¶ Hidradenitis Suppurativa
| Indication | Moderate-to-Severe Hidradenitis Suppurativa (FDA-approved & off-label) |
| Access | Rx (Biologics / Oral Systemics) / OTC (Wound Care) |
| Dosing Sched | Varies (e.g., Weekly Biologics, Daily Antibiotics) |
| Safety Profile | Moderate (High risk of infection, pre-screening mandatory) |
| Key Marker | IHS4 Score, Pain Severity, DLQI, Infectious screening |
| Est. Cost | $1,000 - $5,000/month (biologics without insurance) |
Hidradenitis suppurativa (HS), historically referred to as acne inversa, is a chronic, debilitating, follicular-occlusive inflammatory skin disease characterized by recurrent, painful nodules, abscesses, and deep-seated draining tunnels (sinus tracts) primarily affecting intertriginous regions [1][2], frequently leading to severe scarring and tissue destruction. Managing HS requires a rapid transition from sequential antibiotic monotherapy to structured, multimodal strategies combining early biologic therapy and precise surgical interventions [3][4], alongside supportive medical nutrition therapies [5], to prevent permanent physiological disfigurement [3:1][4:1].
¶ At a Glance
¶ Key Points
- Systemic Pathophysiology: HS is not an infectious disease, nor is it a disorder of apocrine glands; it is a chronic inflammatory disorder of the hair follicles characterized by follicular occlusion, follicular rupture, and systemic immune dysregulation [6][2:1].
- "Hit Hard and Early" Paradigm: Current clinical consensus heavily discourages prolonged, sequential antibiotic monotherapies, favoring early escalation to targeted biologic therapies (e.g., TNF-alpha and IL-17 inhibitors) in moderate-to-severe cases to prevent irreversible scarring and sinus tract formation [7][4:2].
- Multimodal Integration: Best clinical outcomes are achieved when systemic immunomodulatory treatment is strategically integrated with tailored surgical procedures (such as deroofing and wide local excision) and proactive screening for metabolic and inflammatory comorbidities [8][3:2].
¶ What People Use It For
- Main Goals: Direct reduction of the systemic inflammatory load, pain mitigation, resolution of active draining tunnels, prevention of permanent hypertrophic scarring, and restoration of the Dermatology Life Quality Index (DLQI) [9][3:3].
- Evidence Quality: High certainty for TNF-alpha inhibitors (adalimumab, infliximab) and IL-17A inhibitors (secukinumab); moderate-to-high certainty for surgical interventions, specialized systemic antibiotic regimens, and medical nutrition therapy [1:1][10][5:1][6:1].
¶ Recognition & Clinical Presentation
Recognizing hidradenitis suppurativa early is critical, yet patients routinely experience a 7-to-10 year delay in diagnosis [11][7:1]. General practitioners and emergency clinicians frequently misdiagnose early lesions as simple furuncles (boils), isolated abscesses, or superficial bacterial skin infections, leading to repeated, ineffective incision and drainage (I&D) and prolonged, unnecessary antibiotic courses [11:1].
The hallmark clinical presentation of HS is defined by three diagnostic criteria: lesion type, anatomical location, and chronicity (recurrence) [8:1]:
- Lesion Types: Recurrent, exquisitely painful, deep-seated subcutaneous nodules and sterile abscesses, double-ended comedones ("tombstone comedones"), and actively draining sinus tracts (epithelialized tunnels) that discharge a malodorous, serosanguinous fluid [8:2][11:2][2:2].
- Anatomical Locations: Intertriginous areas rich in apocrine sweat glands and terminal hair follicles, primarily the axillae, inguinal creases, perineum, perianal region, inframammary folds, and gluteal cleft [8:3][11:3].
- Chronicity: Lesions must recur at least twice within a 6-month period, although most patients present with a continuous, fluctuating course of flares [8:4].
¶ Access Barriers & Healthcare Burden
Severe access barriers further compound the diagnostic delay. There is a critical lack of specialized dermatologists and dermatosurgeons familiar with modern HS therapeutic algorithms, forcing many patients to rely on emergency departments for acute, non-resolving flares [12][11:4]. Furthermore, the high financial cost of targeted biologics and systemic therapies, coupled with high healthcare resource utilization, creates significant socioeconomic and management burdens [13].
¶ Staging & Severity Assessment
To guide therapeutic decision-making and measure clinical response, several validated static and dynamic staging systems are utilized in clinical practice.
¶ Hurley Staging System
The Hurley staging system is the traditional and most widely used clinical classification. It is a static classification based on the presence or absence of sinus tracts and scarring, making it useful for establishing initial surgical candidacy but insensitive to dynamic inflammatory changes [8:5][6:2]:
- Hurley Stage I: Single or multiple isolated abscesses, without sinus tracts or cicatrization (scarring) [8:6][2:3].
- Hurley Stage II: Recurrent, widely separated abscesses or nodules, accompanied by sinus tracts and localized scarring [8:7][2:4].
- Hurley Stage III: Diffuse or near-diffuse involvement of an entire anatomical region, characterized by multiple interconnected sinus tracts, extensive abscess networks, and dense hypertrophic scarring [8:8][2:5].
¶ International Hidradenitis Suppurativa Severity Score System (IHS4)
The IHS4 is a validated, dynamic scoring tool developed by international experts to measure disease severity and track treatment response over time [8:9][14][15]. The score is calculated using the following formula [14:1][15:1]:
Interpretation according to S2k guidelines [14:2][15:2]:
- Mild HS: IHS4 score
- Moderate HS: IHS4 score of
- Severe HS: IHS4 score
¶ The Sartorius Severity Score
The Sartorius score is a continuous severity scale utilized primarily in clinical trials. It provides a detailed, region-by-region assessment of disease severity by tracking lesion counts and disease extent, making it highly sensitive to incremental therapeutic changes [6:3][16].
¶ Sonographic Staging (Ultrasound)
The integration of high-frequency ultrasound (US) in HS management has reached strong international consensus [17]. Standard clinical examinations frequently underestimate the depth, extent, and presence of subclinical sinus tracts and abscesses.
- Clinical Utility: High-frequency ultrasound (typically ) is indicated for the definitive staging of subclinical lesions, monitoring active sub-dermal inflammation via Doppler imaging, distinguishing between fluid-filled abscesses and epithelialized tunnels, and mapping margins prior to surgical intervention [17:1].
- The SOS-HS System: The Sonographic Hidradenitis Suppurativa Severity (SOS-HS) staging system matches ultrasound findings with Hurley-like clinical stages to provide a three-dimensional view of tissue destruction, preventing incomplete surgical excisions [17:2].
¶ Outcome Measures for Treatment Response
In clinical practice, standardized clinician- and patient-reported outcome measures should be applied at regular intervals to evaluate response to immunomodulatory and surgical therapies.
- Clinician-Reported Measure: HS Investigator Global Assessment (HS-IGA) is recommended, and Hidradenitis Suppurativa Clinical Response (HiSCR) is a key clinical endpoint studied and validated in trials [9:1][16:1]. HiSCR is defined as a reduction in inflammatory lesion count (sum of abscesses and inflammatory nodules) with no increase in the number of abscesses or draining tunnels relative to baseline [16:2][18].
- Patient-Reported Measure: HS Quality of Life (HS-QoL) score is recommended to assess patient-reported disease impact [9:2].
- Preferred Interval: By consensus (HiSTORIC Statement), clinicians and patient research partners prefer evaluating these outcome measures at regular intervals in clinical practice to guide shared treatment decision-making [9:3].
¶ Evidence Summary Table (Human Outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Sartorius / IHS4 Score Reduction (TNF-alpha Inhibitors) | High | High | 2 RCTs | Adalimumab weekly leads to significant, sustained reductions in IHS4 and Sartorius scores at 12–36 weeks [7:2][16:3][15:3] | |
| Sartorius / IHS4 Score Reduction (IL-17A Inhibitors) | High | High | 2 RCTs | Secukinumab subcutaneous administration shows high rates of HiSCR at 16–52 weeks [10:1][7:3][14:3] | |
| Pain Severity Reduction (Biologics & Surgery) | Moderate | High | Multiple RCTs | Combined perioperative biologics and wide excision/deroofing yield substantial reduction in patient-reported pain [3:4][19] | |
| Quality of Life (DLQI Improvement) | High | High | Multiple RCTs | Clinically meaningful DLQI score improvement (reduction in impairment) within 12 weeks of starting targeted biologic therapy [9:4][3:5][7:4] | |
| Recurrence Rate after Deroofing (Treated Site) | High | Moderate | Cohorts | Site-specific recurrence rate is low compared to the high recurrence rate typical of standard incision and drainage [3:6][14:4] | |
| Acute Flare Resolution (Systemic Antibiotics) | Moderate | Moderate | Cohorts / RCTs | Systemic combination antibiotics (e.g., clindamycin and rifampicin) for structured courses; high initial response but high post-therapy recurrence [1:2][4:3][15:4] |
- Effect: Number of arrows (1-3) indicates magnitude. Direction: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Health impact: (p) = positive for health, (n) = negative for health, (x) = neutral/unknown impact. Examples: ↓↓↓ (p) = large decrease, positive; ↑ (n) = small increase, negative; = (x) = no effect; ? = unclear.
- Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- Trials: Number of RCTs or total trials informing this outcome (shows evidence depth at a glance)
- REQUIRED: You MUST include a citation key (e.g.
[^1]) in the "Notes" column for every single row. If you claim a result, you must link the specific Meta-Analysis or Key RCT that proves it.
¶ Pathophysiology & Etiology
Hidradenitis suppurativa is an immunologically driven, chronic, and recurrent inflammatory skin disease [11:5][2:6].
¶ Non-Stigmatizing Etiology
HS is not infectious, contagious, or caused by poor personal hygiene, dirty skin, or lack of cleanliness. Framing the disease as a "hygiene issue" is clinically inaccurate, highly stigmatizing, and severely exacerbates the psychological burden on patients [2:7].
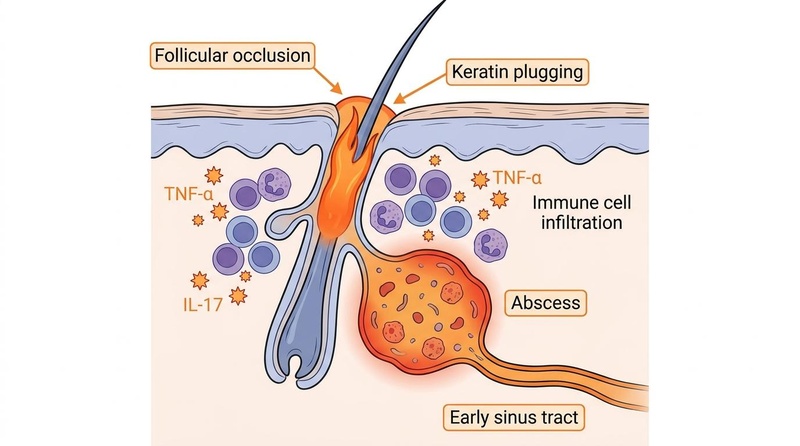
The pathogenesis is rooted in a primary follicular-occlusive defect, followed by a severe, autoinflammatory dermal reaction [4:4][2:8]. The pathophysiological sequence consists of four distinct stages:
- Follicular Hyperkeratosis & Occlusion: Hyperkeratotic proliferation of the follicular infundibulum leads to keratin plugging and progressive dilation of the hair follicle [20][2:9].
- Follicular Rupture: As the occluded follicle expands under mechanical stress, friction, and cellular buildup, it ruptures, spilling keratin, sebum, hair fragments, and commensal bacterial antigens into the surrounding dermis [11:6][2:10].
- Acute and Chronic Inflammation: The presence of these foreign antigens in the dermis triggers a massive, neutrophil-rich inflammatory response, leading to abscess formation [3:7][2:11]. This is mediated by elevated local and systemic expression of tumor necrosis factor-alpha (TNF-), interleukin-1 beta (IL-1), interleukin-17 (IL-17), and interleukin-23 (IL-23) [7:5][2:12].
- Sinus Tract / Tunnel Formation: Chronic, recurrent rupture and localized tissue destruction prompt epithelial cells from the epidermis or outer root sheath to migrate into the deep dermis. This leads to the formation of epithelial-lined, draining sinus tracts (tunnels) that connect subcutaneous abscesses to the skin surface, accompanied by severe, hypertrophic scarring [11:7][3:8].
¶ Mechanistic Risk Factors (Non-Stigmatizing Framing)
Two dominant environmental and physical factors are strongly associated with HS susceptibility and disease flares. They are presented here strictly as biological and biomechanical mechanisms rather than lifestyle choices:
- Smoking (Nicotine Exposure): Nicotine is highly associated with follicular occlusion and disease severity. It upregulates infundibular hyperkeratosis, promoting follicular plugging and local inflammatory response within the pilosebaceous unit, thereby creating a highly susceptible follicular microenvironment [8:10][2:13].
- Elevated Body Mass Index (BMI): Obesity contributes to disease progression and severity through biomechanical friction in intertriginous skin folds, which triggers physical rupture of distended hair follicles, and through local microclimate alteration (sweat retention and skin maceration) that promotes follicular occlusion and intensifies local and systemic inflammation [8:11][2:14].
¶ Clinical Decision-Making Matrix (Stage-Driven Action Plan)
The following clinical decision-making matrix maps a patient's severity profile directly to integrated medical, surgical, and lifestyle interventions.
| Hurley Stage | IHS4 Score | First-Line Medical Therapy | Local / Surgical Procedures | Lifestyle & Supportive Care |
|---|---|---|---|---|
| Stage I | (Mild) | • Topical Clindamycin [8:12][14:5][15:5] • Hormonal therapy (e.g., spironolactone) for select female patients [1:3][8:13] |
• Localized deroofing or excision of single, chronic lesions [3:9][15:6] | • Smoking cessation counseling [8:14][4:5] • Weight management support [8:15][4:6] • Non-adherent dressings [8:16] • Mediterranean Diet (MedDiet) [5:2] |
| Stage II | (Moderate) | • Combination oral Clindamycin and Rifampicin for a structured multi-week course [1:4][4:7][15:7] • If failing antibiotics, escalate immediately to approved biologics (e.g., Adalimumab or Secukinumab) [7:6][4:8] |
• Deroofing of persistent draining tunnels [3:10][15:8] • Ultrasound-guided needle aspiration [17:3] |
• Medical Nutrition Therapy (VLEKT) for flare control [5:3] • Antiseptic cleansing (e.g., Chlorhexidine) [8:17] • NSAIDs for pain control [8:18] |
| Stage III | (Severe) | • Approved subcutaneous biologics (e.g., Adalimumab or Secukinumab) [1:5][7:7][16:4] • Consider Bimekizumab or small molecules (JAK inhibitors) for refractory disease [7:8][21] |
• Radical Wide Local Excision (WLE) [3:11][15:9] • Reconstruction with skin grafts or local tissue flaps [3:12][15:10] |
• Standardized inpatient care protocol [12:1] • Complex, non-adherent wound management • Structured pain management plans [8:19] |
¶ Medical & Surgical Therapeutic Ladder
A structured progression along the therapeutic ladder, combining systemic immunomodulators and surgical interventions, is required to prevent irreversible tissue damage [3:13][4:9].
¶ Topical Interventions
- Topical Clindamycin: Formulated as a gel, solution, or lotion. It has clinical trial and guideline data supporting its use in mild disease, functioning as both an antibacterial and mild anti-inflammatory agent [8:20][14:6][15:11].
- Antiseptic Wash: Used during bathing in affected regions (such as chlorhexidine gluconate) to help reduce surface microbial colonization and manage odor [8:21][14:7][15:12].
¶ Oral & Systemic Therapies
- Systemic Tetracyclines: Oral tetracyclines may be used as systemic therapy in mild-to-moderate presentations where topical therapy is insufficient [1:6][14:8][15:13].
- Combination Clindamycin and Rifampicin: Historically utilized as systemic combination antibiotic therapy in moderate-to-severe disease [1:7][4:10][15:14].
- Clinical Warning: Prolonged or sequential antibiotic monotherapy is highly discouraged, as it fails to address the underlying immunological drivers, has high recurrence rates upon cessation, and rapidly induces antimicrobial resistance [4:11]. Systemic antibiotic combinations should be used strictly as a short-term bridging therapy prior to biologic initiation or surgery [4:12].
¶ Targeted Biologics & Small Molecules
When patients present with moderate-to-severe disease (IHS4 ), multiple affected regions, frequent flares ( in 12 weeks), or specific severe phenotypes (such as anogenital involvement), immediate escalation to targeted therapy is indicated [7:9][4:13]:
- Adalimumab (TNF-alpha Inhibitor): The first FDA-approved biologic for HS. High-level evidence from Phase 3 trials (PIONEER I and II) supports its efficacy when administered weekly [7:10][16:5]. Maintenance of weekly dosing is critical, as bi-weekly dosing is associated with a significant loss of clinical response [16:6].
- Infliximab (TNF-alpha Inhibitor): Administered via intravenous infusion, it is utilized as an off-label therapy for severe, refractory cases [1:8][14:9][15:15].
- Secukinumab (IL-17A Inhibitor): Approved for moderate-to-severe HS, administered subcutaneously. High-level evidence demonstrates robust, long-term efficacy in reducing inflammatory nodules and abscesses [7:11][14:10].
- Bimekizumab (IL-17A/F Inhibitor): An emerging biologic that selectively neutralizes both IL-17A and IL-17F, demonstrating rapid and profound clinical response rates [7:12][21:1].
- Small Molecules (JAK Inhibitors): Oral Janus kinase (JAK) inhibitors and interleukin-23 (IL-23) inhibitors are utilized off-label for patients who fail multiple anti-TNF and anti-IL-17 therapies [1:9][7:13][14:11][15:16].
¶ Surgical & Procedural Interventions
Surgery is not a treatment of last resort; it is a mechanical solution to a mechanical problem (fibrotic tunnels and epithelialized sinus tracts) that cannot be resolved by medical therapy alone [3:14][4:14].
- Deroofing (Unroofing / Marsupialization): A tissue-saving, outpatient surgical technique performed under local anesthesia, ideal for localized, recurrent sinus tracts (Hurley Stage I or II) [3:15]. The surgeon removes the superficial wall (roof) and leaves the epithelialized floor of the tunnel intact [3:16][15:17]. The wound is curetted and left to heal by secondary intention, resulting in low recurrence rates at the treated site and minimal tissue loss [1:10][3:17].
- Wide Local Excision (WLE): Indicated for diffuse, chronic disease (Hurley Stage III) characterized by extensive fibrosis and interconnected sinus tracts [3:18]. The surgeon excises the entire hair-bearing and inflamed area, extending margins beyond the clinically apparent borders of inflammation [3:19][15:18]. The resulting defect is left to heal by secondary intention, closed with skin grafts, or reconstructed using local tissue flaps [3:20][15:19].
¶ Recurrence Risks & Perioperative Biologic Management
Local recurrence at the surgical site is relatively low for radical wide local excision and moderate for deroofing [3:21]. However, regional or systemic recurrence remains high if underlying systemic inflammation is uncontrolled [3:22].
To optimize outcomes, systemic biologics (such as adalimumab) should be maintained continuously throughout the perioperative period. Consensus guidelines and clinical trials (such as the SHARPS trial) confirm that continuing biologic therapy perioperatively reduces the inflammatory load, improves healing rates, and does not increase the risk of postoperative infectious complications [1:11][3:23][19:1].
¶ Wound Care & Pain Management
¶ Safe Wound Care Practices
Proper wound care in HS is essential to manage exudate, control odor, and protect the skin barrier without causing mechanical trauma to highly friable, inflamed tissue [8:22]:
- Non-Adherent Dressings: Adhesive dressings should be avoided on fragile skin. Instead, non-adherent dressings, such as silicone-bordered or polyurethane foam dressings, are recommended to manage drainage without causing skin trauma [8:23].
- Gentle Cleansing: Wounds should be cleansed gently with saline or water. Harsh over-the-counter soaps should be avoided [8:24].
- Antiseptic Washes: Daily washing with antiseptic cleansers (such as chlorhexidine gluconate) reduces surface bacterial colonization and manages wound odor [8:25].
¶ Systemic & Local Pain Control
HS is associated with some of the highest pain scores in dermatology, severely impairing physical mobility and quality of life [9:5][3:24].
- Systemic Analgesics: Pain management is critical. Non-steroidal anti-inflammatory drugs (NSAIDs) are first-line systemic agents to target the inflammatory component of the pain [8:26].
- Topical Analgesics: Topical local anesthetics can provide temporary, localized relief during acute flares [1:12][14:12][15:20].
- Intralesional Corticosteroids: Clinicians may perform intralesional corticosteroid injections directly into acute, painful inflammatory nodules to induce rapid regression and pain relief [1:13][14:13][15:21].
¶ Rejection of Unsafe Drainage & Self-Lancing
Strictly warn patients against self-lancing, squeezing, or manual drainage of lesions. Clinical incision and drainage (I&D) or needle aspiration of HS lesions is associated with high recurrence rates. Furthermore, manual squeezing or self-lancing causes severe tissue damage, forces inflammatory debris deeper into the dermis, triggers secondary inflammation, and worsens permanent scarring [3:25][4:15].
¶ Lifestyle, Diet & Medical Nutrition Therapy
Modulating systemic metabolic and inflammatory pathways can help reduce the severity of HS flares [5:4][8:27].
¶ Medical Nutrition Therapy (MNT)
There is emerging clinical evidence highlighting the role of diet in modulating HS severity, as the disease is driven by chronic inflammation and oxidative stress [5:5][8:28].
- Very Low-Energy Ketogenic Therapy (VLEKT): High-level clinical consensus supports VLEKT as a promising short-term intervention for moderate-to-severe HS, demonstrating rapid improvements in disease severity [5:6].
- The Mediterranean Diet (MedDiet): For long-term dietary management, the MedDiet is recommended due to its anti-inflammatory and immunomodulatory effects, utilizing food patterns rich in antioxidants, polyphenols, and unsaturated fatty acids [5:7].
- Specific Nutrients: Supplementation with specific nutrients, including omega-3 fatty acids, probiotics, and micronutrients, may further support disease management [5:8].
¶ Smoking Cessation & Weight Management
- Smoking Cessation: Cigarette smoking is strongly associated with HS susceptibility and disease progression. Nicotine and other components can stimulate follicular hyperactivity and drive local inflammatory pathways, making smoking cessation a cornerstone of management [8:29][4:16].
- Weight Reduction: Elevated body mass index (BMI) is associated with increased mechanical friction in skin folds and systemic subclinical inflammation. Sustained weight reduction is associated with significant improvements in overall disease burden [8:30][4:17].
¶ Safety, Screening & Special Populations
¶ Infectious Disease Screening Prior to Immunomodulatory Therapy
Before initiating any biologic or systemic immunosuppressant therapy, clinician consensus guidelines from the Asia-Pacific Hidradenitis Suppurativa Foundation mandate a standardized infectious disease screening protocol [22]:
- Mandatory Screening Panel:
- Tuberculosis (TB): Interferon-Gamma Release Assay (IGRA) or Purified Protein Derivative (PPD) skin test to rule out latent TB infection prior to starting biologics [10:2][22:1].
- Hepatitis B Virus (HBV): Serological screening prior to therapy [10:3][22:2].
- Hepatitis C Virus (HCV): Serological screening prior to therapy [10:4][22:3].
- Endemic and Occupational Considerations: Pre-treatment infectious disease screening should include patient- and location-specific considerations for endemic local diseases (such as strongyloidiasis, leishmaniasis, or leprosy) or high-risk exposures [22:4].
¶ Special Patient Populations
The North American guidelines establish distinct, evidence-based recommendations for specific patient cohorts using the GRADE system [10:5]:
- Pregnancy & Breastfeeding: Guideline consensus emphasizes the importance of managing HS in pregnant and breastfeeding patients, taking into account specific population-level considerations for safety and treatment selection [10:6][4:18].
- Malignancy: Approved biologics should be used with appropriate caution in patients with active or recent malignancy [10:7].
- Pediatrics: Pediatric HS patients require unique considerations in their management, with guidelines supporting appropriate early intervention based on family history and disease progression [10:8][7:14].
¶ Systemic Comorbidities & Mental Health
HS is a systemic disease that extends far beyond the skin. Proactive screening for several major associated comorbidities is mandatory [8:31][7:15]:
- Metabolic & Cardiovascular Comorbidities: Patients have a significantly higher prevalence of metabolic syndrome, insulin resistance, type 2 diabetes, dyslipidemia, and arterial stiffness, culminating in a highly elevated risk of major adverse cardiovascular events (MACE) [8:32][2:15].
- Inflammatory Comorbidities: High associations exist with inflammatory bowel disease (such as Crohn's disease) and inflammatory arthritis/spondyloarthropathies [2:16].
- Mental Health Burden: Due to chronic pain, physical disfigurement, malodorous drainage, and social isolation, HS patients suffer from exceptionally high rates of severe anxiety, clinical depression, suicidal ideation, and profound DLQI impairment [9:6][3:26].
¶ Complications & Inpatient Care Thresholds
While typical HS flares present with painful, fluctuating, localized swelling and drainage, patients are at risk for severe, life-threatening complications that require urgent clinical evaluation and potentially inpatient hospitalization [12:2].
According to international consensus guidelines for inpatient management, hospitalization and specialized supportive care are indicated for patients presenting with severe HS or acute inflammatory flares that cannot be managed in an outpatient setting [12:3]. Inpatient management protocols emphasize:
- Pain Management: Severe, intractable pain requiring intravenous analgesia or structured pain control plans.
- Systemic Inflammatory Monitoring: Close monitoring of patients with severe disease for signs of systemic involvement or secondary severe soft-tissue infections that require intravenous antibiotic therapy.
- Wound Care Integration: Comprehensive, non-adherent wound dressing and local care for diffuse, highly exudative lesions.
¶ FAQs
What is the difference between hidradenitis suppurativa and a standard boil or infection?
Standard furuncles or boils are isolated, acute infections that typically resolve with local care. In contrast, hidradenitis suppurativa is a chronic, non-infectious, immunologically driven disease. It is characterized by recurrent, deep-seated, painful lesions in intertriginous areas that can progress to form subdermal tunnels (sinus tracts) and scars [11:8][2:17].
Why is prolonged antibiotic monotherapy discouraged in HS management?
Prolonged or sequential antibiotic monotherapy is discouraged because it does not address the underlying immunological drivers, has high recurrence rates once discontinued, and increases the risk of antimicrobial resistance [4:19]. Systemic antibiotics should be reserved for short, structured courses to reduce the acute inflammatory load and bridge patients to targeted biologics or surgical interventions [1:14][4:20].
Is it safe to undergo surgery while taking a biologic medication like adalimumab?
Yes. Clinical guidelines and clinical trials (such as the SHARPS trial) demonstrate that maintaining biologic therapy throughout the perioperative period is safe and beneficial [3:27][19:2]. Continuing the biologic reduces local and systemic inflammatory loads, improves healing rates, and does not increase the risk of postoperative wound infections [3:28][19:3].
How does ultrasound imaging change the treatment plan for HS?
High-frequency ultrasound reveals subclinical disease that is invisible during standard clinical examinations, such as deep-seated abscesses and networks of subdermal tunnels [17:4]. Clinicians use ultrasound to accurately stage patients, monitor active inflammation, and map the exact margins of sinus tracts before surgical excision [17:5].
How does diet affect HS severity?
Emerging clinical evidence shows that metabolic and inflammatory status can modulate HS severity [5:9]. Short-term Very Low-Energy Ketogenic Therapy (VLEKT) has shown promise in rapidly improving disease severity [5:10], while the Mediterranean Diet (MedDiet) is recommended for long-term management due to its anti-inflammatory effects [5:11].
Is self-lancing ever appropriate for a painful HS flare?
No. Self-lancing or manual squeezing of HS lesions is strictly contraindicated [3:29][4:21]. It causes mechanical tissue damage, forces inflammatory debris deeper into the dermis, increases the risk of serious bacterial infections, promotes the development of draining sinus tracts, and accelerates scarring [3:30][4:22]. Painful lesions should instead be evaluated by a healthcare professional [1:15][8:33][14:14].
¶ References
Kolios AGA, Laffitte E, Mainetti C, et al. Swiss S1 Guidelines for the Management of Hidradenitis Suppurativa. Dermatology. 2026. https://pubmed.ncbi.nlm.nih.gov/41712494/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sabat R, Alavi A, Wolk K, et al. Hidradenitis suppurativa. Lancet. 2025. https://pubmed.ncbi.nlm.nih.gov/39862870/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Offidani A, Marzano AV, Peris K, et al. Guidelines How to Integrate Surgery and Targeted Therapy with Biologics for the Treatment of Hidradenitis Suppurativa: Delphi Consensus Statements from an Italian Expert Panel. Dermatology. 2024. https://pubmed.ncbi.nlm.nih.gov/39004081/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Frew J, Smith A, Penas PF, et al. Australasian hidradenitis suppurativa management guidelines. Australas J Dermatol. 2025. https://pubmed.ncbi.nlm.nih.gov/39578415/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Barrea L, Verde L, Annunziata G, et al. Medical Nutrition Therapy in Dermatological Diseases. Curr Obes Rep. 2025. https://pubmed.ncbi.nlm.nih.gov/40358870/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Hendricks AJ, Hsiao JL, Lowes MA, et al. A Comparison of International Management Guidelines for Hidradenitis Suppurativa. Dermatology. 2021. https://pubmed.ncbi.nlm.nih.gov/31645040/ ↩︎ ↩︎ ↩︎ ↩︎
Nikolakis G, Alpsoy E, Anzengruber F, et al. Delphi consensus: First-line use of biologics and small molecules in hidradenitis suppurativa. JEADV. 2026. https://pubmed.ncbi.nlm.nih.gov/41580305/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Ameen A, Albreiki F, Alnaeem A, et al. Management of Hidradenitis Suppurativa in the United Arab Emirates (UAE): A Consensus Statement from the Emirates Dermatology Society. Dermatol Ther (Heidelb). 2026. https://pubmed.ncbi.nlm.nih.gov/41701451/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Mastacouris N, Tannenbaum R, Strunk A, et al. Outcome Measures for the Evaluation of Treatment Response in Hidradenitis Suppurativa for Clinical Practice: A HiSTORIC Consensus Statement. JAMA Dermatol. 2023. https://pubmed.ncbi.nlm.nih.gov/37755725/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Alhusayen R, Dienes S, Lam M, et al. North American clinical practice guidelines for the medical management of hidradenitis suppurativa in special patient populations. J Am Acad Dermatol. 2025. https://pubmed.ncbi.nlm.nih.gov/39725212/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Marzano AV, Magnoni C, Micali G, et al. Improving hidradenitis suppurativa management: consensus statements from physicians and patients' perspectives. Arch Dermatol Res. 2024. https://pubmed.ncbi.nlm.nih.gov/39180694/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Needham M, Pichardo R, Alavi A, et al. Inpatient Management of Hidradenitis Suppurativa: A Delphi Consensus Study. Cutis. 2024. https://pubmed.ncbi.nlm.nih.gov/39082985/ ↩︎ ↩︎ ↩︎ ↩︎
Garg A, Geissbühler Y, Houchen E, et al. Disease Burden and Treatment Patterns Among US Patients with Hidradenitis Suppurativa: A Retrospective Cohort Study. Am J Clin Dermatol. 2023. https://pubmed.ncbi.nlm.nih.gov/37378875/ ↩︎
Zouboulis CC, Bechara FG, Fritz K, et al. S2k guideline for the treatment of hidradenitis suppurativa / acne inversa - Short version. J Dtsch Dermatol Ges. 2024. https://pubmed.ncbi.nlm.nih.gov/38770982/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zouboulis CC, Bechara FG, Benhadou F, et al. European S2k guidelines for hidradenitis suppurativa/acne inversa part 2: Treatment. JEADV. 2025. https://pubmed.ncbi.nlm.nih.gov/39699926/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kimball AB, Okun MM, Williams DA, et al. Two Phase 3 Trials of Adalimumab for Hidradenitis Suppurativa. N Engl J Med. 2016. https://pubmed.ncbi.nlm.nih.gov/27518661/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wortsman X, Alfageme F, Dini V, et al. International consensus statement on the use of ultrasound in hidradenitis suppurativa. JEADV. 2026. https://pubmed.ncbi.nlm.nih.gov/39963815/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kimball AB, Sobell JM, Zouboulis CC, et al. HiSCR (Hidradenitis Suppurativa Clinical Response): a novel clinical endpoint to evaluate therapeutic outcomes in patients with hidradenitis suppurativa from the placebo-controlled portion of a phase 2 adalimumab study. JEADV. 2016. https://pubmed.ncbi.nlm.nih.gov/26201313/ ↩︎
Bechara FG, Podda M, Prens EP, et al. Efficacy and Safety of Adalimumab in Conjunction With Surgery in Moderate to Severe Hidradenitis Suppurativa: The SHARPS Randomized Clinical Trial. JAMA Surg. 2021. https://pubmed.ncbi.nlm.nih.gov/34406349/ ↩︎ ↩︎ ↩︎ ↩︎
Litaiem N, Fazzani M, Ben Kahla M, et al. Management of hidradenitis suppurativa in Tunisia: A Delphi expert consensus. J Cutan Aesthet Surg. 2025. https://pubmed.ncbi.nlm.nih.gov/40212425/ ↩︎
Glatt S, Jemec GBE, Forman S, et al. Efficacy and Safety of Bimekizumab in Moderate to Severe Hidradenitis Suppurativa: A Phase 2, Double-blind, Placebo-Controlled Randomized Clinical Trial. JAMA Dermatol. 2021. https://pubmed.ncbi.nlm.nih.gov/34406364/ ↩︎ ↩︎
Kozera EK, Porter M, Paek SY, et al. Infectious Disease Screening prior to Systemic Immunomodulatory Therapy in Hidradenitis Suppurativa: Consensus Guidelines from the Asia-Pacific Hidradenitis Suppurativa Foundation. Dermatology. 2024. https://pubmed.ncbi.nlm.nih.gov/37963431/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎