¶ Endometriosis
| Condition Type | Systemic, Chronic Inflammatory |
| Primary Outcomes | Dysmenorrhea, Pelvic Pain, Dyspareunia, Infertility |
| Diagnostic Standards | Specialized TVUS, MRI, or Laparoscopy |
| First-Line Medical | NSAIDs, Combined Contraceptives, Progestins |
| Key Risk Profile | Bone loss with GnRH therapy (mitigated with add-back) |
| Prevalence | ~10% of reproductive-aged females globally |
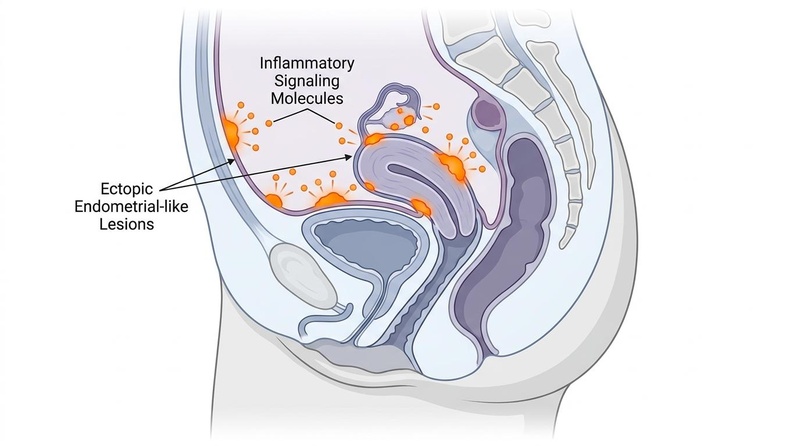
Endometriosis is a chronic, systemic inflammatory condition characterized by the presence of endometrial-like tissue outside the uterine cavity [1]. Far from a localized gynecological pathology, it behaves as a complex multisystem syndrome with deep neuropathic, immunological, and endocrinological sequelae, requiring coordinated, multi-modal clinical management [2][1:1][3][4].
¶ At a glance
- What people use it for / Treatment Goals: Modern clinical management focuses on suppressing ectopic lesion proliferation, alleviating pelvic pain, restoring anatomical relationships, managing infertility, and preventing post-surgical recurrence [2:1][1:2][5].
- Efficacy Verdict: High-certainty evidence supports first-line hormonal therapies (combined oral contraceptives and progestins like dienogest) and second-line GnRH therapies (elagolix or relugolix combination) for pain suppression [2:2][5:1]. Surgical intervention provides significant short-to-medium-term pain relief but carries a high recurrence risk without post-operative suppression, and there is no clear clinical consensus regarding its absolute benefit for managing associated infertility [2:3][1:3][6].
- Key Risks & Limitations: Diagnostic delays average 5 to 12 years [4:1]. Medical suppressive therapies are contraceptive and cannot be used by individuals attempting conception [2:4]. Advanced GnRH therapies carry risks of hypoestrogenic bone mineral density loss and vasomotor symptoms, necessitating structured add-back therapy [7][8]. Surgical intervention carries risks of visceral injury and pelvic adhesions [2:5][1:4][6:1].
¶ Clinical Presentation
Endometriosis presents with highly heterogeneous symptomatic phenotypes that frequently fail to correlate with disease stage. Ectopic tissue reacts to cyclic ovarian hormones by shedding and bleeding, driving localized immune recruitment, inflammation, neuroangiogenesis, and progressive fibrosis [1:5].
¶ Typical Symptom Patterns
The hallmark clinical presentation of endometriosis revolves around cyclic, pelvic pain syndromes [2:6][1:6]:
- Dysmenorrhea: Severe, progressive menstrual cramping, often incapacitating, occurring before and during menses.
- Non-Menstrual Chronic Pelvic Pain (CPP): Persistent pain lasting over six months, decoupled from the menstrual cycle.
- Deep Dyspareunia: Deep pelvic pain associated with sexual intercourse, driven by cervical motion, stretch of the uterosacral ligaments, or irritation of the cul-de-sac.
- Dysuria and Dyschezia: Cyclical pain on urination or defecation, indicative of bladder or bowel involvement.
- Infertility: Observed in a significant proportion of affected patients (with approximately 26% reporting infertility [4:2]), resulting from tubal occlusion, distorted pelvic anatomy, chronic follicular inflammation, and impaired oocyte quality [2:7][1:7].
¶ Atypical Symptom Patterns
Atypical presentations occur when endometrial-like tissue implants in extrapelvic sites [2:8][1:8]:
- Extrapelvic Endometriosis: Ectopic implants can occur in extrapelvic locations, leading to varying presentations and cyclical symptoms outside the pelvic cavity [2:9][1:9].
- Constitutional Symptoms: Profound cyclical fatigue and immune-mediated malaise can accompany the inflammatory state [1:10].
¶ Diagnostic Challenges and Overlap Syndromes
Diagnostic confusion remains a major contributor to the average 5-to-12-year delay from symptom onset to diagnosis [4:3]. The symptoms of endometriosis significantly overlap with other chronic visceral and somatic pelvic pain disorders, creating diagnostic challenges:
- Irritable Bowel Syndrome (IBS): The chronic pain and systemic inflammatory nature of endometriosis frequently overlap with bowel symptoms, leading to chronic abdominal pain and bowel distress that can mimic or co-exist with IBS [9]. Patients are frequently misdiagnosed with IBS or experience comorbid bowel symptoms.
- Interstitial Cystitis / Bladder Pain Syndrome (IC/BPS): Bladder mucosal involvement or pelvic cross-sensitization leads to urinary frequency, urgency, and pelvic pressure that mimics bladder wall pathology.
- Pelvic Floor Dysfunction (Hypertonic Pelvic Floor): Chronic pelvic pain triggers protective guarding of the pelvic floor muscles (levator ani, coccygeus). This myofascial spasm causes secondary somatic pelvic pain, pelvic floor tension, and deep dyspareunia, persisting even when the primary visceral lesions are medically suppressed [10].
¶ Differential Diagnosis
The clinical features of endometriosis mimic multiple acute and chronic abdominal and pelvic conditions. Differential diagnosis is critical to prevent unnecessary surgical procedures or catastrophic delays in addressing surgical emergencies.
| Diagnosis | Distinguishing Clinical Features | Key Diagnostic Findings |
|---|---|---|
| Ectopic Pregnancy | Acute unilateral pelvic pain, abnormal vaginal bleeding, missed menses. | Elevated serum -hCG; absence of intrauterine gestational sac on transvaginal ultrasound (TVUS). |
| Ovarian Torsion | Sudden-onset, severe, sharp unilateral lower abdominal pain, often accompanied by nausea and vomiting. | TVUS with color Doppler showing enlarged ovary with diminished or absent stromal blood flow. |
| Ruptured Ovarian Cyst | Sudden-onset unilateral pain, often occurring mid-cycle or after vigorous physical activity. | TVUS demonstrating free fluid in the pelvis and a collapsed or hemorrhagic ovarian cyst shell. |
| Pelvic Inflammatory Disease (PID) | Bilateral pelvic pain, purulent cervical discharge, cervical motion tenderness, fever. | Leukocytosis, elevated CRP, positive cervical swab for Chlamydia or Neisseria; TVUS showing hydrosalpinx or tubo-ovarian abscess. |
| Adenomyosis | Diffuse pelvic pain, severe dysmenorrhea, heavy menstrual bleeding (menorrhagia), enlarged and tender globoid uterus [1:11]. | TVUS or MRI showing asymmetric myometrial thickening, subendometrial cysts, or external adenomyosis [11]. |
| Uterine Fibroids (Leiomyomas) | Pelvic pressure, heavy menstrual bleeding, palpable abdominal/pelvic masses. | Well-circumscribed hypoechoic myometrial masses on ultrasound or MRI. |
| Malignancy (Ovarian/Peritoneal Cancer) | Bloating, early satiety, pelvic pain, weight loss, progressive abdominal distention (ascites). | Complex solid-cystic adnexal masses on TVUS/MRI; elevated CA-125, HE4, and abnormal cytology. |
| Acute Appendicitis | Periumbilical pain migrating to the right lower quadrant (McBurney's point), fever, anorexia, signs of localized peritonitis. | Computed Tomography (CT) or ultrasound showing appendiceal diameter with wall thickening; neutrophilic leukocytosis. |
¶ Diagnostic Evaluation
The diagnostic paradigm of endometriosis has undergone a structural shift [2:10][1:12]. Historically, definitive diagnosis was established via surgical visualization of lesions during laparoscopy, but current international consensus guidelines support starting empirical therapy based on a clinical diagnosis supported by history and imaging [2:11][4:4]. Current international consensus guidelines, including the European Society of Human Reproduction and Embryology (ESHRE) (2022), support a clinical and imaging-based diagnostic model to initiate early intervention and avoid unnecessary surgical morbidity [2:12][1:13][3:1].
Symptomatic Suspect (Dysmenorrhea, Dyspareunia, Pelvic Pain)
│
▼
Standard Pelvic Exam &
High-Resolution TVUS / Pelvic MRI
│
┌───────────┴───────────┐
▼ ▼
Lesions Identified Negative / Equivocal
(Endometrioma, DIE) │
│ ▼
│ Empirical Therapy Trial
│ │
│ ┌─────────┴─────────┐
│ ▼ ▼
│ Responded Non-Responder /
│ (Continue Meds) Suspicion of Deep Disease
│ │ │
└─────────────┼───────────────────┘
▼
Therapeutic Laparoscopy
(Excision, Biopsy, Pathology confirmation)
¶ 1. Clinical / Empirical Diagnosis
Clinical diagnosis is established via a cluster of characteristic history-taking findings (menstrual pain, cyclic bowel/bladder changes, dyspareunia) coupled with targeted physical examination. Physical examination findings can support a clinical diagnosis, but a normal physical examination does not exclude the diagnosis [4:5]. A positive clinical presentation justifies the initiation of empirical medical therapy without surgical verification [2:13][3:2].
¶ 2. Specialized Imaging Modes
High-resolution imaging has high accuracy for detecting deep infiltrating endometriosis (DIE) and endometriomas, though it may miss superficial peritoneal implants [2:14][1:14].
- Transvaginal Ultrasound (TVUS) with Deep Endometriosis Protocol: First-line imaging. Standard pelvic TVUS is enhanced with bowel preparation and dynamic maneuvers (e.g., assessing the "sliding sign" to evaluate pouch of Douglas obliteration). TVUS is highly accurate for identifying ovarian endometriomas and deep bowel implants, although its ability to detect superficial peritoneal implants is limited [2:15][1:15].
- Magnetic Resonance Imaging (MRI): Second-line imaging, particularly indicated for pre-operative planning or when ultrasound is equivocal. The European Society of Urogenital Radiology (ESUR) guidelines recommend a standardized protocol including multiplanar T2W and T1W sequences, with T1W fat-suppressed (T1WFS) sequences to describe superficial peritoneal implants, and a compartment-based evaluation [11:1]. This standardized mapping improves communication and surgical planning [11:2].
¶ 3. Laparoscopy: Diagnostic vs. Therapeutic
While non-invasive imaging has advanced, laparoscopy remains the final definitive step for biopsy confirmation and when superficial disease is suspected but imaging is negative [2:16][1:16].
- Diagnostic Laparoscopy: Solely visualizing the pelvic cavity to confirm disease. It is discouraged as an isolated procedure because it exposes the patient to surgical risk without therapeutic benefit [2:17][6:2].
- Therapeutic Laparoscopy: Visualization combined with immediate, concurrent surgical eradication of lesions (excision or ablation). It is indicated when empirical medical therapies fail, for acute complications (e.g., ruptured endometrioma), or for surgical management of associated infertility [2:18][1:17][6:3].
¶ Empirical Therapy
The rationale for empirical therapy is to suppress disease progression, manage pain, and prevent central sensitization while avoiding the risks, costs, and delays of surgery [2:19][1:18][3:3].
¶ Recommended Drug Classes
- NSAIDs: Indicated for baseline, non-specific cyclic pain control [2:20][5:2].
- Hormonal Suppression: Combined oral contraceptives (COCs) or progestins are the first-line empirical options [2:21][6:4]. Continuous administration is preferred over cyclic to eliminate menstruation and minimize cyclical inflammatory spikes.
¶ Trial Duration and Monitoring
- Duration: A clinical trial of empirical therapy is conducted for a defined trial period to monitor clinical response [3:4].
- Monitoring Criteria: Efficacy is assessed via standardized pain scales (Visual Analogue Scale, VAS), reduction in school or work absenteeism, and improvement in quality-of-life indices [2:22][3:5].
- Clinical Success: Indicated by a clinically meaningful reduction in pelvic pain, improvement in health-related quality of life, and the tolerability of side effects under continuous treatment [12][13]. Non-responders must be re-evaluated with advanced imaging (MRI) or considered for therapeutic laparoscopy [2:23][1:19].
¶ Therapeutic Interventions
Management of endometriosis requires an individualized, multi-disciplinary approach [2:24][1:20]. Therapies target different aspects of the disease, from direct hormone suppression to mechanical pelvic release.
¶ 1. NSAIDs
- Mechanism of Action: Ectopic endometrial lesions express high levels of cyclooxygenase-2 (COX-2), leading to elevated local and systemic prostaglandin () levels [1:21]. drives hyperalgesia, uterine smooth muscle hyper-contractility, and neuroangiogenesis. NSAIDs inhibit COX-1 and COX-2 enzymes, suppressing prostaglandin synthesis to reduce nociceptor activation [5:3].
- Clinical Protocol: NSAID therapy (such as ibuprofen or naproxen sodium) is commonly utilized as a first-line option for baseline pain control [2:25][5:4].
- Efficacy & Safety: NSAIDs provide effective short-term relief for dysmenorrhea, but have low efficacy for chronic non-menstrual pelvic pain [5:5]. Chronic use is limited by gastrointestinal mucosal injury, increased risk of peptic ulcer disease, renal perfusion impairment, and potential inhibition of ovulation when taken during the pre-ovulatory phase.
¶ 2. Hormonal Suppression
¶ Combined Oral Contraceptives (COCs)
- Mechanism of Action: COCs deliver a combination of synthetic estrogen (ethinyl estradiol) and a progestin. They suppress gonadotropin-releasing hormone (GnRH) pulsatility in the hypothalamus, downregulating follicle-stimulating hormone (FSH) and luteinizing hormone (LH) secretion [1:22][5:6]. This suppresses ovarian follicular development and endogenous -estradiol production, while creating a stable, thin, decidualized endometrium that undergoes atrophy [1:23].
- Clinical Protocol:
- Efficacy & Safety: Highly effective for mild-to-moderate dysmenorrhea [2:27][5:8]. Major safety concerns include venous thromboembolism (VTE) risk (particularly in smokers or those with thrombophilia), hepatic adenomas, hypertension, and minor side effects like breast tenderness, mood lability, and breakthrough bleeding.
¶ Progestins (Oral / Depot)
- Mechanism of Action: Progestins induce extensive decidualization of endometrial-like tissue, followed by profound atrophy of the implants. They also downregulate estrogen receptors inside the lesions, inhibiting local estrogen production and downstream inflammatory cascades [1:24][13:1].
- Clinical Protocol:
- Dienogest (Oral): orally daily, taken continuously [13:2][14].
- Medroxyprogesterone Acetate (Depot): intramuscularly every 12 weeks.
- Levonorgestrel Intrauterine System (LNG-IUS): Local delivery of of levonorgestrel directly to the pelvic cavity, highly effective for dysmenorrhea and adenomyosis [2:28][6:5].
- Efficacy & Safety: Dienogest 2 mg has high efficacy for reducing chronic pelvic pain, dysmenorrhea, and dyspareunia, demonstrating comparable efficacy and pain reduction to standard COCs [5:9][14:1]. The VIPOS study [12:1] is a large observational cohort study designed to monitor long-term safety, and pooled clinical trials [13:3] show dienogest 2 mg is well tolerated over up to 65 weeks with headache, breast discomfort, depressed mood (<10%), and acne as the most common mild-to-moderate adverse drug reactions. Common side effects include altered bleeding patterns (amenorrhea or unscheduled spotting), mild weight gain, breast tenderness, and mood changes.
¶ 3. GnRH Therapies
GnRH therapies target the hypothalamic-pituitary-ovarian axis to induce profound hypoestrogenism, creating a temporary "medical menopause" that deprives the estrogen-dependent endometriotic implants of their essential growth signal [1:25].
¶ GnRH Agonists (e.g., Leuprolide)
- Mechanism of Action: Continuous administration of GnRH agonists triggers an initial "flare effect" due to hyper-stimulation of pituitary GnRH receptors, resulting in a transient spike in FSH, LH, and estrogen [1:26]. Within 10 to 14 days, continuous receptor occupancy drives profound receptor downregulation and pituitary desensitization, suppressing gonadotropins and reducing serum -estradiol to postmenopausal levels () [1:27].
- Clinical Protocol:
- Leuprolide Acetate: intramuscularly monthly, or intramuscularly every 3 months.
- Must be combined with add-back therapy from day one of treatment.
¶ GnRH Antagonists (e.g., Elagolix, Relugolix)
- Mechanism of Action: GnRH antagonists competitively and reversibly bind to pituitary GnRH receptors, immediately blocking endogenous GnRH signaling without an initial flare [7:1][8:1]. They achieve rapid, dose-dependent suppression of LH, FSH, and estradiol [7:2][5:10].
- Clinical Protocol:
- Efficacy & Safety: GnRH antagonists have high efficacy for suppressing refractory dysmenorrhea and non-menstrual pelvic pain [5:11]. The main therapeutic challenge is managing profound hypoestrogenism, which causes vasomotor symptoms (hot flashes, night sweats), vaginal dryness, insomnia, adverse lipid profile changes, and progressive bone mineral density (BMD) loss [7:4][8:3].
¶ The Role of Add-Back Therapy
Profound hypoestrogenism can drive bone mineral density loss and vasomotor symptoms [7:5][1:28]. To prevent these effects, add-back therapy (low-dose estrogen and progestin) is co-administered to maintain sufficient estradiol levels to protect bone density and prevent vasomotor symptoms without stimulating lesions [7:6][8:4][1:29].
- Add-Back Protocol: Co-administration of low-dose estrogen and progestin. Standard regimens include:
- Mandatory Monitoring: Dual-energy X-ray absorptiometry (DEXA) scans must be performed at baseline and every 12 months if a GnRH agonist or un-supplemented antagonist is used for more than six months.
¶ 4. Surgery
- Laparoscopic Excision and Ablation: Both excision and ablation are utilized to eradicate visible lesions [2:29][6:6]. Clinical guidelines and reviews note ongoing discussions regarding their comparative effectiveness, with choice of technique often determined by lesion location, disease severity, and surgeon experience [2:30][1:30][6:7].
- Indications:
- Failure of, or contraindications to, first- and second-line medical suppressive therapies [2:31].
- Presumed deep infiltrating disease involving the muscularis of the bowel, ureters, or bladder with functional impairment [1:31].
- Ovarian endometriomas, particularly when symptomatic or of significant size, to address pain and rule out malignancy [2:32].
- Infertility associated with distorted pelvic anatomy or advanced stages of disease [2:33].
- Surgical Limits and Risks: Surgery is technically demanding due to the obliteration of normal tissue planes. Surgical intervention carries risks of visceral injury and pelvic adhesions [2:34][1:32][6:8]. There is no clear consensus regarding the absolute benefit of surgical intervention for endometriosis-associated infertility [2:35][1:33][6:9].
¶ 5. Non-pharmacological and Adjunctive Care
- Pelvic-Floor Physical Therapy (PFPT): Target-directed therapy for secondary hypertonic pelvic floor dysfunction. Chronic visceral pelvic pain induces protective muscle guarding, leading to chronic pelvic floor spasm and myofascial tension [10:1]. Physical therapy techniques, including massage combined with perineal stretching, exercise, and education, are effective at reducing chronic pelvic pain and dyspareunia [16]. Alternatively, a multimodal outpatient neuromuscular protocol consisting of pelvic floor physical therapy, trigger point injections, peripheral nerve blocks, and cognitive behavioral therapy can be utilized to decrease pain and improve sexual function [17].
- Unidisciplinary/Multidisciplinary Pain Clinics: Integrating pain specialists, gynecologists, pelvic physiotherapists, and pain psychologists (employing cognitive behavioral therapy and mindfulness-based stress reduction) is critical to address the neuropathic and psychosocial layers of chronic pain [1:34].
- Dietary and Lifestyle Adjustments:
- Anti-inflammatory Dietary Patterns: Transitioning to dietary patterns such as the Mediterranean diet can support overall nutritional status and manage symptoms, although strong evidence for a specific superior diet is limited [18].
- Antioxidant Supplementation: Systematic reviews and meta-analyses demonstrate that oral supplementation with Vitamin E (alone or combined with Vitamin C) can help reduce chronic pelvic pain and dysmenorrhea [19].
- Regular Physical Activity: Structured exercise (aerobic training, yoga) may improve pain intensity and physical functioning, although overall clinical evidence remains limited [20].
¶ Key Clinical Considerations
¶ 1. Central Sensitization and CPPS
Persistent, chronic nociceptive input from pelvic endometrial lesions drives neuroplastic changes in the dorsal horn of the spinal cord and central nervous system, a process known as central sensitization [10:2][9:1]. Over time:
- Hyperalgesia and Allodynia: The threshold for pain activation is lowered; non-painful pelvic stimuli (such as bowel/bladder filling or light touch) are perceived as painful [10:3][9:2].
- Decoupling of Pain from Lesion Burden: The pain pathway becomes independent of the physical lesions [10:4]. Consequently, surgical removal of all visible implants may fail to resolve pain because the central pain processing pathways remain hyper-reactive, establishing Chronic Pelvic Pain Syndrome (CPPS) [10:5][9:3]. Multimodal therapies targeting the nervous system (e.g., gabapentinoids, amitriptyline, PFPT) are necessary to manage this neuropathic component.
¶ 2. Fertility Management
Endometriosis impairs fertility through anatomical distortion, chronic intraperitoneal inflammation, and compromised oocyte quality [2:36][1:35].
- Surgical Management: There is no clear consensus regarding the absolute benefit of surgical intervention for endometriosis-associated infertility, and surgical intervention carries risks of visceral injury and pelvic adhesions [2:37][1:36][6:10].
- Assisted Reproductive Technology (ART) / IVF: Recommended for patients with compromised tubal function, advanced maternal age, or diminished ovarian reserve [2:38]. Pre-treatment with continuous medical suppression (such as GnRH agonists or continuous progestins) prior to embryo transfer is utilized in clinical practice to support pregnancy outcomes [2:39].
Patient with Endometriosis-Associated Infertility
│
┌─────────────────────┴─────────────────────┐
▼ ▼
Anatomical Distortion / Tubal Factor /
Younger Age Advanced Age
│ │
▼ ▼
Laparoscopic Excision Direct Referral to IVF
(Restore anatomy, excise cyst) │
│ ▼
▼ Pre-Transfer suppression
Spontaneous Conception Trial (GnRH Therapy)
(1 Year) │
│ ▼
┌─────────┴─────────┐ Embryo Transfer
▼ ▼
Successful Unsuccessful ──► Referral to IVF
¶ 3. Recurrence Rates and Post-Operative Suppression Strategies
Endometriosis is a chronic condition with high recurrence rates after surgery [2:40][1:37].
- Recurrence Risk: Endometriosis is a chronic condition with a high likelihood of symptom recurrence and persistence following surgery if no post-operative medical suppression is utilized [2:41][1:38][12:2].
- Prevention Strategy: Long-term medical suppression must be initiated immediately after surgery unless the patient is actively attempting conception [2:42]. Continuous COCs, oral progestins (such as dienogest 2 mg daily), or the LNG-IUS are highly effective at suppressing micro-residual disease, reducing pain recurrence, and preventing the reformation of endometriomas [2:43][12:3][13:4].
¶ 4. Evidence Gaps
Despite its high prevalence, significant gaps remain in our understanding and clinical management of endometriosis [1:39]:
- Diagnostic Delay: Addressing the average 5 to 12-year diagnostic delay remains a critical research and clinical priority, with a focus on improving primary care clinical recognition and developing non-invasive diagnostic pathways to initiate early empirical treatment [3:6][4:6].
- Non-Hormonal Therapeutic Targets: Current medical therapies rely on suppressing ovulation and systemic estrogen, which prevents conception and causes menopausal side effects. Evidence gaps remain, particularly the need to determine clinically informative sub-classifications of endometriosis that predict prognosis, enhance treatment prioritization, and identify non-hormonal therapeutic targets [1:40][5:12].
¶ Evidence Summary Table (Human Outcomes)
The following matrix summarizes the therapeutic effects of key endometriosis interventions based on pooled human clinical trials and meta-analyses.
| Intervention | Target Outcome | Effect* | Consistency | Evidence Quality | Clinical Context & Protocols | Notes / References |
|---|---|---|---|---|---|---|
| Combined Oral Contraceptives | Dysmenorrhea | High | High | Monophasic COCs taken continuously (amenorrhea protocol); suppresses ovarian activity. [2:44][6:11][5:13] | [2:45], [6:12], [5:14] | |
| Combined Oral Contraceptives | Deep Dyspareunia | Moderate | Moderate | Moderate relief; local tissue stretch is often not fully resolved by standard COCs. [5:15][14:2] | [5:16], [14:3] | |
| Dienogest (Progestin) | Dysmenorrhea | High | High | Oral dosing of 2 mg daily continuously; induces endometrial tissue atrophy and decidualization. [5:17][13:5][14:4] | [5:18], [13:6], [14:5] | |
| Dienogest (Progestin) | Deep Dyspareunia | High | High | Shows comparable efficacy and pain reduction to standard COCs in head-to-head randomized trials over 6 months. [14:6] | [14:7] | |
| GnRH Antagonists (Elagolix) | Dysmenorrhea | High | High | Oral dosing (150 mg QD or 200 mg BID); dose-dependent pain relief; monitored for bone density loss. [7:7][5:19] | [7:8], [5:20] | |
| Relugolix Combo Therapy | Dysmenorrhea | High | High | Once-daily co-formulated oral relugolix 40 mg, estradiol 1 mg, NETA 0.5 mg; preserves BMD. [8:6][15:2] | [8:7], [15:3] | |
| Relugolix Combo Therapy | Non-Menstrual Pelvic Pain | High | High | Sustained reduction in chronic non-menstrual pelvic pain demonstrated up to 104 weeks. [15:4] | [15:5] | |
| Laparoscopic Excision | Dysmenorrhea / Pelvic Pain | Moderate | Moderate | Superior to ablation; short-term relief is high, but pain often recurs without suppressive meds. [2:46][1:41][6:13] | [2:47], [1:42], [6:14] | |
| Laparoscopic Excision | Spontaneous Fertility | Moderate | Moderate | Some guidelines suggest potential benefit, but clinical consensus regarding the absolute fertility benefit of surgical intervention remains limited [2:48][1:43][6:15]. | [2:49], [1:44], [6:16] | |
| Pelvic Floor Physical Therapy | Dyspareunia / CPPS | High | Moderate | Physical therapy techniques including massage combined with perineal stretching, exercise, and education. [16:1] | [16:2] | |
| Antioxidant Supplementation | Chronic Pelvic Pain | Moderate | Moderate | Oral Vitamin E (with or without Vitamin C) can help reduce chronic pelvic pain and dysmenorrhea. [19:1] | [19:2] | |
| Structured Exercise | Pain and Fatigue | Moderate | Moderate | Structured exercise (aerobic training, yoga) may improve pain intensity and physical functioning, although overall clinical evidence remains limited [20:1] | [20:2] |
*Compact renderer encoding: <effect e="d2p"></effect> where the three-character e attribute code is composed of direction (u/d/e/q), magnitude (0–3), and health impact (p/n/x).
¶ Safety, Contraindications, and Red Flags
¶ 1. Emergency Mimics & Red Flags
Clinical presentation of acute, severe pelvic pain must be screened for emergency conditions that mimic endometriosis or represent direct complications [2:50][1:45][3:7][4:7]:
- Ectopic Pregnancy: Rupture of an ectopic pregnancy presents as acute pelvic pain, hypotension, shoulder tip pain, and peritonitis.
- Ovarian Torsion or Ruptured Endometrioma: Presents as sudden, localized, severe abdominal or pelvic pain, often unilateral, accompanied by signs of an acute abdomen (rebound tenderness, guarding).
- Sepsis / Pelvic Abscess: Indicated by high fever, purulent vaginal discharge, chills, and severe pelvic tenderness, requiring immediate diagnostic imaging and intravenous antibiotics.
¶ 2. Clinical Contraindications
Specific therapies in the endometriosis armamentarium carry strict absolute and relative contraindications:
- GnRH Therapies (Without Add-Back):
- Dienogest or Progestin-Only Therapies: Dienogest 2 mg is well tolerated in clinical practice; pooled trials show a favorable safety profile over up to 65 weeks, with common mild-to-moderate side effects including changes in bleeding patterns, headache, breast discomfort, or depressed mood (<10%) [13:7]. The VIPOS study is an observational cohort designed to monitor long-term real-world safety outcomes [12:4].
- Combined Oral Contraceptives:
- Contraindications: Standard prescribing guidelines (such as the WHO Medical Eligibility Criteria for Contraceptive Use) list absolute contraindications including women >35 years who smoke, history of venous thromboembolism, known thrombophilic disorders, migraine with aura, and uncontrolled hypertension.
- Surgical Excision:
- Contraindications: Asymptomatic pelvic lesions discovered incidentally (exposing the patient to surgical risk without symptomatic benefit) [2:51].
- Precautions: Any surgical intervention carries risks of visceral injury and pelvic adhesions, and there is no clear consensus regarding the absolute benefit of surgical intervention for endometriosis-associated infertility [2:52][1:46][6:17].
¶ FAQ
¶ Does pregnancy cure endometriosis?
No, pregnancy does not cure endometriosis. Because endometriosis is a chronic, systemic inflammatory disease characterized by ectopic lesions, clinical symptoms and lesions typically persist or recur over time [1:47]. There is no clinical evidence that pregnancy eradicates the underlying disease, and symptoms often recur after delivery and menses resume.
¶ Is laparoscopy always required for diagnosis?
No. International guidelines (including ESHRE 2022) state that a clinical diagnosis supported by transvaginal ultrasound or MRI is sufficient to establish a diagnosis and initiate medical therapy [2:53][3:8]. Laparoscopy is reserved for therapeutic excision or when non-invasive imaging is negative but clinical suspicion remains high [2:54][1:48].
¶ Can diet alone manage endometriosis symptoms?
No. While transitioning to dietary patterns such as the Mediterranean diet can support overall nutritional status and manage symptoms, and antioxidant supplementation (such as Vitamins C and E) can reduce pelvic pain, they do not halt or reverse the growth of ectopic lesions [19:3]. Dietary modifications are adjunctive measures to be integrated with first-line medical suppressive therapies [18:1].
¶ References
Horne AW, Missmer SA. Pathophysiology, diagnosis, and management of endometriosis. BMJ. 2022. https://pubmed.ncbi.nlm.nih.gov/36375827/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Becker CM, Bokor A, Heikinheimo O, Horne A, Jansen FFW, Kiesel L, King K, Montesinos M, Saridogan E, Vermeulen N, ESHRE Endometriosis Guideline Group. ESHRE guideline: endometriosis. Human Reproduction Open. 2022. https://pubmed.ncbi.nlm.nih.gov/35350465/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Crump J, Suker A, White L, et al. Endometriosis: A review of recent evidence and guidelines. Australian Journal of General Practice. 2024. https://pubmed.ncbi.nlm.nih.gov/38316472/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
As-Sanie S, Mackenzie SC, Morrison L. Endometriosis: A Review. JAMA. 2025. https://pubmed.ncbi.nlm.nih.gov/40323608/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kou L, Huang C, Xiao D. Pharmacologic Interventions for Endometriosis-Related Pain: A Systematic Review and Meta-analysis. Obstetrics and Gynecology. 2025. https://pubmed.ncbi.nlm.nih.gov/40373315/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kalaitzopoulos DR, Samartzis N, Kolovos GN, et al. Treatment of endometriosis: a review with comparison of 8 guidelines. BMC Women's Health. 2021. https://pubmed.ncbi.nlm.nih.gov/34844587/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Taylor HS, Giudice LC, Lessey BA, et al. Treatment of Endometriosis-Associated Pain with Elagolix, an Oral GnRH Antagonist. The New England Journal of Medicine. 2017. https://pubmed.ncbi.nlm.nih.gov/28525302/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Giudice LC, As-Sanie S, Arjona Ferreira JC, et al. Once daily oral relugolix combination therapy versus placebo in patients with endometriosis-associated pain: two replicate phase 3, randomised, double-blind, studies (SPIRIT 1 and 2). The Lancet. 2022. https://pubmed.ncbi.nlm.nih.gov/35717987/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Meisenheimer ES, Carnevale AM. Chronic Pelvic Pain in Women: Evaluation and Treatment. American Family Physician. 2025. https://pubmed.ncbi.nlm.nih.gov/40106288/ ↩︎ ↩︎ ↩︎ ↩︎
Aredo JV, Heyrana KJ, Karp BI. Relating Chronic Pelvic Pain and Endometriosis to Signs of Sensitization and Myofascial Pain and Dysfunction. Seminars in Reproductive Medicine. 2017. https://pubmed.ncbi.nlm.nih.gov/28049214/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Thomassin-Naggara I, Dolciami M, Chamie LP, et al. ESUR consensus MRI for endometriosis: protocol, lexicon, and compartment-based analysis. European Radiology. 2025. https://pubmed.ncbi.nlm.nih.gov/40425755/ ↩︎ ↩︎ ↩︎
Heinemann K, Imthurn B, Marions L, et al. Safety of Dienogest and Other Hormonal Treatments for Endometriosis in Real-World Clinical Practice (VIPOS): A Large Noninterventional Study. Advances in Therapy. 2020. https://pubmed.ncbi.nlm.nih.gov/32301063/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Strowitzki T, Faustmann T, Gerlinger C, et al. Safety and tolerability of dienogest in endometriosis: pooled analysis from the European clinical study program. International Journal of Women's Health. 2015. https://pubmed.ncbi.nlm.nih.gov/25926759/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
El Taha L, Abu Musa A, Khalifeh D, et al. Efficacy of dienogest vs combined oral contraceptive on pain associated with endometriosis: Randomized clinical trial. European Journal of Obstetrics, Gynecology, and Reproductive Biology. 2021. https://pubmed.ncbi.nlm.nih.gov/34826668/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Becker CM, Johnson NP, As-Sanie S, et al. Two-year efficacy and safety of relugolix combination therapy in women with endometriosis-associated pain: SPIRIT open-label extension study. Human Reproduction. 2024. https://pubmed.ncbi.nlm.nih.gov/38243752/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Mena-González A, et al. Effectiveness of physical therapy techniques and methods in the management of endometriosis symptoms: A systematic review with meta-analysis. Brazilian Journal of Physical Therapy. 2026. https://pubmed.ncbi.nlm.nih.gov/42308873/ ↩︎ ↩︎ ↩︎
Shrikhande A, Patil S, Subhan M. A Comprehensive Treatment Protocol for Endometriosis Patients Decreases Pain and Improves Function. International Journal of Women's Health. 2023. https://pubmed.ncbi.nlm.nih.gov/36713131/ ↩︎
Lalla AT, Onyebuchi C, Jorgensen E. Impact of lifestyle and dietary modifications for endometriosis development and symptom management. Current Opinion in Obstetrics & Gynecology. 2024. https://pubmed.ncbi.nlm.nih.gov/38869435/ ↩︎ ↩︎
Zheng SH, Chen XX, Chen Y, et al. Antioxidant vitamins supplementation reduce endometriosis related pelvic pain in humans: a systematic review and meta-analysis. Reproductive Biology and Endocrinology. 2023. https://pubmed.ncbi.nlm.nih.gov/37644533/ ↩︎ ↩︎ ↩︎ ↩︎
Tennfjord MK, Gabrielsen R, Tellum T. Effect of physical activity and exercise on endometriosis-associated symptoms: a systematic review. BMC Women's Health. 2021. https://pubmed.ncbi.nlm.nih.gov/34627209/ ↩︎ ↩︎ ↩︎