¶ Gastroesophageal Reflux Disease
Gastroesophageal Reflux Disease (GERD) is a highly prevalent, chronic gastrointestinal condition defined by the retrograde movement of gastric contents—including hydrochloric acid, pepsin, and bile—into the esophagus, resulting in troublesome symptoms or mucosal damage. Its sister pathology, Laryngopharyngeal Reflux (LPR), involves the retrograde migration of refluxate into the upper aerodigestive tract, presenting major diagnostic and therapeutic challenges due to clinical uncertainty.
| Primary Pathology | Gastroesophageal Junction (GEJ) Dysfunction |
| Main Mechanisms | TLESRs, Hiatal Hernia, Acid Pocket, Obesity |
| First-line Interventions | Lifestyle, Positioning, Alginate Gel Rafts |
| Pharmacotherapy | PPIs (short-term), H2RAs (intermittent) |
| Critical Risks | Barrett's Esophagus, Long-term PPI Hazards |
| Key Diagnostic Tool | Upper Endoscopy, pH-Impedance Monitoring |
¶ At a glance
¶ Key Points
- Mechanical Dysfunction: GERD is primarily a structural and mechanical failure of the gastroesophageal junction (GEJ) barrier, rather than a simple excess of stomach acid.
- Non-Systemic Preference: Physical, non-systemic barriers—specifically alginate gel rafts—offer rapid, target-specific relief and displace the postprandial "acid pocket" without systemic side effects.
- Suppression Hazards: Chronic proton pump inhibitor (PPI) therapy is associated with systematic long-term risks, including bone fractures, micronutrient deficiencies, chronic kidney disease, and enteric infections.
¶ What People Use It For
- Symptom Resolution: Alleviating typical symptoms (heartburn, acid regurgitation) and extraesophageal symptoms (chronic cough, throat clearing).
- Mucosal Healing: Healing erosive esophagitis and preventing complications (peptic strictures, Barrett's esophagus).
- Evidence Quality: High (Tier 1 systematic reviews and clinical guidelines support lifestyle and pharmacological therapies).
¶ Safety "Traffic Light"
- ● RED LIGHT (STOP & ESCALATE): The presence of Alarm Features (dysphagia, odynophagia, unexplained weight loss, gastrointestinal bleeding, anemia, or persistent vomiting) mandates immediate referral for urgent upper endoscopy to rule out esophageal adenocarcinoma or strictures.
- ● YELLOW LIGHT (CAUTION): Continuous use of Proton Pump Inhibitors (PPIs) beyond 8 weeks, or Histamine-2 Receptor Antagonists (H2RAs) beyond 2 weeks, requires explicit clinical justification. Long-term PPIs induce hypochlorhydria, causing malabsorption and infection risks, while H2RAs trigger rapid tachyphylaxis (tolerance).
- ● GREEN LIGHT (GO): First-line lifestyle modifications (weight loss, sleep positioning, meal-to-sleep timing) and on-demand, non-systemic alginate therapies are highly safe and should be utilized as baseline interventions for all patients.
¶ Protocol Card
¶ 1. The Sleep & Mechanical Positioning Protocol
- Bed Elevation: Elevate the head of the bed by 15–20 cm (6–8 inches) using solid blocks under the bedposts or a high-density polyurethane sleep wedge [1][2].
- Sleep Posture: Prioritize sleeping in the left lateral decubitus (left-side) position. This positions the gastroesophageal junction above the level of gastric acid pool, structurally reducing reflux events [2:1].
- Meal-to-Sleep Gap: Maintain a strict minimum 3-hour upright window between the final meal of the day and reclining or sleeping [3].
¶ 2. The Non-Systemic Alginate Raft Protocol
- Formulation: Utilize a high-potency sodium alginate or magnesium alginate formulation combined with a bicarbonate buffering agent.
- Dosing: Take 500–1000 mg of alginate in liquid or chewable tablet form 30 minutes post-meal and immediately before bedtime [4][5].
- Administration: Avoid drinking water or fluids immediately after intake to preserve the physical integrity of the floating gel raft.
¶ 3. Standard Pharmacological Tapering Protocol (For PPI De-escalation)
- Objective: Prevent rebound acid hypersecretion upon discontinuation [6].
- Step-Down: Reduce the PPI dose by 50% every 1–2 weeks (e.g., from 40 mg daily to 20 mg daily, then to 20 mg every other day).
- Bridging Therapy: Co-administer on-demand alginate rafts [7] or an H2RA (e.g., Famotidine 20 mg) on alternate days during the tapering phase to manage breakthrough symptoms.
¶ Bottom Line
Gastroesophageal Reflux Disease is fundamentally a failure of the mechanical anti-reflux barrier. Long-term management should prioritize mechanical and non-systemic solutions—such as physical positioning, weight loss, and alginate raft-forming agents—while reserving systemic acid suppressants for short-term mucosal healing of documented erosive esophagitis.
¶ The "Why" (Benefits of Reflux Control)
Maintaining optimal gastroesophageal junction integrity and preventing chronic reflux of gastric contents yields profound local and systemic physiological benefits:
- Esophageal Mucosal Integrity: Chronic exposure to hydrochloric acid and pepsin destroys the esophageal squamous epithelium, leading to painful erosions, peptic strictures, and the metaplastic transformation known as Barrett's esophagus [8][9].
- Aerodigestive and Pulmonary Preservation: Uncontrolled micro-aspiration of gastric contents can induce severe airway hyperresponsiveness, chronic laryngitis, dental erosion, and accelerate fibrotic pulmonary decline [10].
- Sleep Architecture Optimization: Nocturnal reflux triggers brief cortical arousals and activates autonomic stress pathways. Controlling nocturnal acid exposure restores deep sleep architecture and prevents micro-arousals [2:2][7:1].
- Systemic Inflammatory Reduction: Chronic epithelial damage and subsequent immune activation in the esophagus promote localized cytokine release, contributing to systemic low-grade inflammatory loads.
¶ Reality Check & Clinical Nuance
¶ Human Clinical Reality vs. Mouse Hopes
Reflux pathophysiology in rodents is heavily restricted by anatomical differences, such as a highly developed forestomach and different mechanical angles of the diaphragm, making animal models poor representations of human GERD. In humans, reflux is predominantly a mechanical and hydrostatic pressure disease [8:1]. The primary clinical drivers are:
- Transient Lower Esophageal Sphincter Relaxations (TLESRs): Brief, vagally mediated relaxations of the LES independent of swallowing, triggered by gastric distension [11].
- Visceral Adiposity: Central obesity acts as a mechanical bellows, directly increasing intra-abdominal pressure and forcing gastric contents upward through the GEJ [8:2][11:1].
¶ The "Trigger Food" Myth
For decades, clinical guidelines mandated the strict, universal elimination of dietary triggers: caffeine, alcohol, chocolate, carbonated drinks, citrus, and mint. However, modern high-quality clinical data has challenged this dogma.
The 2022 ACG Clinical Guideline explicitly states that routine, universal elimination of these foods is not recommended [8:3]. Clinical trials have shown that blanket dietary restrictions do not consistently improve esophageal pH profiles or symptom scores across unselected populations [11:2]. Instead, modern clinical practice advocates for a targeted elimination approach: patients should only restrict specific items that they have empirically identified as reproducible triggers of their symptoms.
¶ Non-Systemic Solutions: The Alginate Advantage
Traditional treatment pathways default to systemic acid suppression using PPIs. While highly effective at elevating gastric pH, PPIs do not prevent the mechanical act of reflux; they merely make the refluxate less acidic.
Alginates, derived from brown seaweed (Phaeophyceae), present a paradigm shift. Upon contact with gastric acid, alginate precipitates into a low-density, pH-neutral cohesive gel raft within minutes [4:1][5:1]. This raft floats on top of the gastric contents, creating a physical barrier at the GEJ that blocks both acid and non-acid (pepsin, bile) reflux. Clinical trials show alginates are superior to antacids and comparable to PPIs for rapid, on-demand symptom relief without disrupting systemic biochemistry or acid-dependent nutrient absorption [4:2][12].
¶ Practical Integration
¶ Daily Lifestyle and Ergonomics
Successfully managing GERD requires a highly structured, mechanical approach to daily routines:

[Wake Up] ──> [Light Physical Activity] ──> [Dinner: Low Volume, >3h before bed] ──> [Alginate Raft] ──> [Sleep: Left-Side & Elevated]
- Meal Volume and Composition: Large, high-fat meals delay gastric emptying and increase gastric volume, directly provoking TLESRs and mechanical tension on the LES [13][11:3]. Patients should transition to smaller, nutrient-dense meals.
- Physical Activity Timing: Avoid high-impact exercise, deep bending, or abdominal compression (e.g., heavy squats or core work) within 2 hours of eating, as these activities compress the stomach and overwhelm the LES barrier.
- Bariatric and Surgical Interventions: In patients with severe, medically refractory obesity (BMI >35 kg/m²) and comorbid GERD, surgical choices are critical. Laparoscopic Roux-en-Y gastric bypass (RYGB) is highly effective and considered the gold standard for resolving GERD, whereas sleeve gastrectomy can worsen or induce de novo GERD in up to 30% of patients due to increased intragastric pressure [14][15].
¶ Mechanism of Action
¶ 1. LES Physiology and TLESRs
The anti-reflux barrier is a sophisticated "double-sphincter" system consisting of:
- The Lower Esophageal Sphincter (LES): An intrinsic smooth muscle bundle at the distal esophagus, maintaining a baseline resting pressure of 10–30 mmHg.
- The Crural Diaphragm: The extrinsic skeletal muscle of the diaphragm surrounding the LES, which acts as an external pinch-cock during inspiration and periods of increased intra-abdominal pressure.
In healthy individuals, transient lower esophageal sphincter relaxations (TLESRs) occur to facilitate gas belching. These relaxations are mediated by a vago-vagal reflex pathway triggered by mechanoreceptors in the gastric cardia and fundus sensing distension [11:4]. In GERD patients, the frequency or duration of TLESRs is pathologic, or they occur at inappropriate times, allowing gastric contents to escape.
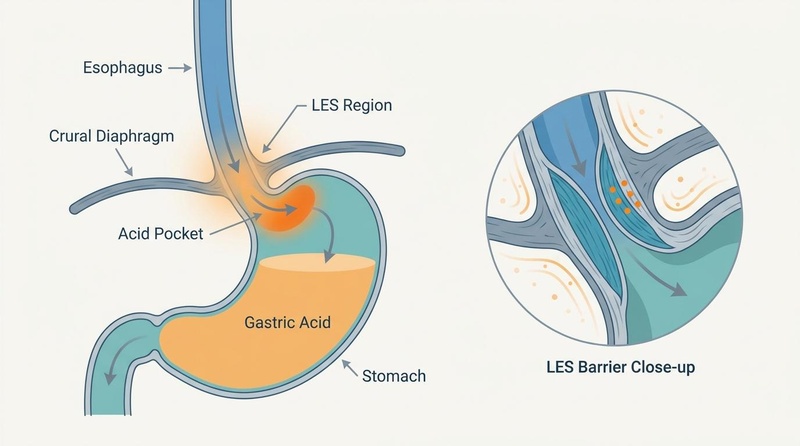
¶ 2. Hiatal Hernia and the "Acid Pocket"
The presence of a sliding hiatal hernia severely disrupts the spatial alignment of this double-sphincter system. The GEJ slides upward through the diaphragmatic hiatus into the low-pressure thoracic cavity. This separation abolishes the synergistic mechanical support of the crural diaphragm on the LES.
Normal Anatomy: Hiatal Hernia Disruption:
│ │ │ │
────┴───┴──── <-- Diaphragm ────┴ ┴──── <-- Diaphragm (Widened)
[LES] [LES] <-- Slid upward into thorax
Stomach Stomach
Furthermore, hiatal hernias promote the formation of the gastric acid pocket. Following a meal, a highly acidic (pH 1.5–2.0) layer of unbuffered gastric juice pools at the top of the gastric contents, immediately below the GEJ [11:5]. In patients with a hiatal hernia, this acid pocket becomes trapped within the hernia sac, acting as an unbuffered reservoir that is easily pushed into the esophagus during inspiration or minor abdominal compression [11:6].
¶ 3. Alginate Raft Chemistry
The mechanical blocking action of alginates relies on a rapid, three-step chemical reaction in the gastric lumen:
- Precipitation: Upon exposure to gastric acid, soluble sodium alginate immediately precipitates into an insoluble, viscous alginic acid gel raft [4:3].
- Entrapment of Gas: Concurrently, calcium carbonate or sodium bicarbonate reacts with gastric acid to produce carbon dioxide () gas bubbles. These bubbles become trapped within the precipitating gel matrix.
- Cross-linking: Calcium ions () released from calcium carbonate cross-link the alginate polymer chains, drastically increasing the tensile strength and cohesiveness of the raft, which floats buoyantly atop the gastric acid pool [12:1].
¶ Evidence Summary Table (Human Outcomes)
The clinical efficacy of major interventions for GERD and extraesophageal reflux is summarized below, based exclusively on human clinical trials and systematic reviews:
| Intervention | Primary Outcome | Effect Size / Clinical Impact | Efficacy Consistency | Evidence Quality (GRADE) | Key Clinical Details |
|---|---|---|---|---|---|
| Weight Loss | Reduction in esophageal acid exposure & symptoms | High | High | Strongly recommended for all overweight or obese GERD patients [8:4]. | |
| Head of Bed Elevation | Reduction in nocturnal acid exposure & sleep disturbance | High | Moderate | Requires physical bed elevation (15–20 cm) or high-density wedges, not pillows [2:4]. | |
| Meal-to-Sleep Gap (>3h) | Reduced nocturnal reflux episodes | Moderate | Moderate | Critical for patients with nocturnal heartburn or laryngopharyngeal reflux [3:2]. | |
| Alginate Raft Therapy | Rapid postprandial symptom control | High | High | Non-systemic; ideal for on-demand use, mild GERD, and during pregnancy [4:5][12:2]. | |
| Proton Pump Inhibitors (PPIs) | Healing of erosive esophagitis and symptom control | High | High | Most potent acid suppressants; should be used for the shortest necessary duration [8:6]. | |
| H2 Receptor Antagonists | Short-term acid suppression | Low | Moderate | Limited by rapid tachyphylaxis (tolerance) within 7–14 days of continuous use [16:1]. |
¶ Clinical Decision Pathway
The structured clinical workflow for the triage, diagnostic evaluation, and therapeutic management of reflux symptoms is detailed below:
[Patient Presents with Reflux Symptoms]
│
┌────────────────┴────────────────┐
▼ ▼
[Alarm Features Present?] [No Alarm Features]
(Dysphagia, Weight Loss, Anemia) │
│ ▼
▼ [Typical GERD Symptoms?]
[Urgent Upper Endoscopy] (Heartburn, Regurgitation)
│ │
┌──────────────┴──────────────┐ ┌─────────┴─────────┐
▼ ▼ ▼ ▼
[Esophageal Ca / [Benign/Erosive] [Yes] [No / Atypical / LPR]
Stricture] │ │ (Cough, Hoarseness)
│ ▼ ▼ │
[Oncology / Surgical] [Lifestyle + [Lifestyle + ▼
Intervention] PPI course] Alginates] [Diagnostic Uncertainty]
│ │
▼ ▼
[Empiric 8-Wk [pH-Impedance Monitoring]
PPI Trial] │
│ ▼
▼ [Confirm Reflux Source?]
[Refractory?] ┌─────────┴─────────┐
┌───────┴───────┐ ▼ ▼
▼ ▼ [Yes] [No]
[Yes] [No] │ │
│ │ ▼ ▼
▼ ▼ [Targeted PPI/ [Rule out Functional
[pH-Impedance [Taper to Alginate Rx] or Neuropathic Vocal
Monitoring] Minimum] Cord Etiologies]
¶ Comprehensive Safety, Toxicology, & Clinical Considerations
¶ 1. Proton Pump Inhibitors: Long-Term Hazards
Proton pump inhibitors (e.g., Omeprazole, Esomeprazole, Pantoprazole) are highly effective at suppressing gastric acid by irreversibly binding to the active ATPase pump of parietal cells [8:7]. However, their chronic, long-term use is associated with systemic physiological disruptions:
- Micronutrient Depletion: Gastric acid is highly necessary for liberating vitamin B12 from dietary proteins and solubilizing minerals for absorption. Chronic hypochlorhydria leads to clinical vitamin B12 deficiency [8:8], hypomagnesemia (which can cause cardiac arrhythmias), and impaired calcium absorption [13:2].
- Osteoporosis and Fractures: Impaired calcium absorption and direct osteoclast inhibition by PPIs increase the risk of osteoporosis and hip, wrist, or spine fractures with long-term high-dose therapy [13:3].
- Renal Impairment: PPI use is associated with a significantly increased risk of acute interstitial nephritis and a gradual decline in glomerular filtration rate, culminating in chronic kidney disease (CKD) [8:9].
- Infection Susceptibility: Gastric acid is a primary immunological barrier. Hypochlorhydria permits bacterial overgrowth, leading to a 2- to 3-fold increased risk of Clostridioides difficile-associated diarrhea and an increased incidence of small intestinal bacterial overgrowth (SIBO) and community-acquired pneumonia [13:4].
¶ 2. Histamine-2 Receptor Antagonists: The Tachyphylaxis Limitation
Histamine-2 receptor antagonists (H2RAs; e.g., Famotidine, Cimetidine) inhibit acid secretion by blocking H2 receptors on parietal cells. While highly useful for managing mild GERD or nocturnal acid breakthrough, their efficacy rapidly decays:
- Rapid Tolerance: Continuous daily administration of H2RAs induces tachyphylaxis (pharmacological tolerance) within 7 to 14 days [16:2]. This is driven by compensatory upregulation of gastrin receptors and alternative parietal cell stimulation pathways, rendering daily H2RA monotherapy ineffective for long-term control [16:3]. H2RAs must be used intermittently or as short-term bridging agents only.
¶ 3. Barrett's Esophagus Screening
Barrett's esophagus is a premalignant metaplastic change wherein the normal stratified squamous epithelium of the esophagus is replaced by simple columnar epithelium with goblet cells (intestinal metaplasia), driven by chronic acid and bile exposure [9:1]. It carries a major risk of progression to esophageal adenocarcinoma.
- Screening Criteria (ACG 2022 Guidelines): Routine screening is recommended in patients with chronic GERD symptoms (>5 years) and two or more of the following established risk factors [9:2]:
- Male sex (male-to-female ratio is up to 8:1 for adenocarcinoma)
- Age > 50 years
- White race
- Chronic tobacco use (current or history)
- Central adiposity (obesity)
- First-degree relative with Barrett's esophagus or esophageal adenocarcinoma
- Screening Modality: Screening is performed via upper endoscopy (EGD) with target biopsy using Seattle protocol. If negative, routine repeat screening is not indicated [9:3].
¶ 4. Laryngopharyngeal Reflux (LPR) Clinical Uncertainty
Laryngopharyngeal reflux, also termed "silent reflux" or extraesophageal reflux, represents a distinct clinical entity where refluxate breaches the upper esophageal sphincter to affect the larynx, pharynx, and trachea [10:1]. It is characterized by high clinical uncertainty:
- Non-Specific Symptoms: Symptoms like throat clearing, globus sensation (feeling of a lump in the throat), hoarseness, and chronic dry cough are highly non-specific and are frequently caused by non-reflux etiologies (e.g., environmental allergies, post-nasal drip, vocal abuse, or laryngeal sensory neuropathy) [10:2].
- Poor PPI Response Rate: Over 50–60% of patients diagnosed with LPR fail to respond to empiric PPI therapy [10:3]. This suggests that either the symptoms are not caused by acid reflux, or that non-acid components (pepsin and bile) are driving the laryngeal irritation.
- Objective Monitoring Mandate: Expert clinical guidelines (AGA 2023 Update) recommend against long-term, high-dose empiric PPI therapy for LPR without objective verification. Patients presenting with suspected LPR should undergo 24-hour ambulatory dual-probe pH-impedance monitoring off PPI therapy to confirm a temporal association between physical reflux events and symptoms before committing to chronic medical therapy [10:4].
¶ 5. Clinical Red Flags (Alarm Features)
The presence of any of the following symptoms represents a major clinical risk and requires immediate diagnostic referral for upper endoscopy (EGD) to rule out malignancy or advanced structural complications:
- Dysphagia: Difficulty swallowing food or liquids (highly suggestive of mechanical stricture or adenocarcinoma).
- Odynophagia: Painful swallowing (often indicating deep esophageal ulceration or severe esophagitis).
- Unexplained Weight Loss: Rapid, involuntary weight loss (>5% of body weight over 6 months).
- Gastrointestinal Bleeding: Hematemesis ("coffee-ground" vomit) or melena (black, tarry stools).
- Unexplained Anemia: Iron-deficiency anemia of unknown origin (suggesting chronic occult blood loss).
- Persistent Vomiting: Intractable, recurrent vomiting of gastric contents.
¶ Age and Gender Stratification
Reflux epidemiology, risks, and management choices differ significantly across life stages and biological sexes:
- Young Adults: Experiencing a rising incidence of GERD, heavily associated with sleep deprivation, high-stress environments, and consumption of late-night ultra-processed foods [13:5]. Management should strictly focus on lifestyle modification and on-demand alginate use to avoid early-onset, lifelong PPI dependency.
- Pregnancy (Women): Up to 50% of pregnant women experience severe GERD, driven by progesterone-mediated relaxation of the LES and increased intra-abdominal pressure from the gravid uterus [11:8]. Because systemic drugs can cross the placental barrier, non-systemic alginate formulations are highly favored and have demonstrated an exceptional safety and efficacy profile in this population [12:3].
- Men: Carry a highly disproportionate risk of developing Barrett's esophagus and progressing to esophageal adenocarcinoma compared to women [9:4]. Long-standing, untreated GERD (>5 years) in men over age 50 with central obesity requires rigorous clinical screening [9:5].
- Older Adults (65+): Frequently present with atypical, "silent" symptoms due to age-related visceral hyposensitivity (reduced esophageal pain perception) [13:6]. They may present solely with recurrent micro-aspiration pneumonia, chronic cough, or unexplained weight loss. Older adults are also highly vulnerable to the long-term side effects of PPIs, particularly bone loss/fractures and cognitive interactions, necessitating regular deprescribing audits [13:7].
¶ Comparisons & Engagement
¶ "Compare With" (Reflux Therapies)
| Feature / Metric | Proton Pump Inhibitors (PPIs) | H2 Receptor Antagonists (H2RAs) | Alginate Raft Formulations | Standard Antacids |
|---|---|---|---|---|
| Primary Mechanism | Irreversible inhibition of parietal cell ATPase pumps. | Competitive inhibition of H2 receptors on parietal cells. | Forms a physical, buoyant gel barrier atop gastric acid. | Chemical neutralization of gastric hydrochloric acid. |
| Systemic Absorption | High (requires systemic circulation to act). | High (systemic H1/H2 blockade). | None (purely physical, local action). | Variable (calcium/magnesium absorption). |
| Onset of Action | 1–3 days (requires steady-state accumulation). | 30–60 minutes. | 1–3 minutes (immediate local precipitation). | 5–15 minutes. |
| Duration of Action | 24–48 hours. | 4–10 hours. | 2–4 hours (typically postprandially). | 30–60 minutes. |
| Tachyphylaxis Risk | None. | High (tolerance develops within 7–14 days) [16:4]. | None (mechanism is purely mechanical). | None. |
| Key Long-Term Risks | CKD, osteoporosis, hypomagnesemia, C. diff, B12 deficiency [8:10]. | Gynecomastia (with cimetidine), cognitive dysfunction in older adults. | Minor sodium/potassium load (must monitor in severe hypertension/renal failure). | Rebound acidity, hypercalcemia, constipation, or diarrhea. |
| Bile/Pepsin Blocking | No (only raises pH; does not block mechanical reflux). | No (only raises pH; does not block mechanical reflux). | Yes (entrapment and physical blocking of all refluxate components) [4:6]. | No. |
¶ References
¶ Update Log
¶ March 2026
- Established comprehensive gastroesophageal reflux disease guide covering TLESRs, hiatal hernia, gastric acid pocket mechanics, and LPR diagnostic clinical uncertainty.
- Added GRADE-assessed evidence summaries for mechanical positioning, lifestyle triggers, alginate rafts, and systemic acid-suppressant risk-benefit profiles.
Villamil Morales IM, Gallego Ospina DM, Otero Regino WA. Impact of head of bed elevation in symptoms of patients with gastroesophageal reflux disease: a randomized single-blind study (IBELGA). Gastroenterologia y Hepatologia. 2020 Jun-Jul;43(6):317-323. https://pubmed.ncbi.nlm.nih.gov/32229033/ ↩︎ ↩︎
Person E, Rife C, Freeman J, et al. A Novel Sleep Positioning Device Reduces Gastroesophageal Reflux: A Randomized Controlled Trial. Journal of Clinical Gastroenterology. 2015 Sep;49(8):655-660. https://pubmed.ncbi.nlm.nih.gov/26053170/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Piesman M, Hwang I, Maydonovitch C, et al. Nocturnal reflux episodes following the administration of a standardized meal. Does timing matter? The American Journal of Gastroenterology. 2007 Oct;102(10):2128-2134. https://pubmed.ncbi.nlm.nih.gov/17573791/ ↩︎ ↩︎ ↩︎
Zhao CX, Wang JW, Gong M. Efficacy and safety of alginate formulations in patients with gastroesophageal reflux disease: a systematic review and meta-analysis of randomized controlled trials. European Review for Medical and Pharmacological Sciences. 2020 Nov;24(22):11843-11850. https://pubmed.ncbi.nlm.nih.gov/33275256/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Pizzorni N, Ambrogi F, Eplite A, et al. Magnesium alginate versus proton pump inhibitors for the treatment of laryngopharyngeal reflux: a non-inferiority randomized controlled trial. European Archives of Oto-Rhino-Laryngology. 2022 May;279(5):2613-2621. https://pubmed.ncbi.nlm.nih.gov/35032204/ ↩︎ ↩︎ ↩︎
Reimer C, Søndergaard B, Hilsted L. Proton-pump inhibitor therapy induces acid-related symptoms in healthy volunteers after withdrawal of therapy. Gastroenterology. 2009 Jul;137(1):80-87. https://pubmed.ncbi.nlm.nih.gov/19362552/ ↩︎
Bolt J, Thompson W, Inglis C. Appropriate Use of Proton Pump Inhibitors in Older Adults: Concerns and Solutions. Drugs & Aging. 2026 Jan. https://pubmed.ncbi.nlm.nih.gov/41269594/ ↩︎ ↩︎
Katz PO, Dunbar KB, Schnoll-Sussman FH. ACG Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease. The American Journal of Gastroenterology. 2022 Jan 1;117(1):27-56. https://pubmed.ncbi.nlm.nih.gov/34807007/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Shaheen NJ, Falk GW, Iyer PG. Diagnosis and Management of Barrett's Esophagus: An Updated ACG Guideline. The American Journal of Gastroenterology. 2022 Apr 1;117(4):559-585. https://pubmed.ncbi.nlm.nih.gov/35354777/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chen JW, Vela MF, Peterson KA. AGA Clinical Practice Update on the Diagnosis and Management of Extraesophageal Gastroesophageal Reflux Disease: Expert Review. Clinical Gastroenterology and Hepatology. 2023 Jun;21(6):1414-1421.e1. https://pubmed.ncbi.nlm.nih.gov/37061897/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kaltenbach T, Crockett S, Gerson LB. Are lifestyle measures effective in patients with gastroesophageal reflux disease? An evidence-based approach. Archives of Internal Medicine. 2006 May 8;166(9):965-971. https://pubmed.ncbi.nlm.nih.gov/16682569/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Senthilkumaran M, Hui K, Li C. Alginate Therapy for Gastroesophageal Reflux in Pregnancy: A Scoping Review. The Laryngoscope. 2026 Apr. https://pubmed.ncbi.nlm.nih.gov/41342394/ ↩︎ ↩︎ ↩︎ ↩︎
Andrawes M, Andrawes W, Das A. Proton Pump Inhibitors (PPIs)-An Evidence-Based Review of Indications, Efficacy, Harms, and Deprescribing. Medicina. 2025 Aug 31;61(9):410. https://pubmed.ncbi.nlm.nih.gov/41010960/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kraljevic M, Süsstrunk J, Wölnerhanssen BK. Long-Term Outcomes of Laparoscopic Roux-en-Y Gastric Bypass vs Laparoscopic Sleeve Gastrectomy for Obesity: The SM-BOSS Randomized Clinical Trial. JAMA Surgery. 2025. https://pubmed.ncbi.nlm.nih.gov/39969869/ ↩︎
Ani FC, Loo GH, Chua RHB. Integrating cruroplasty with laparoscopic sleeve gastrectomy: a strategy to mitigate GERD symptoms in obese patients. A randomized control trial. Langenbeck's Archives of Surgery. 2025 Aug 13. https://pubmed.ncbi.nlm.nih.gov/40796984/ ↩︎
Clark JH, Hussain Z, Akst L. Histamine 2-Receptor Antagonists Tachyphylaxis: A Scoping Review. The Laryngoscope. 2026 Jun. https://pubmed.ncbi.nlm.nih.gov/41459837/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎