¶ Intestinal Permeability and the Gut Barrier: Deep Dive
¶ TL;DR
- The Verdict: Intestinal permeability is a highly regulated, dynamic physiological state, not a static disease. Targeted support can stabilize transient barrier leakage within 2 to 4 weeks.
- Who It Is For: Individuals experiencing stress-induced barrier disruption, athletes suffering from gut ischemia, or older adults managing NSAID-related mucosal irritation.
- Who It Is Not For: Patients experiencing acute clinical barrier failure (sepsis, acute abdomen, or advanced refractory inflammatory bowel disease).
- Key Risks: Over-reliance on commercial testing (e.g., highly unreliable serum zonulin kits) and delaying standard clinical treatment for severe inflammatory pathologies.
- What to Do Next: Implement a foundation of stress mitigation, reduce non-essential NSAID use, and support enterocyte health with L-Glutamine and Zinc Carnosine.
¶ Quick Answer
Intestinal permeability (commonly popularized as "leaky gut") refers to a compromise in the paracellular pathway—the microscopic spaces between adjacent intestinal epithelial cells regulated by tight junction protein complexes [1]. In healthy individuals, these gaps restrict macromolecular translocation while allowing fluid and micronutrient absorption. When compromised by inflammatory, dietary, or psychological stressors, paracellular transport of immunogenic molecules (such as lipopolysaccharides, or LPS) increases, leading to subclinical systemic inflammation [2][1:1][3]. Clinical management focuses on addressing root-cause lifestyle disruptors (such as psychological stress and NSAIDs) and utilizing evidence-backed supplements like L-Glutamine and Zinc Carnosine to support tight junction reassembly [1:2][4][3:1].
¶ What It Is: Biology & Physiology of the Barrier
The intestinal gut barrier is a highly sophisticated, multi-layered defensive system designed to perform two conflicting tasks: maximizing nutrient absorption while completely excluding harmful pathogens, toxins, and immunogenic macromolecules [1:3]. This barrier consists of several distinct functional layers:
- The Mucosal Layer: Divided into an outer, loose mucus gel (which houses commensal bacteria and traps pathogens) and an inner, dense mucus bilayer that is virtually sterile [1:4]. This layer is heavily populated by secretory Immunoglobulin A (sIgA), dimeric antibodies that neutralize pathogens and prevent microbial adherence to epithelial cells [1:5].
- The Epithelial Cell Monolayer: A single layer of columnar epithelial cells (primarily enterocytes in the small intestine and colonocytes in the colon) that forms the primary physical seal [1:6].
- Tight Junction Protein Complexes: Specialized protein networks that physically seal the paracellular space (the gaps between adjacent epithelial cells). These include integral transmembrane proteins—such as occludin and various claudins—which anchor into the cellular cytoskeleton via intracellular scaffold proteins like zonula occludens-1 (ZO-1) [5][6][7].
- Gut-Associated Lymphoid Tissue (GALT): The underlying immunological layer located in the lamina propria, containing macrophages, dendritic cells, T-cells, and mast cells that continually monitor translocated antigens [1:7].
INTESTINAL LUMEN
=======================================================================
[ Outer Mucus Layer ] Commensal Bacteria & Secretory IgA (sIgA)
-----------------------------------------------------------------------
[ Inner Mucus Layer ] Dense, sterile mucin gel layer
=======================================================================
Enterocyte Enterocyte Enterocyte Enterocyte
[ Brush Border ] [ Brush Border ] [ Brush Border ] [ Brush Border ]
| | | | | | | |
| (Nucleus) |=[TJ]= | (Nucleus) |=[TJ]= | (Nucleus) |=[TJ]= | (Nucleus) |
| | | | | | | |
=======================================================================
BASEMENT MEMBRANE
-----------------------------------------------------------------------
LAMINA PROPRIA (GALT Immune Cells, Mast Cells, Capillaries & Venules)
¶ The 60-Second Analogy
Think of the gut barrier as a high-security international border. The outer mucus layer acts as a buffer zone; secretory IgA serves as local border patrol; the epithelial monolayer represents the physical border wall; and tight junctions are the smart electronic gates. Under normal conditions, these gates open briefly to allow verified citizens (amino acids, glucose, and micronutrients) to pass, but remain firmly locked against unauthorized trespassers. When "barrier dysfunction" occurs, these electronic gates glitch and remain stuck open, allowing unauthorized particles to slip across the border unnoticed.
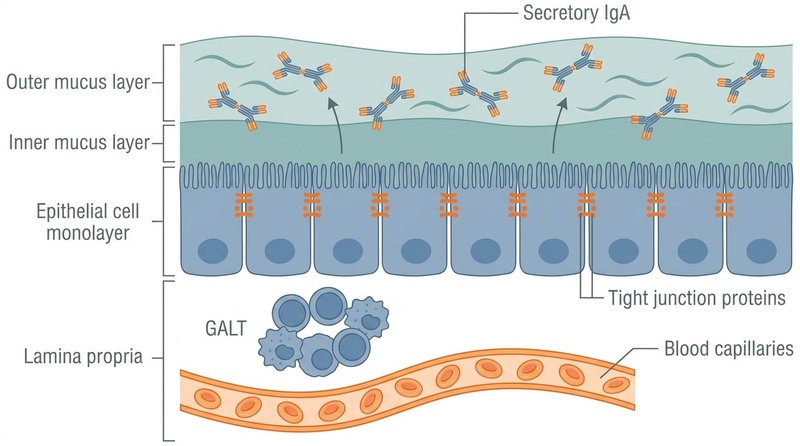
Figure 1: Anatomy of the Intestinal Barrier. The multi-layered defense system includes a dual mucus bilayer, secretory IgA, a single layer of epithelial cells sealed by tight junctions, and a network of capillaries and immune cells (GALT).
¶ Mechanisms of Tight Junction Breakdown
Tight junction disassembly is a tightly regulated molecular process. Cellular stressors—such as localized pro-inflammatory cytokines (TNF-alpha, IL-1beta) or intracellular ATP depletion—trigger intracellular signaling cascades, particularly the mitogen-activated protein kinase (MAPK) pathway [5:1]. Activation of the MAPK pathway upregulates the expression of zonulin (a eukaryotic protein that triggers tight junction disassembly) [5:2][6:1]. Zonulin binds to epidermal growth factor receptors (EGFR) and protease-activated receptor 2 (PAR2) on enterocytes, inducing the intracellular phosphorylation and endocytosis of ZO-1, occludin, and claudins [5:3][6:2].
Once these proteins are internalised and degraded, the paracellular channels widen, allowing luminal macromolecules—such as lipopolysaccharide (LPS), a highly immunogenic cell wall component of Gram-negative bacteria—to flood into the lamina propria and portal circulation [2:1][1:8]. This translocation drives systemic inflammatory cascades (metabolic endotoxemia) [2:2].
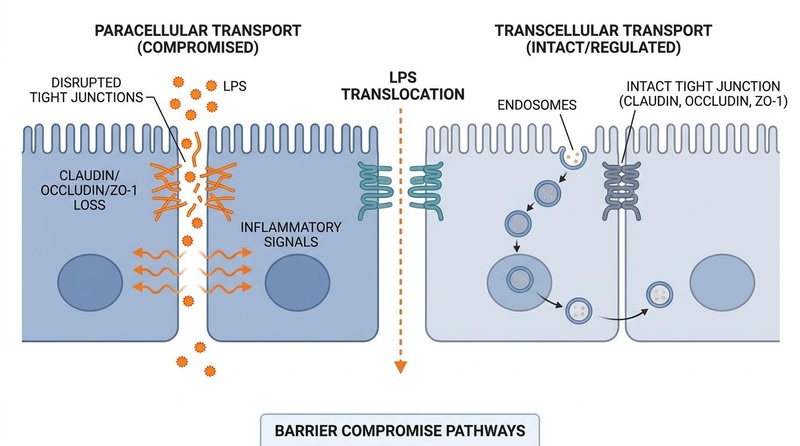
Figure 2: Mechanisms of Tight Junction Breakdown. Inflammatory, dietary, or toxic stressors trigger the disassembly of occludin, claudins, and ZO-1. This increases paracellular permeability, allowing lipopolysaccharides (LPS) and pathogenic macromolecules to translocate into the systemic circulation (metabolic endotoxemia).
¶ What is Real vs. What is Oversold: Deconstructing "Leaky Gut"
In commercial wellness marketing, "leaky gut syndrome" is frequently depicted as the singular, foundational cause of nearly all chronic medical conditions, ranging from chronic fatigue and autoimmune diseases to clinical depression and obesity. While gut barrier health is a key clinical component, this presentation oversimplifies human pathology and reverses cause and effect:
- Epithelial Barrier Dysfunction is Often Secondary: Increased intestinal permeability is rarely the primary, standalone driver of systemic disease. Instead, it is almost always a secondary consequence of upstream physiological disruptions, such as localized mucosal inflammation, severe gut dysbiosis, chronic psychological stress, or metabolic endotoxemia [8][2:3][1:9][3:2].
- Association vs. Causation: While clinical studies show clear associations between increased intestinal permeability and systemic conditions (such as rheumatoid arthritis [8:1] or first-diagnosed atrial fibrillation [2:4]), restoring barrier integrity is an adjunct therapy, not a magical cure-all.
- Dynamic, Not Permanent: Paracellular permeability fluctuates naturally throughout the day in response to meals, exercise, circadian rhythms, and acute stress [9][1:10][3:3]. The gut is designed to handle transient permeability; chronic, unremitting barrier failure is what carries pathological weight [1:11].
¶ Biomarkers & Testing Pitfalls
Accurately measuring gut barrier function in a clinical setting is challenging. Many popular diagnostic offerings marketed to the public lack scientific validity.
¶ 1. The Dual-Sugar Absorption Test (Lactulose/Mannitol Recovery)
This is the accepted physiological gold standard in clinical research [10][1:12][3:4].
- The Concept: The patient ingests a standardized solution containing a small sugar molecule (mannitol, ~182 Da) and a large sugar molecule (lactulose, ~342 Da) [10:1][1:13].
- The Physiology: Mannitol is small enough to be easily absorbed via the transcellular pathway (through the cells), serving as a control for overall mucosal surface area and absorptive capacity. Lactulose is too large to cross the cell membrane and can only cross the barrier paracellularly via compromised tight junctions [10:2][1:14].
- The Output: Urine is collected over 2 to 6 hours. An elevated Lactulose-to-Mannitol (L/M) urinary ratio (typically >0.03) objectively indicates compromised tight junction integrity and increased paracellular permeability [10:3][3:5].
¶ 2. Serum Zonulin: A Major Commercial Pitfall
Serum zonulin is widely offered as a standalone direct marker of a "leaky gut" by commercial testing laboratories. However, robust clinical validation studies have revealed major diagnostic limitations:
- Lack of Assay Specificity: Research demonstrates that standard commercial serum zonulin ELISA (enzyme-linked immunosorbent assay) kits exhibit high cross-reactivity with unrelated proteins (such as haptoglobin and complement factors), failing to selectively measure bioactive monomeric zonulin [10:4].
- No Physiological Correlation: In clinical studies of Crohn’s disease relatives, serum zonulin levels measured by commercial kits completely failed to correlate with the in vivo physiological gold standard L/M ratio [10:5].
- High Inter-individual Fluctuation: Serum zonulin is highly dynamic and fluctuates wildly based on acute stress, diet, and circadian rhythms, rendering a single blood test clinically uninformative for chronic assessment [10:6].
¶ 3. Fecal Calprotectin: An Inflammation Marker, Not a Permeability Marker
Fecal calprotectin is a highly stable protein marker released by neutrophils during active mucosal inflammation [6:3].
- The Distinction: It is an excellent clinical biomarker for monitoring disease activity and progression in Inflammatory Bowel Disease (IBD) [6:4]. It does not directly measure paracellular tight junction leakage, but because local mucosal inflammation directly triggers tight junction breakdown, an elevated fecal calprotectin (>50–100 μg/g) highly correlates with increased barrier permeability [6:5].
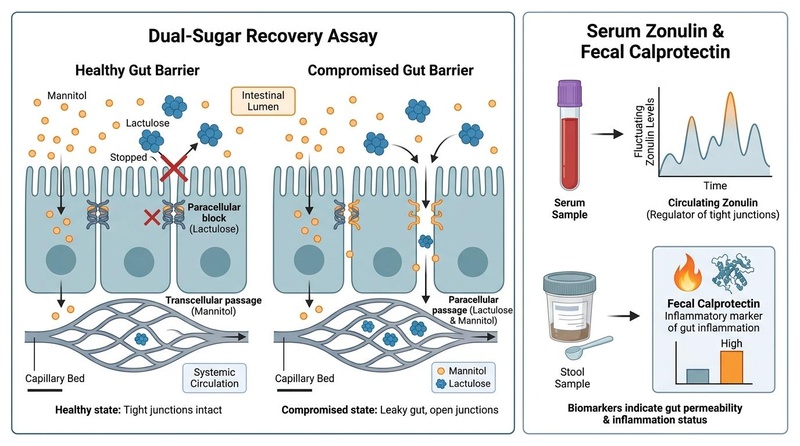
Figure 3: Biomarker Assessment Pathway. The dual-sugar lactulose/mannitol recovery test remains the physiological gold standard. Ingested mannitol (small molecule) is readily absorbed, while lactulose (large molecule) should be blocked. An elevated urinary ratio reflects paracellular barrier compromise. Serum zonulin is highly variable and lacks physiological specificity.
¶ Dietary & Lifestyle Disruptors
The integrity of the tight junction complex is highly sensitive to a variety of exogenous and endogenous stressors:
- Nonsteroidal Anti-Inflammatory Drugs (NSAIDs): NSAIDs (such as indomethacin, ibuprofen, and naproxen) are potent disruptors of the gut barrier [1:15][4:1]. They inhibit cyclooxygenase (COX) enzymes, depleting cytoprotective prostaglandins, reducing mucosal blood supply, and directly damaging epithelial mitochondria, which impairs the ATP-dependent assembly of tight junction complexes [1:16][4:2]. In clinical studies, a single standard dose of indomethacin rapidly and significantly increases paracellular permeability [3:6].
- Heavy Alcohol Use: Ethanol and its primary toxic metabolite, acetaldehyde, directly damage enterocyte membranes and disrupt the microtubule cytoskeleton [1:17]. This cellular injury promotes rapid paracellular translocation of highly inflammatory lipopolysaccharides (LPS) into the portal circulation [1:18].
- Psychological Stress & Mast Cell Activation: Human physiological studies have conclusively established that acute psychological stress (e.g., public speaking, anticipation of pain) triggers gut barrier leakage [3:7]. Stress stimulates the release of corticotropin-releasing hormone (CRH), which directly binds to receptors on mucosal mast cells [3:8]. This triggers rapid mast cell degranulation, releasing tryptase and histamine, which dismantle tight junction proteins [3:9]. Pretreatment with the mast cell stabilizer disodium cromoglycate (DSCG) completely blocks stress-induced intestinal permeability in human subjects [3:10].
- Circadian Disruption & Sleep Deprivation: Sleep restriction downregulates the expression of tight junction scaffolding proteins and reduces protective mucin production, compromising the physical barrier [1:19].
- Ultra-Processed High-Fat/High-Sugar Diets: High intakes of saturated fats and refined sugars shift the intestinal microbiome toward a pro-inflammatory state, reducing the abundance of short-chain fatty acid (SCFA)-producing taxa and causing a direct loss of tight junction integrity [11][1:20].
¶ Does It Work? (Evidence Snapshot)
Clinically studied interventions targeting the intestinal barrier vary significantly in their level of human evidence.
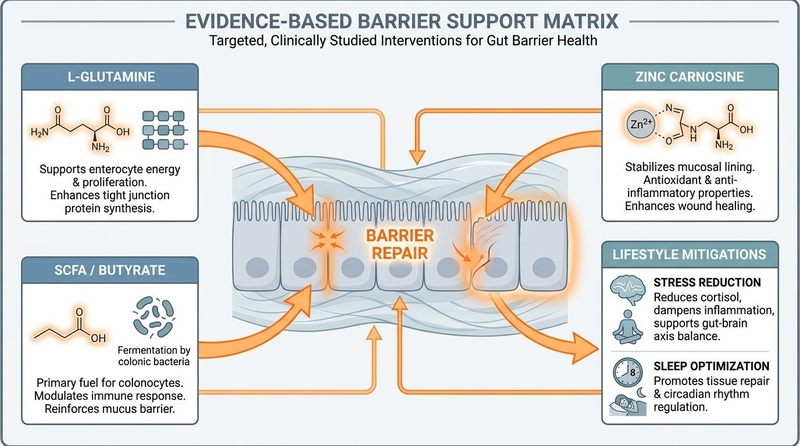
Figure 4: Evidence-Based Barrier Support Matrix. Interventions are categorized by their cellular targets: L-Glutamine provides fuel for enterocyte regeneration, Zinc Carnosine stabilizes tight junctions, SCFAs (butyrate) promote mucin production, and lifestyle mitigations control stress-induced mast cell degranulation.
¶ Evidence Summary Table (Human Outcomes)
| Intervention | Mechanism of Action | Clinical / Physiological Outcomes | Study Count & Type | Certainty Grade | Timeframe | Citations |
|---|---|---|---|---|---|---|
| L-Glutamine | Serves as the primary metabolic fuel for enterocytes; promotes tight junction protein synthesis and prevents stress-induced junction disassembly [1:21]. | Restores L/M ratio to normal range; preserves mucosal thickness and tight junction density under stress [1:22]. | Multiple human RCTs [1:23]. | High | 14 to 30 days | [1:24] |
| SCFA-Producing Probiotics & Metabolites | Generates short-chain fatty acids (primarily butyrate), which serve as fuel for colonocytes and stimulate mucin production [11:1]. | Significantly relieves clinical abdominal symptoms (IBS) and directly improves epithelial barrier function (increases TEER) [11:2]. | Double-blind, randomized controlled trial [11:3]. | High | 28 to 56 days | [11:4] |
| Zinc Carnosine | Directly protects the mucosal lining; promotes epithelial wound healing and tight junction stability [1:25]. | Dampens NSAID-induced small bowel injury and limits increases in paracellular permeability [1:26]. | Human clinical trials [1:27]. | Moderate to High | 10 to 14 days | [1:28] |
| Essential Amino Acids (EAAs) | Protects enterocyte mitochondria from inflammatory stress; supports intracellular ATP levels required for tight junction assembly [12]. | Maintains barrier integrity under conditions of metabolic and inflammatory stress; prevents mitochondrial breakdown [12:1]. | Preclinical in vivo & in vitro models (Insufficient direct human RCTs) | Low (Preclinical) | N/A | [12:2] |
| BPC-157 (Gastric Peptide) | Stabilizes epithelial cell membranes; exerts cytoprotection and endothelial protection; prevents vascular and mucosal leakage [4:3]. | Directly counteracts and rescues NSAID-induced epithelial cytotoxicity; stabilizes paracellular permeability in vivo [4:4]. | Extensive preclinical in vivo / in vitro studies (No published human RCTs for barrier permeability) | Low (Preclinical) | N/A | [4:5] |
| Cowpea Protein Isolate (CPI) | Plant-derived protein isolate that preserves mucosal SCFA levels and downregulates genes linked to excessive nutrient absorption [13]. | Maintains propionic and acetic acid production; reduces digestive/absorptive enzyme gene expression (SGLT1) to prevent epithelial stress [13:1]. | Preclinical in vivo rodent models [13:2]. | Low (Preclinical) | N/A | [13:3] |
| Lactobacillus yoelii Lac-2 | Probiotic strain that downregulates zonulin expression by inhibiting the MAPK signaling pathway [5:4]. | Inhibits pathogenic translocation (e.g., E. coli), maintains tight junction structure (ZO-1, occludin, claudin-1), and reduces cell apoptosis [5:5]. | Preclinical in vitro & in vivo models [5:6]. | Low (Preclinical) | N/A | [5:7] |
| Bovine Colostrum & Vitamin D | Enhances mucosal immunoglobulins; supports tight junction expression and dampens exertional heat stress-induced barrier leakage [1:29]. | Minimizes exercise-induced increases in intestinal permeability; supports sIgA secretion [1:30]. | Small human RCTs [1:31]. | Moderate | 14 to 28 days | [1:32] |
| Collagen / Collagen Peptides | Provides structural amino acids (glycine, proline, hydroxyproline) to support mucosal extracellular matrix assembly and enterocyte cell division [1:33]. | May support overall mucosal healing and epithelial repair, but direct human evidence for reducing paracellular permeability is sparse [1:34]. | Primarily preclinical models (Insufficient direct human RCTs) | Low (Preclinical / Sparse Human Data) | N/A | [1:35] |
| Polyphenol-Rich Extracts | Upregulates cellular antioxidant defenses, downregulates pro-inflammatory cytokines that drive tight junction disassembly, and promotes beneficial butyrate-producing taxa [1:36]. | Dampens oxidative stress in enterocytes and upregulates claudins and ZO-1; direct clinical outcomes on human paracellular permeability remain exploratory [1:37]. | Extensive preclinical models; small exploratory human clinical trials [1:38]. | Low (Preclinical / Sparse Human Data) | N/A | [1:39] |
Note: In vivo human clinical data is the primary gold standard. Interventions graded "Low (Preclinical)" demonstrate robust cellular and animal proof-of-concept but require validation in large-scale human randomized controlled trials.
¶ Who Benefits Most / Least
¶ 1. Young Adults (Stress & Athletics)
- High Benefit: Young adults undergoing high academic or occupational stress are highly susceptible to CRH-mediated mast cell degranulation, which compromises the barrier [3:11]. This cohort also includes competitive or recreational endurance athletes, who experience transient gut-ischemia (blood flow shunted away from the viscera to skeletal muscle during prolonged exercise), leading to temporary tight junction breakdown and endotoxemia [9:1][1:40].
- Sex Differences: Young women have higher baseline rates of functional gastrointestinal disorders (such as IBS) due to hormonal influences on mast cell activation, estrogen-receptor-mediated modulation of tight junctions, and physiological stress responses [9:2][3:12].
¶ 2. Middle-Aged & Older Adults (Joint Pain & Aging)
- High Benefit: Older adults experience a natural, age-related decline in protective mucin production and are susceptible to immunosenescence (gradual decline in mucosal immune defense) [1:41].
- The NSAID Impact: This demographic has the highest rate of chronic NSAID use for managing age-related joint pain and osteoarthritis. This chronic exposure leads to cumulative, direct mucosal damage and increased paracellular permeability, making targeted barrier-protectant protocols (such as Zinc Carnosine or BPC-157) highly valuable [1:42][4:6].
¶ Prerequisites for Success
- Mitochondrial Health & Energetics: Tight junction reassembly is an active, ATP-dependent process [12:3]. Adequate cellular energy production is a prerequisite; if enterocyte mitochondria are compromised (due to toxicity, severe nutrient deficiencies, or ischemia), barrier-support protocols will exhibit limited efficacy [12:4].
¶ Contexts Where Interventions Fail
- Unmitigated Underlying Stressors: Utilizing L-Glutamine while maintaining heavy daily alcohol intake, high NSAID usage, or unmanaged, severe psychological stress will not yield significant barrier restoration [1:43][4:7][3:13].
- Severe Mechanical Barrier Failure: Functional supplements are completely ineffective when severe, systemic barrier compromise (such as sepsis, necrotizing pancreatitis, or advanced active inflammatory bowel disease) is present [14][6:6][7:1].
¶ How to Try It (Actionable Protocols)
The following protocols are designed for clinical reference and professional education.
¶ Protocol 1: The Lifestyle-First Starter Protocol (2 Weeks)
- Objective: Remove top disruptors to allow natural, physiological tight junction reassembly.
- NSAID Elimination: Restrict non-essential NSAID use. Substitute with non-disruptive alternatives (such as acetaminophen for basic pain management, or systemic anti-inflammatory lifestyle strategies) under clinical supervision [1:44][4:8].
- Stress Management: Implement daily nervous system regulation techniques (such as box breathing, meditation, or clinical biofeedback) to directly block CRH-mediated mast cell degranulation and subsequent barrier leakage [3:14].
- Sleep Regularity: Maintain a consistent 7-to-8 hour sleep schedule to support circadian tight-junction expression [1:45].
¶ Protocol 2: The Standard Barrier Support Protocol (30 Days)
- Objective: Provide essential substrates and direct mucosal protective agents to accelerate healing.
- L-Glutamine: Ingest 5g to 15g daily of pure L-Glutamine powder dissolved in room-temperature water [1:46]. Take on an empty stomach in divided doses (e.g., 5g in the morning, 5g in the evening) to provide steady metabolic fuel for enterocytes [1:47].
- Zinc Carnosine: Take 37.5mg to 75mg twice daily (standard therapeutic dosing) with meals to directly stabilize the mucosal lining and promote epithelial wound repair [1:48].
- Prebiotic Soluble Fiber: Incorporate 5g daily of partially hydrolyzed guar gum (PHGG) or inulin to encourage fermentation by commensal taxa and promote endogenous butyrate production [11:5].
¶ Protocol 3: The Advanced Gut-Microbiome Integration (60 Days)
- Objective: Suppress zonulin pathways and promote long-term epithelial integrity via targeted probiotics and metabolites.
- SCFA-Producing Probiotics: Incorporate probiotic strains known to produce high levels of short-chain fatty acids (such as Bifidobacterium and specific Lactobacillus species) [5:8][11:6].
- Butyrate Supplementation: Ingest 300mg to 600mg of sodium or calcium butyrate daily with meals to directly fuel colonocytes and promote tight-junction gene expression [11:7].
- Essential Amino Acids (EAAs): Add a standardized EAA supplement (providing leucine, isoleucine, and valine) to support enterocyte mitochondrial energetics and cellular repair [12:5].
¶ Alternatives if Protocols Fail
- If standard protocols fail to resolve gut-associated symptoms, clinicians should screen for underlying Small Intestinal Bacterial Overgrowth (SIBO), where excessive bacterial fermentation of prebiotic fibers can worsen abdominal symptoms and maintain local inflammation.
- If mucosal inflammation is suspected, a fecal calprotectin test should be performed to differentiate functional permeability from active, organic inflammatory bowel disease [6:7].
¶ Safety, Interactions, and Clinical Red Flags
¶ Functional Permeability vs. Severe Barrier Failure
It is clinically critical to differentiate minor, functional fluctuations in paracellular permeability (reversible tight junction adjustments) from severe, life-threatening barrier failure.
- Functional Permeability: Transient, subclinical leakage of molecules, typically managed with supportive lifestyle and nutritional strategies [1:49][3:15].
- Severe Barrier Failure: Complete collapse of the physical and immunological barrier. This occurs in clinical emergencies such as septic shock, severe systemic inflammatory response syndrome (SIRS), major mechanical trauma, acute cellular rejection after intestinal transplantation [7:2], or acute graft-versus-host disease (GVHD) [14:1]. In these states, massive translocation of bacteria and endotoxins into the sterile systemic compartment occurs [14:2][7:3].
¶ Clinical Red Flags and Escalation Triggers
The following objective diagnostic signs indicate severe underlying pathology or systemic barrier failure, rather than minor functional permeability. In the presence of any of these symptoms, all experimental barrier support protocols must be discontinued immediately, and standard medical diagnostic protocols must be initiated:
- Severe, Acute, or Localized Abdominal Pain: Indicative of possible bowel obstruction, perforation, or acute surgical abdomen.
- Persistent High Fever (>38.5°C) accompanied by systemic chills or rigors: Strongly indicative of bacterial translocation, bacteremia, or systemic infection [14:3][7:4].
- Gross Blood in Stool: Melena (black, tarry stools) or hematochezia (bright red blood), which signal active, severe mucosal erosion, ulceration, or hemorrhage [6:8].
¶ Drug & Supplement Interactions
- Immunosuppressant Therapies: High-dose L-Glutamine or immunomodulatory supplements should be used with caution in patients undergoing active immunosuppressive therapy (such as post-transplantation or active GVHD management) [14:4][7:5].
- Zinc Accumulation: Standard, long-term high-dose zinc supplementation can induce copper deficiency. Limit zinc carnosine supplementation to recommended clinical durations (typically 4 to 8 weeks) unless copper status is actively monitored.
¶ Tracking & What "Good" Looks Like
¶ Objective Biomarkers
- Lactulose/Mannitol Ratio (L/M Ratio): Repeat the dual-sugar urinary recovery test after 4 to 6 weeks. A reduction in the L/M ratio to <0.03 is the primary objective marker of tight-junction restoration [3:16].
- Fecal Calprotectin: In cases with mild baseline mucosal inflammation, a reduction in fecal calprotectin to <50 μg/g confirms resolved localized inflammatory activity [6:9].
¶ Subjective Metrics
- Stool Consistency: Track using the Bristol Stool Chart. A transition from Type 6/7 (loose/watery) or Type 1/2 (hard/pellet-like) to a consistent Type 3 or 4 (smooth, sausage-like) indicates stabilized transit time and balanced fluid absorption.
- Abdominal Comfort: Decreased postprandial bloating, cramping, and systemic "brain fog" within 2 to 4 weeks [11:8].
¶ Timeline to Benefit and Washout
- Time-to-Benefit: Tight junction protein synthesis and mucosal repair occur rapidly. Clinical improvements in barrier integrity are typically measurable within 10 to 14 days of initiating a targeted L-Glutamine and Zinc Carnosine protocol [1:50].
- Time-to-Washout: Upon cessation of barrier-support nutrients, enterocytes turn over completely every 3 to 5 days. If underlying dietary and lifestyle disruptors (NSAIDs, alcohol, stress) have not been corrected, barrier integrity can degrade back to baseline within 1 week of stopping supplements.
¶ Simple N-of-1 Protocol Template (4-Week A/B Testing)
[ Week 1-2: Phase A (Baseline) ] --> [ Week 3-4: Phase B (Intervention) ]
- Maintain normal diet/lifestyle - Add L-Glutamine (10g/day) + Zinc Carnosine (75mg/day)
- Log daily Bristol stool type - Restrict all non-essential NSAID use
- Rate daily bloating (Scale 1-10) - Maintain stress regulation (10 min daily deep breathing)
- Rate cognitive fatigue / fog - Compare stool, bloating, and fatigue ratings
¶ Common Mistakes & Myths
- Mistake 1: Relying on Commercial "Food Sensitivity" Panels (IgG Tests): Many commercial laboratories offer IgG food sensitivity tests, claiming that elevated IgG antibodies to dozens of foods indicate a "leaky gut" allowing food proteins to leak. Physiological Reality: Serum IgG antibodies to food are completely normal physiological markers of immunological tolerance, not pathological food sensitivities or paracellular permeability.
- Myth 2: "Bone Broth" is a Complete Cure: While bone broth provides glycine and collagen peptides, it lacks the specific molecular potency and clinical evidence of L-Glutamine and Zinc Carnosine. It is a helpful dietary addition but not a primary clinical therapeutic.
- Mistake 3: Treating Permeability While Continuing NSAIDs: Attempting to rebuild the barrier with supplements while continuing a daily regimen of high-dose NSAIDs is biochemically futile, as NSAIDs continuously dismantle the tight junction proteins you are trying to assemble [1:51][4:9].
- Myth 3: "All autoimmune diseases are caused by a leaky gut": Autoimmunity is highly complex and multi-factorial. While transient barrier leakage can play a role in systemic inflammation [8:2], claiming it is the sole, direct cause of all autoimmune conditions is scientifically inaccurate.
¶ Decision Tree (Text-Based)
Are any Clinical Red Flags present?
(Severe pain, fever/chills, gross blood in stool)
/ \
YES NO
/ \
[ DISCONTINUE ALL EXPERIMENTAL ] Is there active chronic NSAID use
[ SUPPLEMENTS IMMEDIATELY ] or heavy alcohol consumption?
[ Standard Clinical Diagnostic ] / \
[ Workup / Sepsis Protocol ] YES NO
/ \
[ Eliminate/Minimize Disruptors ] Are you experiencing
[ Switch pain meds if possible ] chronic high stress?
| / \
| YES NO
| / \
v [ Add mast-cell protocols ] [ Optimize barrier ]
v [ Stress management, DSCG ] [ L-Glutamine, Zinc]
+------------------------------> |
v
[ Implement Standard Protocol ]
[ Glutamine + Zinc Carnosine ]
|
v
Evaluate progress at 4 weeks
(Bristol stool, bloating log)
¶ FAQs (People Also Ask)
¶ Can you heal a leaky gut while still drinking alcohol?
No, it is biochemically difficult to restore the gut barrier while regularly consuming ethanol. Alcohol and its metabolite, acetaldehyde, directly damage enterocyte cell membranes, disrupt the supporting microtubule cytoskeleton, and trigger mast cell degranulation, continuously dismantling tight junctions [1:52][3:17]. Complete cessation or drastic restriction of alcohol is required for successful barrier repair.
¶ Is Apple Cider Vinegar good for intestinal permeability?
There is no direct human clinical evidence demonstrating that apple cider vinegar improves tight junction protein expression or reduces the urinary lactulose-to-mannitol ratio. While it may support gastric acidity in some individuals, it is not an evidence-backed intervention for intestinal permeability.
¶ How does stress physically cause a leaky gut?
Stress triggers the release of corticotropin-releasing hormone (CRH) from the HPA axis [3:18]. CRH binds to specific receptors on mucosal mast cells in the gut, causing them to degranulate and release inflammatory mediators like tryptase and histamine [3:19]. These compounds directly break down tight junction proteins, causing rapid increases in paracellular permeability [3:20].
¶ How long does it take L-Glutamine to restore the gut barrier?
In human clinical trials, L-Glutamine supplementation shows measurable improvements in enterocyte health and paracellular tight-junction seal within 14 to 30 days of consistent, empty-stomach dosing [1:53].
¶ Can children take Zinc Carnosine for intestinal permeability?
While Zinc Carnosine has excellent safety and mucosal protective properties in adults [1:54], clinical pediatric dosing and safety protocols are sparse. Pediatric barrier support must be tailored and monitored by a pediatric gastroenterologist.
¶ Glossary
- Enterocyte: The primary type of simple columnar epithelial cell lining the inner surface of the small and large intestines.
- Paracellular Pathway: The microscopic space and transport pathway between adjacent epithelial cells, regulated by tight junction proteins.
- Transcellular Pathway: The transport pathway directly through the cell membrane and cytoplasm of an epithelial cell.
- Tight Junction (TJ): Highly specialized protein complexes (occludin, claudins, ZO-1) that seal the intercellular space between epithelial cells.
- Lipopolysaccharide (LPS): Large molecules consisting of a lipid and a polysaccharide; major components of the outer membrane of Gram-negative bacteria, highly immunogenic.
- Metabolic Endotoxemia: A state of low-grade, systemic inflammation triggered by elevated levels of circulating bacterial endotoxins (LPS).
- Mast Cell: A type of immune cell containing granules rich in histamine and heparin, heavily involved in stress-induced barrier disruption.
- Lactulose: A large disaccharide sugar probe used in urinary excretion tests; cannot cross an intact intestinal membrane.
- Mannitol: A small monosaccharide sugar probe used in urinary excretion tests; easily crosses healthy cell membranes.
¶ Methods (Transparency)
This deep-dive guide is based on a rigorous, profile-aware evidence search of the PubMed, MEDLINE, and Europe PMC databases conducted up to March 2026.
¶ Inclusion and Exclusion Criteria
- Inclusion: Human randomized controlled trials (RCTs), prospective controlled cohort studies, and high-impact biomedical reviews analyzing tight junction proteins (ZO-1, occludin, claudins), zonulin pathways, and clinical biomarkers.
- Exclusion: Non-peer-reviewed whitepapers, commercial promotional literature, and uncontrolled open-label trials with high risk of bias. Uncorroborated animal models were excluded from the primary human outcomes matrix but utilized where mechanistically relevant (e.g., BPC-157).
¶ Evidence Grading Rubric
- High: Multiple double-blind, placebo-controlled human RCTs with consistent, statistically significant clinical effects.
- Moderate: At least one high-quality human RCT or multiple prospective clinical cohorts with minor limitations.
- Low: Mechanistic hypotheses, preclinical in vitro or animal models, or inconsistent open-label human data.
¶ References
¶ Update Log
- March 30, 2026: Initial release of the comprehensive Intestinal Permeability and Gut Barrier deep-dive guide. Evidence-graded targeted compounds (L-Glutamine, Zinc Carnosine, SCFAs) and deconstructed "leaky gut" commercial pitfalls.
Camilleri M. Human Intestinal Barrier: Effects of Stressors, Diet, Prebiotics, and Probiotics. Clinical and Translational Gastroenterology. 2021. https://pubmed.ncbi.nlm.nih.gov/33492118/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Blöbaum L, Witkowski M, Wegner M, et al. Intestinal Barrier Dysfunction and Microbial Translocation in Patients with First-Diagnosed Atrial Fibrillation. Biomedicines. 2023. https://pubmed.ncbi.nlm.nih.gov/36672684/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Vanuytsel T, van Wanrooy S, Vanheel H, et al. Psychological stress and corticotropin-releasing hormone increase intestinal permeability in humans by a mast cell-dependent mechanism. Gut. 2014. https://pubmed.ncbi.nlm.nih.gov/24153250/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Park JM, Lee HJ, Sikiric P, et al. BPC 157 Rescued NSAID-cytotoxicity Via Stabilizing Intestinal Permeability and Enhancing Cytoprotection. Current Pharmaceutical Design. 2020. https://pubmed.ncbi.nlm.nih.gov/32445447/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Liu Z, Zhang Z, Ni M, et al. Lactobacillus yoelii Lac-2 mediates the mechanism of MAPK signaling pathway involved in the regulation of intestinal barrier and pathogen translocation by Zonulin expression. Scientific Reports. 2026. https://pubmed.ncbi.nlm.nih.gov/42236822/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Górecka A, Jura-Półtorak A, Koźma EM. Biochemical Modulators of Tight Junctions (TJs): Occludin, Claudin-2 and Zonulin as Biomarkers of Intestinal Barrier Leakage in the Diagnosis and Assessment of Inflammatory Bowel Disease Progression. Molecules. 2024. https://pubmed.ncbi.nlm.nih.gov/39407507/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chen Y, Tseng SH, Chen CY. Application of Intestinal Barrier Molecules in the Diagnosis of Acute Cellular Rejection After Intestinal Transplantation. Transplant International. 2023. https://pubmed.ncbi.nlm.nih.gov/37745643/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
García-Studer A, Mucientes A, Lisbona-Montañez JM. Association between intestinal permeability, systemic inflammation, and response to anti-TNF therapy in patients with rheumatoid arthritis: a prospective controlled study. Frontiers in Immunology. 2026. https://pubmed.ncbi.nlm.nih.gov/41972162/ ↩︎ ↩︎ ↩︎
Russo F, Bianco A, Prospero L. Physical capacity modulates intestinal barrier dysfunction in functional disorders: phenotype-specific patterns in fibromyalgia and irritable bowel syndrome. Frontiers in Physiology. 2025. https://pubmed.ncbi.nlm.nih.gov/41234694/ ↩︎ ↩︎ ↩︎
Power N, Turpin W, Espin-Garcia O, et al. Serum Zonulin Measured by Commercial Kit Fails to Correlate With Physiologic Measures of Altered Gut Permeability in First Degree Relatives of Crohn's Disease Patients. Frontiers in Physiology. 2021. https://pubmed.ncbi.nlm.nih.gov/33841181/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Li E, Wang J, Guo B. Effects of short-chain fatty acid-producing probiotic metabolites on symptom relief and intestinal barrier function in patients with irritable bowel syndrome: a double-blind, randomized controlled trial. Frontiers in Cellular and Infection Microbiology. 2025. https://pubmed.ncbi.nlm.nih.gov/40575487/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Spataro L, Ragni M, Segala A, et al. Essential amino acids preserve intestinal barrier integrity via mitochondrial protection in obesity and gut inflammation. Frontiers in Pharmacology. 2025. https://pubmed.ncbi.nlm.nih.gov/41415575/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Silva AA, Queiroz VAV, de Lana VS, et al. Physicochemical properties and metabolic effects of cowpea protein isolate. Food Research International. 2026. https://pubmed.ncbi.nlm.nih.gov/41942185/ ↩︎ ↩︎ ↩︎ ↩︎
Rimondi E, Melloni E, Secchiero P. Targeting Intestinal Permeability for Graft-versus-Host Disease Treatment: A Therapeutic Perspective with Defibrotide. Journal of Experimental Pharmacology. 2025. https://pubmed.ncbi.nlm.nih.gov/40927405/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎