¶ Gait Speed and Chair-Stand Testing
| Clinical Domain | Neuromuscular & Functional Capacity |
| Primary Tests | 4MGS, 5XSTS, 30-Sec Chair Stand |
| Key Equipment | Stopwatch, Standard Armless Chair, Tape |
| Primary Marker | Usual Gait Speed (m/s), Chair Rise Time (s) |
| Clinical Cutoff | Gait Speed <1.0 m/s; SPPB Score <9 |
| Safety Profile | High (requires spotter for fall risk) |
Gait speed and repeated chair-stand tests are low-cost, objective, and highly validated clinical tools used to assess neuromuscular function, lower-limb muscular power, and postural control. Slower walking speed serves as an objective clinical marker of functional decline: while it should be used cautiously in isolation as part of a comprehensive assessment [1], it predicts a significantly higher risk of prospective falls [2], acts as a powerful predictor of hospitalization and 1-year mortality [3], and serves as a reliable indicator of accelerated biological aging and cognitive deterioration [4]. Together, these assessments form the cornerstone of standardized clinical batteries, such as the Short Physical Performance Battery (SPPB), enabling high-resolution tracking of neuromuscular aging and physical frailty [3:1].
¶ At a Glance
¶ Key Takeaways
- Neuromuscular Vital Signs: Comfortable usual gait speed is a direct mirror of systemic vitality, reflecting integrated cardiovascular, neurological, and musculoskeletal health [4:1].
- Sarcopenia Diagnostics: Handgrip strength and the 5-time chair-stand test are key muscle strength measures in the sarcopenia diagnosis algorithm [5]. Usual comfortable gait speed below 1.0 m/s is a standard definition of slow gait [6], while low five-repetition chair stand performance predicts a 2-fold higher fall risk [2:1].
- High Sensitivity to Change: These tests are responsive to therapeutic interventions, with targeted exercise snacking programs [7] demonstrating high feasibility, supervised elastic band resistance training protocols [8] evaluated for physical performance in institutionalized elderly, and pharmacological MAS receptor activation [9] yielding clinically meaningful gains.
- Safety Requirements: While highly safe, testing requires standardized protocols, a flat blemish-free pathway, a sturdy armless chair of standardized height placed securely against a wall to prevent slipping, and a trained spotter to mitigate fall risks according to standard clinical safety protocols.
¶ Safety "Traffic Light" & Contraindications
¶ Clinical Protocol Cards
¶ 1. 4-Meter Usual Gait Speed (Dynamic Start)
- Pathway Setup: Mark a flat 4-meter timed zone, with an additional 1-meter zone before (acceleration) and after (deceleration) the zone.
- Instruction: "Walk at your normal, comfortable pace, as if you are walking to the store."
- Timing: Start stopwatch when the lead foot crosses the 0m line; stop when the lead foot crosses the 4m line.
¶ 2. 5-Repetition Chair Stand Test (5XSTS)
- Chair Setup: Sturdy, armless chair of standardized height, placed securely against a wall to prevent slipping.
- Positioning: Sit upright, feet flat on the floor, arms folded tightly across the chest.
- Instruction: "Stand up straight and sit back down five times as quickly as you can, keeping your arms crossed."
- Timing: Start timing on "Go"; stop timing at the peak of the fifth full extension.
¶ Why Measure Gait Speed and Chair Rise?
The clinical utility of physical functional assessments lies in their ability to capture integrated biological systems. Unlike isolated blood biomarkers or static muscle mass scans, which measure capacity, functional tests evaluate dynamic biological reserves.
¶ Musculoskeletal Power vs. Strength
Skeletal muscle aging is characterized by a decline in muscular strength and performance, often associated with malnutrition and physical deconditioning [10]. Slower chair-stand pace and lower muscle strength are highly correlated with walking speed and self-reported mobility difficulty in middle-aged and older adults [6:1]. Upper limb strength and lower limb strength (assessed via handgrip strength and the chair-stand test) show positive associations with physical performance metrics (such as the 6-minute walk test, timed up and go, and gait speed), with lower limb muscle quality showing significant associations with walking performance (such as the 6-minute walk test) in females [11]. Power generation depends heavily on muscle quality and lower-extremity power, which declines with aging [12][11:1], and while ultrasonographic measurements of muscle thickness and echo intensity correlate moderately to strongly with muscle strength, they exhibit weak or non-significant correlations with gait speed, the Timed Up and Go (TUG) test, and repeated chair-stand performance [13]. Consequently, repeated chair stands serve as an early, sensitive warning system for neuromuscular deconditioning [2:2][11:2].
¶ The Neurology of Bipedal Locomotion
Comfortable walking is not merely a mechanical action; it is a complex cognitive and neurological task. Normal bipedal gait requires continuous, integrated signaling from the motor cortex, cerebellum, vestibular system, and peripheral sensory pathways. Because gait speed is limited by the weakest link in this neural loop, bipedal locomotion correlates closely with brain health. Usual gait speed in midlife (age 45) is strongly associated with brain health, including smaller brain volume, more cortical thinning, smaller cortical surface area, more white matter hyperintensities, and lifelong cognitive trajectories [4:2]. Slower usual gait speed reflects accelerated biological aging across multiple organ systems [4:3], and changes in walking speed are dynamically linked to changes in fluid cognition [14].
¶ Standardized Gait Speed Protocols
To ensure that changes in gait speed reflect true biological changes rather than testing variability, clinicians must implement highly standardized protocols. Minor alterations in timing methods or course setup can skew results, masking clinical decline or simulating false improvement [15].
Standard 4-Meter Gait Speed (4MGS) Dynamic Start Setup:
|-- 1 to 2m Acceleration Zone --|------- 4-Meter Timed Zone -------|-- 1 to 2m Deceleration Zone --|
[Start Line] [Timing Start] [Timing End] [Finish Line]
o x x o
|-------------------- Participant Walks Continuously -------------------------------------------->
^-- Timer Starts ^-- Timer Stops
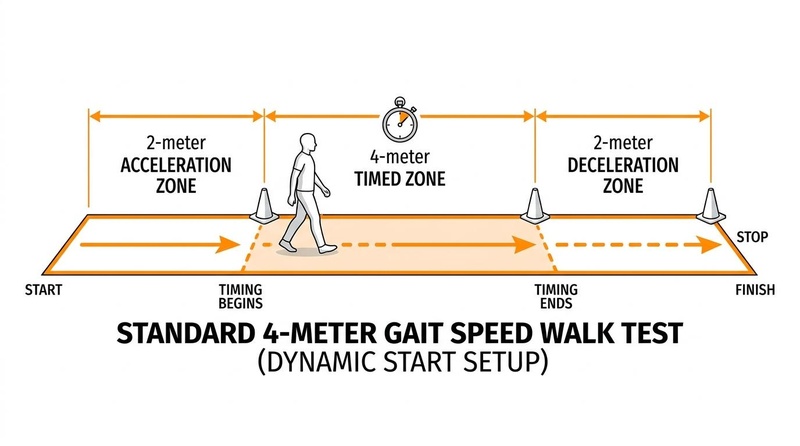
Figure 1: Standard 4-Meter Gait Speed (4MGS) Walk Test Setup showcasing the dynamic start acceleration and deceleration zones.
¶ Usual vs. Fast Pace
- Usual (Habitual) Gait Speed: The participant is instructed to walk at their normal, comfortable pace, "as if you are walking down the street to the store." This measures habitual neuromuscular efficiency and predicts long-term health outcomes, fall risk, and cognitive trajectories [2:3][4:4].
- Fast Gait Speed: The participant is instructed to walk "as fast and safely as you can, without running." Fast gait speed assesses maximum physiological reserve. In midlife cohorts, maximum gait speed has been established at 1.99 ± 0.29 m/s [4:5]. While standard mobility assessments may have limited sensitivity to detect early decline in high-functioning populations [12:1], measuring maximum gait speed and physical fitness helps evaluate overall functional capacity [4:6][16].
¶ Course Lengths
- 4-Meter Walk Test: The clinical standard, utilized in the Short Physical Performance Battery (SPPB) and common geriatric clinical guidelines [3:2]. It is highly space-efficient and ideal for standard clinical exam rooms.
- Other Course Lengths: Longer courses (such as the 10-meter walk test) are utilized in rehabilitation clinics and neurological assessments. Longer courses minimize the relative error introduced by manual stopwatch timing delays but require larger, unobstructed spaces.
¶ Acceleration vs. Deceleration Zones (Static vs. Dynamic Starts)
The timing state significantly influences the recorded gait speed:
- Static Start: The participant stands at the starting line and begins walking on the command "Go." The timer starts immediately. This protocol captures the initial acceleration phase, resulting in a significantly underestimated calculated gait speed [15:1].
- Dynamic Start: The participant stands 1 to 2 meters behind the timed zone. They begin walking and are already at steady-state comfortable velocity when they cross the timing start line [15:2]. Timing begins as their lead foot crosses the start line and stops as their lead foot crosses the 4-meter end line. A deceleration zone is provided past the end line to allow the participant to slow down naturally.
Protocol Standardization Rule: Standardized protocols are essential to prevent measurement errors. Dynamic start protocols are preferred for measuring pure, comfortable velocity [15:3]. Research using light detection and ranging (LiDAR) demonstrated that static start protocols significantly underestimate usual gait speed compared to dynamic starts (0.7 m/s vs 1.05 m/s, p < 0.001) [15:4]. This underestimation occurs because static starts include the acceleration phase, which averages 0.92 ± 0.51 meters [15:5]. A dynamic start protocol (removing the first 0.5 to 1.0 meter) provides a more accurate measure of comfortable velocity, with an acceleration phase of 0.5 to 1 meter appearing sufficient to align with other physical performance results [15:6].
¶ Standardized Chair-Stand Protocols
Repeated chair-rise tests evaluate a combination of lower-limb strength, postural control, balance, and sensory-motor coordination.
¶ Five Times Sit-to-Stand (5XSTS) Protocol
The 5XSTS measures the time taken to complete five consecutive chair rises as quickly as possible.
- Equipment Setup: Use a standard armless chair with a flat, sturdy seat. The seat height must be standardized (typically utilizing a standard medical or office chair height) to ensure measurement consistency across repeated trials.
- Participant Positioning: The participant sits in the middle of the seat with their feet flat on the floor, shoulder-width apart. Arms must be folded snugly across the chest and held there throughout the test.
- Standardized Instructions: "I want you to stand up straight and sit back down as quickly as you can five times in a row without stopping. Keep your arms folded across your chest. I will start timing when I say 'Go' and will stop when you stand up fully for the fifth time."
- Execution and Timing: The tester commands "Go" and starts the stopwatch. The participant performs five full extensions. The tester stops the watch at the peak of the fifth extension, before the participant sits back down. The repetition is void if the participant uses their arms to push off or fails to achieve full hip and knee extension.
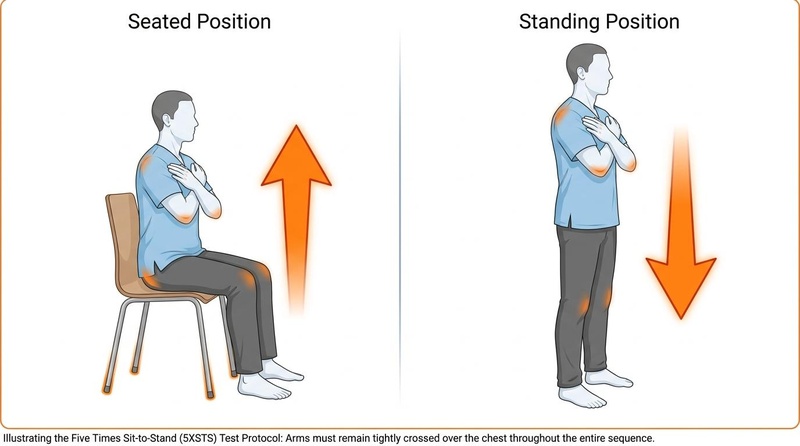
Figure 2: Five Times Sit-to-Stand (5XSTS) Test Protocol showcasing seat setup and proper posture with arms folded tightly across the chest throughout both seated and standing phases.
Visual Progression of the 5XSTS Test Repetition:
[ Sitting ] [ Phase 1: Lean ] [ Phase 2: Momentum ] [ Phase 3: Erect ]
O O O O
/|\ /|\ /|\ /|\
/ | \ / | \ / | \ / | \
_|_ _|_ _|_ _|_
[ ] [ ] / \ | |
| | | | | | | |
========================================================================================
Back on chair; Trunk flexes forward; Buttocks leave seat; Full hip & knee
arms crossed. hips flex. concentric quadriceps rise. extension achieved.
¶ 30-Second Chair Stand Test
Instead of measuring time to complete a fixed number of rises, this protocol counts the maximum number of completed rises within a strict 30-second window. It is highly useful in cohorts with functional limitations where a timed test might be difficult to complete.
- Repetitions are counted if they are fully completed within 30 seconds.
- The 30-second chair-stand test (CST) counts the repetitions completed within 30 seconds, reflecting dynamic muscle strength and lower-limb quality [11:3]. Lucena et al. demonstrated that in females, both upper-limb strength (handgrip strength) and lower-limb strength (30-second CST) show positive, significant associations with physical performance outcomes including the 6-minute walk test, timed up and go, maximum gait speed, and balance [11:4]. In males, lower-limb strength was significantly associated with the timed up and go test, highlighting distinct sex-specific profiles in physical function screening [11:5].
¶ Clinical Safety and Administration Guidelines
Physical performance testing is active and dynamic. Thus, strict adherence to safety protocols is mandatory to prevent falls, acute joint strain, or adverse cardiovascular events.
¶ Pre-Test Screening and Contraindications
Before administering gait speed or chair-stand tests, clinicians must conduct a brief medical screening.
- Absolute Contraindications:
- Acute chest pain (suspected angina) or acute myocardial infarction within the past 30 days.
- Uncompensated congestive heart failure.
- Acute deep vein thrombosis or pulmonary embolism.
- Unstable, severe orthopedic conditions (e.g., acute pelvic or femoral fracture, severe unmanageable joint pain).
- Severe cognitive impairment rendering the participant unable to safely understand or follow basic physical instructions.
- Relative Contraindications:
- Severe resting hypertension (Systolic BP >180 mmHg or Diastolic BP >110 mmHg).
- Resting tachycardia (>120 bpm) or severe brain bradycardia (<40 bpm).
- Moderate-to-severe symptomatic spinal stenosis or peripheral artery disease (ischemic claudication) that restricts bipedal weight-bearing.
¶ Safety Equipment and Fall Mitigation
- Spotter Positioning: According to standard clinical safety protocols, the examiner must act as a spotter. For gait speed, the spotter should walk slightly behind and to the side of the participant, maintaining an active, balanced stance. For chair stands, the spotter stands close to the side of the participant, ready to stabilize them at the shoulder or torso if they sway or lose balance.
- Pathway Safety: The testing pathway must be completely flat, level, and free of rugs, electrical cords, or surface blemishes.
- Assistive Devices: If the participant cannot walk safely without a cane or walker, they may use it during the gait speed test. However, this must be documented explicitly. It alters the biomechanics, and their score cannot be directly compared to standard normative curves for unassisted cohorts. Assistive devices are not permitted during standard 5XSTS testing; if a participant cannot stand without using their arms, the test is scored as unable to complete (0 points).
¶ Learning Effects and Repeatability
Physical performance outcomes can be influenced by learning effects and participant familiarization with the testing procedures. During repeated testing, individuals often show artificial performance improvements on subsequent trials simply due to decreased anxiety, better comprehension of instructions, and motor learning (familiarization with the biomechanical task). This repeatability bias is particularly pronounced in repeated chair-stand tests and maximum gait speed trials. To manage learning effects and ensure high test-retest reliability, clinicians must standardize testing administration:
- Practice Trials: Administer one or two submaximal practice trials before recording official timed results. For the gait speed test, a single warm-up walk allows the participant to establish a steady-state comfortable pace. For repeated chair stands, a single practice rise ensures proper arm crossing and foot placement.
- Trial Averaging: Many clinical protocols record two trials and utilize the average or the fastest time to represent true functional capacity, minimizing the impact of trial-to-trial cognitive and motor adjustments.
- Consistent Cueing: Standardize the verbal prompts and countdowns (e.g., "Ready, set, go") across all trials and longitudinal visits to maintain uniform motivational and attentional states.
¶ Reality Check & Sarcopenia Diagnostics
While animal models evaluate muscle biology, clinical decisions must rely on human functional results. In humans, muscle mass alone is limited for predicting real-world physical performance [11:6]. Instead, muscle strength and muscle quality (derived from functional tests like the 30-s chair-stand) provide more clinically useful indicators of impairment [11:7].
In the diagnostic landscape, handgrip strength (HGS) and the 5-time chair-stand test are the dual pillars of sarcopenia algorithms [5:1]. However, screening tools show differing detection rates: handgrip strength typically identifies a higher prevalence of possible, confirmed, and severe sarcopenia than the 5-time chair-stand test [5:2]. This variance demonstrates the need for comprehensive diagnostic protocols that include both upper-limb and lower-limb functional metrics [3:3][5:3]. Additionally, rapid screening tools such as the 3-item SARC-F (focusing on strength, stair climbing, and walking assistance) can be utilized for fast clinical triage [17].
These clinical metrics are highly sensitive to therapeutic interventions and technological monitoring. Technological systems like the FACET ecosystem (Frailty Care and Well Function) can track functional tests such as gait speed and chair stands at home to detect early functional decline [18]. Standard clinical trials and pilot studies show that targeted exercises—such as home-based "exercise snacking" circuits [7:1] (evaluated for feasibility and functional improvements), creative dance investigated to support fitness and functional balance [19], active video games that can improve gait speed and mobility [20], supervised elastic band resistance training protocols evaluated for physical performance [8:1], and Qigong [21]—demonstrate beneficial effects on physical performance. Additionally, pharmacological agents like the MAS receptor activator BIO101 have demonstrated clinically relevant increases in walking speed, with a 0.09 m/s improvement in the per-protocol population [9:1] close to the sarcopenia MCID of 0.1 m/s [9:2]. Dietary factors also play a critical role; a greater proportion of daily ultra-processed food (UPF) consumption is associated with poorer physical function, including slower gait speed and worse joint-related outcomes like thinner cartilage in knee osteoarthritis [22].
¶ Evidence Summary Table (Human Outcomes)
The clinical outcomes, prognostic implications, and interventional responsiveness of gait speed and chair-stand performance are supported by high-quality human trials and systematic reviews.
| Intervention / Performance State | Clinical & Sarcopenia Outcome | Effect Size / Predictive Change | Evidence Quality (GRADE) | Supporting Studies (PMIDs) | Clinical Guidelines & Notes |
|---|---|---|---|---|---|
| Usual Gait Speed & Falls | Slower usual gait speed predicts near-term falls in older adults [1:1][2:4]. | Moderate | PMID: 40394423, PMID: 35879666 | No single gait, balance, or functional mobility assessment in isolation can predict fall risk with high certainty, but gait speed is useful as part of a comprehensive evaluation [1:2]. | |
| 5-Repetition Chair Stand (5CS) & Falls | Low performance on 5CS is a powerful predictor of falls within one year [2:6]. | High | PMID: 40394423 | Reflects lower-limb strength and balance; highly useful for fall risk screening in outpatient clinics [2:8]. | |
| SPPB Score & Outpatient Prognosis | Low performance on SPPB predicts adverse outcomes in acutely ill outpatients [3:4]. | High | PMID: 31886817 | Combining gait speed, chair-rise, and balance improved predictions over gait speed alone [3:6]. | |
| Midlife Gait Speed & Aging | Slower gait speed at age 45 is a marker of accelerated aging and poor brain health [4:7]. | High | PMID: 31603488 | Strongly associated with smaller brain volume, more cortical thinning, smaller cortical surface area, more white matter hyperintensities, and lifelong cognitive trajectories [4:9]. | |
| Surgical Prehabilitation (AktivA) | 6–12 weeks of preoperative exercise improves pre-surgery performance [23]. | High | PMID: 40050814 | Associated with a significant pre-surgery improvement in fast-paced walking speed, though long-term post-surgery outcomes did not differ between groups [23:2]. | |
| MAS Receptor Activator (BIO101) | 6–9 months of BIO101 in sarcopenic seniors improves walking speed [9:3]. | Moderate | PMID: 40026058 | Treatment effect approaches the minimal clinically important difference (MCID) of 0.1 m/s in sarcopenia [9:5]. | |
| Home-Based "Exercise Snacking" | 28 days of remotely-supervised, brief home resistance circuits [7:2]. | Moderate | PMID: 41658611 | Remotely delivered and acceptable strategy to support physical function and activity in community-dwelling older adults [7:4]. | |
| Malnutrition Status | Malnourished older adults show significantly worse physical function [10:1]. | Moderate | PMID: 35415390 | Better nutritional status is associated with better grip strength, faster gait speed, faster TUG, and higher SPPB [10:3]. | |
| Ultra-Processed Foods (UPF) | Greater proportion of daily NOVA-4 UPF is linked to poorer physical function [22:1]. | Moderate | PMID: 40480603 | Greater UPF proportion is linked to slower gait speed, along with worse pain and thinner cartilage in women [22:3]. | |
| Zumba & Daily Caffeine | Zumba training combined with daily caffeine improves performances [24]. | Moderate | PMID: 39463442 | Daily caffeine (100 mg/day) serves as an effective booster of physical training benefits in middle-aged women [24:2]. | |
| MCID Thresholds (Perera et al.) | Establishes small and substantial meaningful changes in physical function [25]. | High | PMID: 16696738 | Standard reference for evaluating clinical improvements in older adults [25:2]. |
¶ Midlife Baseline Benchmarks & Sarcopenia Screening
To accurately interpret performance, a participant's scores should be compared to age-matched baseline benchmarks and clinical algorithms.
¶ Midlife Baseline Benchmarks
In healthy midlife adults at age 45 years, typical gait speeds under different walking conditions represent physiological baselines before significant neuromuscular decline. The Dunedin multidisciplinary study provides robust population-representative benchmarks [4:10]:
- Usual Comfortable Gait Speed: 1.30 ± 0.17 m/s [4:11]
- Cognitive Dual-Task Gait Speed: 1.16 ± 0.23 m/s [4:12]
- Maximum Gait Speed: 1.99 ± 0.29 m/s [4:13]
¶ Sarcopenia Diagnostic Prevalence & Agreement
Among community-dwelling older adults (mean age 70.35 ± 7.24 years), possible, confirmed, and severe sarcopenia are detected differently by upper-limb vs lower-limb metrics. A cross-sectional evaluation of 1027 older adults demonstrated the following diagnostic prevalence and consistency [5:4]:
- Possible Sarcopenia (by Handgrip Strength): 50.8% [5:5]
- Possible Sarcopenia (by 5-Time Chair Stand): 27.6% [5:6]
- Confirmed Sarcopenia (HGS + gait speed + BIA): 20.3% [5:7]
- Confirmed Sarcopenia (5XSTS + gait speed + BIA): 10.8% [5:8]
- Severe Sarcopenia (with slow gait speed): 14.5% (HGS-based) vs. 10.9% (5XSTS-based) [5:9]
The agreement (Kappa) between handgrip strength and the 5-time chair-stand test in assessing sarcopenia varies across different classifications [5:10]. While there is a general lack of evidence and consensus regarding which muscle strength measure has a higher detection rate in community practice, Li et al. found that handgrip strength identified a significantly higher prevalence of possible, confirmed, and severe sarcopenia compared to the 5-time chair-stand test, suggesting that the choice of metric is a critical factor for community-based screening programs [5:11].
¶ Minimally Clinically Important Differences (MCIDs)
The Minimally Clinically Important Difference (MCID) is the smallest change in a clinical parameter that reflects a meaningful improvement or deterioration for the patient. Clinicians utilize MCIDs to evaluate whether a physical therapy protocol, nutritional intervention, or medical treatment has yielded a real-world functional benefit.
¶ Gait Speed MCID Thresholds
In older adults, the consensus thresholds for meaningful change in comfortable usual gait speed are highly established. According to the landmark study by Perera et al. (2006), the threshold for a small meaningful change in usual gait speed is 0.05 m/s, while the threshold for a substantial meaningful change is 0.10 m/s [25:3]. This substantial threshold is also widely considered the minimal clinically important difference (MCID) for sarcopenic populations [9:6][25:4].
Clinical trials show that targeted interventional programs can yield substantial gait speed improvements:
- MAS Receptor Activation: Pharmacological activation of the MAS receptor (BIO101, 350 mg bid) in seniors at risk of mobility disability demonstrated a per-protocol usual gait speed improvement of 0.09 m/s after 6 to 9 months of treatment, approaching the sarcopenia MCID of 0.1 m/s [9:7].
- Surgical Prehabilitation: Older adults awaiting total hip replacement who completed a 6–12 week prehabilitation exercise program achieved a significant improvement in fast-paced walking speed (measured by the 40 m Fast-Paced Walk Test) prior to surgery [23:3].
¶ Chair Stand Test MCID Thresholds
For physical functional batteries, Perera et al. (2006) established that a small meaningful change in the Short Physical Performance Battery (SPPB) is 0.5 points, while a substantial meaningful change is 1.0 point [25:5]. These benchmarks are critical for evaluating functional improvements across various clinical cohorts and structured exercise programs:
- Exercise Snacking: Remotely supervised exercise snacking circuits (brief, twice-daily 9-minute circuits of body weight- and chair-based resistance exercises over 28 days) are highly feasible, acceptable, and safe for community-dwelling older adults [7:5].
- Zumba & Caffeine: Combining Zumba training with daily caffeine (100 mg/day) over 12 weeks significantly optimized lower-body endurance strength gains as measured by the 30-Second Chair Stand Test compared to exercise alone [24:3].
- Qigong: An 8-week Qigong exercise program (16 sessions) in older adults produced significant improvements in repeat chair stand performance with effect sizes ranging from 0.45 to 0.87 [21:1].
- Creative Dance: An 8-week creative dance program has been investigated as an active physical activity to support fitness and functional balance in older adults [19:1].
- Perturbation-Based Balance Training: Progressive balance programs, such as technology-supported perturbation treadmills or unstable surface training (using balance pads), have demonstrated high feasibility and task-specific efficacy in improving functional performance, balance, and leg strength capacity in fall-prone cohorts [26].
¶ Biomechanical & Neuromuscular Mechanisms
An analysis of bipedal gait and sit-to-stand transitions reveals several integrated physiological pathways.
¶ The Biomechanics of the Sit-to-Stand Transition
The sit-to-stand movement is clinically divided into four distinct phases, each requiring coordinated muscle contraction and joint stabilization:
Biomechanics of the Sit-to-Stand:
Phase 1: Flexion Momentum --> Phase 2: Momentum Transfer --> Phase 3: Extension --> Phase 4: Stabilization
- Eccentric erector spinae - Maximum hip flexion - Concentric quadriceps - Co-contraction of ankle
- Forward trunk lean - Buttocks leave seat - Hip & knee extension - Center of mass deceleration
- Phase 1 (Flexion Momentum): Starts with the initiation of the movement and ends when the buttocks leave the seat. This phase is characterized by a forward trunk lean, requiring eccentric contraction of the erector spinae and hip extensors to generate forward horizontal momentum.
- Phase 2 (Momentum Transfer): Begins as the buttocks lift off the chair. Horizontal momentum is transferred into vertical lift. This is the most unstable phase of the test, demanding significant eccentric knee and hip stabilizer control to transition the body's center of mass over the feet.
- Phase 3 (Extension): Characterized by rapid vertical acceleration. It requires maximum concentric force generation from the quadriceps femoris (knee extension), gluteus maximus (hip extension), and soleus/gastrocnemius complex (ankle plantarflexion). This phase is highly dependent on lower-limb muscle power and strength [11:8].
- Phase 4 (Stabilization): Begins when vertical extension is complete and ends when the body is fully upright and stable. It requires co-contraction of the ankle stabilizers (tibialis anterior and soleus) and core musculature to decelerate the upward momentum and establish quiet standing balance.
¶ Physiological Factors in Gait Speed
Walking speed is the product of stride length and cadence (step frequency). As biological aging progresses, changes in neuromuscular pathways alter these variables:
- Stride Length Reduction: Older adults often exhibit a shortened stride length due to age-related stiffness in the ankle plantarflexor tendons and a loss of concentric power in the hip extensors (gluteus maximus and hamstrings).
- Double-Support Phase Prolongation: To compensate for balance instability, older or frail individuals spend a greater percentage of the gait cycle in the "double-support phase" (both feet on the ground), which inherently reduces walking velocity.
¶ Confounders and Screening Limitations
While gait speed and chair-stand tests are highly valuable clinical markers, their diagnostic accuracy can be compromised by several confounding factors. Clinicians must identify these limitations to prevent misclassification.
¶ 1. Floor and Ceiling Effects
- Floor Effect in 5XSTS: Severely sarcopenic, osteoarthritic, or highly frail older adults may be completely unable to complete a single chair rise without using their arms. This results in a "failed" test (0 points on the SPPB), rendering the test insensitive to further functional decline in very frail patients.
- Ceiling Effect in Gait Speed: Healthy, active middle-aged and young-old adults (aged 50–65) will easily achieve comfortable gait speeds within normal reference ranges (>1.2 m/s), making the standard comfortable walk test insensitive to early, subclinical neuromuscular deconditioning in these cohorts.
¶ 2. Cognitive Impairment and Adherence
Walking is a complex cognitive-motor task. Normal gait is dynamically related to fluid cognition [14:1], and cognitive decline can alter gait patterns. High cognitive load (dual-task walking) causes gait speed to slow down (e.g., to 1.16 ± 0.23 m/s in midlife [4:14]), reflecting shared neural pathways and limited cognitive-motor reserve.
¶ 3. Dietary and Orthopedic Confounders
Sensory deficits, severe joint cartilage thinning in osteoarthritis, and highly processed diets can affect walking mechanics independently of skeletal muscle mass [22:4]. As highlighted by Lucena et al., skeletal muscle mass has a limited capacity to predict physical performance compared to functional strength and quality, which makes evaluating these dynamic parameters crucial for accurate clinical assessment [11:9].
¶ 4. Home-Testing Limitations
With the rise of telehealth and remote patient monitoring, home-based physical function testing has become increasingly popular; however, unsupervised home environments present severe limitations that compromise both safety and measurement accuracy:
- Lack of Physical Spotting: The absence of a trained clinical spotter dramatically elevates the risk of falls, particularly during the unstable transition phases of the chair-stand test or maximum-velocity gait speed trials. If balance is lost, a lone patient has no immediate physical stabilization.
- Inaccurate Timing Mechanisms: Clinical timing often requires precise sub-second accuracy to detect meaningful changes (such as the 0.1 m/s gait speed MCID). Unsupervised home testing relies on manual smartphone timers, video uploads with variable frame rates, or patient self-reporting, introducing substantial measurement error.
- Unstandardized Surfaces and Equipment: Home settings rarely feature standard clinical chairs or completely level walking courses. Variations in carpet thickness, rug slippage, unstandardized chair heights, and deep-cushioned seating significantly alter the biomechanical work of standing up and walking, making longitudinal tracking unreliable.
¶ Next Steps & Clinical Pathways
When physical functional testing reveals concerning results—such as a usual gait speed below the 1.0 m/s threshold [6:2], a Short Physical Performance Battery (SPPB) score below 9 [3:7], or an abnormally slow 5-repetition chair-rise time [2:9]—it is critical to initiate structured clinical pathways to address the underlying impairments and preserve functional independence:
- Seek Professional Clinical Evaluation: A concerning test result warrants a prompt and comprehensive clinical evaluation to investigate potential underlying etiologies. Clinicians should evaluate cardiorespiratory status, peripheral neurological function, joint health, and nutritional status [10:4] (including screening for malnutrition or risk of malnutrition) to identify treatable contributors to mobility decline.
- Request a Physical Therapy Referral: Refer the patient to a licensed physical therapist for an individualized, prescription-based physical therapy program. Targeted therapy should focus on lower-limb muscular strengthening (addressing dynapenia and power loss), progressive balance challenges (to mitigate fall risk), and gait biomechanics optimization.
- Undergo a Comprehensive Geriatric Assessment (CGA): For older adults exhibiting multi-system vulnerability, undergoing a comprehensive geriatric assessment (CGA) is the gold standard clinical pathway. A CGA is a multidimensional, interdisciplinary diagnostic process that evaluates medical, psychological, and functional capacity (including cognitive screening, polypharmacy review, and home safety assessments) to develop a coordinated, long-term intervention plan.
¶ Comparison of Functional Assessments
Each clinical functional test has unique biomechanical demands, clinical targets, and limitations.
| Clinical Test | Primary Biomechanical Demand | Clinical Target | Primary Advantage | Main Limitation |
|---|---|---|---|---|
| Usual Gait Speed (4MGS) | Neuromuscular coordination, quiet balance, cardiorespiratory efficiency | Global physical frailty, systemic biological age, survival [3:8] | Exceptionally strong prognostic validation; simple and low-cost | Exhibits a ceiling effect in higher-functioning or younger adults |
| 5-Repetition Chair-Stand (5XSTS) | Concentric lower-limb muscular power (quadriceps, gluteals) | Sarcopenia [5:12], dynapenia, fall risk [2:10], functional independence | Measures dynamic lower-limb power; highly sensitive to early aging | Floor effect in highly frail patients who cannot stand without arms |
| 30-Second Chair Stand | Muscular endurance, lower-limb power under fatigue | Functional aerobic capacity, fatigue resistance | Avoids the floor effect; captures work-rate and fatigue curves | Manual counting can introduce minor recording error at start/stop |
| Timed Up and Go (TUG) | Dynamic balance, transitional mobility, agility, turning control | Real-world fall risk, institutional readiness | Evaluates sequential tasks (sit, stand, walk, turn, return, sit) | Highly complex; difficult to isolate specific musculoskeletal deficits |
| Handgrip Strength | Static isometric upper-limb strength | General muscle mass correlation, systemic sarcopenia [5:13] | Extremely reliable; unaffected by lower-limb orthopedic pain | Weakly correlates with real-world functional mobility (e.g., walking, climbing) |
¶ FAQs
¶ References
https://pubmed.ncbi.nlm.nih.gov/35879666/ - Beck Jepsen D, Robinson K, Ogliari G. Predicting falls in older adults: an umbrella review of instruments assessing gait, balance, and functional mobility. BMC Geriatrics. 2022. ↩︎ ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/40394423/ - Kawamura K, Iwase T, Ishino S. Low five-repetition chair stand test and usual gait speed scores predict falls within one year in an outpatient clinic for frailty. European Geriatric Medicine. 2025. ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/31886817/ - Fortes-Filho SQ, Aliberti MJR, Apolinario D. Role of Gait Speed, Strength, and Balance in Predicting Adverse Outcomes of Acutely Ill Older Outpatients. The Journal of Nutrition, Health & Aging. 2020. ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/31603488/ - Rasmussen LJH, Caspi A, Ambler A. Association of Neurocognitive and Physical Function With Gait Speed in Midlife. JAMA Network Open. 2019. ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/39113223/ - Li YH, Wang XH, Ya S. Prevalence and Diagnostic Agreement of Sarcopenia Based on Handgrip Strength and 5-Time Chair-Stand Test Among Chinese Community-Dwelling Older Adults. International Journal of Older People Nursing. 2024. ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/34984437/ - Cai Y, Tian Q, Gross AL. Motor and Physical Function Impairments as Contributors to Slow Gait Speed and Mobility Difficulty in Middle-Aged and Older Adults. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences. 2022. ↩︎ ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/41658611/ - Hu Z, Li S, Shi X. Feasibility and acceptability of a remotely delivered, home-based "exercise snacking" to improve physical function in community-dwelling older adults: a 28-day pilot study. Frontiers in Medicine. 2026. ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/26341720/ - Oesen S, Halper B, Hofmann M. Effects of elastic band resistance training and nutritional supplementation on physical performance of institutionalised elderly--A randomized controlled trial. Experimental Gerontology. 2015. ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/40026058/ - Fielding RA, Dao MM, Cannon K. BIO101 in Sarcopenic Seniors at Risk of Mobility Disability: Results of a Double-Blind Randomised Interventional Phase 2b Trial. Journal of Cachexia, Sarcopenia and Muscle. 2025. ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/35415390/ - Kramer CS, Groenendijk I, Beers S. The Association between Malnutrition and Physical Performance in Older Adults: A Systematic Review and Meta-Analysis of Observational Studies. Current Developments in Nutrition. 2022. ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/42315100/ - Lucena C, Freire YA, Vlietstra L. Sex-Specific Associations of Limb Muscle Strength, Mass, and Quality With Physical Performance in Older Adults: Handgrip and Chair Stand Tests. Journal of Aging and Physical Activity. 2026. ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/41965513/ - Werner C, Schumacher A, Lau S. Cross-sectional and prospective associations between jump performance and functional outcomes in older adults: a systematic review and meta-analysis. BMC Geriatrics. 2026. ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/39399106/ - Yuan H, Kim MK. Exploring the relationship between ultrasound parameters and muscle strength in older adults: a meta-analysis of sarcopenia-related exercise performance. Frontiers in Medicine. 2024. ↩︎
https://pubmed.ncbi.nlm.nih.gov/23349427/ - Clouston SA, Brewster P, Kuh D. The dynamic relationship between physical function and cognition in longitudinal aging cohorts. Epidemiologic Reviews. 2013. ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/39574258/ - Ji S, Jung HW, Yoon S. Comparative Analysis of Gait Speed Measurement Protocols: Static Start Versus Dynamic Start in a Cross-Sectional Study Using Light Detection and Ranging. The Journal of Frailty & Aging. 2024. ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/36292383/ - Lee BK, So WY, Kang HJ. Analysis of Fall Events, Physical Fitness, and Gait Speed According to Fall Risk in Older Korean Women. Healthcare. 2022. ↩︎
https://pubmed.ncbi.nlm.nih.gov/29079030/ - Woo J, Yu R, Leung J. A 3-Item SARC-F. Journal of the American Medical Directors Association. 2018. ↩︎
https://pubmed.ncbi.nlm.nih.gov/39436684/ - Valdés-Aragonés M, Pérez-Rodríguez R, Carnicero JA. Effects of Monitoring Frailty Through a Mobile/Web-Based Application and a Sensor Kit to Prevent Functional Decline in Frail and Prefrail Older Adults: FACET Pilot Randomized Controlled Trial. Journal of Medical Internet Research. 2024. ↩︎
https://pubmed.ncbi.nlm.nih.gov/31055579/ - Joung HJ, Lee Y. Effect of Creative Dance on Fitness, Functional Balance, and Mobility Control in the Elderly. Gerontology. 2019. ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/34935178/ - Suleiman-Martos N, García-Lara R, Albendín-García L. Effects of active video games on physical function in independent community-dwelling older adults: A systematic review and meta-analysis. Journal of Advanced Nursing. 2022. ↩︎
https://pubmed.ncbi.nlm.nih.gov/32942949/ - Chang PS, Lu Y, Nguyen CM. Effects of Qigong Exercise on Physical and Psychological Health among African Americans. Western Journal of Nursing Research. 2021. ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/40480603/ - Akkaya Z, Sims WM, Lynch JA. Ultra-processed food consumption is associated with knee osteoarthritis: Data from the Osteoarthritis Initiative. Osteoarthritis and Cartilage. 2025. ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/40050814/ - Svinøy OE, Nordbø JV, Pripp AH. The effect of prehabilitation for older patients awaiting total hip replacement. A randomized controlled trial with long-term follow up. BMC Musculoskeletal Disorders. 2025. ↩︎ ↩︎ ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/39463442/ - Waer FB, Alexe DI, Chaari F. Caffeine optimizes Zumba training benefits on functional performances in middle-aged women: a randomized trial study. Scientific Reports. 2024. ↩︎ ↩︎ ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/16696738/ - Perera S, Mody SH, Woodman RC, Studenski SA. Meaningful change and responsiveness in common physical performance measures in older adults. Journal of the American Geriatrics Society. 2006. ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
https://pubmed.ncbi.nlm.nih.gov/36921581/ - Brüll L, Hezel N, Arampatzis A. Comparing the Effects of Two Perturbation-Based Balance Training Paradigms in Fall-Prone Older Adults: A Randomized Controlled Trial. Gerontology. 2023. ↩︎