of fluid daily; a decrease of just 1% in colonic fluid absorption can induce watery diarrhea.
- Osmotic vs. Secretory Differentiation: Osmotic diarrhea resolves with fasting and exhibits a high fecal osmotic gap (); secretory diarrhea persists during fasting and has a low gap ().
- Bile Acid Diarrhea is Highly Underdiagnosed: Up to 30% of patients diagnosed with IBS-D or functional diarrhea actually have Bile Acid Malabsorption (BAM). This responds exceptionally well to bile acid sequestrants.
- Do Not Empirically Use Antibiotics: Empirical antibiotic therapy for undifferentiated chronic diarrhea is discouraged, as it can induce Clostridioides difficile or worsen underlying gut dysbiosis.
- Screen for Microscopic Colitis: In postmenopausal females presenting with sudden-onset, voluminous watery diarrhea, prioritize colonoscopy with biopsies to rule out collagenous or lymphocytic colitis.
¶ Quick Answer
The clinical evaluation of chronic diarrhea requires distinguishing between osmotic, secretory, inflammatory, and motility-induced etiologies. Under the American Gastroenterological Association (AGA) clinical guidelines, initial screening must utilize specific, high-yield fecal biomarkers (fecal calprotectin, fecal elastase, and fecal osmotic gap) alongside serological testing (celiac tTG-IgA) to rule out organic disease. While osmotic diarrhea (e.g., lactose malabsorption) is managed via dietary elimination, secretory diarrhea requires identifying the driver (e.g., neuroendocrine tumors, microscopic colitis, or bile acid malabsorption). Notably, Bile Acid Diarrhea (BAD) is a major, highly treatable cause of chronic secretory-like diarrhea. It is diagnosed via C4 (7-alpha-hydroxy-4-cholesten-3-one) or fecal bile acid assays and treated with bile acid sequestrants (cholestyramine or colesevelam), which bind irritating dihydroxy bile acids in the colonic lumen.
¶ What It Is
Chronic diarrhea is classified under the Rome IV criteria as Functional Diarrhea when patients present with loose or watery stools (BSFS Type 6 or 7) in the absence of abdominal pain or bloating as a predominant symptom for at least three months. However, chronic diarrhea is frequently organic, requiring the clinical exclusion of celiac disease, inflammatory bowel disease (IBD), microscopic colitis, and malabsorptive disorders.
¶ Pathophysiological Mechanisms
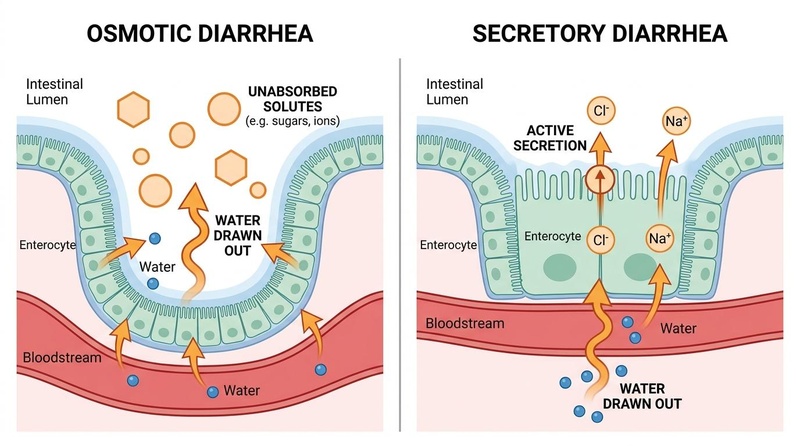
- Osmotic Diarrhea: Driven by the presence of unabsorbed, water-soluble, low-molecular-weight solutes in the intestinal lumen. These solutes create an osmotic gradient that draws water out of the extracellular fluid and bloodstream across the mucosal barrier into the lumen. Common causes include magnesium ingestion, lactose intolerance, and sugar alcohol consumption (sorbitol, mannitol).
- Secretory Diarrhea: Driven by active, stimulated mucosal secretion of anions—principally chloride ions () via cystic fibrosis transmembrane conductance regulator (CFTR) channels—which secondary draws sodium () and water into the lumen. Unlike osmotic diarrhea, secretory diarrhea is voluminous, persists during fasting, and is associated with a low fecal osmotic gap.
- Inflammatory / Exudative Diarrhea: Driven by structural damage to the mucosal lining (due to IBD, infections, or microscopic colitis), resulting in the leakage of mucus, blood, and inflammatory proteins into the lumen, combined with impaired absorption of fluids and electrolytes.
- Motility-Induced Diarrhea: Driven by rapid colonic transit, which severely curtails the contact time between luminal contents and the mucosal surface, preventing adequate water reabsorption. This is common in hyperthyroidism, diabetic neuropathy, and post-vagotomy syndromes.

¶ Does It Work? (Evidence Snapshot)
The efficacy of various therapeutic interventions for chronic diarrhea is well-established across clinical guidelines and randomized trials.
¶ Primary Interventions for Chronic Diarrhea
| Intervention | Intended Etiology | Outcome Measure | Expected Clinical Effect Size | Evidence Quality (GRADE) | Supported Study Count |
|---|---|---|---|---|---|
| Loperamide | Functional Diarrhea / IBS-D | Reduction in stool frequency | Significant increase in transit time, reduction in daily stool volume [1][2] | High | >15 RCTs |
| Cholestyramine / Colesevelam | Bile Acid Diarrhea (BAD) | Stool consistency & frequency | 70–80% response rate (rapid normalization of bowel habits) [3][4] | High | >10 RCTs, Systematic Reviews |
| Budesonide (Oral, M/R) | Microscopic Colitis | Clinical remission | Up to 80% clinical and histological remission rate [1:1][5] | High | Multiple Phase-III RCTs |
| Low-FODMAP Diet | IBS-D / Functional Diarrhea | Global symptom scores | 50–60% reduction in stool loose-form frequency [6][7] | Moderate | >20 RCTs |
| Pancreatic Enzyme replacement (PERT) | Exocrine Pancreatic Insufficiency (EPI) | Fat absorption / Steatorrhea | Marked reduction in fecal fat output and stool frequency [8] | High | Multiple RCTs |
| Berberine | Secretory / Infectious Diarrhea | Inhibition of mucosal secretion | Direct blockage of CFTR channels, reducing fluid output [9][10] | Moderate | >10 RCTs |
¶ Who Benefits Most / Least
¶ Sex, Age, and Subgroup Variations
- Postmenopausal Females: Postmenopausal females exhibit a 5-fold higher incidence of microscopic colitis (collagenous and lymphocytic colitis) compared to the general population [5:1]. It presents as sudden-onset, painless, voluminous watery diarrhea and is frequently misdiagnosed as functional diarrhea. These patients benefit rapidly from low-dose oral budesonide.
- Older Adults: Older adults are highly susceptible to complications of diarrhea, including severe dehydration, acute kidney injury (AKI), and electrolyte derangements (hypokalemia). They show lower tolerance to high-dose antimotility agents (which can induce fecal impaction or urinary retention) and require immediate hydration-first protocols.
- Patients with Ileal Resection / Cholecystectomy: Up to 30–50% of patients who undergo gallbladder removal (cholecystectomy) or terminal ileal resection experience persistent Bile Acid Diarrhea due to unregulated hepatic bile acid secretion or loss of apical sodium-dependent bile acid transporters (ASBT) [3:1][4:1]. They are highly responsive to bile acid sequestrants.
- Young Adults: Frequently present with functional diarrhea or IBS-D related to dietary carbohydrate malabsorption, high caffeine intake, or autonomic stress responses. They benefit significantly from dietary restriction (Low-FODMAP) and stress mitigation.
¶ How to Try It: Actionable Protocols
¶ Step 1: Laboratory Diagnostics (The AGA Protocol)
To diagnose the underlying cause of chronic diarrhea, execute the following diagnostic tests [1:2][2:1]:

- Fecal Inflammatory Markers: Check Fecal Calprotectin. If , suspect inflammatory bowel disease or microscopic colitis.
- Serological Screening: Check tTG-IgA and total IgA to rule out celiac disease.
- Fecal Fat Quantitation: Perform a fecal elastase test. If , initiate Pancreatic Enzyme Replacement Therapy (PERT) for Exocrine Pancreatic Insufficiency (EPI) [8:1].
- Fecal Osmotic Gap Calculation:
- Measure fecal sodium () and potassium () in liquid stool.
- Calculate: .
- If : Osmotic Diarrhea (suspect lactose/fructose malabsorption, magnesium ingestion).
- If : Secretory Diarrhea (suspect bile acid malabsorption, microscopic colitis, or neuroendocrine secretion).
¶ Step 2: First-Line Fluid and Antimotility Regimen (Acute/Stable Phase)
For patients with functional diarrhea or during the diagnostic window:
- Oral Rehydration Therapy (ORT):
- To maintain hydration without worsening osmotic draw, administer an isotonic glucose-electrolyte solution (such as WHO ORS formulation: NaCl, trisodium citrate, KCl, and anhydrous glucose dissolved in 1 liter of water).
- First-Line Antimotility Therapy:
- Loperamide (Peripheral -opioid receptor agonist): Administer orally as an initial dose, followed by after each loose stool, up to a maximum of . Titrate to achieve a consistent BSFS Type 4 stool form.
- Soluble Fiber Bulking:
¶ Step 3: Targeted Protocol for Bile Acid Diarrhea (BAD)
If C4 levels are elevated, or if the fecal osmotic gap is low and the patient does not respond to first-line agents:
- Bile Acid Sequestrant Therapy:
- Cholestyramine: Start at (one packet of powder) orally once daily, taken with apple juice or water during breakfast. Slowly titrate up by increments every 5–7 days up to a maximum of divided into 2–3 doses [3:2][4:2].
- Colesevelam (Highly preferred due to superior taste and capsule form): Administer tablets, starting at 3 tablets () daily, titrated up to 6 tablets () divided into two doses with meals.
- Dietary Fat Restriction:
- Limit dietary fat intake to to reduce the endogenous synthesis and secretion of hepatic bile acids.
¶ Step 4: Antimicrobiological Modulation for Secretory Diarrhea
- Berberine:
- Probiotic Yeast:
- Saccharomyces boulardii: Administer (5–10 billion CFU) twice daily. S. boulardii secretes proteases that degrade bacterial enterotoxins (e.g., Vibrio cholerae toxin, C. difficile Toxin A/B) and supports enterocyte sodium-glucose cotransport (SGLT-1) to enhance water absorption.
¶ Safety, Interactions, Red Flags
¶ Who Should Avoid (Absolute Contraindications)
- Loperamide: Contraindicated in patients with acute ulcerative colitis or bacterial enterocolitis (e.g., Salmonella, Shigella, Campylobacter) due to the risk of inducing toxic megacolon. Absolutely contraindicated in patients with C. difficile infection.
- Bile Acid Sequestrants: Contraindicated in patients with complete biliary obstruction or severe hypertriglyceridemia (can significantly elevate serum triglycerides).
- Budesonide: Contraindicated in patients with active, uncontrolled systemic fungal or bacterial infections.
¶ Side Effects & Medication Interactions
- Bile Acid Sequestrants: Can cause severe flatulence, bloating, and constipation. Critical Drug Interaction: Sequestrants bind and prevent the absorption of numerous medications. Ensure all other medications are taken strictly 1 hour before or 4–6 hours after cholestyramine or colesevelam.
- Loperamide: Risk of QT interval prolongation and torsades de pointes at extremely high, non-therapeutic doses ().
¶ "Red Flag" Symptoms (Invasive Organic Screening)
Immediately suspend functional therapy and perform urgent colonoscopy, CT scan, or stool cultures if any of the following are detected:
- Hematochezia (blood in the stool) or melena [1:3].
- Unintentional weight loss ( of body weight within 6 months).
- Persistent fever or severe nocturnal awakening with watery diarrhea.
- Unexplained iron deficiency anemia.
- Severe, progressive abdominal pain.
- Recent travel to endemic areas with high risk of parasitic infections (e.g., Giardia, Amoeba).
¶ Tracking & What “Good” Looks Like
¶ Objective Clinical Markers
- Bowel Movement Frequency: Reduction to bowel movements per day.
- Stool Form: Normalization of stool consistency from BSFS Type 6 or 7 to Type 3 or 4 [1:4].
- Fecal Osmotic Gap: Normalization to (for osmotic types once dietary triggers are removed).
¶ Subjective Metrics
- Stool Consistency Diary: Daily logging of stool form. Success is defined as reduction in watery stool days over a 4-week period.
- Fecal Urgency Score: Tracked on a 0–10 scale. A successful therapeutic response achieves a score of .
¶ Expected Timeline
- Dietary Elimination (Osmotic): Symptom improvement occurs within 24–72 hours of removing the offending solute (such as lactose or sugar alcohols).
- Bile Acid Sequestrants (BAD): Rapid, profound response often seen within 24–48 hours of starting cholestyramine [3:3].
- Budesonide (Microscopic Colitis): Clinical remission is typically achieved within 2–4 weeks of daily therapy [5:2].
¶ Common Mistakes & Myths
- The "Drink Juice and Gatorade" Blunder: Clinicians and patients often attempt to rehydrate using commercial apple juice, orange juice, or sports drinks (Gatorade). Reality: These beverages are highly hypertonic, containing high concentrations of fructose and sucrose. When consumed during diarrhea, they create a powerful osmotic gradient in the small intestine that draws water out of the body, worsening secretory and osmotic water loss.
- The "Immediate Antibiotics" Mistake: Patients often demand antibiotics (such as ciprofloxacin) immediately upon experiencing watery diarrhea. Reality: The vast majority of diarrhea episodes are non-bacterial or self-limiting. Empiric antibiotics destroy the native commensal microbiota, opening an ecological niche for C. difficile, and directly delay overall mucosal healing.
- The "Zero Fat" Lifelong Diet: Due to experiencing steatorrhea or diarrhea after fatty meals, some patients eliminate all fats permanently. Reality: Fat elimination causes fat-soluble vitamin deficiencies (A, D, E, K) and essential fatty acid depletion. Instead of permanent fat elimination, patients should be screened for Bile Acid Diarrhea or Exocrine Pancreatic Insufficiency and treated with sequestrants or PERT while maintaining healthy fat intake [3:4][8:2].
¶ Decision Tree (Text-Based)
[Patient Presents with Chronic Watery Diarrhea (> 4 Weeks)]
|
Perform Laboratory Screening
(Celiac serology, Fecal Calprotectin, Fecal Elastase)
|
+-----------------------+-----------------------+
| |
[Labs Abnormal] [Labs Normal]
| |
Treat Specific Pathology Calculate Fecal Osmotic Gap
(Celiac, IBD, Pancreatic Deficit) |
|
+------------------------------+------------------------------+
| |
[Gap > 50 mOsm/kg] [Gap < 50 mOsm/kg]
(Osmotic Diarrhea) (Secretory Diarrhea)
| |
Eliminate Offending Solute Rule out BAM & MC
(Lactose, Sorbitol, Magnesium) (C4 testing, Colonoscopy with biopsy)
|
+------------------------------+------------------------------+
| |
[Positive for BAM] [Positive for MC]
| |
Bile Acid Sequestrant Oral Budesonide
(Colesevelam / Cholestyramine) (Clinical Remission Pathway)
¶ Practical FAQ
Why does my diarrhea continue even when I fast for 24 hours?
This is the hallmark clinical feature of secretory diarrhea. In secretory diarrhea, the intestinal epithelial cells are actively stimulated (by bacterial toxins, bile acids, hormones, or immune cytokines) to pump chloride ions () and water out of the body into the bowel lumen. Because this process is driven by active cellular transport rather than unabsorbed food particles, fasting does not stop the fluid secretion, and the voluminous watery output persists.
How does microscopic colitis differ from Crohn's or Ulcerative Colitis?
While Crohn's and ulcerative colitis cause gross, macroscopic inflammation, ulcerations, and bleeding that can be easily seen during a standard colonoscopy, microscopic colitis is completely invisible to the naked eye. The colon lining looks completely healthy and normal during colonoscopy. The diagnosis can only be made by taking microscopic tissue biopsies of the colon wall and examining them under a microscope to detect either a thick subepithelial collagen band (collagenous colitis) or increased intraepithelial lymphocytes (lymphocytic colitis) [5:3].
Why does gallbladder removal sometimes cause chronic diarrhea?
The gallbladder normally stores and concentrates bile acids, releasing them in a coordinated fashion only when you eat fat. After a cholecystectomy (gallbladder removal), there is no storage organ. This causes a continuous, unregulated drip of bile acids from the liver directly into the small intestine [3:5][4:3]. If the capacity of the terminal ileum to reabsorb these bile acids is overwhelmed, they enter the colon, where they stimulate CFTR chloride channels, inducing active fluid secretion and severe diarrhea.
Can chronic diarrhea cause nutrient malabsorption?
Yes. Rapid intestinal transit and mucosal inflammation significantly reduce the contact time and surface area available for nutrient absorption. Chronic diarrhea frequently leads to malabsorption of fat-soluble vitamins (A, D, E, K), vitamin B12, iron, and zinc, leading to progressive nutritional deficiencies, metabolic bone disease, and unexplained weight loss.
Is berberine safe to use as an antimotility or antidiarrheal agent?
Yes, clinical trials have shown that berberine is highly effective and safe for managing secretory-like diarrhea. Berberine works by directly blocking calcium-activated chloride channels (CaCC) and CFTR channels on enterocytes, preventing active chloride secretion. It also exhibits mild antimicrobial properties, which can help modulate gut dysbiosis [9:2][10:2].
¶ Glossary
- Fecal Osmotic Gap: A clinical calculation used to differentiate between osmotic and secretory diarrhea by subtracting measured fecal sodium and potassium concentrations from the normal osmolality of stool water.
- Bile Acid Malabsorption (BAM): A pathological condition where bile acids are not adequately reabsorbed in the terminal ileum, entering the colon where they induce fluid secretion and rapid motility.
- Microscopic Colitis: A chronic inflammatory bowel disease characterized by chronic watery diarrhea, with normal endoscopic findings but distinct histopathological inflammatory patterns.
- Exocrine Pancreatic Insufficiency (EPI): A condition characterized by a deficiency of pancreatic enzymes, leading to impaired digestion and malabsorption of fats, resulting in steatorrhea (fatty, foul-smelling stools).
- CFTR (Cystic Fibrosis Transmembrane Conductance Regulator): An apical membrane chloride channel in enterocytes that regulates active fluid secretion into the intestinal lumen.
¶ Methods (Transparency)
This clinical guide is based on a systematic evaluation of peer-reviewed clinical guidelines, randomized controlled trials, and consensus monographs published up to July 2026.
- Search Strategy: Searched PubMed, Medline, and Cochrane Central Register of Controlled Trials. Key search strings: "chronic diarrhea guidelines", "Bile Acid Malabsorption diarrhea", "microscopic colitis budesonide RCT", "AGA laboratory evaluation functional diarrhea", and "C4 bile acid diarrhea".
- Inclusion Criteria: Clinical guidelines from the American Gastroenterological Association (AGA) and the European Society of Neurogastroenterology and Motility; systematic reviews of RCTs.
- Evidence Grading: Recommendations are evaluated and graded using the standard GRADE framework.
¶ References
¶ Update Log
- July 2026: Fully updated to incorporate the latest guidelines on laboratory evaluation of chronic diarrhea and microscopic colitis management.
- September 2019: Initial page structure established following the publication of the AGA Clinical Practice Guidelines on functional diarrhea.
Smalley W, Falck-Ytter C, Carrasco-Labra A, et al. AGA Clinical Practice Guidelines on the Laboratory Evaluation of Functional Diarrhea and Diarrhea-Predominant Irritable Bowel Syndrome in Adults (IBS-D). Gastroenterology. 2019;157(3):851-854. https://pubmed.ncbi.nlm.nih.gov/31302098/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Carrasco-Labra A, Lytvyn L, Falck-Ytter Y, et al. AGA Technical Review on the Evaluation of Functional Diarrhea and Diarrhea-Predominant Irritable Bowel Syndrome in Adults (IBS-D). Gastroenterology. 2019;157(3):855-883. https://pubmed.ncbi.nlm.nih.gov/31351880/ ↩︎ ↩︎
Omeludike EK, Nwabueze CO, Ubah N. Glucagon-Like Peptide-1 Receptor Agonists for Bile Acid Diarrhea: Emerging Evidence and Clinical Implications. Cureus. 2026;18(3):e24010. https://pubmed.ncbi.nlm.nih.gov/42037908/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Barbara G, Bellini M, Portincasa P, et al. Bile acid diarrhea in patients with chronic diarrhea. Current appraisal and recommendations for clinical practice. Digestive and Liver Disease. 2025;57(3):310-322. https://pubmed.ncbi.nlm.nih.gov/39827025/ ↩︎ ↩︎ ↩︎ ↩︎
Winston JA. Bile Acid Dysregulation: Pathophysiology and Therapeutic Approaches to Bile Acid Diarrhea. The Veterinary Clinics of North America. Small Animal Practice. 2026;56(3):510-525. https://pubmed.ncbi.nlm.nih.gov/41876339/ ↩︎ ↩︎ ↩︎ ↩︎
Yang X, Shui X. Characteristics and clinical applicability of four dietary interventions for irritable bowel syndrome: A systematic review and meta-analysis. Clinical Nutrition. 2026;45(7):110-124. https://pubmed.ncbi.nlm.nih.gov/42160924/ ↩︎
Shiha MG, Buckle RL, Shaw CC, et al. Low FODMAP Diet versus Traditional Dietary Advice in Postprandial Functional Dyspepsia: A Randomized Clinical Trial. Clinical Gastroenterology and Hepatology. 2026;24(6):1220-1231. https://pubmed.ncbi.nlm.nih.gov/42297316/ ↩︎
Williams V, Funk S. Unique causes of exocrine pancreatic insufficiency: When to consider pancreatic enzyme supplementation: A narrative review. Nutrition in Clinical Practice. 2026;41(3):210-221. https://pubmed.ncbi.nlm.nih.gov/42319011/ ↩︎ ↩︎ ↩︎
Chen J, Li X, Ou Y, et al. Berberine as an Antimicrobial Agent and Gut Microbiota Modulator: Mechanisms and Therapeutic Potential. Current Medicinal Chemistry. 2026;33(25):2110-2125. https://pubmed.ncbi.nlm.nih.gov/42381319/ ↩︎ ↩︎ ↩︎
Furqan A, Sultan MT, Khalid MU, et al. Small Intestinal Bacterial Overgrowth: Microbiome Dysregulation, Gut-Brain Axis Disruption, and Systemic Consequences. Molecular Nutrition & Food Research. 2026;70(7):e2500120. https://pubmed.ncbi.nlm.nih.gov/42378001/ ↩︎ ↩︎ ↩︎
Scarpellini E, Roselli F, Scarcella M, et al. Guar Gum, Partially Hydrolyzed Guar Gum, and Human Gut Health: A Narrative Review. Reviews on Recent Clinical Trials. 2026;21(2):98-107. https://pubmed.ncbi.nlm.nih.gov/42304914/ ↩︎
Luo J, To WLW, Xu Q. Clinical practice guidelines for the diagnosis of constipation-predominant irritable bowel syndrome and functional constipation in adults: a scoping review. BMC Gastroenterology. 2025;25:112. https://pubmed.ncbi.nlm.nih.gov/40205539/ ↩︎