¶ Fertility Preservation and Ovarian Reserve
| Indication | Elective and Medical Fertility Preservation, Ovarian Reserve Assessment [^1][^2][^3] |
| Access | Clinical Referral (Reproductive Endocrinology & Infertility Specialists) [^1][^2] |
| Diagnostic Criteria | Clinically assessed via biochemical and sonographic markers of ovarian reserve [^3][^4] |
| Safety Profile | Moderate (Surgical retrieval risks, Ovarian Hyperstimulation Syndrome) [^2][^4] |
| Key Markers | Anti-Müllerian Hormone (AMH), Antral Follicle Count (AFC) [^3][^4] |
| Est. Cost | Substantial; high out-of-pocket costs and annual storage fees represent major barriers [^2][^8][^9] |
Ovarian reserve assessment and fertility preservation technologies represent a major advancement in reproductive medicine, offering a highly validated methodology to quantify the remaining oocyte pool and safeguard future reproductive potential [1][2][3]. Evaluating ovarian reserve relies primarily on endocrine and sonographic markers, which guide the personalization of controlled ovarian stimulation (COS) protocols [2:1][4][5]. General ovarian reserve testing and elective (planned) fertility preservation are governed by reproductive medicine guidelines, such as those from the American Society for Reproductive Medicine (ASRM) [2:2][5:1] and the European Society of Human Reproduction and Embryology (ESHRE) [4:1]. In contrast, the American Society for Clinical Oncology (ASCO) establishes clinical guidelines strictly focused on patients undergoing cancer treatment (medical oncofertility) before receiving gonadotoxic therapies [6][7][8].
¶ At a Glance
¶ Key Points
- Ovarian Reserve: Represents the quantity of oocytes remaining, which declines progressively over a female's reproductive lifespan, resulting in lower live birth rates as maternal age advances [2:3][9].
- Cryopreservation Options: Vitrification of oocytes or embryos is the clinical standard of care, offering high post-thaw survival and clinical success rates compared to obsolete slow-freezing methods [1:1][5:2][10].
- Clinical Consensus: Prominent oncology clinical guidelines, such as those from the American Society for Clinical Oncology (ASCO) and the National Comprehensive Cancer Network (NCCN), emphasize early, patient-centered discussions about fertility risks and preservation options before patients undergo gonadotoxic cancer treatments [6:1][7:1][11].
¶ Safety "Traffic Light"
- Critical Contraindications: Patient selection and the feasibility of controlled ovarian stimulation or tissue cryopreservation are determined by individual clinical factors, including the type of cancer, treatment urgency, patient age, and overall medical condition [1:2][11:1].
- Timing & Safety: Standard fertility preservation procedures must not significantly delay the initiation of necessary gonadotoxic cancer treatments [6:2][1:3][7:2].
- Risk Mitigation: The selection of specific stimulation protocols and starting gonadotropin doses must be individualized to minimize clinical risks (such as Ovarian Hyperstimulation Syndrome) in patients undergoing controlled ovarian stimulation [4:2][5:3].
¶ Protocol Card / Quick Reference
- Controlled Ovarian Stimulation (COS):
- Ovarian Reserve Assessment: Biomarkers such as Anti-Müllerian Hormone (AMH) and Antral Follicle Count (AFC) are utilized clinically to estimate expected ovarian response and guide the selection of gonadotropin doses [2:4][4:3].
- Regimen: COS involves the administration of exogenous gonadotropins (such as follicle-stimulating hormone) to induce the development of multiple mature follicles [4:4][5:4].
- Oocyte Retrieval: Mature oocytes are harvested via ultrasound-guided transvaginal needle aspiration under conscious sedation [1:4][2:5].
- Cryopreservation: Mature oocytes are cryopreserved immediately via vitrification, or fertilized with partner or donor sperm to create embryos for cryopreservation [1:5][5:5][10:1].
¶ Bottom Line
Vitrified oocytes and cryopreserved embryos provide highly effective, long-term options to preserve reproductive potential [1:6][5:6][10:2]. However, because ovarian reserve markers exclusively measure oocyte quantity rather than oocyte quality (which is strictly age-dependent), clinicians must emphasize that a normal AMH/AFC is not a guarantee of future live birth, nor does a low AMH/AFC in a young patient indicate infertility [2:6][5:7].
¶ What is Ovarian Reserve & Ovarian Aging?
¶ Pathophysiological Overview of Reproductive Aging
In clinical practice, a female's ovarian reserve refers to the size of the remaining follicle pool [2:7][9:1]. Unlike males, who undergo continuous spermatogenesis throughout post-pubertal life, the total quantity of follicles in a female is finite, established during fetal development, and naturally declines with increasing reproductive age [2:8][9:2]. This progressive, age-dependent decline in follicle quantity is accompanied by a concurrent decline in oocyte quality, leading to lower live birth rates as maternal age advances [2:9][5:8].
Evaluating a patient's ovarian reserve relies on biochemical and biophysical markers, which serve as surrogate measures for the remaining follicle pool [2:10][4:5]. Clinicians utilize these markers primarily to predict oocyte yield following controlled ovarian stimulation, helping to tailor starting gonadotropin doses and select appropriate stimulation protocols [2:11][4:6].
- Anti-Müllerian Hormone (AMH): AMH is a serum biomarker secreted by small growing follicles, making it a highly validated marker of oocyte quantity [2:12][4:7].
- Antral Follicle Count (AFC): AFC is a sonographic marker representing the number of antral follicles visualized in both ovaries via transvaginal ultrasound [2:13][4:8]. It serves as a direct biophysical measure of the responsive follicle pool [2:14][4:9].
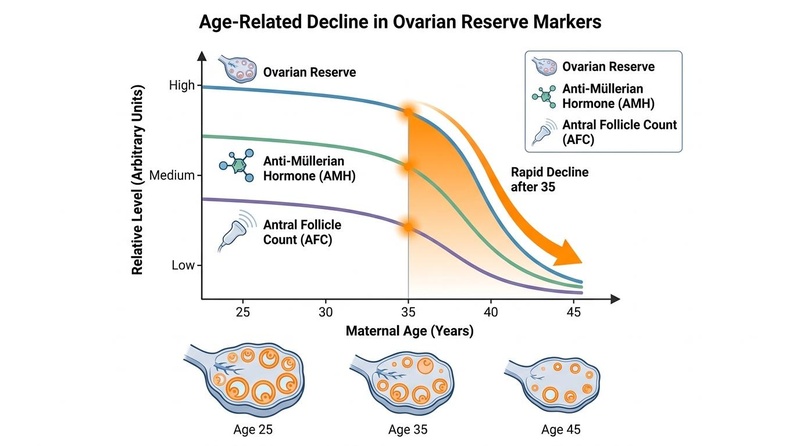
Figure 1: Progressive age-related decline of ovarian reserve, Anti-Müllerian Hormone (AMH), and Antral Follicle Count (AFC) with marked acceleration beginning at age 35 [2:15][9:3].
¶ Chronological Age vs. Biological Ovarian Reserve
A fundamental concept in reproductive endocrinology is the distinction between chronological age and biological ovarian reserve [2:16][5:9]:
- Chronological Age (Primary Determinant of Quality): Chronological age is the single most reliable predictor of oocyte quality, which refers to the chromosomal normalcy (euploidy) and developmental competence of the gamete [2:17][5:10]. Fecundity declines naturally with age primarily due to declines in oocyte quality, leading to lower live birth rates particularly after age 35, highlighting that chronological age remains the primary driver of reproductive success [2:18][5:11].
- Biological Ovarian Reserve (Primary Determinant of Quantity): Ovarian reserve reflects the quantitative size of the remaining follicle pool [2:19][9:4]. While highly correlated with age on a population level, there is wide individual variation in the rate of follicle depletion [2:20][9:5]. A young patient may exhibit a prematurely diminished ovarian reserve (DOR) due to genetic, autoimmune, environmental, or surgical factors, which can also progress to premature ovarian insufficiency [2:21][9:6]. Crucially, while a young patient with DOR has fewer follicles, the oocytes retrieved from those follicles typically maintain the high chromosomal normalcy characteristic of their young chronological age [2:22][5:12].
¶ Ovarian Reserve Testing & Limitations
Evaluating a patient's ovarian reserve involves a systematic assessment of biochemical and biophysical markers [2:23][4:10][3:1]. These tests serve as surrogate measures for the size of the resting follicle pool and are primarily utilized to estimate response to controlled ovarian stimulation [2:24][4:11].
¶ Clinical Markers
¶ Anti-Müllerian Hormone (AMH)
Anti-Müllerian Hormone (AMH) is a serum biomarker secreted by small growing follicles that serves as a clinical marker to estimate ovarian reserve [2:25][4:12]. AMH levels decline progressively with age, serving as an indicator of the shrinking follicle pool [2:26][9:7]. While AMH is a validated marker of oocyte quantity, it does not reflect oocyte health, quality, or the overall likelihood of achieving a pregnancy [2:27][5:13].
¶ Antral Follicle Count (AFC)
Antral Follicle Count (AFC) is a sonographic marker that measures the number of antral follicles visualized in both ovaries via transvaginal ultrasound [2:28][4:13]. It serves as a real-time biophysical measure of the responsive follicle pool, which helps guide the selection and customization of gonadotropin doses [2:29][4:14]. However, AFC is subject to inter-observer variability and is dependent on operator experience and ultrasound resolution.
¶ Follicle-Stimulating Hormone (FSH) & Estradiol
Basal FSH and estradiol levels are measured during the early follicular phase of the menstrual cycle [2:30][9:8]. As the ovarian follicle pool declines, basal FSH levels typically exhibit a compensatory rise due to decreased negative feedback [2:31][9:9]. Early follicular estradiol must be co-evaluated, as elevated estradiol can artificially suppress FSH levels, potentially masking a decline in ovarian reserve [2:32][9:10].
¶ CRITICAL WARNING: Predictor of Yield vs. Fertility
CRITICAL CLINICAL REALITY
Ovarian reserve tests (such as AMH and AFC) must NOT be marketed or utilized as diagnostic markers of natural fertility or spontaneous conception in fertile women [2:33]. Clinical guidelines and reviews emphasize that measures of ovarian reserve do not reflect a patient's probability of natural conception [2:34]. Ovarian reserve is defined as the number of oocytes remaining in the ovary (oocyte quantity/number), and markers of ovarian reserve are strictly validated as predictors of oocyte yield following controlled ovarian stimulation and oocyte retrieval, helping clinicians customize stimulation protocols [2:35][4:15].
¶ Fertility Preservation Modalities
Modern assisted reproductive technology (ART) provides three primary established modalities to safeguard future reproductive potential [1:7][5:14][10:3].
¶ Oocyte Cryopreservation
Oocyte cryopreservation is the standard of care for single individuals opting for planned (elective) or medical fertility preservation [1:8][5:15][12].
- Controlled Ovarian Stimulation (COS): Exogenous gonadotropins are administered to induce multifollicular development in the ovaries [4:16][5:16].
- Retrieval: Transvaginal ultrasound-guided needle aspiration is performed to harvest mature oocytes [1:9][2:36].
- Vitrification: Vitrification (ultra-rapid freezing) is the standard method for oocyte cryopreservation [1:10][5:17][10:4]. Metaphase II oocyte vitrification is recommended by major guidelines as the preferred option to achieve high post-thaw survival and successful outcomes [5:18][13][10:5].
¶ Embryo Cryopreservation
Embryo cryopreservation is an established, highly successful modality for individuals with a committed partner or those utilizing donor sperm [1:11][5:19][10:6].
- Process: Retrieved oocytes are fertilized immediately via conventional IVF or Intracytoplasmic Sperm Injection (ICSI) [1:12][4:17]. The resulting embryos are cultured to the blastocyst stage (day 5 or 6) and vitrified [1:13][10:7].
- Considerations: Embryo vitrification is associated with high post-thaw survival and clinical pregnancy rates [10:8]. Conversely, embryo freezing requires fertilizing the eggs with partner or donor sperm [1:14]. This introduces potential clinical and personal complexities, as the future utilization of the embryos is linked to that specific partner or donor agreement, which can lead to difficult ethical or legal challenges if relationship dynamics change, whereas oocyte cryopreservation preserves complete reproductive autonomy [1:15][12:1].
¶ Ovarian Tissue Cryopreservation (OTC)
Once classified as experimental, OTC is now an established standard clinical option, particularly for prepubertal females (for whom it is the only established method) or adult patients who cannot delay the initiation of gonadotoxic therapies for the 10 to 14 days required for standard ovarian stimulation [6:3][1:16][13:1][10:9].
- Procedure: Laparoscopic surgery is performed to excise the ovarian cortex (or an entire ovary), which contains a high density of primordial follicles [1:17][13:2]. The cortical tissue is processed into thin strips and vitrified [13:3][10:10].
- Replantation: Post-remission, the vitrified strips are autotransplanted back into the pelvis (orthotopic) or onto the abdominal wall (heterotopic) [13:4][10:11].
- Outcomes: OTC is highly effective at restoring ovarian endocrine function and has resulted in spontaneous and IVF-assisted live births [1:18][13:5][10:12].
¶ Gonadotoxic Treatment & Medical Pathways
Oncofertility represents a crucial intersection between clinical oncology and reproductive medicine to optimize patient-centric quality of life post-remission [6:4][1:19][10:13].
¶ Gonadotoxic Pathways
- Chemotherapeutic Exposure: Certain chemotherapy drug classes, particularly alkylating agents such as cyclophosphamide, pose a high threat to ovarian function [1:20]. These agents increase the risk of treatment-induced ovarian dysfunction, progressive follicular depletion, and permanent premature ovarian insufficiency (POI) [1:21]. The extent of the risk depends on factors such as the specific drug class, cumulative dose, and the patient's baseline ovarian reserve and age [1:22].
- Radiotherapy: Pelvic, abdominal, or total body irradiation is highly gonadotoxic [1:23]. The ovaries are extremely sensitive to radiation, and exposure can cause direct, dose-dependent damage to the follicular pool, leading to acute or gradual ovarian dysfunction and permanent POI [1:24].
- Surgical Interventions: Bilateral oophorectomy or extensive pelvic surgery for gynecologic malignancies, endometriosis, or deep pelvic pathologies directly reduces functional ovarian volume and can lead to surgical menopause [1:25].
¶ Role of GnRH Agonists (Ovarian Suppression)
During chemotherapy, GnRH agonists may be administered to suppress the hypothalamic-pituitary-ovarian axis, putting the ovaries into a temporary suppressed state [6:5][5:20][7:3].
- Consensus & Guidelines: Clinical trial data has led to a strong consensus among major guidelines, including ASCO and NCCN [6:6][7:4][11:2]:
- GnRH agonists should NOT be used in place of established, proven fertility preservation methods (such as oocyte, embryo, or ovarian tissue cryopreservation) [6:7][7:5][11:3].
- They may be offered as an adjunct therapy during chemotherapy for young patients with breast cancer or other malignancies to reduce the risk of chemotherapy-induced POI and to provide menstrual suppression to prevent severe bleeding [6:8][7:6][11:4].
¶ Success Rates & Age-Specific Predictors
The clinical success of fertility preservation is a function of age at the time of retrieval and the quantity of vitrified gametes [5:21].
¶ Age-Specific Live Birth Rates
The clinical success of utilizing cryopreserved oocytes is highly age-dependent, with significantly superior outcomes observed when oocytes are retrieved and stored at a younger chronological age [5:22].
While specific live birth percentages vary across clinical settings, medical guidelines and registry data confirm that the rate of successful live birth per cycle is higher for women who store oocytes at a younger age (such as under 35 years) compared to those who store them at older ages, reflecting the age-dependent decline in oocyte chromosomal normalcy [5:23]. Clinical registry data and professional society guidelines indicate that live birth rates are significantly higher for oocytes cryopreserved at a younger age (e.g., age 35 or younger) compared to older cohorts, illustrating the profound impact of chronological age on overall oocyte quality and reproductive success [5:24].
¶ Oocyte Quantity and Cumulative Probability
Clinicians must counsel patients that there are no guarantees of a future live birth, and that the probability of success is a cumulative function of the number of vitrified mature oocytes [5:25]. Generally, storing a larger number of mature oocytes increases the cumulative probability of at least one live birth, but older patients typically require a larger number of retrieved oocytes to achieve comparable success rates due to advancing chronological age being the primary determinant of reproductive success [5:26].
¶ Socioeconomic, Storage, Legal, & Access Issues
The implementation of fertility preservation involves significant financial, legal, and sociological complexities [1:26][14][15].
¶ Cost Burdens & Storage Fees
Fertility preservation is associated with substantial out-of-pocket costs and ongoing storage fees, which represent major financial barriers to care [1:27][14:1]. The cost of medications, clinical monitoring, surgical retrieval, and long-term liquid nitrogen cryostorage can be prohibitive for many patients, particularly when not covered by insurance [1:28][14:2]. Socioeconomic barriers heavily limit access; patients living in non-urban or lower socioeconomic status areas are significantly less likely to undergo fertility preservation [14:3].
¶ Counseling Barriers & Guidelines Compliance
A major issue is that despite clear guidelines from ASCO and ASRM recommending early consultation, actual counseling rates remain low [1:29][15:1]. A mixed-methods study evaluating the integration of ASCO guidelines in practice found that oncologist awareness of specific fertility discussion guidelines was low, and more than half of adolescents and young adults reported that only two components of ASCO guidelines were included in discussions [15:2]. Barriers such as communication issues, lack of time, and cost represent major factors [15:3].
¶ Legal & Ethical Dilemmas
The long-term storage of genetic material introduces complex legal and ethical questions [1:30]:
- Disposition of Unused Tissue: Clear, legally binding consent forms must be executed prior to cryopreservation to outline the disposition of unused oocytes or embryos in the event of death, divorce, separation, or abandonment [1:31].
- Embryo Disputes: Embryo cryopreservation carries significant legal risks; if a couple separates, one partner may seek to utilize the embryos to achieve pregnancy while the other partner objects, leading to protracted litigation [1:32]. Oocyte cryopreservation avoids these interpersonal legal risks, preserving complete reproductive autonomy [1:33][12:2].
¶ Evidence Limits of Ovarian Rejuvenation & Supplement Claims
In response to the natural decline of ovarian reserve, several experimental interventions have emerged, marketed under the umbrella of "ovarian rejuvenation." Clinicians must counsel patients that these therapies are considered experimental, lack high-quality clinical validation, and are not recommended or supported by major clinical consensus guidelines (such as ASCO or NCCN) [6:9][5:27][7:7][11:5].
Established guidelines strictly recognize oocyte, embryo, and ovarian tissue cryopreservation as standard and clinically validated options for preserving female reproductive potential [6:10][5:28][10:14]. There are currently no large-scale, high-quality randomized controlled trials (RCTs) demonstrating that alternative therapies—such as intraovarian platelet-rich plasma (PRP) injections, stem cell therapies, or oral supplements—improve clinical pregnancy rates or live birth rates in patients with diminished ovarian reserve or premature ovarian insufficiency [6:11][5:29][10:15]. Clinicians should not present these options as clinically validated or established, and should focus patient education on standard, proven cryopreservation techniques [6:12][5:30][10:16].
¶ Evidence Summary Table (Human Outcomes)
The major clinical interventions utilized to assess and preserve reproductive potential are evaluated below based on current clinical evidence.
| Outcome / Goal | Effect* | Consistency | Evidence Quality | Trials | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Oocyte Vitrification (LBR for age ) | High | High | Cohorts / Guidelines | Yields high cumulative live birth rates; highly dependent on storing a sufficient cohort of mature oocytes [5:31]. | |
| Oocyte Vitrification (LBR for age ) | High | High | Cohorts / Guidelines | Lower live birth rate per thaw cycle due to advanced chronological age and baseline rate of oocyte aneuploidy [5:32]. | |
| Embryo Vitrification | High | High | Registries / Guidelines | Highly established method of fertility preservation; associated with high post-thaw survival and success [1:34][10:17]. | |
| Ovarian Tissue Cryopreservation (OTC) | High | Moderate | Cohorts / Guidelines | Restores ovarian endocrine function post-transplant; standard for prepubertal and urgent medical cases [1:35][13:6][10:18]. | |
| GnRH Agonist Ovarian Suppression | Moderate | Moderate | RCTs / Guidelines | Recommended only as an adjunct during chemotherapy for breast cancer to reduce POI risk, not as a replacement for cryopreservation [6:13][7:8][11:6]. | |
| Fertility Preservation Counseling | High | High | Guidelines | Universally recommended by major guidelines to discuss fertility risks and preservation options before initiating treatment [6:14][7:9][11:7]. | |
| Sperm Cryopreservation | High | High | Registries / Guidelines | Highly established, standard method to preserve reproductive potential in post-pubertal males [6:15][7:10][11:8]. |
¶ FAQ
¶ Does a low Anti-Müllerian Hormone (AMH) level mean that a patient is currently infertile?
No. AMH is utilized clinically as an indirect measure of ovarian reserve to estimate expected oocyte yield during controlled ovarian stimulation and to customize starting gonadotropin doses [2:37][4:18]. However, because AMH exclusively measures follicle quantity and does not reflect oocyte quality (which is strictly age-dependent), it is a poor predictor of natural reproductive potential and should not be used as a standalone fertility test to predict the likelihood of spontaneous, unassisted conception [2:38]. In young patients, a low AMH does not indicate subfertility, as oocyte quality remains high and is primarily driven by their young chronological age [2:39].
¶ Is embryo freezing superior to oocyte freezing for fertility preservation?
Both embryo and oocyte cryopreservation are standard, highly effective clinical options for preserving reproductive potential [5:33][10:19]. While embryo freezing has historically been associated with high post-thaw success, it requires fertilizing the oocytes with partner or donor sperm, which can introduce complex interpersonal, ethical, and legal challenges regarding future disposition in the event of divorce, separation, or death [1:36]. Oocyte freezing avoids these interpersonal legal risks, preserving complete reproductive autonomy for the individual [1:37][12:3].
¶ How many frozen oocytes are required to provide a reasonable chance of a future live birth?
The cumulative probability of achieving a future live birth depends heavily on both the total number of vitrified mature oocytes and the patient's age at the time of retrieval [5:34]. Because oocyte quality is strictly age-dependent, younger patients have significantly higher live birth rates per thawed oocyte [5:35]. Registry data confirms that live birth rates are significantly superior for individuals who store oocytes at age 35 or younger compared to those who store them at older ages [5:36]. Older patients typically require a significantly larger number of retrieved oocytes to achieve comparable success rates [5:37].
¶ Can cancer patients safely undergo ovarian stimulation without delaying their oncological treatments?
In many clinical scenarios, standard fertility preservation can be safely performed prior to initiating gonadotoxic therapies [1:38]. However, because the feasibility, safety, and timing of controlled ovarian stimulation depend heavily on the type of cancer, treatment urgency, patient age, and overall medical condition, early referral and rapid, multidisciplinary coordination between oncology and reproductive teams are essential [6:16][1:39]. For patients who cannot undergo stimulation due to urgent oncological timelines, alternative options such as ovarian tissue cryopreservation may be utilized [1:40][13:7][10:20].
¶ What is Ovarian Tissue Cryopreservation (OTC), and who is it intended for?
OTC is an established standard clinical option involving the surgical removal and vitrification of outer ovarian cortex tissue, which contains a dense population of primordial follicles [13:8][10:21]. It is the only option for prepubertal girls facing gonadotoxic treatments (as they cannot undergo ovarian stimulation) and for adult patients who cannot delay their chemotherapy by 10 to 14 days to undergo a standard oocyte retrieval cycle [1:41][13:9][10:22]. Post-remission, the tissue is autotransplanted back into the patient, where it restores ovarian endocrine function and has led to spontaneous and IVF-assisted pregnancies [13:10][10:23].
¶ References
Kalluru S, Vu M, Brady PC. Fertility preservation for cancer: referral guidelines, treatment options, and specific considerations. Fertility and Sterility. 2025. https://pubmed.ncbi.nlm.nih.gov/40854469/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Practice Committee of the American Society for Reproductive Medicine. Testing and interpreting measures of ovarian reserve: a committee opinion. Fertility and Sterility. 2020;114(6):1151-1157. https://pubmed.ncbi.nlm.nih.gov/33280722/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Practice Committee of the American Society for Reproductive Medicine. Fertility evaluation of infertile women: a committee opinion. Fertility and Sterility. 2021;116(5):1255-1265. https://pubmed.ncbi.nlm.nih.gov/34607703/ ↩︎ ↩︎
ESHRE Guideline Group on Ovarian Stimulation, Bosch E, Broekmans F, et al. ESHRE guideline: ovarian stimulation for IVF/ICSI. Human Reproduction Open. 2020;2020(2):hoaa009. https://pubmed.ncbi.nlm.nih.gov/32395637/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Practice Committee of the American Society for Reproductive Medicine. Evidence-based outcomes after oocyte cryopreservation for donor oocyte in vitro fertilization and planned oocyte cryopreservation: a guideline. Fertility and Sterility. 2021;116(1):26-47. https://pubmed.ncbi.nlm.nih.gov/34148587/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Su HI, Lacchetti C, Letourneau J, et al. Fertility Preservation in People With Cancer: ASCO Guideline Update. Journal of Clinical Oncology. 2025;43. https://pubmed.ncbi.nlm.nih.gov/40106739/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Oktay K, Harvey BE, Partridge AH, et al. Fertility Preservation in Patients With Cancer: ASCO Clinical Practice Guideline Update. Journal of Clinical Oncology. 2018;36(19):1994-2001. https://pubmed.ncbi.nlm.nih.gov/29620997/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Oktay K, Harvey BE, Loren AW, et al. Fertility Preservation in Patients With Cancer: ASCO Clinical Practice Guideline Update Summary. Journal of Oncology Practice. 2018;14(6):381-385. https://pubmed.ncbi.nlm.nih.gov/29768110/ ↩︎
Practice Committee of the American Society for Reproductive Medicine. Testing and interpreting measures of ovarian reserve: a committee opinion. Fertility and Sterility. 2012;98(6):1407-1415. https://pubmed.ncbi.nlm.nih.gov/23095141/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Martinez F, International Society for Fertility Preservation–ESHRE–ASRM Expert Working Group. Update on fertility preservation from the Barcelona International Society for Fertility Preservation-ESHRE-ASRM 2015 expert meeting: indications, results and future perspectives. Human Reproduction / Fertility and Sterility. 2017;32(9):1802-1811 / 108(3):407-415. https://pubmed.ncbi.nlm.nih.gov/29117320/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bhinder JK, Peera M, Al-Khaifi M, et al. Comparison of Fertility-Related Recommendations Across National Comprehensive Cancer Network, ASCO, Clinical Oncology Society of Australia, and European Society for Medical Oncology Guidelines for People With Cancer. JCO Oncology Practice. 2026. https://pubmed.ncbi.nlm.nih.gov/41534015/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Schon SB, Shapiro MV, Gracia C, et al. Medical and elective fertility preservation: impact of removal of the experimental label from oocyte cryopreservation. Journal of Assisted Reproduction and Genetics. 2017;34(9):1207-1215. https://pubmed.ncbi.nlm.nih.gov/28656539/ ↩︎ ↩︎ ↩︎ ↩︎
Knight S, Lorenzo A, Maloney AM. An approach to fertility preservation in prepubertal and postpubertal females: a critical review of current literature. Pediatric Blood & Cancer. 2015;62(6):935-939. https://pubmed.ncbi.nlm.nih.gov/25739552/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Meernik C, Engel SM, Wardell A. Disparities in fertility preservation use among adolescent and young adult women with cancer. Journal of Cancer Survivorship. 2023;17(5):1339-1348. https://pubmed.ncbi.nlm.nih.gov/35169982/ ↩︎ ↩︎ ↩︎ ↩︎
Stal J, Yi SY, Roche CI, et al. Are guidelines guiding? A mixed methods study examining the integration of ASCO fertility discussion guidelines in practice among oncologists and adolescents and young adults. Journal of Cancer Survivorship. 2025. https://pubmed.ncbi.nlm.nih.gov/40536662/ ↩︎ ↩︎ ↩︎ ↩︎