¶ Grip Strength Testing
| Mechanism | Isometric force transduction (hydraulic/strain-gauge) |
| Key Spec | Peak Force (kg or lbs) |
| Protocol | 3 trials per hand, 10–60s rest, record maximum |
| FDA Class | Class I (Exempt) |
| Entry Cost | $15 - $50 (electronic) / $300+ (hydraulic) |
Handgrip strength testing, performed via isometric handgrip dynamometry, is a validated, non-invasive diagnostic measurement used to quantify upper-extremity muscle function [1]. Serving as a primary clinical screening tool for sarcopenia, dynapenia, and physical frailty, handgrip strength (HGS) acts as an exceptionally robust biomarker of systemic physiological reserve and is strongly associated with long-term survival and overall health status [2][3][4][1:1][5].
¶ At a Glance
¶ Key Takeaways
- Does HGS testing work?: Yes. Handgrip strength (HGS) testing is an exceptionally reliable and validated clinical measurement [1:2]. It possesses high test-retest and inter-rater reliability when performed under standardized conditions, making it an essential screening tool for identifying muscle weakness and probable sarcopenia [1:3][5:1].
- Who needs it?: Older adults seeking early identification of age-related sarcopenia or frailty [5:2], and longevity enthusiasts using absolute grip strength as a functional biomarker to track neuromuscular aging and systemic physiological reserve [2:1][3:1][1:4].
- Verdict: Handgrip dynamometry is a low-cost, rapid, and non-invasive assessment of upper-extremity muscle function [2:2][1:5]. It serves as a valuable clinical screening tool, where lower absolute grip strength is strongly associated with elevated mortality risks [2:3][3:2][4:1].
- Safety "Traffic Light":
- ● GREEN: Safe to proceed for the general population, healthy adults, and clinical screening cohorts seeking baseline physical assessment [2:4][1:6].
- ● AMBER: Proceed with caution under clinical guidance for individuals with active localized hand or wrist pain, or a history of recent minor hand, wrist, or finger injury. In patients with inflammatory joint pathology (such as rheumatoid arthritis), systemic inflammation and joint degradation can significantly impair force generation, requiring careful clinical interpretation of scores [6][7].
- ● RED: Strictly contraindicated for individuals with acute or unhealed bone fractures of the hand, wrist, or forearm, unhealed tendon or ligament ruptures in the active hand, or unstable cardiovascular disease where high-intensity isometric contractions can induce dangerous spikes in blood pressure or myocardial oxygen demand.
¶ Protocol Card
- Equipment: Standard clinical hydraulic or validated digital dynamometer [1:7][8][9].
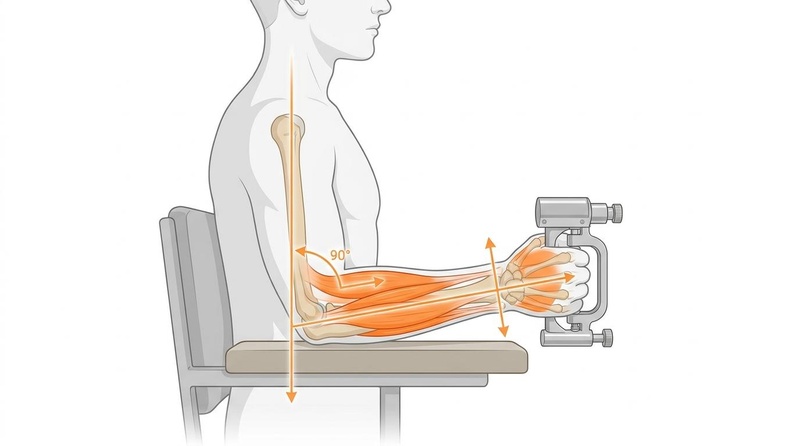
- Posture: Position varies across protocols, with the subject's position representing a major source of variation in clinical and epidemiological studies [10][1:8].
- Arm Position: No single standard exists, as studies show wide variation in arm support and positioning, which can directly affect recorded grip values [10:1][1:9].
- Execution: Squeeze with maximal isometric effort; scoping reviews indicate that verbal encouragement is typically omitted during clinical testing to maintain standardized conditions [10:2].
- Trial Count & Scoring: Typically measured three times (often in the dominant hand alone or both hands), with the maximum or mean score being recorded [10:3][1:10].
- Rest Period: Provide a rest interval between successive trials on the same hand, typically ranging from 10 to 20 seconds up to 1 minute, to prevent localized muscular fatigue [10:4].
¶ Bottom Line
Handgrip strength testing is a rapid, inexpensive, and exceptionally robust clinical biomarker of physiological reserve [1:11], where lower absolute HGS is associated with a significantly higher risk of long-term mortality [2:5][3:3][4:2]. It serves as an essential assessment tool for identifying early neuromuscular decline and guiding targeted physical or nutritional interventions, such as progressive resistance exercise [5:3][11][12].
¶ Evidence Summary Table (Human Outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence Quality | Trials / Cohorts*** | Notes (Population, Duration, Context) |
|---|---|---|---|---|---|
| Sarcopenia Screening Accuracy | High | High | Clinical Consensus | Formally established as the primary screening gateway and diagnostic indicator for probable sarcopenia in clinical guidelines [5:4][11:1]. | |
| All-Cause Mortality Prognostication | High | High | Longitudinal Cohorts | Lower HGS is significantly associated with an increased hazard of premature mortality, functional decline, and prolonged hospital stays in older adults [2:6][3:4][4:3], and predicts hospitalizations and long-term mortality in stable chronic obstructive pulmonary disease (COPD) rehabilitation patients [13]. | |
| Cardiovascular Risk Stratification | High | Moderate | Large Prospective Cohort | In patients with type 2 diabetes, low HGS (particularly combined with obesity) independently predicts a 2.29-fold higher risk of incident heart failure [14]; also strongly associated with delayed orthostatic blood pressure recovery and orthostatic hypotension [15][16]. | |
| Biological Age / Functional Capacity Correlation | High | High | Multi-Cohort Normative Studies | Acts as a robust indicator of systemic physiological reserve and biological aging; normative references show clear curvilinear decline across the lifespan [17], while serial testing variability serves as an entropic biomarker of aging [18]. | |
| Physical Fitness & Frailty Association | High | High | Systematic Reviews & Meta-Analyses | Strongly associated with physical fitness components and frailty syndrome in older populations, with usual walking speed being the most strongly associated fitness test [19]. | |
| Sarcopenia Rehabilitation | High | High | Systematic Reviews & Meta-Analyses | Progressive resistance exercise significantly improves handgrip strength, muscle quality, and physical performance in older adults [5:5][11:2][12:1]. |
- *Effect: Number of arrows (1-3) indicates magnitude. Direction: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Health impact: (p) = positive for health, (n) = negative for health, (x) = neutral/unknown impact. Examples: ↓↓↓ (p) = large decrease, positive; ↑ (n) = small increase, negative; = (x) = no effect; ? = unclear.
- *Compact renderer encoding:
e="[dir][mag][impact]"wheredir=u|d|e|q(up/down/equal/question),mag=0|1|2|3(magnitude),impact=p|n|x(positive/negative/neutral). Examples:↓↓ (p)->d2p,= (x)->e0x,?->q0x. - **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- ***Trials/Cohorts: Represents clinical guidelines, pooled databases, and long-term longitudinal studies.
¶ Mechanism
¶ Physiology of Handgrip Strength
Grip strength is not merely a localized measure of forearm muscular force, but an integrated output of multiple physiological systems. Generating maximal grip force requires seamless neuromuscular coordination, initiated by the motor cortex of the brain. The central nervous system transmits electrical signals down the spinal cord to the peripheral nerves (such as the radial, ulnar, and median nerves), facilitating rapid motor unit recruitment within the forearm flexor muscles and intrinsic hand muscles. The absolute magnitude of force generated is intrinsically dependent on skeletal muscle mass (the cross-sectional area of the contracting fibers) and muscle quality [2:7]. Additionally, manual muscle testing in rehabilitation contexts often evaluates grip strength alongside wrist and finger extension to characterize peripheral motor function [20].
Standard grip testing measures this combined isometric force, with Jamar-style dynamometers serving as the clinical standard [1:12]. Standard reference ranges demonstrate that handgrip strength varies significantly by biological sex and declines progressively with age [17:1]. This progressive decline represents underlying neuromuscular aging, loss of muscle mass, and general degradation of muscle quality, which can be addressed through targeted progressive resistance training and nutritional interventions [2:8][5:6][11:3][12:2].
¶ Local Pathologies Confounding Measurement
Because handgrip strength is a localized measurement of upper-extremity force, the presence of specific local joint and nerve pathologies in the hand and forearm can confound results, meaning low HGS scores must be interpreted with clinical caution:
- Inflammatory Joint Pathology: Chronic inflammatory conditions, such as rheumatoid arthritis, are strongly associated with local joint degradation and muscle depletion, which can significantly alter handgrip strength [6:1]. In patients with rheumatoid arthritis, chronic inflammation can accelerate muscle wasting, leading to lower absolute grip strength and a significantly higher prevalence of sarcopenia compared to healthy controls [6:2].
- Peripheral Neuropathies: Localized nerve lesions, such as radial nerve palsy, directly impair the innervation of the forearm muscles. In patients with peripheral paresis of radial-innervated forearm muscles, clinical scales like the Medical Research Council (MRC) scale and dynamometric measurements of grip strength have been validated as reliable tools to quantify the localized degree of motor impairment [20:1].
¶ Device Types: Hydraulic vs. Electronic
Quantification of isometric handgrip force in clinical and epidemiological research typically utilizes one of two primary device types:
- Hydraulic Dynamometers: The standard hydraulic Jamar dynamometer remains the most widely cited and utilized instrument in clinical literature [1:13]. It operates as a sealed system where the force exerted on the adjustable handle is mechanically transmitted to a dual-dial pressure gauge calibrated in kilograms and pounds [1:14]. It is highly valued for its established test-retest, inter-rater, and intra-rater reliability [1:15].
- Electronic and Digital Dynamometers: Modern digital dynamometers utilize electronic force sensors or load cells (such as strain gauges) to capture and display grip strength [8:1][9:1]. These electronic devices are increasingly employed in clinical trials and large-scale normative studies due to their ease of data recording and precise digital readouts, showing high reliability and clinical diagnostic utility comparable to traditional hydraulic instruments [8:2][9:2].
¶ Preclinical Modeling and Variability Research
To better understand factors affecting dynamometric measurements, specialized research paradigms have investigated both animal performance models and non-traditional analytic frameworks:
- Rodent Performance Factors: Preclinical studies demonstrate that factors other than pure muscular strength, such as body weight changes, skeletal muscle mass loss, and sensory impairment, can significantly affect grip performance in rodent models [21]. Additionally, operational parameters such as the equipment sampling rate and system type play a critical role in data consistency, indicating that exact experimental conditions must be detailed to prevent confounding [21:1].
- Entropic Biomarkers: In human subjects, repetitive serial testing (e.g., 60 consecutive maximum grip trials) has been analyzed from an entropic perspective using Poincaré plots [18:1]. This research suggests that hand grip strength variability over serial trials acts as a complex biomechanical indicator that can successfully differentiate between young and older hand function patterns, providing an alternative entropic biomarker of neuromuscular aging [18:2].
¶ Device Comparability & Calibration
¶ Standard Hydraulic Dynamometers (The Jamar)
The hydraulic Jamar dynamometer is widely recognized as the clinical standard, showing excellent test-retest, inter-rater, and intra-rater reliability [1:16]. It relies on a sealed hydraulic system where force exerted on the handle is transmitted directly to a pressure gauge.
¶ Electronic & Digital Load-Cell Dynamometers
Standard clinical protocols utilize both hydraulic and validated electronic or digital handgrip dynamometers to measure muscle strength [8:3][9:3]. Digital models with electronic strain-gauge or load-cell sensors are increasingly utilized in clinical and research trials due to ease of recording, demonstrating high reliability and diagnostic accuracy [8:4][9:4].
¶ Calibration and Inter-Device Interchangeability
Due to the wide variety of equipment and protocols used across clinical studies, comparison of absolute grip strength measurements is highly challenging [1:17]. There is clear evidence that variations in device selection and testing approach directly affect the recorded values [1:18]. While standard clinical procedures emphasize maintaining device accuracy and checking calibration, research studies frequently fail to provide detailed protocols for device use or interchangeability [1:19]. For longitudinal patient tracking and research trials, clinicians must consistently utilize the exact same device brand, model, and testing protocol to ensure internal validity and avoid confounding the assessment of systemic muscle status [1:20].
¶ Protocols
¶ Measurement Variability and Protocol Setup
A comprehensive review of handgrip strength measurement highlights widespread protocol and equipment variation across clinical and epidemiological studies, noting that "standard conditions remain to be defined" [1:21]. Variations in body positioning, handle settings, rest intervals, and scoring methods can significantly affect the values obtained, which makes comparison between studies difficult and requires clinicians and researchers to apply identical methodology consistently within their own cohorts to ensure longitudinal validity [10:5][1:22].
The major areas of variation and established consensus findings from clinical literature include:
- Posture and Arm Position: Widespread variation exists regarding whether subjects are tested in a seated or standing position, and whether the arm is supported or completely unsupported [10:6][1:23]. There is clear evidence that these variations in positioning affect the recorded strength values, underscoring the necessity of using identical positioning across longitudinal trials [1:24].
- Handle Setting and Mechanics: The Jamar dynamometer features five adjustable handle positions to accommodate different hand sizes [22]. While most handle settings yield highly reliable measurements, comparative research demonstrates that position 1 (the narrowest setting) is significantly less reliable than positions 2 through 5 [22:1]. Therefore, handle adjustment should be performed under standard clinical guidance and kept consistent across successive tests [1:25].
- Laterality and Tested Hand: Clinical and research studies vary in laterality, with assessments measuring grip strength in either the dominant hand alone, the non-dominant hand, or both hands [1:26]. For instance, comparative reviews of hand dominance in specific neuropathies like Charcot-Marie-Tooth disease have evaluated both hands to analyze asymmetrical deficits, finding no significant difference in grip strength between the dominant and non-dominant side [23].
- Trial Repetitions and Rest Intervals: Standard clinical practice typically measures grip strength three times [10:7][1:27]. To prevent localized muscular fatigue, a rest interval must be provided between successive trials on the same hand, with studies describing rest periods ranging from 10 to 20 seconds up to 1 minute [10:8][1:28]. Additionally, scoping reviews indicate that verbal encouragement is typically not provided during clinical assessments to avoid introducing external bias and ensure standardized conditions [10:9].
- Scoring Methodology (Maximum vs. Mean):
- The Maximum Value: Many clinical consensus protocols and sarcopenia guidelines record and report the single strongest (maximum) score of three trials [10:10][1:29].
- The Mean Value: Other research paradigms utilize the mean value of multiple attempts [1:30].
- Reliability Comparison: While the maximum and mean values are not mathematically interchangeable, clinical trials comparing different methods—including the score of one trial, the mean of two trials, the mean of three trials, and the highest of three trials—demonstrate that there is no statistically significant difference in test-retest reliability among these methods, meaning no single scoring method can be recommended as more accurate [22:2]. Accordingly, the same method must be consistently utilized for a given individual's long-term evaluation [1:31].
¶ Evidence & Clinical Context
¶ Sarcopenia Case-Finding in Primary Care
Under the revised Asian Working Group for Sarcopenia (AWGS 2019) guidelines, handgrip strength serves as a primary tool for the screening and diagnostic pathway [5:7]:
- Step 1: Case-Finding: Initial screening is conducted in primary care using calf circumference or validated questionnaires (such as the SARC-F) [5:8].
- Step 2: Assessment of Possible Sarcopenia: If case-finding suggests risk, clinicians perform handgrip strength testing [5:9]. AWGS 2019 establishes clear diagnostic cut-off thresholds for low muscle strength: <28 kg for men and <18 kg for women [5:10]. Identifying handgrip strength below these thresholds is sufficient to diagnose "possible sarcopenia" in primary care settings and immediately initiate lifestyle interventions, physical rehabilitation, and nutritional education [5:11].
¶ Diagnostic Utility and Accuracy
In community-dwelling older adults and specialized cohorts, HGS provides essential diagnostic utility:
- Prognostic Power in COPD: Sarcopenia is common with advancing age and a number of long-term conditions, and is associated with adverse health outcomes including impaired mobility, increased morbidity, and mortality [24]. In rehabilitation patients with stable chronic obstructive pulmonary disease (COPD), sarcopenia diagnosed according to the revised EWGSOP2 criteria (incorporating low handgrip strength and low muscle mass) is a significant and independent predictor of both hospitalizations and long-term mortality [13:1].
- Systemic Physical Status: Low grip strength is a robust indicator of decreased physical status, loss of independence, and increased postoperative complications, serving as a key biomarker of general muscle health rather than a localized parameter [2:9][3:5][4:4].
¶ Environmental and Lifestyle Interactions
Neuromuscular function and sarcopenia progression are deeply influenced by lifestyle and rehabilitation factors:
- Sarcopenia Rehabilitation: Progressive resistance exercise is recognized as the first-line therapy to improve muscle strength and quality in patients with age-related sarcopenia [5:12][11:4]. Consensus guidelines recommend physical activity, focusing on progressive resistance (strength) training, as a first-line therapy for the management of sarcopenia [5:13][11:5][12:3].
- Nutritional Support: Muscle function and grip strength react early to nutritional deprivation, making HGS a highly responsive marker of nutritional status in clinical nutrition assessments [4:5]. Combining progressive resistance exercise with optimized protein and nutritional intake (such as consuming at least 1.2 g of protein/kg/d and incorporating amino acids like leucine) is recommended to support skeletal muscle synthesis and improve clinical outcomes [5:14].
¶ Cardiovascular Risk Markers
The relationship between muscle strength and cardiovascular parameters is highly nuanced:
- Cardiovascular Associations: In healthy populations, handgrip strength varies significantly by sex and age, and correlates with anthropometric factors such as height and weight [17:2].
- Systemic Physical Status: Low grip strength is a robust indicator of decreased physical status, loss of independence, and increased postoperative complications, serving as a key biomarker of general muscle health [2:10][3:6][4:6].
¶ The Hand-Squeezer Fallacy
Among health and longevity enthusiasts, handgrip strength is widely tracked as an indicator of physiological reserve and neuromuscular health [1:32]. However, this has led to a common clinical misunderstanding known as the hand-squeezer fallacy. Because prospective epidemiological studies show that lower handgrip strength is associated with an increased hazard of all-cause mortality [2:11][3:7][4:7], some consumers conclude that directly training grip strength with hand squeezers, grip rings, or localized forearm training is the primary means to address the health risks associated with low grip strength.
In reality, grip strength is a surrogate biomarker of systemic physiological reserve, general muscle quality, and overall physical fitness—it is not a direct causal driver of longevity [2:12][3:8]. To address the underlying physiological deficits associated with low grip strength, clinical guidelines recommend progressive resistance training, which has been shown to improve overall muscle strength, muscle quality, and physical performance [5:15][11:6][12:4]. Meta-analyses of clinical trials demonstrate that progressive resistance training interventions, such as elastic band training (typically performed for 40–60 minutes per session, more than three times per week for at least 12 weeks) or kettlebell exercises, significantly improve both handgrip strength and broader indices of muscle health [12:5].
¶ Safety & Contraindications
¶ Clinical Red Flags
Testers must recognize clinical red flags during handgrip testing that dictate immediate cessation of assessment and urgent medical evaluation:
- Unilateral Muscle Wasting: Significant asymmetrical atrophy of the hand or forearm musculature, which may indicate localized peripheral nerve pathology or cervical radiculopathy.
- Sudden Loss of Strength: Sudden, unexplained loss of hand or forearm strength without a history of localized trauma.
- Fasciculations: Visible, involuntary muscle twitching in the forearm or hand at rest.
- Sensory Loss: Numbness, paresthesia, or loss of sensation in the hand or fingers.
¶ Absolute Contraindications
Testing must not be performed under any of the following conditions:
- Acute Fractures: Unhealed bone fractures of the hand, wrist, or forearm.
- Unhealed Ruptures: Unhealed tendon, ligament, or joint capsular ruptures in the active hand or wrist.
- Unstable Cardiovascular Disease: Unstable angina, acute coronary syndrome, or severe aortic stenosis, where high-intensity isometric contractions can induce dangerous spikes in blood pressure or myocardial oxygen demand.
¶ Relative Contraindications
Proceed with caution, utilizing clinical judgement or submaximal assessments:
- Active Musculoskeletal Inflammation: Moderate-to-severe tendonitis (e.g., lateral epicondylitis), severe localized joint pain, or active hand/wrist flares.
- Inflammatory Arthritis: Patients with active rheumatoid arthritis or other localized joint pathologies of the hand and wrist. Elevated systemic inflammation (as indexed by C-reactive protein levels) and disease burden are independently associated with reduced grip strength, muscle dysfunction, and sarcopenia in these cohorts [6:3][7:1]. Active inflammation and joint pain can affect a patient's ability to generate maximal force. Because chronic inflammatory states (such as active rheumatoid arthritis) are associated with muscle wasting and reduced strength, clinical evaluations of muscle health in these populations should account for disease activity, inflammation markers like C-reactive protein (CRP), and corticosteroid use [6:4][7:2].
¶ Limitations and Potential Confounders
- Local Upper Extremity Pathology: A patient may record a lower HGS score due to localized upper-extremity conditions, such as peripheral neuropathies (including radial palsy or Charcot-Marie-Tooth disease) or localized joint diseases like rheumatoid arthritis, rather than systemic muscle wasting [20:2][6:5][23:1]. Consequently, when localized hand, wrist, or nerve pathology is present, HGS should be interpreted with caution and accompanied by a comprehensive physical assessment [20:3][6:6][1:33][23:2].
- Lower-Body Functional Disconnect: While handgrip strength is a robust indicator of upper-extremity muscle strength, it does not directly assess lower-extremity function or overall physical mobility. Systematic reviews and meta-analyses show that other physical fitness components, such as usual walking speed, are more strongly associated with frailty status and functional decline than grip strength alone [1:34][19:1]. Consequently, HGS should be interpreted as one component of a comprehensive physical assessment [1:35][19:2].
- Handle Setting Selection and Reliability: Standard clinical hydraulic and electronic dynamometers (such as the Jamar) utilize predefined, discrete handle settings to accommodate varying hand sizes [1:36][22:3]. Literature reviews indicate widespread variation in how handle settings are configured and documented in clinical trials, which can directly affect recorded grip strength values and limit comparability across cohorts [1:37]. Reliability studies evaluating all five handle positions of the Jamar dynamometer demonstrate that while all positions are within acceptable limits of reliability, position 1 (the narrowest setting) is significantly less reliable than positions 2 through 5 [22:4]. Since absolute handgrip strength is strongly correlated with anthropometric characteristics such as age, height, and weight [17:3], selecting an appropriate handle position and maintaining that exact setting across serial assessments is critical to ensuring measurement validity and avoiding artificial variations in force generation [1:38][22:5].
¶ Practical FAQ
- Incorporate Detailed Clinical Assessments: Perform detailed clinical examinations to investigate possible localized hand/wrist pathology or peripheral neuropathies (such as radial nerve palsy or inflammatory joint pathologies like rheumatoid arthritis) which could artificially suppress grip strength measurements [^1][^7][^29].
- Implement Tailored Physical Rehabilitation and Strength Training: Encourage tailored progressive resistance training (such as elastic band training or comprehensive multi-joint resistance training) as a first-line therapy to restore skeletal muscle function, mass, and overall physical performance [^18][^19][^23].
- Engage in Systemic Lifestyle Adaptations and Nutritional Support: Initiate nutritional interventions focused on optimized protein intake (at least 1.2 g of protein/kg/d) and general diet architecture to support overall metabolic and musculoskeletal health [^6][^18].
¶ References
Roberts HC, Denison HJ, Martin HJ, et al. A review of the measurement of grip strength in clinical and epidemiological studies: towards a standardised approach. Age and Ageing. 2011;40(4):423-429. https://pubmed.ncbi.nlm.nih.gov/21624928/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bohannon RW. Muscle strength: clinical and prognostic value of hand-grip dynamometry. Current Opinion in Clinical Nutrition and Metabolic Care. 2015;18(5):465-470. https://pubmed.ncbi.nlm.nih.gov/26147527/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bohannon RW. Hand-grip dynamometry predicts future outcomes in aging adults. Journal of Geriatric Physical Therapy. 2008;31(1):3-10. https://pubmed.ncbi.nlm.nih.gov/18489802/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Norman K, Stobäus N, Gonzalez MC. Hand grip strength: outcome predictor and marker of nutritional status. Clinical Nutrition. 2011;30(2):135-142. https://pubmed.ncbi.nlm.nih.gov/21035927/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Won CW. Management of Sarcopenia in Primary Care Settings. Korean Journal of Family Medicine. 2023;44(2):65-72. https://pubmed.ncbi.nlm.nih.gov/36966736/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Dietzel R, Wiegmann S, Borucki D, et al. Prevalence of sarcopenia in patients with rheumatoid arthritis using the revised EWGSOP2 and the FNIH definition. RMD Open. 2022;8(2):e002434. https://pubmed.ncbi.nlm.nih.gov/36180102/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Mochizuki T, Yano K, Ikari K, et al. Sarcopenia-associated factors in Japanese patients with rheumatoid arthritis: A cross-sectional study. Geriatrics & Gerontology International. 2019;19(9):907-912. https://pubmed.ncbi.nlm.nih.gov/31342647/ ↩︎ ↩︎ ↩︎
Polo-Ferrero L, Méndez-Sánchez R, Martín-Vallejo J, et al. Validity, reliability, and diagnostic accuracy of the InGrip digital dynamometer compared with the Jamar hydraulic model in older adults. European Geriatric Medicine. 2026;17(3):215-223. https://pubmed.ncbi.nlm.nih.gov/41746539/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sánchez-Aranda L, Fernández-Ortega J, Martín-Fuentes I, et al. Reliability and Concurrent Validity of a Low-Cost Handgrip Dynamometer: The Camry. The American Journal of Occupational Therapy. 2025;79(5). https://pubmed.ncbi.nlm.nih.gov/40829039/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Mehmet H, Yang AWH, Robinson SR. Measurement of hand grip strength in the elderly: A scoping review with recommendations. Journal of Bodywork and Movement Therapies. 2020;24(1):151-160. https://pubmed.ncbi.nlm.nih.gov/31987550/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zanker J, Sim M, Anderson K, et al. Consensus guidelines for sarcopenia prevention, diagnosis and management in Australia and New Zealand. Journal of Cachexia, Sarcopenia and Muscle. 2023;14(1):142-156. https://pubmed.ncbi.nlm.nih.gov/36349684/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zhao H, Cheng R, Song G. The Effect of Resistance Training on the Rehabilitation of Elderly Patients with Sarcopenia: A Meta-Analysis. International Journal of Environmental Research and Public Health. 2022;19(23):15491. https://pubmed.ncbi.nlm.nih.gov/36497565/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Dávalos-Yerovi V, Marco E, Sánchez-Rodríguez D, et al. Sarcopenia According to the Revised European Consensus on Definition and Diagnosis (EWGSOP2) Criteria Predicts Hospitalizations and Long-Term Mortality in Rehabilitation Patients With Stable Chronic Obstructive Pulmonary Disease. Journal of the American Medical Directors Association. 2019;20(8):1047-1049. https://pubmed.ncbi.nlm.nih.gov/31133471/ ↩︎ ↩︎
Jia X, Zhang L, Yang Z, et al. Impact of sarcopenic obesity on heart failure in people with type 2 diabetes and the role of metabolism and inflammation: A prospective cohort study. Diabetes & Metabolic Syndrome. 2024;18(5):103023. https://pubmed.ncbi.nlm.nih.gov/38749096/ ↩︎
Duggan E, Murphy CH, Knight SP, et al. Differential Associations Between Two Markers of Probable Sarcopenia and Continuous Orthostatic Hemodynamics in The Irish Longitudinal Study on Ageing. The Journals of Gerontology, Series A: Biological Sciences and Medical Sciences. 2023;78(8):1456-1463. https://pubmed.ncbi.nlm.nih.gov/36480700/ ↩︎
Soysal P, Kocyigit SE, Dokuzlar O, et al. Relationship between sarcopenia and orthostatic hypotension. Age and Ageing. 2020;49(6):1045-1052. https://pubmed.ncbi.nlm.nih.gov/32614946/ ↩︎
Wang YC, Bohannon RW, Li X. Hand-Grip Strength: Normative Reference Values and Equations for Individuals 18 to 85 Years of Age Residing in the United States. The Journal of Orthopaedic and Sports Physical Therapy. 2018;48(9):685-693. https://pubmed.ncbi.nlm.nih.gov/29792107/ ↩︎ ↩︎ ↩︎ ↩︎
Iconaru EI, Ciucurel C. Hand grip strength variability during serial testing as an entropic biomarker of aging: a Poincaré plot analysis. BMC Geriatrics. 2020;20(1):15. https://pubmed.ncbi.nlm.nih.gov/31931730/ ↩︎ ↩︎ ↩︎
Navarrete-Villanueva D, Gómez-Cabello A, Marín-Puyalto J, et al. Frailty and Physical Fitness in Elderly People: A Systematic Review and Meta-analysis. Sports Medicine. 2021;51(1):143-157. https://pubmed.ncbi.nlm.nih.gov/33201455/ ↩︎ ↩︎ ↩︎
Paternostro-Sluga T, Grim-Stieger M, Posch M, et al. Reliability and validity of the Medical Research Council (MRC) scale and a modified scale for testing muscle strength in patients with radial palsy. Journal of Rehabilitation Medicine. 2008;40(8):665-671. https://pubmed.ncbi.nlm.nih.gov/19020701/ ↩︎ ↩︎ ↩︎ ↩︎
Maurissen JP, Marable BR, Andrus AK. Factors affecting grip strength testing. Neurotoxicology and Teratology. 2003;25(5):543-553. https://pubmed.ncbi.nlm.nih.gov/12972067/ ↩︎ ↩︎
Hamilton A, Balnave R, Adams R. Grip strength testing reliability. Journal of Hand Therapy. 1994;7(3):163-170. https://pubmed.ncbi.nlm.nih.gov/7951708/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Roberts-Clarke D, Fornusek C, Fiatarone Singh MA. Examining hand dominance using dynamometric grip strength testing as evidence for overwork weakness in Charcot-Marie-Tooth disease: a systematic review and meta-analysis. International Journal of Rehabilitation Research. 2016;39(3):191-197. https://pubmed.ncbi.nlm.nih.gov/27177353/ ↩︎ ↩︎ ↩︎
Sayer AA, Cruz-Jentoft A. Sarcopenia definition, diagnosis and treatment: consensus is growing. Age and Ageing. 2022;51(10):afac220. https://pubmed.ncbi.nlm.nih.gov/36273495/ ↩︎