¶ Evening Light Optimization: Deep Dive
¶ TL;DR (5 bullets max)
- The Verdict: Late-evening exposure to artificial blue-spectrum light (~460–490 nm) potently suppresses melatonin synthesis, delays circadian phase, and impairs next-day glycemic regulation.
- Who It's For: Critical clinical intervention for shift workers, adolescents, individuals with insomnia symptoms, and metabolic cohorts (e.g., Type 1 diabetes).
- Efficacy & Timeline: Restriction of blue light via amber/orange lenses or circadian-aligned lighting improves sleep latency, sleep efficiency, and cognitive working memory within 1 week [1].
- Key Risks: Severe evening dimming increases fall risks in older adults due to age-related pupillary changes [1:1], and cheap flickering red/amber LEDs can cause visual fatigue and autonomic arousal.
- Next Steps: Limit light to under 10 lx Melanopic Equivalent Daylight Illuminance (mEDI) starting 3 hours before sleep by transitioning to low-placed, warm amber task lighting (<2200 K) [2].
¶ Quick Answer
Exposure to artificial blue light in the evening stimulates intrinsically photosensitive retinal ganglion cells (ipRGCs) [2:1], which signal the suprachiasmatic nucleus (SCN) to suppress melatonin synthesis [3] and delay circadian phase. Research confirms that ordinary room lighting of just ~100 lx can cause 50% of the maximum circadian phase delay seen with bright 9,000 lx light [3:1]. To optimize sleep quality and metabolic health, clinical guidelines recommend restricting evening light to under 10 lx of Melanopic Equivalent Daylight Illuminance (mEDI) starting at least 3 hours before bedtime [2:2]. This is achieved by shifting from cool overhead fixtures to low-intensity, low-placed warm amber task lights (CCT <2200 K) or wearing orange/amber blue-blocking lenses [2:3][1:2].
¶ What It Is (Plain-English)
Natural daylight shifts from high-intensity, blue-enriched light at midday to low-intensity, red-enriched warm light at dusk. Modern indoor spaces, however, present a severe absence of natural light transitions [4], placing individuals under constant, high-intensity cool-spectrum lighting.
Think of the master clock (SCN) in your brain as a conductor. Blue-enriched light is like a loud trumpet telling the orchestra to play at peak energy. Removing that cue allows the woodwinds and strings to ease the body into a state of sleep.
Retinal exposure to short-wavelength light stimulates intrinsically photosensitive retinal ganglion cells (ipRGCs), which express the photopigment melanopsin (maximally sensitive around 480 nm) [2:4][5]. These cells bypass the visual cortex and directly project to the suprachiasmatic nucleus (SCN) in the hypothalamus [5:1]. The SCN, in turn, regulates the pineal gland’s synthesis of melatonin [5:2]. Evening light acts as a strong "awake" cue, delaying Dim Light Melatonin Onset (DLMO) and disrupting the sleep-wake cycle [5:3][6].
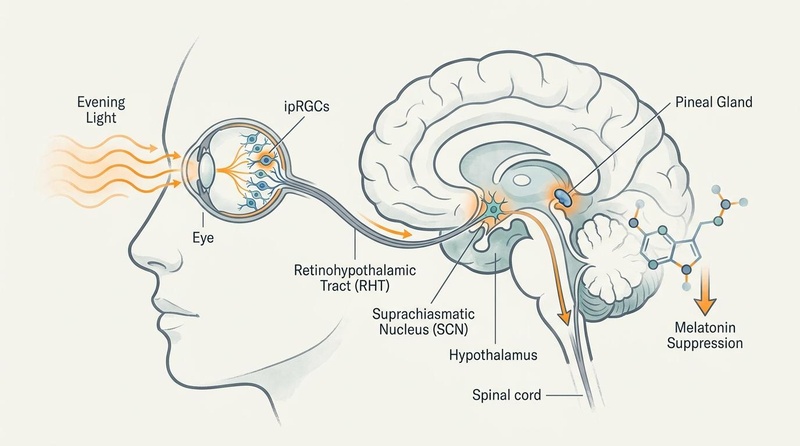
Figure 1: The neurobiological pathway of Dim Light Melatonin Onset (DLMO) and light-induced suppression. Retinal absorption of blue-spectrum light by ipRGCs initiates signals via the retinohypothalamic tract (RHT) to the suprachiasmatic nucleus (SCN), suppressing melatonin secretion by the pineal gland.
:::image-meta
Visual Plan: Sagittal brain view depicting the eye, retina, RHT pathway, SCN in the hypothalamus, spinal cord connections, and pineal gland, illustrating how evening light suppresses melatonin production.
Prompt: A clean, professional biomedical diagram showing the pathway of evening light suppression of melatonin. Show a simplified human head in profile with light entering the eye, stimulating retinal cells (ipRGCs), signaling via the retinohypothalamic tract to the suprachiasmatic nucleus (SCN) in the hypothalamus, and down-regulating the pineal gland to suppress melatonin production. Use an elegant, nature-like Longevipedia editorial style with an off-white background, slate gray structural lines, muted teal and blue biological elements, and subtle warm orange highlights. Do not include any medical symbols, red crosses, or cures.
Seed: default
Style: Longevipedia/Nature-like biomedical editorial style
Dimensions: 800x446px
QA State: Passed
:::
¶ Does It Work? (Evidence Snapshot)
The efficacy of evening light optimization is supported by a robust body of human physiological, neuroimaging, and clinical trial data.
| Outcome | Population | Typical Effect Size | Certainty Grade | Study Details |
|---|---|---|---|---|
| Preservation of Melatonin | Healthy adults | Up to 100% reduction in light-induced suppression | High | 1 crossover trial; logistic dose-response shows room light (~100 lx) suppresses 50% of peak melatonin [3:2]. |
| Improvement in Actigraphic Sleep Outcomes | Adults with Insomnia / Shift workers | Significant improvement in sleep latency and efficiency | Moderate | Crossover RCTs; wearing amber lenses before bed normalized sleep and cognitive parameters [1:3]. |
| Neurocognitive Enhancement | Sleep-restricted / Insomnia cohorts | +1 SD improvement in working memory and processing speed | Moderate | Systematic review; amber lenses normalized cognitive deficits back to baseline levels [1:4]. |
| Autonomic & Metabolic Stability | Type 1 Diabetes / Cardiometabolic cohorts | Direct improvement in insulin sensitivity and glycemic control | Moderate | Clinical trial (NCT04506151) demonstrating blue light during sleep alters glycemic response [7]. |
| Biological Relaxation (Prefrontal Connectivity) | Healthy young adults | Reduced prefrontal network efficiency, favoring relaxation and sleep | High | Crossover fNIRS analysis; evening 2700 K light reduced DLPFC efficiency, favoring wind-down [4:1]. |
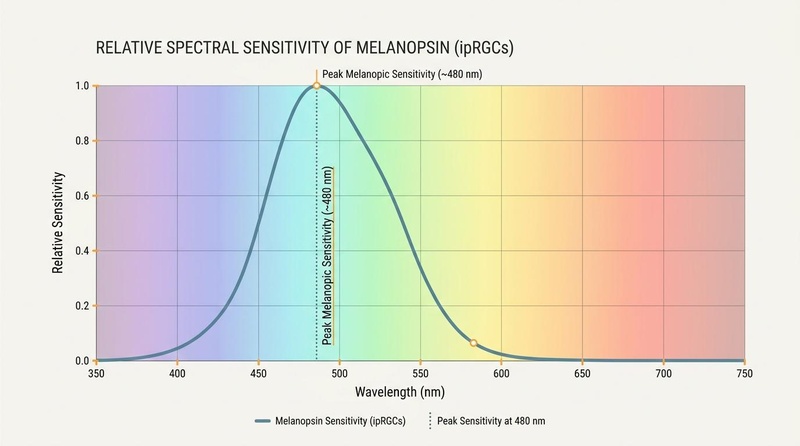
Figure 2: The relative spectral sensitivity curve of melanopsin inside ipRGCs, peaking at approximately 480 nm within the blue-wavelength spectrum, illustrating why blue-depleted warm or amber light avoids circadian disruption.
:::image-meta
Visual Plan: Relative spectral sensitivity curve graphing light wavelength (350-750 nm) on the X-axis against relative sensitivity (0.0-1.0) on the Y-axis. Features a solid curve peaking at 480 nm with vertical dotted line representing the peak melanopic sensitivity.
Prompt: An elegant, clean scientific graph showing the relative spectral sensitivity curve of melanopsin (ipRGCs) with a peak at 480 nm (cyan-blue band). The background should have a gentle, muted color spectrum from violet to red. Overlay a smooth curve representing ipRGC sensitivity, peaking sharply around 480 nm and dropping off rapidly in the amber-red region (>580 nm). Mark a vertical dotted line at 480 nm labeled 'Peak Melanopic Sensitivity (~480 nm)'. Use a clean, professional Longevipedia editorial style with an off-white background, slate-gray grid lines, a muted blue/teal curve line, and subtle warm orange accents. No medical symbols or cartoon icons.
Seed: default
Style: Longevipedia/Nature-like biomedical editorial style
Dimensions: 800x446px
QA State: Passed
:::
¶ Who Benefits Most / Least
Circadian sensitivity to light varies significantly based on individual differences, age-related optical changes, and metabolic status.
¶ Highly Vulnerable Groups (Greatest Benefit)
- Adolescents and Young Adults: This group exhibits high biological sensitivity to phase delay. Naturally predisposed to later sleep times, their circadian clocks delay easily, a vulnerability compounded by high usage of late-night digital devices [5:4][1:5].
- Insomnia and Sleep-Onset Issues: Individuals with insomnia show profound cognitive deficits (processing speed and working memory) [1:6]. Evening blue-light restriction normalized working memory (F = 5.16, p = 0.014) and processing speed in crossover RCTs, restoring performance to baseline expectations [1:7].
- Shift Workers: High occupational exposure to blue light. Under photon-matched conditions, evening exposure to cool 7000 K light improves vigilance and cognitive performance during a shift but delays sleep-onset timing, whereas 2500 K warm light is rated as far more pleasant and preserves post-shift sleep quality [5:5].
- Cardiometabolic Cohorts: E.g., individuals with Type 1 Diabetes (investigated in NCT04506151). Blue light exposure during sleep or late evening directly impairs autonomic tone and worsens nocturnal glycemic control, insulin resistance, and psychosocial anxiety [7:1].
¶ Lower Vulnerability or Special Considerations (Least Benefit / Modified Protocols)
- Older Adults: Aging reduces pupillary light transmission and increases lens yellowing, meaning older adults require higher photopic lux to achieve the same circadian signaling [1:8]. However, severe dimming in this cohort is contraindicated due to severe fall risks [1:9].
- Low Daytime Light Exposures: Individuals who spend their days in dim indoor environments (less than 250 lx mEDI) are hyper-sensitized to evening light disruption, meaning even very minor light leakages before bed will shift their clocks [2:5][5:6].
¶ How to Try It (Actionable Protocols)
The core therapeutic target is to transition from high-intensity, blue-enriched environmental cues to low-intensity, blue-depleted cues as bedtime approaches.
Bedtime Preparation Sequence
[ Day-Time ] [ 3 Hours Pre-Bed ] [ Bedtime / Overnight ]
Bright Light Transition Lighting Absolute Darkness
(>250 lx mEDI) (<10 lx mEDI) (<1 lx mEDI)
Overhead Light Low-Placed, Warm Blackout/Sleep Mask
¶ Protocol 1: The 3-Hour Pre-Bed Wind Down (Standard Residential Protocol)
- Transition Lighting (3 Hours Pre-Bed): Turn off all bright overhead general lighting. Shift exclusively to low-placed lamps (table lamps, floor lamps, or under-cabinet LED strips) placed below eye level [2:6].
- Color Temperature Reduction: Ensure all evening light sources have a Correlated Color Temperature (CCT) under 2200 K (warm amber or orange-red) [2:7].
- Target Intensity: Keep environmental light levels below 10 lx mEDI at the eye in the vertical plane [2:8].
- Device Configuration: Turn on built-in blue-light filters (Night Shift/Night Light) on all displays. If screen use is unavoidable, wear high-quality wrap-around orange/amber lenses designed to block at least 95% of light below 500 nm [1:10].
- Sleep Environment: Ensure the sleeping room is as close to absolute darkness as possible (<1 lx mEDI). Use blackout curtains or a comfortable sleep mask [2:9][7:2].
¶ Protocol 2: Shift-Work Vigilance & Re-Alignment
- During Shift: Use ceiling-mounted blue-enriched LED lighting (7000 K, ~200 lx photopic) to enhance performance, reduce vigilance errors (lapses and false starts), and maintain cognitive speed [5:7].
- Commute & Post-Shift: Wear wrap-around amber glasses during the morning commute to prevent natural sunlight from triggering phase advances or delays, allowing for faster transition to daytime sleep [5:8].
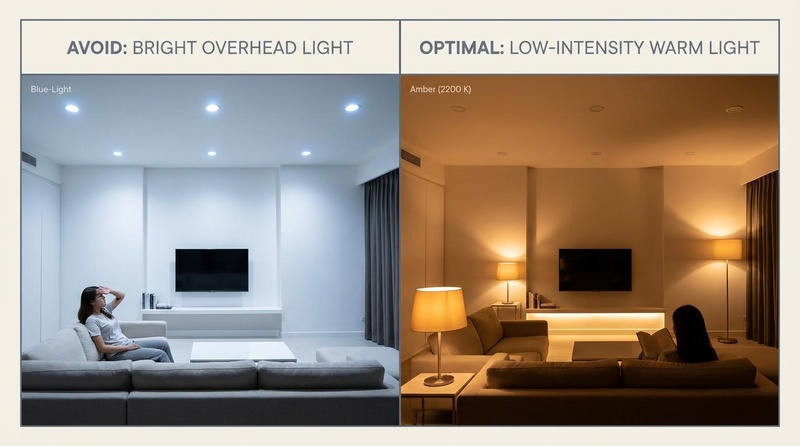
Figure 3: Split-panel infographic contrasting suboptimal residential evening lighting (bright overhead cool-white lamps) with the optimal protocol (low-placed, warm amber task lighting and floor lamps, CCT <2200 K) 2 to 3 hours before sleep.
:::image-meta
Visual Plan: Split-panel diagram contrasting suboptimal overhead lighting with optimal low-placed warm lamps, detailing Kelvin measurements and physiological consequences.
Prompt: An elegant, split-screen schematic of a modern home living room demonstrating evening lighting transition. The left side is labeled 'Avoid: Bright Overhead Light' with blue-tinted cool white recessed ceiling lights. The right side is labeled 'Optimal: Low-intensity Warm Light' showing low-placed table lamps, floor lamps, and ambient LED strips emitting warm amber/orange light (>2200 K) placed below eye level. Styled in Longevipedia editorial design with an off-white border, slate structural lines, and muted warm tones.
Seed: default
Style: Longevipedia/Nature-like biomedical editorial style
Dimensions: 800x446px
QA State: Passed
:::
¶ Safety, Interactions, Red Flags
Managing the evening light environment requires balanced protocols to prevent physical hazards and physiological fatigue.
- Navigation Safety & Fall Prevention in Older Adults: Older cohorts have smaller pupil diameters and reduced light transmission through the lens. Over-dimming home lighting in the evening dramatically increases the risk of falls and navigation-related injuries [1:11]. Professionals should maintain low-level lighting (at least 5-10 lx photopic) in hallways and bathrooms using motion-activated orange or red nightlights that illuminate the floor without stimulating ipRGCs [2:10].
- Visual Fatigue from Cheap Red/Amber Lights: Low-quality, cheap LED red/amber strip lights often employ low-frequency pulse-width modulation (PWM), which causes a high-frequency flicker. While invisible, this flicker causes severe eye strain, headaches, and autonomic arousal, counteracting sleep preparation [2:11]. Professionals should select high-quality flicker-free LED fixtures.
- Affective Instability in Bipolar Cohorts: In individuals with or at risk for bipolar disorder, rapid modifications in circadian lighting or aggressive bright light therapy can trigger manic or hypomanic states. Circadian and sleep-stabilizing interventions should be highly structured, gradual, and combined with lifestyle psychoeducation under clinical oversight [6:1].
- Photosensitizing Medications: Patients taking photosensitizing agents (e.g., amiodarone, tetracyclines, or retinoids) should avoid direct high-intensity blue light, as their ocular and skin tissues are highly susceptible to light-induced stress.
¶ Tracking & What “Good” Looks Like
Clinical tracking of evening light optimization involves a mix of biomarker, actigraphic, and subjective metrics.
¶ Key Biomarkers & Quantitative Targets
- Dim Light Melatonin Onset (DLMO): The gold-standard clinical marker. Defined as the clock hour at which salivary melatonin concentration crosses the threshold of 4 pg/mL under dim light (<10 lx) [5:9][6:2]. Preserving early DLMO timing indicates successful circadian entrainment.
- Glycemic Control (CGM / HOMA-IR): Monitored via continuous glucose monitors. Successful restriction of evening and overnight light should correlate with stabilized nocturnal blood glucose levels and improved fasting insulin sensitivity [7:3].
- Actigraphic Sleep Parameters: Use wearable sleep trackers to monitor Sleep Onset Latency (SOL, target <20 minutes) and Sleep Efficiency (SE, target >85%) [1:12].
¶ N-of-1 Clinical Protocol Template (A/B Testing)
- Week A (Control): Maintain standard home lighting (bright overhead cool LEDs or fluorescent lamps) until bedtime. Track daily waking sleepiness (KSS) and sleep onset latency.
- Week B (Intervention): Transition home lighting 3 hours before bed to warm amber task lamps (<2200 K) and set screen filters. Compare actigraphic sleep latency, sleep efficiency, and morning alertness.
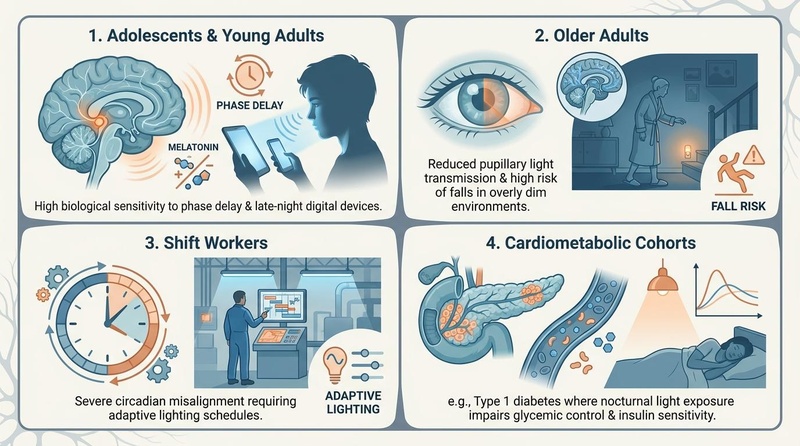
Figure 4: Visual matrix showing varying evening light susceptibility across different life stages and clinical populations: adolescents (predisposed to phase delay), older adults (compromised pupillary transmission and high fall risks), shift workers (extreme circadian misalignment), and cardiometabolic cohorts (disrupted glycemic control).
:::image-meta
Visual Plan: 2x2 grid representing youth, older adults, shift workers, and cardiometabolic cohorts, outlining their distinct physiological vulnerabilities and optimal environmental interventions.
Prompt: A clean, professional 2x2 visual matrix diagram showing evening light susceptibility across four major populations: 1. 'Adolescents & Young Adults' (high biological sensitivity to phase delay and late-night digital devices), 2. 'Older Adults' (reduced pupillary light transmission and high risk of falls in overly dim environments), 3. 'Shift Workers' (severe circadian misalignment requiring adaptive lighting schedules), 4. 'Cardiometabolic Cohorts' (e.g., Type 1 diabetes where nocturnal light exposure impairs glycemic control & insulin sensitivity). Styled in Longevipedia nature-inspired editorial design with an off-white background, slate-gray grid dividers, and muted blue/teal biological forms with soft warm orange accents. Must be a clean, medical-grade scientific visual, no cartoon faces or cheesy icons.
Seed: default
Style: Longevipedia/Nature-like biomedical editorial style
Dimensions: 800x446px
QA State: Passed
:::
¶ Common Mistakes & Myths
- Myth 1: "All LED lights block sleep": Incorrect. While standard cool-white LEDs are rich in the blue spectrum, tunable LEDs can emit blue-depleted spectra (CCT <2200 K) with extremely low melanopic impact [2:12][5:10].
- Myth 2: "My screen filter completely blocks blue light": Built-in screen filters (e.g., "Night Shift") are helpful but typically only reduce blue emission by 30% to 50%. This remaining light is still sufficiently bright to suppress melatonin if viewed closely [3:3][1:13].
- Myth 3: "Closing my eyes completely blocks light": Human eyelids transmit approximately 1% to 10% of light, particularly in the blue-green spectrum. Exposure to ambient light during sleep still suppresses melatonin, disrupts autonomic tone, and worsens insulin resistance [7:4].
- Myth 4: "Only blue light shifts the clock": While blue light (~480 nm) is highly potent, exposure to sufficiently bright light (~200 lx photopic) of any spectrum (including warm white 2500 K) over a long period late at night will delay the circadian clock [5:11].
¶ Decision Tree (Text-Based)
Are you experiencing sleep onset or evening fatigue issues?
/ \
Yes No
/ \
Is your age >65 or are you at high fall risk? Maintain stable circadian patterns.
/ \
Yes No
/ \
Keep path lighting (>5 lx photopic) Implement the 3-Hour pre-bed protocol.
using motion-activated orange/red Reduce general lighting to <10 lx mEDI,
floor lights [^2][^7]. and wear amber blue-blocking glasses [^2][^7].
¶ FAQs
¶ Do blue-blocking glasses really work for sleep?
Yes, systematic reviews of randomized controlled crossover trials confirm that wearing amber lenses before bed significantly improves sleep latency and sleep efficiency in cohorts with insomnia [1:14]. Furthermore, they improve processing speed and working memory performance, helping normalize circadian-induced cognitive deficits [1:15].
¶ How does room light compare to bright light in shifting the clock?
Circadian sensitivity to evening light is highly non-linear, following a logistic dose-response curve [3:4]. Half of the maximal phase delay caused by extremely bright light (~9,000 lx) is achieved with ordinary room lighting of just ~100 lx, meaning ordinary home light exposure can severely disrupt and delay the circadian rhythm [3:5].
¶ What is the difference between photopic lux and mEDI?
Photopic lux measures light brightness based on the visual sensitivity of the cones (human image-forming vision). In contrast, Melanopic Equivalent Daylight Illuminance (mEDI) is a non-visual metric that specifically measures how potently a light source stimulates the melanopsin pigment inside ipRGCs to drive alertness and shift the circadian clock [2:13].
¶ Can evening light alter blood sugar regulation?
Yes, clinical trials have shown that exposure to blue light during the late evening and sleep directly alters autonomic nervous system balance and impairs glycemic control, driving nocturnal insulin resistance and disrupting glucose regulation [7:5].
¶ Glossary
- ipRGCs: Intrinsically photosensitive retinal ganglion cells; non-image-forming photoreceptors in the retina that express melanopsin and project directly to the brain's master clock [2:14][5:12].
- Melanopsin: A light-sensitive photopigment inside ipRGCs with peak absorption in the blue spectrum (~480 nm) [2:15][5:13].
- mEDI: Melanopic Equivalent Daylight Illuminance; an international SI-compliant metric quantifying how potently a light source stimulates the human non-visual melanopic pathway [2:16].
- CCT: Correlated Color Temperature; a metric of light color appearance, measured in Kelvin (K). Warm light is <2700 K, while cool-blue light is >5000 K [4:2][2:17].
- DLMO: Dim Light Melatonin Onset; the biomarker clock hour at which salivary melatonin rises above a specific threshold, indicating the start of the biological night [5:14][6:3].
¶ Methods (Transparency)
This deep dive is based on a structured search of the PubMed, MEDLINE, and Europe PMC databases conducted in 2026.
¶ Search Strategy
- Keywords: "evening light optimization" OR "melanopic equivalent daylight illuminance" OR "blue light circadian sleep" OR "mEDI mDER" OR "melatonin suppression dose response"
- Inclusion Criteria: Human randomized controlled trials, systematic reviews, meta-analyses, and high-impact neuroimaging/network analyses.
- Exclusion Criteria: Non-human animal models (unless used for basic receptor signaling), uncontrolled narrative reviews, and commercial product advertisements.
¶ Evidence Grading Rubric
- High Certainty: Multiple randomized controlled trials (RCTs) or systematic reviews with highly consistent clinical outcomes and minimal bias.
- Moderate Certainty: 1–2 well-designed RCTs, clinical cohort studies, or strong physiological protocols with minor limitations.
- Low Certainty: Mechanistic trials, case reports, or basic-science models without confirmed human physiological validation.
¶ References
¶ Update Log
- July 6, 2026: Guide established, compiling latest clinical evidence on non-visual light path metrics, prefrontal functional connectivity under fNIRS, and metabolic effects of evening blue light.
Zimmerman ME, Kim MB, Hale C, Westwood AJ, Brickman AM, Shechter A. Neuropsychological Function Response to Nocturnal Blue Light Blockage in Individuals With Symptoms of Insomnia: A Pilot Randomized Controlled Study. Journal of the International Neuropsychological Society. 2019;25(7):668-677. https://europepmc.org/articles/PMC7045510 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Trinh VQ, Bodrogi P, Khanh TQ. Determination and Measurement of Melanopic Equivalent Daylight (D65) Illuminance (mEDI) in the Context of Smart and Integrative Lighting. Sensors (Basel). 2023;23(11):5000. https://europepmc.org/articles/PMC10255211 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Stone JE, Steven D, Cheng W, et al. Who Needs Bright Light and When? Mapping the Interactions of Lighting Environments and Individual Differences in Circadian Light Sensitivity. Journal of Biological Rhythms. 2026;41(2):104-118. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2270041/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wei D, Wu X, Tan Y, Li Y, Zhu D, Song W. Circadian-dependent neural mechanisms of lighting optimization in underground transit environments: Evidence from fNIRS network analysis. Physiology & Behavior. 2026;311:115329. https://pubmed.ncbi.nlm.nih.gov/41933776/ ↩︎ ↩︎ ↩︎
Sunde E, Mrdalen J, Pedersen T, Toft E, Grønli J, Bjorvatn B, Harris A, Waage S, Steven D, Pallesen S. Blue-Enriched White Light Improves Performance but Not Subjective Alertness and Circadian Adaptation During Three Consecutive Simulated Night Shifts. Frontiers in Psychology. 2020;11:2172. https://europepmc.org/articles/PMC7462016 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zyto S, Jabben N, Schulte PFJ, Regeer EJ, Goossens PJJ, Kupka RW. A multi-center naturalistic study of a newly designed 12-sessions group psychoeducation program for patients with bipolar disorder and their caregivers. International Journal of Bipolar Disorders. 2020;8(1):26. https://europepmc.org/articles/PMC7459037 ↩︎ ↩︎ ↩︎ ↩︎
Hong SJ, Pratuangtham S, Martyn-Nemeth P. Blue Light Exposure During Sleep in Type 1 Diabetes: Impacts on Glycemic Control and Psychosocial Health. Journal of Sleep Research. 2026;35(3):e13580. https://clinicaltrials.gov/search?term=AREA[ReferencePMID]42246173 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎