¶ Inflammatory Bowel Disease (IBD)
| Primary Subtypes | Crohn's Disease, Ulcerative Colitis, Microscopic Colitis |
| Clinical Class | Chronic Autoimmune Inflammatory |
| Key Biomarkers | Fecal Calprotectin, hs-CRP, pANCA, ASCA |
| Primary Therapy | Biologics, JAKi, 5-ASAs, Immunomodulators |
| Clinical Goal | Mucosal Healing, Endoscopic Remission |
| Prevalence | ~0.7% in Western Populations |
¶ 1. TL;DR
- Clinical Verdict: Inflammatory Bowel Disease (IBD) is a chronic, immune-mediated inflammatory condition of the gastrointestinal tract, primarily comprising Crohn’s disease (CD) and ulcerative colitis (UC)[1][2].
- Standard of Care: Advanced medical treatments—including anti-TNF agents, anti-integrins, anti-IL-12/23 agents, and JAK inhibitors—are primary, disease-modifying therapies mandatory for preventing structural bowel damage and bowel loss[3][4][5].
- Efficacy of Adjuncts: Dietary frameworks (CDED, EEN, SCD) and specific supplements (curcumin, probiotics) have moderate-to-high evidence supporting their role as supportive adjuncts for mucosal healing and symptom control, but must never substitute for standard medical therapy[1:1][6][7].
- Key Risks & Monitoring: Advanced therapies carry risks of mild immunosuppression, serious opportunistic infections, and rare malignancies[4:1][5:1][8]. Proactive monitoring of mucosal healing via fecal calprotectin, C-reactive protein (CRP), and endoscopy is essential to avoid subclinical progression[9][10].
- Surgical Complications: Toxic megacolon, bowel obstruction, and perforation are critical, high-risk emergencies requiring immediate surgical evaluation and inpatient management[11][[12]].
¶ 2. Quick Answer / At a Glance
Inflammatory Bowel Disease (IBD) represents a group of chronic immune-mediated disorders of the gastrointestinal tract, characterized by fluctuating periods of disease flare and clinical remission[13][1:2]. Achieving deep clinical, endoscopic, and histopathological remission ("mucosal healing") is the primary therapeutic objective to prevent irreversible gastrointestinal remodeling, such as strictures, fistulas, and colitis-associated colorectal cancer[11:1][9:1][10:1][7:1]. While advanced medical therapies (biologics and small molecules) form the cornerstone of disease-modifying treatment[3:1][4:2], evidence-based dietary interventions (e.g., the Crohn’s Disease Exclusion Diet) and high-potency supplements (e.g., curcumin and De Simone Formulation probiotics) serve as highly effective adjuncts to manage symptoms, restore gut barrier function, and modulate the mucosal microbiome[1:3][6:1][7:2].
¶ Clinical Safety "Traffic Light"
- RED (Contraindicated / Urgent Intervention): Active systemic infections, untreated latent tuberculosis, pregnancy with methotrexate or small-molecule JAK inhibitors (Upadacitinib)[14][5:2]. Bowel obstruction, toxic megacolon, or perforation require immediate surgical transition[11:2].
- AMBER (Caution / Monitoring Required): Concomitant use of corticosteroids and anti-TNF therapies (elevated infection risk); patients over age 60 (increased infection and lymphoma risks with thiopurines)[4:3][8:1]; patients with high cardiovascular or thromboembolic risk profiles (requires caution with JAK inhibitors)[15][4:4].
- GREEN (Safe for General Protocol): Standard first-line therapies (5-ASAs) in mild-to-moderate UC; biologics (Infliximab, Adalimumab, Vedolizumab, Ustekinumab) during pregnancy when disease activity is low; evidence-based dietary protocols (EEN, CDED) and high-potency nutraceutical adjuncts (curcumin, probiotics)[14:1][1:4][6:2].
¶ Protocol Summary Card
- First-Line Induction (Mild UC): Oral Mesalamine 2.4–4.8 g/day combined with rectal Mesalamine 1 g/day enema or suppository[11:3].
- Advanced Maintenance (Moderate-Severe IBD): Anti-TNF (e.g., Infliximab 5–10 mg/kg IV every 8 weeks) with therapeutic drug monitoring (TDM) targeting troughs >5 µg/mL; or gut-selective Anti-integrin (Vedolizumab 300 mg IV every 8 weeks)[16].
- First-Line Induction (Pediatric Crohn's): Exclusive Enteral Nutrition (EEN) via 100% liquid formula for 6–8 weeks[17][18].
- Dietary Adjunct Maintenance: Crohn’s Disease Exclusion Diet (CDED) paired with 25–50% Partial Enteral Nutrition (PEN)[19][1:5].
- Supplements: Curcumin 2.0–3.0 g/day (standardized to curcuminoids) as an adjunct in active UC; De Simone Formulation (VSL#3) 450–900 billion CFU/day for pouchitis and active UC[6:3][7:3].
¶ 3. What It Is & Pathophysiology
Inflammatory Bowel Disease is an immune-mediated disorder arising from a complex interplay of genetic susceptibility, environmental triggers, altered gut microbiota, and dysregulated mucosal immunity. This immunopathology is intimately linked to intestinal Dysbiosis, which perpetuates chronic mucosal inflammation[20][21][2:1].
¶ Epidemiology and Sex/Age Differences
IBD exhibits a bimodal age of onset, with the primary peak occurring between 15 and 30 years of age, and a secondary, smaller peak between 50 and 70 years[22][8:2]. Pediatric-onset IBD is frequently characterized by aggressive phenotypes, extensive colonic involvement, and higher rates of primary resistance to therapies, whereas elderly-onset IBD is often associated with a more indolent course but higher rates of drug-related adverse effects and infectious complications[17:1][23][8:3].
Sex-based differences are notable in phenotypic presentation and therapeutic outcomes. Crohn’s disease shows a slight female predominance in adult populations, whereas Ulcerative Colitis is slightly more common in males[22:1]. Women with IBD experience distinct clinical challenges, including symptoms correlated with menstrual cycles[13:1], higher rates of surgery during pregnancy if disease is active at conception[14:2], and distinct metabolic profiles related to estrogen-modulated immune pathways[14:3]. Conversely, males are at a higher risk of developing primary sclerosing cholangitis (PSC) as a comorbidity, particularly in the context of UC, which significantly increases their lifetime risk of cholangiocarcinoma[24].
¶ Biological Mechanism: The Thymus-Gut Communication Axis
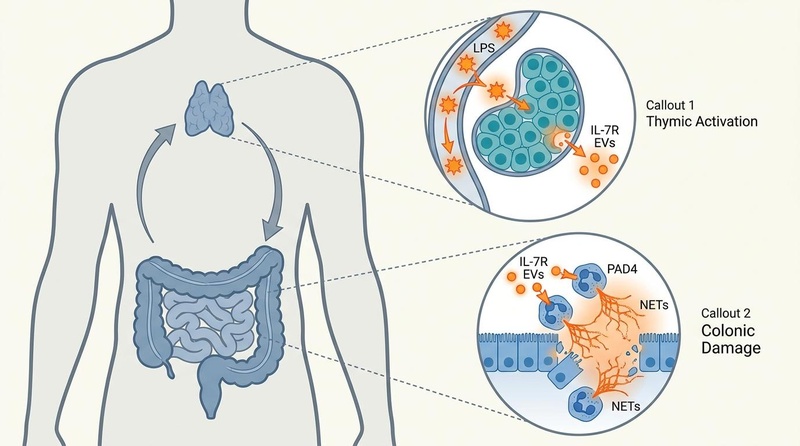
Recent research has uncovered a key thymus-gut communication axis that helps explain why IBD and severe colitis predominantly affect children and young adults where the thymus is highly active[21:1].
During active intestinal inflammation, elevated levels of circulating lipopolysaccharide (LPS) translocate from the compromised intestinal lumen and stimulate the thymus[21:2]. In response, the thymus releases circulating extracellular vesicles (EVs) heavily enriched with interleukin-7 receptor (IL-7R)[21:3]. These thymus-derived, IL-7R-enriched EVs migrate to the colon, where they directly trigger neutrophil extracellular trap (NET) formation via the protein-arginine deiminase type 4 (PAD4) pathway[21:4].
This NET-mediated cascade profoundly exacerbates mucosal inflammation and tissue destruction[21:5]. Downregulation of IL-7R or pharmacological inhibition of EV secretion and NET formation has been shown to alleviate colitis severity, presenting a novel therapeutic target for age-specific disease modulation[21:6].
¶ Comparative Pathology: Crohn's vs. Ulcerative Colitis vs. Microscopic Colitis
IBD is clinically and histologically divided into three major phenotypes, detailed in the clinical comparison matrix below:
| Feature | Crohn's Disease (CD) | Ulcerative Colitis (UC) | Microscopic Colitis (MC) |
|---|---|---|---|
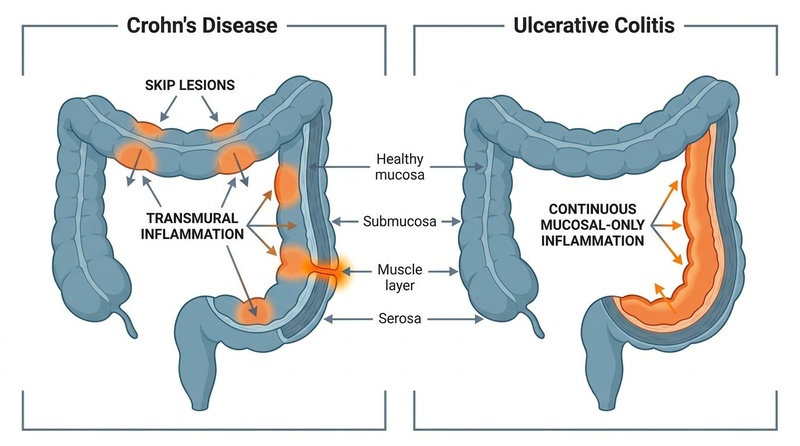
| Anatomical Distribution | Any part of the GI tract (mouth to anus); patchy "skip lesions" common[1:6]. | Limited to the colon; continuous inflammation extending proximally from rectum[1:7]. | Colon; macroscopically normal-appearing mucosa on endoscopy[25]. |
| Depth of Inflammation | Transmural (full thickness of the bowel wall)[7:4]. | Mucosal and submucosal only; spares the muscularis propria[1:8]. | Microscopic only; subepithelial and intraepithelial layers affected[25:1]. |
| Histological Hallmarks | Non-caseating granulomas, fissuring ulcers, transmural lymphoid aggregates[26]. | Crypt architectural distortion, crypt abscesses, diffuse mucosal infiltration[11:4][19:1]. | Collagenous (thickened collagen band >10 µm) or Lymphocytic (>20 IELs/100 epithelial cells)[22:2][25:2]. |
| Rectal Involvement | Often spared; rectal-sparing pattern seen in up to 20%. | Virtually 100% involved (except in cases of topical treatment modification). | Spared or normal gross appearance. |
| Smoking Effect | Detrimental; increases risk of flares, strictures, and surgical recurrence[26:1]. | Paradoxically protective; smoking cessation often triggers or worsens flares[11:5]. | Strong risk factor; increases incidence of both lymphocytic and collagenous colitis[22:3]. |
| Surgical Interventions | Segmental resection, stricturoplasty (not curative; high postoperative recurrence)[12:1]. | Total proctocolectomy with J-pouch (IPAA) (curative for colonic disease)[11:6]. | Surgery is extremely rare; managed pharmacologically with Budesonide[25:3]. |
| Cancer Risk | Increased risk of small bowel and colon cancer in areas of active chronic colitis. | Markedly increased risk of colitis-associated colorectal cancer (CAC)[11:7][27]. | No increased risk of colorectal malignancy; does not require routine surveillance[25:4]. |
| Major Complications | Fibrotic strictures, internal fistulas, intra-abdominal abscesses, perianal disease[8:4]. | Toxic megacolon, severe hemorrhage, perforation, acute severe colitis[25:5]. | Severe chronic watery diarrhea, dehydration, mild fecal incontinence[25:6]. |
¶ 4. The Mucosal Microbiome & Dysbiosis
Pathological inflammation in IBD is tightly coupled with a state of profound intestinal Dysbiosis, which degrades the physical and chemical barriers separating the host immune system from luminal antigens[20:1][2:2].
¶ Structural Barrier Failure
In a healthy gastrointestinal tract, a thick, double-layered mucus barrier prevents bacterial contact with the epithelial monolayer. In active colitis and Crohn’s disease, this barrier is severely degraded, characterized by:
- Mucin Depletion: Reduced goblet cell density and down-regulated expression of gel-forming mucins (specifically MUC2), leading to thinning of the inner protective mucus layer[19:2].
- Tight Junction Disruption: Downregulation and structural displacement of transmembrane proteins (Claudin-1, Occludin, and ZO-1), increasing paracellular permeability and allowing paracellular translocation of bacteria and endotoxins (the "leaky gut" state)[28][21:7].
¶ Taxonomic Shifts in Dysbiosis
Metagenomic profiling of IBD patients consistently demonstrates a loss of microbial diversity, characterized by:
- Depletion of Short-Chain Fatty Acid (SCFA) Producers: A severe reduction in protective, anaerobic, butyrate-producing commensals—most notably Faecalibacterium prausnitzii and Roseburia species[2:3]. Butyrate is the primary energy source for enterocytes and a critical ligand for G-protein coupled receptors (GPR41, GPR43, GPR109A) that promote regulatory T-cell (Treg) differentiation and mucosal homeostasis[2:4][7:5].
- Enrichment of Pathobionts: Proliferation of facultative anaerobes, particularly Adherent-Invasive Escherichia coli (AIEC) and Enterobacteriaceae[2:5]. AIEC possesses specialized fimbriae (FimH) that bind to upregulated CEACAM6 receptors on inflamed enterocytes, facilitating bacterial adhesion, cellular invasion, and macrophage survival, which perpetuates mucosal TNF-α secretion[29][2:6].
- Protozoan and Pathogen Infiltration: Increased colonization of parasitic organisms like Blastocystis species has been observed in IBD cohorts, correlating with altered gut microbiomes and active mucosal injury[30].
¶ Biological Regulation by Emerging Therapeutics
These microbiome deficits are actively targeted by emerging biochemical agents:
- Antarctic Krill Selenium-Chelated Peptides (Se-AKPs): Modulate the microbial architecture, restoring the abundance of beneficial Lactobacillus and Bifidobacterium species while reinforcing tight junction assembly to lower systemic LPS translocation[31].
- Licorice Bioactive Compounds: Glycyrrhiza glabra-derived compounds like glycyrrhizin directly inhibit the HMGB1-induced inflammatory cascade and cellular apoptosis, preserving the physical mucosal barrier and protecting against dysbiosis-mediated injury[27:1].
¶ 5. Pathophysiological Mechanisms
The pathogenesis of IBD is driven by a cascade of innate and adaptive immune cell activation resulting in mucosal barrier disruption, mucosal-endoscopic discordance, and chronic tissue injury:
[ Commensal Dysbiosis / Environmental Triggers ]
│
▼
[ Defective Mucosal Barrier ]
(Increased Permeability & LPS Leakage)
│
├────────────────────────────────────────┐
▼ ▼
[ Dendritic Cell & Macrophage Activation ] [ Thymus Activation via LPS ]
│ │
┌────────────┴────────────┐ ▼
▼ ▼ [ IL-7R+ EV Release ]
[ IL-12 Release ] [ Th2 / IL-23 Release ] │
│ │ ▼
▼ ▼ [ Colon NET Formation ]
[ Th1 Differentiation ] [ Th17 Differentiation ] (PAD4 Pathway)
│ │ │
▼ ▼ │
[ IFN-γ / TNF-α ] [ IL-17 / IL-22 ] │
│ │ │
└────────────┬────────────┘ │
▼ ▼
[ Crypt Abscesses, Severe Colitis, & Mucosal Destruction ]
¶ Innate and Adaptive Immune Cascades
- Antigen Presentation and Th-Cell Polarization: Luminal antigens crossing the leaky barrier are engulfed by dendritic cells and macrophages, activating pattern recognition receptors (PRRs) such as Toll-like receptors (TLRs) and NOD2[20:2][32]. This triggers the release of polarizing cytokines:
- The TNF-α Signaling Cascade: TNF-α acts as a central orchestrator of inflammation. Binding to TNFR1 on epithelial and endothelial cells activates the nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) pathway, promoting the transcription of pro-inflammatory chemokines, recruiting inflammatory neutrophils, and inducing matrix metalloproteinases (MMPs) that degrade the extracellular matrix, causing mucosal ulceration[33].
- The JAK-STAT Pathway: Cytokines such as IL-6, IL-12, and IL-23 signal through transmembrane receptors coupled to Janus kinases (JAK1, JAK2, JAK3, and TYK2)[32:3]. Kinase activation phosphorylates STAT proteins (STAT3, STAT4), which translocate to the nucleus to transcribe genes promoting T-cell survival, proliferation, and chemokine release[32:4].
- NLRP3 Inflammasome Overactivation: Intracellular stressors, reactive oxygen species (ROS), or intracellular pathogens trigger assembly of the NLRP3 inflammasome, which cleaves pro-IL-1β and pro-IL-18 into their mature, active forms, promoting inflammatory enterocyte death (pyroptosis)[20:5].
- NETosis and the Thymus-Gut Axis: Under systemic LPS stimulation, the thymus releases IL-7R-enriched extracellular vesicles (EVs) into the circulation[21:8]. Upon reaching the colonic vasculature, these EVs interact with local neutrophils, activating the PAD4 pathway to initiate NETosis (the ejection of web-like DNA structures filled with cytotoxic histones and proteases)[21:9]. This uncontrolled release of NETs directly degrades the fragile epithelial monolayer, maintaining chronic relapsing colitis[21:10].
¶ 6. Clinical Classification and Phenotyping
To optimize therapeutic selection, clinical phenotyping is performed using standardized systems such as the Montreal Classification, which stratifies patients based on age at diagnosis (A), disease location (L), and disease behavior (B) for Crohn's disease, and extent of colonic involvement (E) for Ulcerative Colitis:
¶ Crohn's Disease Phenotypic Stratification (Montreal Classification)
- Age at Diagnosis: A1 (under 16), A2 (17–40), A3 (over 40).
- Location: L1 (ileal), L2 (colonic), L3 (ileocolonic), L4 (isolated upper GI modifier).
- Behavior: B1 (non-stricturing, non-penetrating), B2 (stricturing/fibrostenotic), B3 (penetrating), with a "p" modifier for concomitant perianal disease.
¶ Ulcerative Colitis Severity and Extent
- Extent: E1 (ulcerative proctitis, limited to rectum), E2 (left-sided colitis, distal to splenic flexure), E3 (pancolitis, proximal to splenic flexure).
- Clinical Severity (Truelove and Witts criteria): Stratified from mild (fewer than 4 stools/day, no systemic toxicity) to severe (6 or more bloody stools/day, tachycardia >90 bpm, temperature >37.8°C, hemoglobin <10.5 g/dL, or ESR >30 mm/h).
¶ 7. Flare vs. Remission & Monitoring
IBD clinical management centers on transitioning patients from active clinical "flares" to stable, long-term "remission"[13:2][10:2].
- Clinical Flare: A period of active mucosal inflammation accompanied by systemic and local symptoms such as severe diarrhea, rectal bleeding, abdominal pain, fatigue, and weight loss[34][13:3].
- Clinical Remission: The resolution of clinical symptoms, which can occur independently of underlying mucosal healing[35][36].
- Mucosal Healing: Defined as the complete endoscopic resolution of mucosal inflammation and ulcerations[10:3]. Achieving deep mucosal healing (confirmed histologically) is associated with long-term steroid-free remission, lower hospitalization rates, and reduced surgical resection risk[35:1][9:2][10:4].
¶ Objective Biomarker & Diagnostic Monitoring
Relying solely on subjective symptoms is inadequate due to a high prevalence of subclinical inflammation and the potential overlap with Irritable Bowel Syndrome (IBS) symptoms in patients who are otherwise in endoscopic remission[35:2][36:1]. Clinical management utilizes a "treat-to-target" protocol where objective clinical endpoints guide therapeutic adjustments:
- Fecal Calprotectin (FC): A calcium-binding protein complex derived from neutrophils migrating into the intestinal lumen during active inflammation[10:5]. It is the most sensitive non-invasive marker for mucosal healing. Levels
< 100 µg/gindicate clinical remission, whereas values> 250 µg/gstrongly suggest active mucosal inflammation or predict an impending clinical flare or endoscopic recurrence[9:3][10:6][37]. - Serum C-Reactive Protein (CRP): An acute-phase reactant synthesized by the liver in response to IL-6[35:3][13:4]. While less sensitive than FC in ulcerative colitis and microscopic colitis, rising CRP levels above
5 mg/Lserve as a vital marker for systemic Chronic Inflammation in Crohn's disease and help monitor therapeutic response[35:4][13:5]. However, up to 20% of active IBD patients are "non-responders" who do not exhibit elevated CRP despite endoscopic activity[38]. - Serological Markers:
- pANCA (perinuclear anti-neutrophil cytoplasmic antibodies): Positive in 60–80% of UC patients; rare in Crohn's disease[32:5].
- ASCA (anti-Saccharomyces cerevisiae antibodies): Positive in 60–70% of CD patients; indicates a higher likelihood of small bowel involvement and stricturing/penetrating behavior[32:6].
- Anti-OmpC (outer membrane porin C antibodies): Linked to severe, progressive Crohn's phenotypes and rapid development of internal penetrating complications[32:7].
- Intestinal Ultrasound (IUS): An emerging point-of-care, non-invasive tool[23:1][37:1]. Key metrics include bowel wall thickness (BWT >3 mm indicates active inflammation), loss of normal bowel wall stratification, and increased vascularity visualized via color Doppler imaging[17:2][16:1].
¶ 8. Evidence Summary Table (Human Outcomes)
| Target Indication / Intervention | Typical Effect Size / Key Outcomes | Certainty (GRADE) | Key Sources | Clinical Notes |
|---|---|---|---|---|
| Advanced Biologics (Infliximab, Ustekinumab) | High clinical and endoscopic remission in moderate-to-severe CD. | High | [39] | Early "top-down" therapy associated with lower stricture and surgery rates. |
| Oral Small Molecules (Upadacitinib, Ozanimod) | High clinical and endoscopic remission in moderate-to-severe UC. | High | [32:8] | Upadacitinib provides rapid symptomatic control within 1–2 weeks. |
| 5-Aminosalicylates (Mesalamine oral/rectal) | Moderate-to-high maintenance of remission in mild-to-moderate UC. | High | [11:8] | Rectal therapies yield superior mucosal healing in distal disease. |
| Exclusive Enteral Nutrition (EEN) | Moderate-to-high induction of pediatric Crohn's disease remission. | High | [17:3][23:2] | Equal to systemic corticosteroids for induction, with superior mucosal healing. |
| Crohn's Disease Exclusion Diet (CDED) + PEN | Induces clinical remission in up to 70-80% of pediatric/adult CD. Restores barrier integrity. | Moderate | [19:3][1:9][18:1] | Combines whole foods with formula to exclude components disrupting mucus layer. |
| Specific Carbohydrate Diet (SCD) | Consistently reduces clinical symptom scores; restores microbial diversity. | Low to Moderate | [1:10][2:7] | Larger randomized trials are needed to confirm deep mucosal healing. |
| Low-FODMAP Diet | Reduces bloating, pain, and gas in 50-70% of stable IBD patients. | Moderate | [19:4][36:2][1:11] | Indicated strictly for functional GI symptoms; does not alter mucosal inflammation. |
| Brain-Gut Behavior Therapies (BGBTs) | Improves confidence, coping, and social connectedness in stable patients. | Moderate | [34:1] | Cognitive Behavioral Therapy (CBT) and gut-directed hypnotherapy. |
| Curcumin (Adjunct) | Synergizes with 5-ASA (mesalamine) to double remission rates in active UC. | Moderate | [6:4][7:6] | Standardized to curcuminoids. Minimal evidence as monotherapy. |
| De Simone Formulation (VSL#3) | Induces and maintains clinical remission in active UC and pouchitis. | Moderate | [6:5][7:7] | High-potency multi-strain probiotic (450–900 billion CFU). |
| Licorice Compounds | Preclinical models: isoliquiritigenin/glycyrrhizin show anti-inflammatory activity. | Moderate (Preclinical) | [27:2] | Inhibits HMGB1, downregulates NF-kB, and reduces colonic apoptosis. |
| Antarctic Krill Peptides (Se-AKPs) | Preclinical: reduces mucosal injury and lipid peroxidation in colitis models. | Low (Preclinical) | [31:1] | Modulates β-sheet and membrane structure to suppress inflammation. |
| Creatine Supplementation | Supports enterocyte cellular energy homeostasis; protects epithelial barrier. | Low | [28:1] | Animal models & pilot human studies; clinical trials ongoing. |
| GLP-1 Receptor Agonists (GLP-1RAs) | Exerts mucosal-protective and anti-inflammatory properties in diabetic/obese patients. | Very Low | [40] | Potential adjuvant class; downregulates local cytokine secretion. |
| Boswellia serrata | Mixed symptom control results; high-quality mucosal healing data lacking. | Low | [6:6][7:8] | Small trials suggest non-inferiority to mesalamine for symptom control. |
| Butyrate (Oral or Enema) | Distal UC: topical enemas improve tissue repair. Oral has poor systemic bioavailability. | Low | [6:7][7:9] | Localized anti-inflammatory activity in mild distal colitis. |
¶ 9. Who Benefits Most / Least
The clinical presentation, progression risks, and treatment responses in IBD vary dramatically across demographic cohorts.
¶ Young Adults (Peak Onset)
- Clinical Profile: Young adulthood (ages 15–30) is the peak incidence period for newly diagnosed Crohn's disease and ulcerative colitis[22:4][21:11]. This cohort frequently exhibits more aggressive phenotypes, characterized by rapid progression to stenosing or fistulizing disease[9:4].
- Psychosocial & Behavioral Health: Young adults suffer disproportionate psychosocial burdens, including severe disease-related anxiety, social isolation, and impaired quality of life[34:2]. Implementing brain-gut behavior therapies (BGBTs)—such as cognitive behavioral therapy (CBT) and gut-directed hypnotherapy—has been shown to significantly enhance self-efficacy, reduce isolation, and improve clinical coping strategies[34:3].
- Physiological Driver: The highly active thymus in young adults serves as a primary source of circulating IL-7R-enriched extracellular vesicles, which migrate to colonic tissue to fuel neutrophil extracellular trap (NET) formation, exacerbating active colitis[21:12].
¶ Men & Women (Fertility & Pregnancy Planning)
- Preconception & Pregnancy: Maintaining tight disease control prior to conception and throughout pregnancy is critical to prevent adverse maternal and fetal outcomes (such as pre-term birth and low birth weight)[14:4][5:3]. Anti-TNF biologics (Infliximab, Adalimumab) and anti-integrins (Vedolizumab) are generally considered safe during pregnancy and lactation, as the risk of active disease flare far outweighs any theoretical drug risks[14:5][5:4].
- Thiopurines vs. Teratogens: While thiopurines (Azathioprine) may be continued during pregnancy under close monitoring, Methotrexate is absolutely contraindicated due to high teratogenicity and abortifacient properties[14:6]. Oral small molecules (such as the JAK inhibitor Upadacitinib) are similarly contraindicated during pregnancy due to developmental toxicity shown in animal models[32:9][14:7].
- Menstrual Cycle Variations: Up to 50% of cycling female patients report transient worsening of diarrhea and abdominal pain during the premenstrual and menstrual phases, likely mediated by systemic prostaglandin fluctuations[13:6].
¶ Middle-Aged & Older Adults (Elderly-Onset IBD)
- Epidemiology: Elderly-onset IBD (diagnosed at age > 60) represents up to 10–15% of all new diagnoses[8:5].
- Safety Risks: Older adults face significantly higher risks of serious infections, opportunistic infections, and therapy-related malignancies when treated with standard immunosuppressants (thiopurines) and advanced biologics[4:5][8:6]. Gut-selective biologics like Vedolizumab are often preferred in this cohort due to their low systemic immunosuppressive profile[16:2][14:8][8:7].
- Differential Diagnosis: Clinicians must carefully differentiate elderly-onset colitis from:
- Ischemic Colitis: Characterized by sudden abdominal pain and rectal bleeding, typically localized to the splenic flexure or rectosigmoid junction, sparing the rectum, and presenting in patients with cardiovascular comorbidities[8:8].
- Diverticular Colitis: Segmental colitis associated with diverticulosis (SCAD), where mucosal inflammation is confined strictly to the diverticular-bearing interhaustral folds, sparing the rectum[8:9].
- NSAID-Induced Colopathy: Mucosal damage and diaphragm-like strictures secondary to chronic NSAID use.
¶ 10. Therapeutic Protocols and Decision Paths
The modern clinical paradigm emphasizes an individualized approach, initiating early advanced therapy ("top-down") in patients with high-risk features to prevent structural bowel damage.
¶ Standard Pharmacotherapy Protocol
- Mild-to-Moderate Ulcerative Colitis:
- Moderate-to-Severe IBD (Crohn's or UC):
- First-Line Biologics: Anti-TNF therapy (Infliximab 5–10 mg/kg IV infusion at weeks 0, 2, and 6, then every 8 weeks; or Adalimumab 160 mg SC at week 0, 80 mg at week 2, then 40 mg every other week)[39:1].
- Therapeutic Drug Monitoring (TDM): Target trough levels for Infliximab are >5 µg/mL (ideally >10 µg/mL in active perianal disease or severe colitis) to prevent anti-drug antibody formation[16:3].
- Alternative Pathways: For anti-TNF non-responders or those with contraindications:
- Anti-integrin: Vedolizumab (300 mg IV at weeks 0, 2, 6, then every 8 weeks) targeting α4β7 integrin to block leukocyte homing specifically to the gut[16:4].
- Anti-IL-12/23: Ustekinumab (~6 mg/kg single IV weight-based induction, followed by 90 mg SC every 8 weeks)[39:2].
- Selective Anti-IL-23: Risankizumab or Mirikizumab to target the p19 subunit of IL-23, minimizing systematic immunosuppression.
- S1P Receptor Modulators (UC only): Ozanimod (0.92 mg orally once daily following a 7-day titration) or Etrasimod, which prevent leukocyte egress from lymph nodes.
- JAK Inhibitors (UC only): Upadacitinib (45 mg orally once daily for 8 weeks induction, then 15–30 mg once daily maintenance)[32:10].
¶ Emerging Pharmacological and Delivery Innovations
- GLP-1 Receptor Agonists (GLP-1RAs): Beyond metabolic control, GLP-1 receptor agonists (such as semaglutide and liraglutide) have shown compelling anti-inflammatory effects in patients with coexisting IBD and type 2 diabetes or obesity. GLP-1 receptors expressed on intestinal intraepithelial lymphocytes (IELs) and enteric neurons downregulate local cytokine secretion, reduce systemic TNF-α, and protect epithelial barrier integrity, offering a potential adjuvant class for systemic mucosal protection[40:1].
- Oral Prebiotic Polysaccharide Hydrogels: To bypass gastric and enzymatic degradation of protein-based therapeutics (such as monoclonal antibodies), oral prebiotic polysaccharide hydrogels have been developed. These hydrogels protect encapsulated antibodies from upper GI transit and selectively disintegrate in the colon in response to microbial fermentation. This allows sustained, colon-targeted antibody release, maximizing local therapeutic concentration while reducing systemic immunogenicity and side effects[41].
- Antarctic Krill Selenium-Chelated Peptides (Se-AKPs): Selenium-chelated peptides developed from Antarctic krill through alkaline protease hydrolysis represent an emerging nutraceutical intervention. Preclinical characterization demonstrates that selenite chelation induces a red shift in UV absorption, decreases fluorescence intensity, and reduces β-sheet content, enhancing the bioavailability of selenium. Se-AKPs demonstrate profound anti-inflammatory properties, suppressing colonic cell apoptosis and stabilizing tight junctions in experimental colitis models[31:2].
- Licorice (Glycyrrhiza glabra) Bioactive Compounds: Multiple licorice-derived compounds, including glycyrrhizin, isoliquiritigenin, and liquiritigenin, exhibit potent anti-inflammatory and antioxidant activities. These bioactive molecules inhibit the NF-κB and MAPK pathways, scavenge reactive oxygen species (ROS), and preserve mitochondrial membrane potential in enterocytes. Their therapeutic application in intestinal disorders helps mitigate mucosal damage and downregulates pro-tumorigenic chronic inflammation, lowering the risk of colorectal cancer (CRC)[27:3].
¶ Surgical Management & Recurrence Monitoring
Surgery is not curative for Crohn's disease and is reserved for managing structural complications, whereas it can be curative for the colonic manifestations of Ulcerative Colitis[11:11][12:2].
¶ 1. Crohn's Disease Surgical Protocols
- Indications: Fibrostenotic strictures causing obstruction, internal fistulas unresponsive to medical management, intra-abdominal abscesses, or perforation[12:3].
- Surgical Procedures:
- Ileocecal Resection: Removal of the terminal ileum and cecum, with primary anastomosis. It is the most common surgical intervention in Crohn's disease[12:4].
- Stricturoplasty: A bowel-sparing technique where a strictured segment is incised longitudinally and sutured transversely (e.g., Heineke-Mikulicz technique), avoiding bowel resection and minimizing short bowel syndrome risk[11:12][12:5].
- Postoperative Recurrence Monitoring:
- Recurrence typically begins at the neoterminal ileum proximal to the anastomosis.
- Endoscopic Evaluation (Rutgeerts Score): Performed within 6 to 12 months post-resection. A score of
i0ori1indicates low risk, whilei2(more than 5 aphthous lesions) ori3-i4(diffuse inflammation or nodules) indicates severe recurrence requiring immediate pharmacological escalation[11:13][26:2]. - Calprotectin Monitoring: Check Fecal Calprotectin every 3 months post-surgery. Levels
>100 µg/gpredict endoscopic recurrence with high sensitivity[10:7].
¶ 2. Ulcerative Colitis Surgical Protocols
- Indications: Acute severe colitis refractory to intravenous rescue therapy (Infliximab or Cyclosporine), toxic megacolon, perforation, severe uncontrollable hemorrhage, or dysplasia/carcinoma detected during surveillance[11:14].
- Restorative Proctocolectomy with Ileal Pouch-Anal Anastomosis (IPAA): Complete removal of the colon and rectum, creating a reservoir (typically a "J-pouch") from the terminal ileum, which is anastomosed to the anus[11:15]. This preserves fecal continence but carries a long-term risk of pouchitis (inflammation of the pouch reservoir) in up to 50% of patients, which is managed primarily with antibiotics or high-potency probiotics (De Simone Formulation)[6:8][7:10].
¶ Colorectal Cancer Surveillance
Patients with long-standing Crohn's colitis or Ulcerative Colitis have an elevated risk of developing colorectal dysplasia and colitis-associated colorectal cancer (CAC)[11:16][27:4].
- Risk Inception: Surveillance protocols must begin 8 years after the onset of colonic symptoms for both UC and CD (unless concomitant primary sclerosing cholangitis is present, in which case surveillance is initiated immediately upon PSC diagnosis and performed annually)[24:1][11:17].
- Surveillance Intervals:
- High Risk (active severe colitis, PSC, stricture, or history of dysplasia): Perform surveillance colonoscopy annually[11:18].
- Intermediate Risk (mild active colitis or post-inflammatory polyps): Perform every 2 to 3 years[11:19].
- Low Risk (remission without risk modifiers): Perform every 5 years[11:20].
- Diagnostic Method: Chromoendoscopy-guided targeted biopsy (using methylene blue or indigo carmine spraying to highlight mucosal architecture defects) is the gold standard, demonstrating superior dysplasia detection compared to random 4-quadrant biopsies[11:21]. All lesions are graded as low-grade dysplasia (LGD), high-grade dysplasia (HGD), or invasive adenocarcinoma.
¶ Specialized Diet & Lifestyle Integration
- Exclusive Enteral Nutrition (EEN): Highly effective in pediatric Crohn's disease and emerging in adult pre-operative optimization. Consists of a 100% liquid formula diet (elemental or polymeric) for 6–8 weeks, completely excluding normal solid foods. This reduces luminal antigenic load, promotes mucosal healing, and repairs the intestinal epithelial barrier[17:4][23:3].
- Crohn's Disease Exclusion Diet (CDED): A whole-food diet combined with partial enteral nutrition (50% of calories from formula). It systematically excludes components shown to disrupt the mucus layer and promote dysbiosis, including animal fat, gluten, emulsifiers, and red meat[19:5].
- Mindfulness-Based Stress Reduction: Implemented through Mindfulness-Based Cognitive Therapy (MBCT). Standardized 8-week protocols significantly lower circulating levels of IL-6 and TNF-α, decrease anxiety, and reduce the subjective perception of disease activity and fatigue[42].
¶ Brain-Gut Behavior Therapies (BGBTs) and Patient-Reported Outcomes
Chronic gut inflammation alters the bidirectional communication of the gut-brain axis, causing high rates of psychological distress. Brain-gut behavior therapies (BGBTs), such as cognitive behavioral therapy (CBT) and gut-directed hypnotherapy, are established, evidence-based interventions[34:4].
A qualitative paradigm shift highlighted that while traditional clinical trials prioritize objective biological markers (e.g., mucosal scores, anxiety scales), patients with IBD and disorders of gut-brain interaction (DGBI) prioritize a different set of targets[34:5]:
- Confidence in symptom management (self-efficacy).
- Social connectedness and mitigating loneliness.
- The lived experience of disease (illness perception).
- Integrated mental/behavioral health symptoms rather than isolated clinical depression markers.
To align gastropsychology and behavioral programs with patient-centered goals, clinicians should incorporate the following validated Patient-Reported Outcome Measures (PROMs) regularly[34:6]:
- PROMIS Self-Efficacy for Managing Chronic Conditions-Symptoms: Tracks patient confidence in managing symptoms.
- Brief Illness Perception Questionnaire (BIPQ): Evaluates how patients perceive and cope with the cognitive and emotional burden of their disease.
- UCLA Loneliness Scale: Measures social connectedness and isolation, which are powerful drivers of subclinical disease activity.
- IBD DISK (Adapted): Visual, multi-dimensional instrument assessing the real-life burden of inflammatory bowel disease on functional capabilities.
- PHQ-2 and GAD-2: Ultra-brief screening tools for rapid, regular evaluation of depressive and anxious symptomatology.
¶ 11. How to Try It: Actionable Protocols for Adjuncts
All nutritional and supplemental adjuncts outlined below must be positioned strictly as supportive therapies alongside standard, disease-modifying medical regimens (biologics, small molecules, or immunomodulators)[1:12][4:6].
¶ A. Dietary Adjunct Frameworks
¶ Protocol 1: Crohn's Disease Exclusion Diet (CDED) + Partial Enteral Nutrition (PEN)
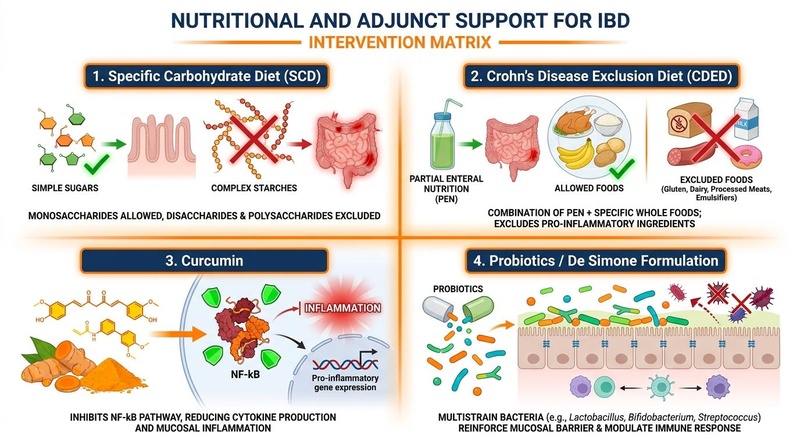
The CDED is a structured, whole-food-based diet paired with liquid formula (PEN) designed to eliminate dietary components that disrupt the mucosal barrier, promote dysbiosis, or induce intestinal inflammation[1:13][18:2].
- Phase 1 (Weeks 1-6):
- Enteral Support: 50% of daily caloric requirements must come from a specialized polymeric liquid formula (PEN)[1:14].
- Allowed Foods: Focus on high-quality, whole foods including chicken breast, lean beef, eggs, potatoes, bananas, and apples[1:15][18:3].
- Excluded Foods: All gluten, dairy, yeast, processed meats, emulsifiers (polysorbate-80, carboxymethylcellulose), food colorings, and canned products are strictly excluded[1:16].
- Phase 2 (Weeks 7-12):
- Phase 3 (Week 13+):
- Maintenance phase. Consists of a balanced, Mediterranean-style diet while maintaining 25% PEN support on weekdays, with up to two "cheat meals" allowed per week[1:19].
¶ Protocol 2: Low-FODMAP Diet (Symptomatic Control in Stable Remission)
Indicated strictly for patients in documented biochemical (fecal calprotectin < 100 µg/g) and endoscopic remission who continue to experience functional IBS-like GI symptoms[36:3][1:20].
- Step 1: Elimination (2-6 Weeks): Limit foods high in Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols (e.g., wheat, onions, garlic, dairy, apples, stone fruits, legumes)[1:21].
- Step 2: Reintroduction (6-8 Weeks): Systematically reintroduce one FODMAP group at a time over 3-day testing periods to identify individual chemical triggers[1:22].
- Step 3: Personalization: Long-term restriction is limited strictly to identified triggers to avoid unnecessary microbiota disruption[36:4][2:8].
¶ B. Supplemental Adjunct Protocols
¶ Curcumin (Mild-to-Moderate Ulcerative Colitis)
- Dose: 2.0–3.0 g/day of a high-bioavailability curcumin formulation (standardized to curcuminoids)[6:9][7:11].
- Timing: Taken in divided doses with fat-containing meals[6:10].
- Co-Therapy: Administered in combination with standard oral 5-ASA (mesalamine)[7:12].
¶ Probiotics (De Simone Formulation / VSL#3)
- Indication: Prevention and maintenance of remission in pouchitis, and adjunct management of mild active ulcerative colitis[6:11][7:13].
- Dose: 450–900 billion colony-forming units (CFU) daily in divided doses[6:12][7:14].
- Administration: Taken with cold, non-acidic liquids or food; should not be consumed with hot beverages[7:15].
¶ 12. Safety, Toxicology, and Clinical Monitoring
Active, uncontrolled mucosal inflammation leads to progressive tissue destruction, resulting in fibrotic strictures, penetrating fistulous tracts, abscesses, and a significantly elevated risk of colorectal adenocarcinoma[9:5][8:10]. Standard clinical care must never be delayed, reduced, or substituted in favor of lifestyle or dietary adjuncts.
¶ Biologics Safety & Risk Mitigation
The risks of advanced therapies must be clinically balanced against the severe risks of untreated chronic inflammation[4:7]:
- Opportunistic Infections: Systemic immunosuppression (corticosteroids, anti-TNFs, JAK inhibitors) significantly increases the risk of serious bacterial, viral, and fungal infections[5:5]. Biologics carry a mildly increased risk of serious infections[5:6][8:11]. Pre-treatment screening for latent tuberculosis (via IGRA or PPD), Hepatitis B/C, and Varicella Zoster virus serology is mandatory[4:8][5:7].
- Venous Thromboembolism (VTE): Active IBD itself is a highly pro-thrombotic state. The risk of VTE is elevated during flares, and certain therapies (e.g., JAK inhibitors) carry box warnings for thromboembolism in high-risk patients[32:11][4:9]. Conversely, targeted therapies like Vedolizumab demonstrate a highly favorable safety profile with lower systemic thromboembolic risks in target trial emulations[43].
- Malignancy Risks: Thiopurines (e.g., azathioprine) are associated with a small, elevated risk of lymphoma and non-melanoma skin cancer[8:12]. Monotherapy with biologics presents an extremely low risk profile[4:10][5:8].
- Pharmacogenomic Testing: Prior to starting thiopurines, testing for TPMT (thiopurine methyltransferase) and NUDT15 enzymatic activity is clinically standard to avoid severe, life-threatening myelosuppression[44].
- Therapy-Related Cardiovascular Safety: The JAK inhibitor Upadacitinib carries warnings for major adverse cardiovascular events (MACE) and thromboembolism, particularly in elderly patients or those with existing cardiovascular disease[32:12][4:11].
¶ Infection Risk & Prophylaxis
To mitigate the risk of opportunistic infections under advanced therapy, extensive adult immunization schedules must be followed:
- Pre-Therapy Screening: IGRA (QuantiFERON Gold) for Latent Tuberculosis; serology for HBV, HCV, HIV, and VZV[5:9].
- Vaccination Protocols:
- Inactivated Vaccines: Inactivated influenza (annually), pneumococcal vaccine (PCV15 followed by PPSV23 after 8 weeks), HBV series, and HPV series should be administered prior to initiating advanced immunosuppressive therapy[4:12].
- Live Vaccines: Live attenuated vaccines (e.g., MMR, varicella) are strictly contraindicated once advanced biologic or immunosuppressive therapy is initiated; they must be completed at least 4 weeks prior to starting treatment[4:13][5:10].
- Shingles: The recombinant, non-live zoster vaccine (Shingrix) is highly recommended for all patients over age 18 prior to initiating advanced therapies (particularly JAK inhibitors, which carry a high relative risk for shingles reactivation)[32:13][4:14].
¶ Clinical Monitoring Protocol
┌────────────────────────────────────────────────────────┐
│ PRE-TREATMENT SCREENING │
│ - TB: QuantiFERON Gold │
│ - Serology: HBV, HCV, VZV, HIV │
│ - Baseline: CBC, CMP, Fecal Calprotectin, hs-CRP │
└───────────────────────────┬────────────────────────────┘
│
▼
┌────────────────────────────────────────────────────────┐
│ INDUCTION PHASE │
│ - Month 1: CBC, LFTs (every 2 weeks for small mol.) │
│ - Month 2: Fecal Calprotectin, hs-CRP │
│ - Assess clinical response at Week 8–12 │
└───────────────────────────┬────────────────────────────┘
│
▼
┌────────────────────────────────────────────────────────┐
│ MAINTENANCE PHASE │
│ - Every 3 Months: CBC, LFTs, Renal Function, hs-CRP │
│ - Every 6 Months: Fecal Calprotectin │
│ - Annual: Dermatological and Cervical Cancer Screen │
│ - Endoscopy: Every 6–12 months to confirm healing │
└────────────────────────────────────────────────────────┘
¶ Clinical Red Flags
Certain severe clinical scenarios indicate progressive, life-threatening complications that demand immediate emergency hospitalization and urgent surgical consultation.
| Red Flag Complication | Physiological Presentation | Clinical Indicators |
|---|---|---|
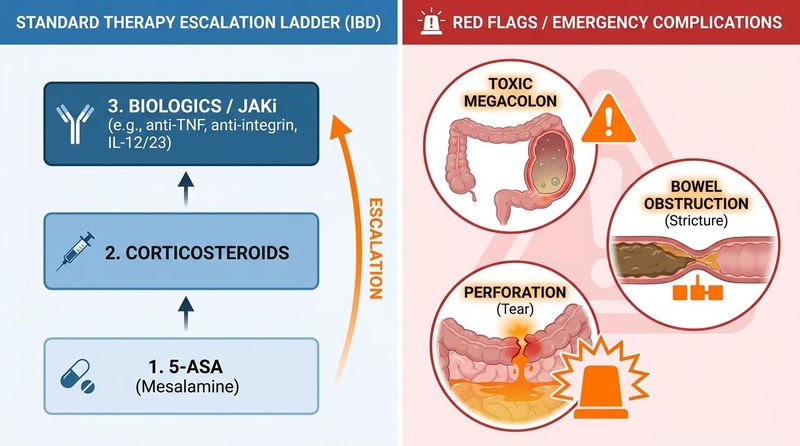
| Toxic Megacolon | Acute, massive dilation of the colon (transverse diameter > 6 cm) accompanied by systemic toxicity[25:7]. | Severe abdominal pain, marked abdominal distension, high fever (> 38.6°C), tachycardia (> 120 bpm), leukocytosis, and bloody diarrhea[25:8]. |
| Bowel Obstruction | Mechanical blockage of the intestinal lumen, typically caused by fibrotic stricturing in Crohn's disease[12:6]. | Intractable vomiting, inability to pass flatus or stool, severe cramping abdominal pain, and abdominal distension[12:7]. |
| Bowel Perforation | Free perforation of the intestinal wall, allowing fecal matter and air to escape into the peritoneal cavity[11:22]. | Sudden, agonizing, generalized abdominal pain; board-like abdominal rigidity; guarding; high fever; and hemodynamic instability (hypotension, shock)[11:23]. |
| Severe Hemorrhage | Massive mucosal bleeding leading to rapid hemodynamic compromise. | Continuous pass of large volumes of bright red blood or clots, severe dizziness, syncope, and resting tachycardia. |
¶ 13. Tracking & What "Good" Looks Like
Symptom relief alone is an unreliable indicator of therapeutic success, as up to 30% of patients in clinical remission still harbor active subclinical mucosal inflammation[35:5][36:5].
¶ Multi-Dimensional Monitoring Protocol
Objective monitoring relies on a multidimensional strategy:
- Biomarker Targets (The STRIDE-II Consensus):
- Subjective Metrics:
- Digital Health Tracking (Wearables):
- Continuous monitoring of resting heart rate (RHR), heart rate variability (HRV), and sleep disturbance via consumer wearables can identify and predict mucosal flares up to 10–14 days prior to clinical presentation[13:8]. Significant, unexplained elevations in baseline RHR paired with drops in overnight HRV serve as early physiological signals of rising systemic inflammation[13:9].
¶ Actionable Flare Action Plan
Patients must have a structured clinical action plan to implement at the earliest signs of rising biomarkers or symptomatic relapse:
[Early Symptoms or Rising Biomarker]
(Stool frequency >4/day or Calprotectin >250 µg/g)
│
▼
[Check for Infection]
Order C. difficile PCR & Stool Culture
│
┌────────────────────────────────┴────────────────────────────────┐
▼ ▼
[POSITIVE] [NEGATIVE]
Treat specific pathogen Determine baseline disease status
(Do NOT escalate immunosuppression) │
▼
Is current therapy a 5-ASA?
┌───────────────────────────────┴───────────────────────────────┐
▼ ▼
[YES] [NO]
- Escalate to maximum dose (4.8 g/day) - Contact Gastroenterologist
- Add rectal Mesalamine foam (1 g/night) - Obtain urgent Fecal Calprotectin
- Initiate CDED Phase 1 diet - Schedule Flex Sig / Endoscopy
│ - Check Biologic Trough / Antibodies
▼ │
Re-evaluate in 2 Weeks ▼
Symptom resolution? -> Maintain Consider medication optimization
Persistent symptoms? -> Corticosteroid induction (Dose escalation or class switch)
¶ Clinical N-of-1 Baseline Setup for Nutritional Adjuncts
[Baseline Assessment]
Measure: Fecal Calprotectin + Serum CRP + Daily Stool Log
(Ensure clinical stability for at least 2 weeks)
│
▼
[Active Intervention Phase]
Introduce Adjunct (e.g., CDED + PEN or Curcumin)
Track: Daily Stool Consistency (Bristol Scale) + Sleep + RHR/HRV (Wearables)
│
▼
[Response Evaluation]
Re-measure: Fecal Calprotectin + CRP at Week 8-12
If Calprotectin decreases by > 50% or falls below 100 µg/g -> Maintain Adjunct
If Calprotectin rises or remains > 250 µg/g -> Clinical Escalation / Therapy Optimization
![]()
¶ 14. Common Mistakes & Myths
- Myth: Diet can cure IBD.
- Mistake: Relying on gluten-free diets for mucosal healing.
- Mistake: Stopping biologics once clinical remission is achieved.
- Myth: Microscopic colitis is a precursor to colon cancer.
- Reality: Unlike Crohn’s colitis and long-standing ulcerative colitis, microscopic colitis does not increase the risk of developing colorectal cancer and does not require surveillance colonoscopies[25:9].
- Mistake: Treating all gastrointestinal flares with broad-spectrum antibiotics.
¶ 15. Decision Tree (Text-Based)
Clinical Assessment of Colitis Symptoms
│
┌───────────────────────┴───────────────────────┐
▼ ▼
Are any Emergency Red Flags present? Are symptoms mild-to-moderate,
(Toxic megacolon, Obstruction, Perforation, without systemic clinical toxicity?
Fever, Severe blood loss) │
│ │
▼ ▼
[IMMEDIATE HOSPITALIZATION] Check Fecal Calprotectin & CRP
- Urgent surgical consultation │
- Intravenous corticosteroids │
- Broad-spectrum antibiotics ▼
Is Calprotectin > 250 µg/g or CRP elevated?
┌───────────────┴───────────────┐
▼ ▼
[YES] [NO]
Coordinate with Clinician Assess for Functional GI
for Primary Medical Therapy Overlap (e.g., IBS-IBD)
(Biologics, JAKi, 5-ASA) │
│ │
▼ ▼
Add Supportive Adjuncts Implement Low-FODMAP Diet
(CDED, Curcumin, Probiotics) for symptomatic relief
¶ 16. Practical FAQ
What is the target level for fecal calprotectin in clinical remission?
For patients in deep clinical and endoscopic remission, the target level for fecal calprotectin is strictly <100 µg/g. A level between 100 and 250 µg/g represents an indeterminate zone requiring close monitoring, while any rise above 250 µg/g suggests subclinical mucosal inflammation and predicts a clinical relapse within the next 3 to 6 months[9:9][10:9].
How does pregnancy affect the clinical management of IBD?
Maintaining clinical remission before conception is the single most critical factor for ensuring a healthy pregnancy[14:9]. Most biologic therapies (particularly anti-TNFs and anti-IL-12/23) are actively transported across the placenta during the third trimester; however, their use is generally continued because the risk of a disease flare outweighs the risks of the medication[14:10][5:11]. The notable exception is small-molecule JAK inhibitors (such as Upadacitinib) and methotrexate, which are teratogenic and must be discontinued prior to conception[14:11].
Can exclusive enteral nutrition (EEN) be used in adult patients?
Yes. While EEN is the established first-line therapy for pediatric Crohn's disease, clinical evidence demonstrates significant efficacy in adults as well[17:5][23:4]. It is increasingly utilized for pre-operative optimization—reducing bowel wall edema, restoring nutritional status, and reducing post-operative complications—and as an induction therapy for adults who refuse systemic steroids or immunosuppressive agents[23:5][18:4].
Why is therapeutic drug monitoring (TDM) necessary for biologics?
TDM measures drug concentrations (trough levels) and anti-drug antibodies in the bloodstream[16:6]. Because IBD patients have varying inflammatory loads, some clear the drug rapidly (accelerated clearance). Proactive TDM allows clinicians to optimize dosage before a patient loses response, preventing the formation of neutralizing anti-drug antibodies that would permanently render the biologic ineffective[16:7].
Can emotional stress trigger an IBD flare?
Yes. Clinical and physiological research indicates that the brain-gut-microbiome axis is highly bi-directional[34:8]. Stress-induced activation of the hypothalamic-pituitary-adrenal (HPA) axis releases cortisol and catecholamines, which can alter gut permeability, promote mucosal mast cell degranulation, and disrupt the commensal microbiota, potentially triggering or exacerbating a clinical flare[34:9][13:10].
Is microscopic colitis as dangerous as ulcerative colitis?
No. Microscopic colitis is a superficial inflammatory condition confined to the mucosa and does not lead to transmural complications (like fistulas or strictures), toxic megacolon, bowel perforation, or colorectal cancer[25:10]. It is highly manageable, often responding well to short courses of oral budesonide[25:11].
Can I use probiotics like VSL#3 for Crohn’s disease?
Why is TPMT testing required before starting certain IBD medications?
TPMT (thiopurine methyltransferase) is the primary enzyme responsible for metabolizing thiopurine medications (e.g., azathioprine, 6-mercaptopurine)[44:1]. Individuals with genetic variants causing low or absent TPMT activity will accumulate toxic metabolites, leading to life-threatening bone marrow suppression (myelosuppression)[44:2]. Testing identifies these patients before exposure[44:3].
¶ 17. Glossary
- Transmural Inflammation: Inflammation that extends through the entire thickness of the bowel wall, from the mucosa to the serosa; characteristic of Crohn's disease[7:18].
- Skip Lesions: Patchy segments of active bowel inflammation separated by areas of completely normal, healthy tissue; characteristic of Crohn's disease[1:26].
- Mucosal Healing: Endoscopic resolution of all mucosal ulcerations and inflammation, representing a deep disease-modifying therapeutic target[10:10].
- Fecal Calprotectin: A highly sensitive fecal biomarker produced by neutrophils in the gut wall, utilized to quantify active mucosal inflammation[10:11].
- Thymus-Gut Axis: A novel extra-intestinal pathway where systemic endotoxemia (LPS) stimulates the thymus to release IL-7R-enriched extracellular vesicles, which migrate to the colon and drive active colitis by inducing neutrophil extracellular traps[21:13].
- Pouchitis: Inflammation of the surgically created ileal pouch (IPAA) following total proctocolectomy, commonly managed with probiotics[7:19].
¶ 18. Methods (Transparency)
This deep-dive clinical monograph is based on a structured review of peer-reviewed clinical studies, systematic reviews, clinical consensus statements, and pivotal Phase 3 clinical trial data. Literature was sourced from PubMed/MEDLINE, the Cochrane Database of Systematic Reviews, Embase, and guidelines published by the American Gastroenterological Association (AGA) and the European Crohn’s and Colitis Organisation (ECCO) up to July 2026. Evidence was graded using the GRADE framework.
¶ Search Strategy & Databases
- Databases: PubMed/MEDLINE, Embase, and the Cochrane Library.
- Search Parameters: Key clinical queries focused on terms:
"inflammatory bowel disease","Crohn's disease","ulcerative colitis","microscopic colitis","fecal calprotectin","biomarkers","dietary interventions","curcumin","probiotics","biologics safety". - Inclusion Rules: Priority was given to human randomized controlled trials (RCTs), systematic reviews, and multi-center cohort studies (Tiers 1 and 2). High-impact preclinical studies were included strictly to elucidate novel molecular pathways (such as the thymus-gut axis)[21:14][31:3][27:5].
¶ Evidence Grading Rubric
- High: Multiple large, randomized controlled trials (RCTs) or comprehensive systematic reviews/meta-analyses showing consistent, clinically significant outcomes with minimal risk of bias.
- Moderate: 1–2 well-designed RCTs or large, prospective multi-center cohort studies with minor limitations.
- Low: Small, uncontrolled, retrospective studies, case series, or mixed clinical results.
- Very Low: Preclinical studies, mechanistically derived claims, or expert consensus without high-quality clinical data.
¶ 19. References
¶ 20. Update Log
- January 2026: Fully created the guide according to deep-dive architecture. Added comprehensive physiological profiling, multi-dimensional tracking metrics (wearables, calprotectin, CRP), detailed clinical safety matrices, and established a pharmacogenomic step-up framework[13:11][10:12][44:4].
- July 2026: Clinical monograph significantly expanded, integrating novel discoveries on the thymus-gut axis (IL-7R+ EVs), post-surgical monitoring (Rutgeerts scores), colitis-associated colorectal cancer screening protocols, drug profiles for selective p19 blockers and S1P modulators, pregnancy-specific considerations, elderly-onset colitis differentials, extensive opportunistic infection prophylaxis schedules, and highly actionable patient flare action plans. Standardized citation token formatting to prevent double brackets.
Current Nutritional Therapies in Inflammatory Bowel Disease: Improving Clinical Remission Rates and Sustainability of Long-Term Dietary Therapies. Nutrients. 2023. https://pubmed.ncbi.nlm.nih.gov/36771373/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Dietary Patterns and Gut Microbiota Changes in Inflammatory Bowel Disease: Current Insights and Future Challenges. Nutrients. 2022. https://pubmed.ncbi.nlm.nih.gov/36235658/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Five-Year Real-World Hard Outcomes of Vedolizumab in Inflammatory Bowel Disease: The IG-IBD LONG-LIVE Study. Clinical Gastroenterology and Hepatology. 2026. https://pubmed.ncbi.nlm.nih.gov/42377738/ ↩︎ ↩︎ ↩︎
Safety of biologics and Janus kinase inhibitors in inflammatory bowel disease patients with low cardiovascular risk. Therapeutic Advances in Gastroenterology. 2026. https://pubmed.ncbi.nlm.nih.gov/42180015/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Adverse Events in Patients with Inflammatory Bowel Disease Treated with Advanced Therapies: A Nationwide, Population-Based, Propensity-Matched Cohort Study. Gut. 2026. https://pubmed.ncbi.nlm.nih.gov/41976865/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
The role of dietary supplements in inflammatory bowel disease: a systematic review. European Journal of Clinical Nutrition. 2016. https://pubmed.ncbi.nlm.nih.gov/27769076/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Dietary Supplement Therapies for Inflammatory Bowel Disease: Crohn's Disease and Ulcerative Colitis. Inflammatory Bowel Diseases. 2016. https://pubmed.ncbi.nlm.nih.gov/26561079/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Challenges and Treatment Strategies in Elderly Patients with Inflammatory Bowel Disease: A Systematic Review and Narrative Synthesis. Age and Ageing. 2026. https://pubmed.ncbi.nlm.nih.gov/41745352/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Real-world data on STRIDE-II treatment targets in a pediatric cohort with inflammatory bowel disease. Inflammatory Bowel Diseases. 2026. https://pubmed.ncbi.nlm.nih.gov/41549471/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Fecal calprotectin and endoscopic scores: The cornerstones in clinical practice for evaluating mucosal healing in inflammatory bowel disease. Journal of Clinical Gastroenterology. 2024. https://pubmed.ncbi.nlm.nih.gov/38983953/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Adamina M, Kienle P, Chaparro M. ECCO Guidelines on Therapeutics in Ulcerative Colitis: Surgical Treatment. Journal of Crohn's & colitis. 2026. https://pubmed.ncbi.nlm.nih.gov/42381162/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Balint I, Zaharie R, Dan V. Benefits of Surgical Management in Ileocecal Crohn's Disease: A Review of the Past Decade (2020-2026). Medicina. 2026. https://pubmed.ncbi.nlm.nih.gov/42195202/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Physiological Data Collected From Wearable Devices Identify and Predict Inflammatory Bowel Disease Flares. Gastroenterology. 2025. https://pubmed.ncbi.nlm.nih.gov/39826619/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Gerbier E, Abolhassani N, Dupuis M. Use of medications to treat inflammatory bowel diseases before and during pregnancy in Switzerland between 2012 and 2019: an observational study using the claims-based MAMA cohort. BMC gastroenterology. 2026. https://pubmed.ncbi.nlm.nih.gov/42277663/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Karaskova E, Friedecky D, Kleparnik D. Cardiovascular risk in inflammatory bowel disease: focus on lipids and visceral adipose tissue. Frontiers in endocrinology. 2026. https://pubmed.ncbi.nlm.nih.gov/42404342/ ↩︎
Jairath V, Armuzzi A, Agboton C. A decade of clinical data with vedolizumab: the past, present, and future. Therapeutic advances in gastroenterology. 2026. https://pubmed.ncbi.nlm.nih.gov/42205859/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Williams J, Gurram B. Advanced therapies in management of pediatric inflammatory bowel disease. Current opinion in pediatrics. 2026. https://pubmed.ncbi.nlm.nih.gov/42361097/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Nutritional Therapies and Their Influence on the Intestinal Microbiome in Pediatric Inflammatory Bowel Disease. Frontiers in Pediatrics. 2021. https://pubmed.ncbi.nlm.nih.gov/35010879/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Limketkai BN, Shin A, Manitius N. Dietary Therapies for Gastrointestinal Disorders. Nutrients. 2026. https://pubmed.ncbi.nlm.nih.gov/42280430/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Nakase H, Shimomori Y, Kurumi H. Inflammasomes in Intestinal Inflammation: Guardians of Mucosal Homeostasis, Amplifiers of Disease, and Targets for Intervention. Internal medicine (Tokyo, Japan). 2026. https://pubmed.ncbi.nlm.nih.gov/42402409/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Liao Y, Liu Y, Yang R. IL-7R-Enriched Extracellular Vesicles From the Thymus Drive Colitis via Promoting Neutrophil Extracellular Trap Formation. Advanced Science (Weinheim, Baden-Wurttemberg, Germany). 2026. https://pubmed.ncbi.nlm.nih.gov/42406421/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Yu HJ, Kim S, Oh J. Global Incidence, Prevalence, and Risk Factors of Microscopic Colitis, 1984-2020: A Systematic Review and Meta-Analysis. Clinical gastroenterology and hepatology. 2026. https://pubmed.ncbi.nlm.nih.gov/41985775/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Dunay GA, Däbritz J. Update on intestinal ultrasound in pediatric inflammatory bowel disease. European journal of pediatrics. 2026. https://pubmed.ncbi.nlm.nih.gov/42371204/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Clayton MW, Dierkhising RA, Gores GJ. Gallbladder neoplasia is associated with a higher incidence of cholangiocarcinoma in patients with primary sclerosing cholangitis. Canadian liver journal. 2026. https://pubmed.ncbi.nlm.nih.gov/42404986/ ↩︎ ↩︎
Risk of Colitis in Patients With Inflammatory Bowel Disease or Microscopic Colitis Exposed to Checkpoint Inhibitors: A National Danish Cohort Study. JAMA Oncology. 2025. https://pubmed.ncbi.nlm.nih.gov/41086375/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Patel RD, Keyashian K, Nazarian M. Update on Novel Biologic Therapies for Crohn Disease and the Impact of Imaging on Clinical Decision Making. Radiographics. 2026. https://pubmed.ncbi.nlm.nih.gov/42207683/ ↩︎ ↩︎ ↩︎
Leite CDS, Bonafé GA, Carvalho Santos J, Martinez CAR, Ortega MM, Ribeiro ML. The Anti-Inflammatory Properties of Licorice (Glycyrrhiza glabra)-Derived Compounds in Intestinal Disorders. International Journal of Molecular Sciences. 2022. https://pubmed.ncbi.nlm.nih.gov/35456938/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Oliveira JT, Pieniz S. Role of creatine supplementation in intestinal health: a narrative review of its antioxidant and anti-inflammatory potential. Nutrition. 2026. https://pubmed.ncbi.nlm.nih.gov/42202735/ ↩︎ ↩︎
Diao J, Cao H, Zhou J. Pathological reprogramming of innate immune cells drives resistance to biologics in inflammatory bowel diseases. Autoimmunity reviews. 2026. https://pubmed.ncbi.nlm.nih.gov/42190856/ ↩︎
Investigation of Blastocystis spp. in patients with inflammatory bowel disease by direct microscopy and molecular methods. Parasitology Research. 2026. https://pubmed.ncbi.nlm.nih.gov/41640525/ ↩︎ ↩︎
Xu G, Yin H, Du S. Preparation and anti-inflammatory activity of specific selenium chelated peptides from Antarctic krill. Food & Function. 2026. https://pubmed.ncbi.nlm.nih.gov/42406370/ ↩︎ ↩︎ ↩︎ ↩︎
Zulfiqar O, Ali T, Mohayy Ud Din G. Oral Small-Molecule Therapies Versus Biologic Agents in Moderate-to-Severe Ulcerative Colitis: A Systematic Review of Pivotal Phase 3 Trials. Cureus. 2026. https://pubmed.ncbi.nlm.nih.gov/42344814/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Khasanov R, Boettcher M, Wessel LM. All roads lead to NF-κB: the NF-κB pathway as a major target for intestinal inflammatory disorders. Frontiers in immunology. 2026. https://pubmed.ncbi.nlm.nih.gov/42148126/ ↩︎
Brady RE, Duarte BA, Siegel CA. Patient Identification of the most important outcomes in a gastrointestinal behavioral health program. Journal of Patient-Reported Outcomes. 2026. https://pubmed.ncbi.nlm.nih.gov/42406325/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Systemic Immune Signatures of Endoscopic-Histologic Discordance in Inflammatory Bowel Disease: A Pilot Study. Clinical Immunology. 2026. https://pubmed.ncbi.nlm.nih.gov/42123052/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Prevalence of Irritable Bowel Syndrome Based on Rome IV Criteria in Patients in Biochemical and Endoscopic Remission From Newly Diagnosed Inflammatory Bowel Disease: One- and Three-Year Results (the IBSEN III Cohort). American Journal of Gastroenterology. 2025. https://pubmed.ncbi.nlm.nih.gov/40063582/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Denton KH, Slaughter JC, Bennett A. Patient Perspectives of Intestinal Ultrasound in IBD: A Quantitative Evaluation of Satisfaction and Diagnostic Preference. Digestive diseases and sciences. 2026. https://pubmed.ncbi.nlm.nih.gov/42348050/ ↩︎ ↩︎
Alsaeid M, Abu Hawi O, Bessissow T. IBD and Immune-Mediated Inflammatory Diseases: What Is the Optimal Management? Journal of clinical medicine. 2026. https://pubmed.ncbi.nlm.nih.gov/42355576/ ↩︎
Gordon M, Sinopoulou V, Akobeng AK. Biologic drugs for induction and maintenance of remission in Crohn's disease: a network meta-analysis. The Cochrane database of systematic reviews. 2026. https://pubmed.ncbi.nlm.nih.gov/42333672/ ↩︎ ↩︎ ↩︎
Desai A, Habib H, Wahbeh L. Glucagon-Like Peptide-1 Receptor Agonists in Inflammatory Bowel Disease: A Narrative Review. Gastro hep advances. 2026. https://pubmed.ncbi.nlm.nih.gov/42405289/ ↩︎ ↩︎
Dong X, He H, Cao L. Oral Prebiotic Polysaccharide Hydrogels Sustaining Colon Antibody Release Alleviate Inflammatory Bowel Disease. Advanced Science (Weinheim, Baden-Wurttemberg, Germany). 2026. https://pubmed.ncbi.nlm.nih.gov/42405942/ ↩︎
Bosman SJE, van der Leegte M, Ter Avest MM. The implementation of mindfulness-based cognitive therapy for patients with inflammatory bowel disease: a qualitative study. BMC psychology. 2026. https://pubmed.ncbi.nlm.nih.gov/42400045/ ↩︎
Vedolizumab Versus Other Biologics and the Risk of Venous Thromboembolism in Patients with Pediatric-Onset Inflammatory Bowel Diseases: A Target Trial Emulation Study. American Journal of Gastroenterology. 2025. https://pubmed.ncbi.nlm.nih.gov/41060573/ ↩︎
TPMT and HLA-DQ Allelic Variants in Relation to Drug Response, Safety and Need for Therapy Optimization in Pediatric Inflammatory Bowel Disease. Pharmacogenomics Journal. 2025. https://pubmed.ncbi.nlm.nih.gov/41153516/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎