¶ Digestive Health: Physiology, Motility, and Symptom Optimization
¶ Layer 1: The Executive Dashboard
¶ At a Glance
Digestive health refers to the optimal physiological functioning of the gastrointestinal tract, including the efficient breakdown of food, the secretion of critical digestive fluids, the absorption of essential nutrients, and the regular motility required to clear waste. Healthy digestion requires coordinated teamwork between gastric acid, pancreatic enzymes, bile acids, and the enteric nervous system (ENS). When this coordination is disrupted, it leads to common functional symptoms like acid reflux, bloating, constipation, and diarrhea.
¶ Safety "Traffic Light"
- Green Light (Go): Daily habits like thorough chewing, gentle walking after meals, staying hydrated, and eating adequate soluble fiber are highly safe, effective strategies to optimize digestive function.
- Yellow Light (Proceed with Caution): Supplementary digestive aids—including betaine HCl (stomach acid support), high-potency pancreatic enzymes, ox bile, or prokinetic agents (like ginger and artichoke extracts)—should be used deliberately. These supplements are highly effective when tailored to specific secretory or motility deficits, but improper use can cause mucosal irritation.
- Red Light (Do NOT Proceed): Certain "red flag" symptoms require immediate diagnostic evaluation by a clinician rather than self-management. These include unexplained weight loss, persistent difficulty swallowing (dysphagia), blood in the stool (hematochezia or melena), recurrent nocturnal waking due to symptoms, or severe, progressive abdominal pain.
¶ Protocol Card
The following table outlines actionable, evidence-based protocols for managing common digestive symptoms and optimizing gastrointestinal function.
| Indication | Clinical Protocol / Intervention | Primary Physiological Mechanism | Target Outcome |
|---|---|---|---|
| Acid Reflux / GERD | Melatonin (3mg at bedtime) + D-Limonene (1,000mg every other day) | Increases lower esophageal sphincter (LES) tone, protects esophageal mucosa [1] | Reduces heartburn severity and frequency |
| Bloating & Gas | 4-week trial of a Low-FODMAP Diet, titrated under guidance | Reduces osmotic water load and rapid microbial gas fermentation in the colon [1:1][2] | Significant reduction in abdominal distension |
| Constipation / Slow Transit | Magnesium Citrate/Oxide (500–1,000mg at night) + Soluble Psyllium Fiber (5g with water) | Draws water into the colon (osmotic laxative) to soften stool and stimulate peristalsis [3][4] | Normalizes transit time to 24–36 hours (Bristol Type 3–4) |
| Sluggish Motility (MMC) | Artichoke Leaf Extract (320mg) + Ginger Root Extract (100mg) | Acts as a natural prokinetic, stimulating gastric emptying and the Migrating Motor Complex | Restores regular bowel movements and reduces early satiety |
¶ Bottom Line
Digestive health is the gateway to systemic longevity. By optimizing the secretion of digestive juices and maintaining steady gastrointestinal transit, you ensure efficient nutrient delivery, prevent toxic microbial overgrowths, and support overall cellular health and vitality [5][6][7].
¶ Layer 2: The Contextual Narrative
¶ The "Why" (Systemic Benefits)
Optimal digestive function is essential for absorbing the micronutrients, amino acids, and fatty acids required for cellular repair, mitochondrial energy production, and systemic healthspan.
- Nutrient and Protein Absorption: Inadequate stomach acid (hypochlorhydria) or low pancreatic enzyme levels prevent the proper breakdown of dietary proteins into free amino acids. This can lead to age-related muscle loss (sarcopenia), impaired bone mineral density, and micronutrient deficiencies (especially vitamin B12, iron, and zinc) [5:1][7:1].
- Preventing Small Intestinal Bacterial Overgrowth (SIBO): Robust stomach acid and bile serve as natural antimicrobials, sterilizing food as it enters the digestive tract. Combined with the Migrating Motor Complex (MMC)—the peristaltic "housekeeping wave" of the small intestine—healthy motility prevents colonic bacteria from migrating backward into the small intestine, keeping SIBO and chronic systemic endotoxemia at bay [1:2].
- Vagal Nerve Coordination: The enteric nervous system (ENS) communicates bidirectionally with the central nervous system via the vagus nerve. Efficient digestion and regular motility send positive, calming feedback to the brain. Conversely, sluggish motility or structural congestion can trigger chronic sympathetic nervous system activation, contributing to anxiety, sleep disturbances, and cognitive fatigue [8][9].
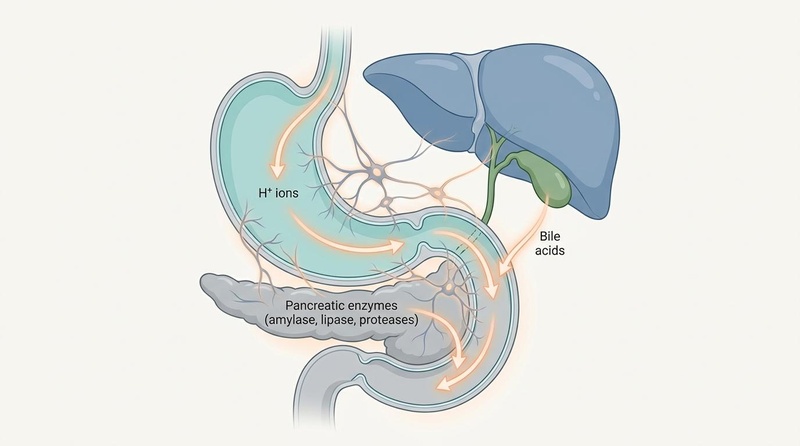
Figure 1: Diagram of the upper gastrointestinal organs, illustrating the localized secretion of gastric acid (H+), pancreatic enzymes, and bile acids, coordinated alongside the enteric nervous system (ENS).
¶ Reality Check & Commercial Context
¶ Human Clinical Reality vs. Mouse Hopes
Many functional digestive conditions, such as irritable bowel syndrome (IBS) or functional dyspepsia, are uniquely human disorders. Because they are defined by subjective symptoms like bloating, visceral hypersensitivity, and abdominal discomfort, they cannot be easily modeled in mice. While animal models are useful for studying basic gut transit speeds or mucosal lining biology, human digestive health relies heavily on complex, integrated factors: the central nervous system, autonomic tone, life stressors, and eating behaviors. Clinical success requires treating the whole human, rather than relying on animal-derived solutions [10][11].
¶ The Stomach Acid Myth
A common misconception is that acid reflux and heartburn are always caused by having too much stomach acid. In reality, especially as we age, gastric acid secretion naturally declines (hypochlorhydria) [7:2]. When stomach acid is low, food sits in the stomach longer, causing delayed gastric emptying. This delayed emptying increases intragastric pressure, forcing even small amounts of stomach acid—along with pepsin and bile—upward through the lower esophageal sphincter (LES) into the esophagus, causing heartburn. Consequently, long-term use of proton pump inhibitors (PPIs) to suppress acid can worsen the root cause of reflux while impairing protein and B12 absorption [7:3].
¶ Commercial Solutions
The wellness market is flooded with digestive enzymes, specialized bile salts, and complex prokinetic herbal formulas. While these products can be highly effective, they must be used strategically:
- Digestive Enzymes: Highly beneficial for individuals with documented pancreatic insufficiency or during large, protein-dense meals. They should not be used as a blanket solution for bloating caused by SIBO or poor chewing habits.
- Betaine HCl: Excellent for restoring gastric acidity, but should never be taken by individuals with active peptic ulcers or those taking NSAIDs, as it can cause mucosal erosions.
- Herbal Prokinetics (Ginger/Artichoke): Excellent, evidence-based tools for stimulating the MMC between meals. However, they will have limited success if chronic constipation and rectal evacuation issues are not addressed first.
¶ Practical Integration
Optimizing digestive function requires combining dietary adjustments with mindful eating habits and physical behaviors.
¶ The Cephalic Optimization Protocol: Enhancing Endogenous Secretions
To maximize your body's natural production of stomach acid and pancreatic enzymes, follow these steps during your main meals:
- The Cephalic Phase Activation: Before eating, take 3 slow, deep breaths. Look at, smell, and appreciate your food. This sensory activation triggers the vagus nerve, initiating up to 30% of your total gastric acid and pancreatic enzyme secretions before a single bite enters your mouth.
- The Mastication Rule: Chew every bite of food 20 to 30 times until it reaches a liquid consistency. Mechanical chewing reduces the workload on your stomach and pancreas, preventing large, undigested food particles from reaching the colon where they cause rapid, painful gas fermentation.
- Liquid Management: Avoid drinking large glasses of ice-cold water during meals. Small sips of warm water or digestive bitters are fine, but excess liquids can dilute gastric juices, lowering stomach acidity and impairing protein digestion.
¶ Daily Motility & Positioning Habits
- The Postprandial Walk: Engage in a gentle 10-to-15 minute walk immediately after your largest meals. Gentle movement stimulates stretch receptors in the stomach and intestines, promoting healthy gastric emptying and transit without shunting blood away from the digestive tract.
- Anatomical Alignment (The Squatty Potty): When evacuating, use a footstool to elevate your knees above your hips, mimicking a squatting position. This relaxes the puborectalis muscle, straightening the anorectal angle and allowing for complete, effortless bowel movements, which prevents pelvic floor strain and hemorrhoids.
- Intermeal Fasting Windows: Avoid continuous grazing throughout the day. Allow at least 4 hours between meals to give the Migrating Motor Complex (MMC) enough time to complete its cleansing cycles, keeping the small intestine clear of bacteria and debris.
¶ Layer 3: The Evidence Room
¶ Mechanism of Action
Efficient digestion and transit rely on four core physiological processes:
[ INGESTED FOOD ]
|
1. Gastric Secretion: Parietal cells secrete H+ via H+/K+-ATPase pumps
| (Chyme enters Duodenum)
2. Duodenal Coordination: Duodenal cells release CCK and Secretin
|
+------------------+------------------+
| |
[ PANCREATIC ENZYMES ] [ BILE ACIDS ]
- Amylase (carbohydrates) - Secreted by Gallbladder
- Lipase (fats) - Emulsifies dietary lipids
- Proteases (proteins) - Recycled via Ileum (95%)
\ /
\ /
v v
3. Peristalsis & MMC: Enteric Nervous System (ENS) coordinates
orderly muscle contractions to drive transit (Bristol 3-4)
- Gastric Acid Secretion: Parietal cells in the stomach lining secrete hydrogen ions () via the -ATPase proton pump, lowering gastric pH to 1.5–2.5. This high acidity is essential for denaturing proteins, activating the pepsinogen enzyme into active pepsin, and neutralizing ingested pathogens [7:4].
- Duodenal Hormone Release: As acidic food (chyme) enters the duodenum, it triggers the release of cholecystokinin (CCK) and secretin into the bloodstream. CCK stimulates the gallbladder to contract, releasing bile acids, and prompts pancreatic acinar cells to secrete active digestive enzymes (amylase, lipase, and proteases). Secretin prompts the pancreas to release bicarbonate, neutralizing the acidic chyme to protect the intestinal lining.
- Enteric Nervous System & Peristalsis: The Enteric Nervous System (ENS)—consisting of the myenteric and submucosal plexuses—induces coordinated, wave-like muscle contractions (peristalsis) to move food through the digestive tract. Between meals, the ENS coordinates the Migrating Motor Complex (MMC), a cyclic housekeeping wave that sweeps through the stomach and small intestine every 90–120 minutes to clear undigested debris and bacteria.
- Bile Acid Circulation: Bile acids are synthesized from cholesterol in the liver, stored in the gallbladder, and released into the duodenum to emulsify fats. They are highly recycled, with 95% reabsorbed in the terminal ileum and returned to the liver via portal circulation (enterohepatic circulation) [10:1].
¶ Lifespan and Sex Differences
- Young Adults: Typically maintain robust gastric acid secretion and efficient intestinal transit. Functional symptoms in this group are often driven by high stress, poor diet, and lifestyle habits.
- Middle-Aged Adults: Estrogen and progesterone receptors are present throughout the gastrointestinal tract. In perimenopausal and postmenopausal women, fluctuations in these hormones can slow colonic transit times, alter bile acid profiles, and increase the risk of gallstone formation and chronic constipation [12][10:2].
- Older Adults: The aging gut often experiences a reduction in parietal cell function (leading to lower stomach acid) and pancreatic enzyme output, which can impair overall nutrient absorption [7:5]. Additionally, age-related enteric neurodegeneration can weaken the muscles of the colon, slowing colonic transit and contributing to chronic constipation [3:1].
¶ Evidence Summary Table (Human Outcomes)
The following matrix summarizes the clinical human evidence for key digestive health interventions.
| GI Symptom / Target | Clinical Intervention | Observed Clinical Effect | Certainty (GRADE) | Key Citations |
|---|---|---|---|---|
| Acid Reflux / GERD | Melatonin (3mg at bedtime) | Compares favorably to omeprazole in reducing heartburn symptoms over 4–8 weeks; increases LES tone | High (Multiple randomized controlled human trials) | Kandil et al., BMC Gastroenterol, 2010 |
| Bloating & Gas | Low-FODMAP Diet | Up to 70–80% reduction in bloating, abdominal pain, and flatulence in functional bowel disorders over 4–6 weeks | High (Multiple systematic reviews and RCTs) | Kuźmin et al., 2025; Eswaran et al., 2016 [1:3][2:1] |
| Chronic Constipation | Magnesium oxide/citrate | Dose-dependent increase in stool frequency and softness; outperforms placebo | High (Randomized, double-blind clinical trials) | Morishita et al., 2021 |
| Sluggish Motility (MMC) | Artichoke and Ginger Extract | Significant reduction in early satiety, bloating, and nausea; accelerates gastric emptying | Moderate (1 major human RCT, supported by physiological studies) | Giacosa et al., Evid Based Complement Alternat Med, 2015 |
| Celiac Disease | Strict Gluten-Free Diet | Reverses mucosal damage, normalizes celiac antibody levels, and resolves malabsorption symptoms | High (Established clinical practice guidelines) | Rubio-Tapia et al., ACG Guidelines, 2013 [13] |
¶ Comprehensive Safety, Toxicology, & Contraindications
¶ Chronic Laxative Dependency Risks
While osmotic laxatives (like magnesium oxide or polyethylene glycol) are highly safe for long-term use, stimulant laxatives (such as senna, bisacodyl, or cascara) should be used with caution. Chronic, daily use of stimulant laxatives can cause colonic tolerance, mucosal pigment changes (melanosis coli), and potentially damage the enteric nervous system, leading to a dependent, "lazy colon" that cannot contract without stimulation [3:2].
¶ Chronic Proton Pump Inhibitor (PPI) Hazards
While PPIs (such as omeprazole, esomeprazole, and pantoprazole) are highly effective for short-term healing of erosive esophagitis or peptic ulcers, chronic use (exceeding 8–12 weeks) carries significant physiological risks. Prolonged acid suppression can cause:
- Malabsorption: Reduced absorption of vitamin B12, calcium, iron, and magnesium due to elevated gastric pH [7:6].
- Infection Risk: Increased susceptibility to SIBO and enteric infections, including Clostridioides difficile, as stomach acid is a key biological barrier against ingested pathogens.
- Hypergastrinemia: Compensatory overproduction of the gastrin hormone, which can lead to parietal cell hypertrophy and rebound acid hypersecretion when the medication is stopped.
¶ Bile Acid Diarrhea and Ox Bile Risks
Supplementary ox bile and bile acids (like TUDCA) are excellent for supporting fat digestion in individuals who have had their gallbladder removed or those with documented fat malabsorption. However, if bile acids are taken in excess or cannot be properly reabsorbed in the terminal ileum, they flow into the colon where they act as potent local irritants. This causes bile acid diarrhea, characterized by urgent, watery, yellow-orange stools and abdominal cramping. If watery diarrhea occurs after supplementing bile acids, immediately reduce the dose or pause the supplement.
¶ Comparisons & Engagement
¶ "Compare With" (Digestive Supports)
When selecting supplements to support digestive secretions, align the intervention with the precise clinical deficiency:
- Betaine HCl: Restores stomach acidity. Best utilized for protein malabsorption, hypochlorhydria, or GERD caused by low stomach acid. It should be taken at the start of protein-containing meals and titrated up slowly until a mild warming sensation is felt.
- Pancreatic Enzymes (Acreon/Pancreatin): Provides active amylase, lipase, and proteases. Best utilized for fat malabsorption (characterized by greasy, floating stools), pancreatic insufficiency, or general digestive support during heavy, nutrient-dense meals.
- TUDCA / Ox Bile: Emulsifies dietary fats. Best utilized for individuals without a gallbladder, those with pale/clay-colored stools, or fat-soluble vitamin (A, D, E, K) deficiencies. It supports bile flow and assists in liver detoxification pathways.
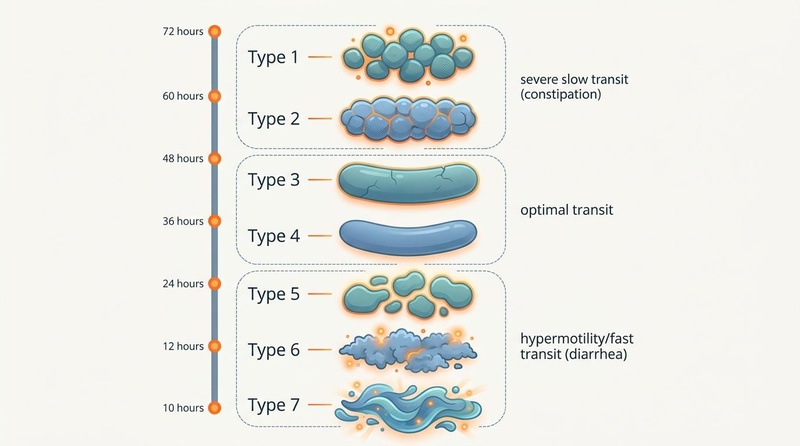
Figure 2: The Bristol Stool Form Scale and transit time correlation. Stool morphology serves as an immediate, non-invasive surrogate biomarker for intestinal transit speed, with Type 3 and 4 representing optimal motility.
¶ Internal Wiki Cross-Links
- For the broader systemic context of gut barrier support and mucosal immunity, see Gut Health Cornerstone Guide.
- To explore the taxonomic structure of the microbiome and the role of postbiotics, see Gut Microbiome Deep Dive.
- For specific botanical and herbal monographs, explore Triphala, Slippery Elm, and Akkermansia muciniphila.
- To learn more about the biology of aging, see The Hallmarks of Aging and Chronic Inflammation.
¶ References
¶ Update Log
- July 2026: Guide established, integrating the latest 2025/2026 clinical guidelines on low-FODMAP efficacy, chronic PPI risk management, hormone-driven GI changes, and the neurodegeneration of the aging colon.
Efficacy of a Low-FODMAP Diet on the Severity of Gastrointestinal Symptoms and Quality of Life in the Treatment of Gastrointestinal Disorders-A Systematic Review of Randomized Controlled Trials. PubMed. https://pubmed.ncbi.nlm.nih.gov/40573159/ ↩︎ ↩︎ ↩︎ ↩︎
A Randomized Controlled Trial Comparing the Low FODMAP Diet vs. Modified NICE Guidelines in US Adults with IBS-D. PubMed. https://pubmed.ncbi.nlm.nih.gov/27725652/ ↩︎ ↩︎
The aging colon: the role of enteric neurodegeneration in constipation. PubMed. https://pubmed.ncbi.nlm.nih.gov/20878508/ ↩︎ ↩︎ ↩︎
Distal colonic transit is linked to gut microbiota diversity and microbial fermentation in humans with slow colonic transit. PubMed. https://pubmed.ncbi.nlm.nih.gov/31869241/ ↩︎
Editorial: Microbial influences on aging: insights from the gut microbiome. PubMed. https://pubmed.ncbi.nlm.nih.gov/42383281/ ↩︎ ↩︎
Early Biomarkers, Risk Factors, and Functional Indicators of Healthy Longevity and Their Relationship with Diet. PubMed. https://pubmed.ncbi.nlm.nih.gov/42280310/ ↩︎
The ageing gastrointestinal tract. PubMed. https://pubmed.ncbi.nlm.nih.gov/26560524/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Paradigm Shift of Microbiota-gut-brain Axis During Aging: Potential Role of Probiotics to Improve Cognitive Decline. PubMed. https://pubmed.ncbi.nlm.nih.gov/42400751/ ↩︎
The Gut-Brain-Muscle Axis: Microbial Regulation of Neuromuscular Aging and Cognitive Frailty. PubMed. https://pubmed.ncbi.nlm.nih.gov/42354990/ ↩︎
Bi-Directional Relationship Between Bile Acids (BAs) and Gut Microbiota (GM): UDCA/TUDCA, Probiotics, and Dietary Interventions in Elderly People. PubMed. https://pubmed.ncbi.nlm.nih.gov/40004221/ ↩︎ ↩︎ ↩︎
Predictors of Symptom-Specific Treatment Response to Dietary Interventions in Irritable Bowel Syndrome. PubMed. https://pubmed.ncbi.nlm.nih.gov/35057578/ ↩︎
Sex differences in the associations between lifestyle, intestinal permeability and brain health in middle-aged adults. PubMed. https://pubmed.ncbi.nlm.nih.gov/42294080/ ↩︎
ACG clinical guidelines: diagnosis and management of celiac disease. PubMed. https://pubmed.ncbi.nlm.nih.gov/23609613/ ↩︎