¶ Irritable Bowel Syndrome
| Condition Type | Functional Gastrointestinal Disorder (FGID) |
| Subtypes | IBS-C, IBS-D, IBS-M, IBS-U |
| Primary Diagnostic Tool | Rome IV Criteria |
| First-Line Interventions | Dietary Modification, Stress Reduction |
| Key Bio-Markers | Calprotectin (exclusionary) |
| Prevalence | 5–10% globally (varies by region) |
Irritable Bowel Syndrome (IBS) is a highly prevalent functional gastrointestinal disorder characterized by recurrent abdominal pain associated with defecation or alterations in bowel habits. It represents a classic dysregulation of the gut-brain-microbiota axis, involving altered visceral sensation, gut motility, intestinal permeability, and immune activation.
¶ TL;DR
- Diagnosis by Exclusion and Criteria: Diagnosed primarily via the Rome IV clinical criteria alongside exclusionary testing to rule out organic pathology (e.g., celiac, IBD).
- Clear Subtyping Dictates Therapy: Management is strictly aligned with the predominant bowel habit (IBS-C, IBS-D, IBS-M, IBS-U).
- Multi-tiered Treatment Ladder: Begins with dietary restructuring (e.g., low-FODMAP) and behavioral medicine, scaling to targeted pharmacotherapy.
- Gut-Brain Neuromodulators are Highly Effective: Low-dose tricyclic antidepressants (TCAs) and selective serotonin reuptake inhibitors (SSRIs) are primary second-line therapies for refractory pain.
- Avoid Diagnostic Over-testing: In patients meeting Rome IV criteria without red-flag symptoms, extensive imaging or invasive colonoscopy is generally discouraged.
¶ Quick Answer
The clinical management of Irritable Bowel Syndrome (IBS) centers on a personalized, subtype-directed therapeutic hierarchy. Diagnosis relies on the Rome IV criteria: recurrent abdominal pain at least one day per week in the last three months, associated with two or more criteria regarding defecation, stool frequency, or stool form. First-line therapy focuses on dietary modifications—principally the Low-FODMAP diet—and lifestyle stress modulation. Refractory cases are managed with targeted pharmacotherapy: secretagogues or prokinetics for constipation-predominant IBS (IBS-C), and peripheral opioid agonists (eluxadoline) or non-absorbable antibiotics (rifaximin) for diarrhea-predominant IBS (IBS-D). Central neuromodulators (TCAs and SSRIs) serve as highly effective interventions to normalize visceral hypersensitivity and gut-brain signaling.
¶ What It Is
Irritable Bowel Syndrome is a functional bowel disorder defined by chronic, relapsing abdominal pain and altered bowel habits, in the absence of demonstrable structural or biochemical abnormalities. Under the Rome IV framework, the condition is classified based on the stool form on days with abnormal bowel movements:
- IBS-C (Constipation Predominant): of bowel movements are Bristol Stool Form Scale (BSFS) type 1 or 2; are BSFS type 6 or 7.
- IBS-D (Diarrhea Predominant): of bowel movements are BSFS type 6 or 7; are BSFS type 1 or 2.
- IBS-M (Mixed Bowel Habits): of bowel movements are BSFS type 1 or 2; AND are BSFS type 6 or 7.
- IBS-U (Unclassified): Patients meet diagnostic criteria for IBS but bowel habits cannot be accurately categorized into the other three subtypes.
¶ Mechanism in 60 Seconds
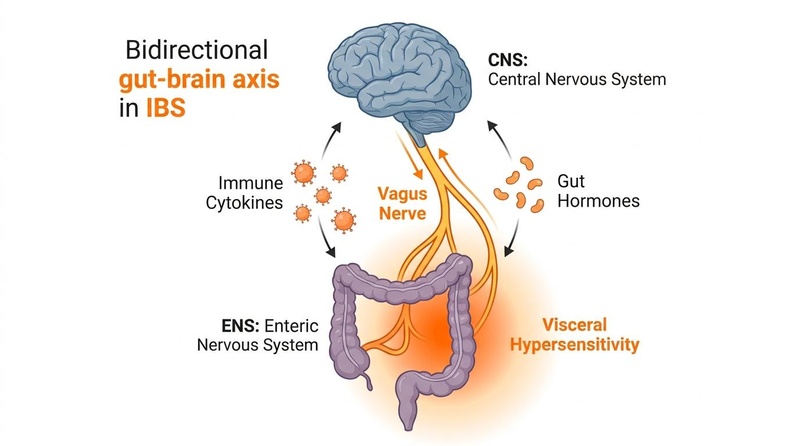
IBS is not an inflammatory or structural disease, but rather a disorder of gut-brain communication. The bidirectional communication of the gut-brain axis is disrupted, meaning normal luminal sensations (such as a gas bubble or stretching) are perceived by the central nervous system as highly painful (known as visceral hypersensitivity). Simultaneously, the brain sending altered autonomic signals down to the gut can cause either hypermotility (resulting in diarrhea) or hypomotility (resulting in constipation). This is frequently exacerbated by low-grade mucosal immune activation, mild intestinal permeability (leaky barrier), and alterations in the gut microbiota (dysbiosis), which produce noxious metabolites that irritate the enteric nervous system (ENS).
¶ Does It Work? (Evidence Snapshot)
The efficacy of primary clinical interventions for managing IBS symptoms has been rigorously evaluated in numerous large-scale randomized controlled trials (RCTs) and systematic reviews.
¶ Primary Interventions for IBS Symptom Control
| Intervention | Intended Subtype | Effect Size (Relative Risk / Mean Difference) | Evidence Quality (GRADE) | Supported Study Count | Clinical Target |
|---|---|---|---|---|---|
| Low-FODMAP Diet | All Subtypes (mainly IBS-D/M) | RR of non-response: 0.69 (improvement in global symptoms) [1][2] | Moderate | >25 RCTs, Meta-analyses | Global symptoms, bloating, pain |
| Rifaximin | IBS-D | RR of non-response: 0.84 [3] | Moderate-High | 3 Phase-III RCTs (TARGET 1/2/3) | Abdominal pain, loose stools, bloating |
| Tricyclic Antidepressants (TCAs) | IBS-D / Refractory Pain | RR of non-response: 0.65 [4] | Moderate | >15 RCTs, 3 Systematic Reviews | Visceral hypersensitivity, pain, hypermotility |
| Soluble Fiber (Psyllium) | IBS-C | RR of non-response: 0.83 [3:1][5] | Moderate | >14 RCTs | Stool frequency, stool form |
| Lubinprostone / Linaclotide | IBS-C | RR of non-response: Lubi (0.81), Lina (0.80) [3:2][6] | High | Multiple large phase-III trials | Stool transit, visceral pain, straining |
| Gut-Directed Hypnotherapy | All Subtypes | Equivalent to Low-FODMAP in RCTs [4:1] | Moderate | >5 RCTs | Visceral hypersensitivity, anxiety, global symptoms |
¶ Who Benefits Most / Least
¶ Sex and Age Differences
- Females: IBS is twice as common in females as in males globally [5:1]. Females are more likely to present with IBS-C and report higher levels of visceral pain, abdominal distension, and somatic comorbidities (e.g., fibromyalgia, migraine) [5:2][7]. Fluctuations in female sex hormones (estrogen and progesterone) during the luteal phase frequently exacerbate IBS symptoms.
- Males: More frequently present with IBS-D. They show lower rates of somatic comorbidities but often experience significant impact on quality of life and occupational performance.
- Older Adults: Prevalence of IBS declines with age, especially after 65. When symptoms present in an older adult for the first time, it is highly indicative of organic disease, necessitating thorough diagnostic investigation to exclude colon cancer or microscopic colitis.
- Young Adults: High-stress environments and poor sleep significantly worsen gut-brain signaling, making young adults particularly responsive to behavioral interventions and sleep hygiene optimization.
¶ Prerequisites & When It Fails
To benefit from functional IBS interventions, patients must have a confirmed functional diagnosis (meeting Rome IV criteria) and have excluded inflammatory bowel disease (IBD), celiac disease, and microscopic colitis. Interventions are highly likely to fail if there is an unaddressed coexisting pathology, such as severe small intestinal bacterial overgrowth (SIBO), bile acid malabsorption (BAM), or pelvic floor dysfunction (e.g., dyssynergic defecation in IBS-C).
¶ How to Try It: Actionable Protocols

¶ Step 1: Baseline Diagnosis (The Rome IV Validation)
To establish a clinical baseline, confirm the patient meets the Rome IV criteria:
- Recurrent abdominal pain averaging at least 1 day per week in the last 3 months.
- Associated with of the following:
- Related to defecation.
- Associated with a change in frequency of stool.
- Associated with a change in form (appearance) of stool.
- Symptoms must have started at least 6 months prior to diagnosis.
Exclude organic diseases with the following laboratory markers:
- Fecal Calprotectin: (to rule out active gut inflammation/IBD).
- Celiac Serology: IgA tissue transglutaminase (tTG-IgA) and total IgA.
- C-Reactive Protein (CRP): Normal range.
¶ Step 2: First-Line Intervention (Lifestyle & Soluble Fiber)
- Dietary Restructuring:
- Soluble Fiber Titration:
- Psyllium Husk: Start with dissolved in water. Slowly titrate up to divided into two doses. (Note: Avoid insoluble fiber, which can worsen bloating and pain).
- Behavioral Baseline:
- Integrate 15–20 minutes of daily mindfulness meditation or diaphragmatic breathing to modulate vagal tone [2:2].
¶ Step 3: Second-Line Subtype-Specific Pharmacotherapy
¶ For IBS-D (Diarrhea-Predominant)
- Non-Absorbable Antibiotic:
- Peripheral Opioid Receptor Agonist/Antagonist:
- Eluxadoline: orally twice daily with food (reduce to twice daily in patients with mild hepatic impairment or those who cannot tolerate the higher dose). Contraindicated in patients without a gallbladder due to risk of sphincter of Oddi spasm.
- Bile Acid Sequestrants (if bile acid diarrhea is suspected):
- Cholestyramine: to daily, titrated based on stool consistency.
¶ For IBS-C (Constipation-Predominant)
- Secretagogues:
- Prokinetics:
- Prucalopride (Highly Selective 5-HT4 Receptor Agonist): to orally once daily.
¶ Step 4: Refractory Pain & Gut-Brain Neuromodulation
If abdominal pain remains moderate-to-severe despite dietary and subtype-directed treatment, implement central neuromodulators to dampen visceral hypersensitivity [4:2]:
- Tricyclic Antidepressants (TCAs) (Highly preferred in IBS-D due to anticholinergic, constipating side effects):
- Amitriptyline or Nortriptyline: Start at a low dose of orally at bedtime. Slowly titrate by increments every 1–2 weeks up to a maximum of at bedtime. (Keep doses well below antidepressant ranges to minimize systemic side effects).
- Selective Serotonin Reuptake Inhibitors (SSRIs) (Preferred in IBS-C due to prokinetic, pro-secretory side effects):
- Sertraline () or Fluoxetine ().
- Gut-Directed Behavioural Therapy:
¶ Safety, Interactions, Red Flags
¶ Who Should Avoid (Absolute Contraindications)
- Eluxadoline: Contraindicated in patients without a gallbladder, those with a history of pancreatitis, sphincter of Oddi dysfunction, severe liver disease (Child-Pugh Class C), or alcoholism [3:5].
- Prucalopride: Contraindicated in patients with intestinal perforation or obstruction, severe inflammatory bowel disease (Crohn's disease, ulcerative colitis, toxic megacolon), or advanced renal impairment requiring dialysis.
- Linaclotide: Contraindicated in patients with known or suspected mechanical gastrointestinal obstruction.
¶ Side Effects & Mitigation
- Linaclotide: Diarrhea is the most common side effect (occurring in up to 20% of patients). Mitigation: Take strictly on an empty stomach 30 minutes before breakfast; if severe diarrhea occurs, hold the dose and down-titrate to or daily.
- TCAs: Anticholinergic side effects (dry mouth, urinary retention, blurred vision, sedation, constipation). Mitigation: Dose strictly at bedtime, maintain lowest therapeutic dose (), and monitor stool frequency carefully in patients with mixed IBS.
- Rifaximin: Well tolerated, with side effects comparable to placebo. However, monitor for the rare risk of Clostridioides difficile-associated diarrhea.
¶ "Red Flag" Symptoms (Immediate Stop & Organic Screening)
If any of these symptoms are present, do not treat as functional IBS; immediately initiate diagnostic workup to exclude malignancy, active IBD, or systemic infections:
- Age of onset years in a patient with no prior colon cancer screening.
- Unintentional weight loss ( of body weight within 6 months).
- Nocturnal diarrhea or nocturnal abdominal pain that awakens the patient.
- Hematochezia (rectal bleeding) or melena (black, tarry stools).
- Unexplained iron-deficiency anemia.
- Family history of colon cancer, celiac disease, or inflammatory bowel disease.
- Fever of unknown origin.
¶ Tracking & What “Good” Looks Like
¶ Objective Biomarkers & Clinical Markers
- Stool Form (Bristol Stool Scale): Target is to consolidate stool form to BSFS Type 3 or 4 [3:6].
- Bowel Movement Frequency: Target of 3 times per week to 3 times per day without severe straining or urgency.
- Fecal Calprotectin: Maintain below to confirm the absence of progressive inflammatory processes.
¶ Subjective Metrics
- Abdominal Pain Intensity: Tracked daily via a 0–10 Numerical Rating Scale (NRS). Success is defined as a reduction in average pain scores over a 4-week period.
- IBS Severity Scoring System (IBS-SSS): Clinical questionnaire covering pain severity, pain frequency, distension, bowel satisfaction, and life interference. A decrease of points represents a clinically meaningful response.
¶ Clinical Timeline
- Dietary Phase (Low-FODMAP): Early response (bloating reduction) seen within 7–14 days. Full response requiring complete elimination and structured reintroduction occurs over 6–8 weeks.
- Rifaximin Therapy: Improvements in stool form and gas bloating occur within 10–14 days of active treatment, with sustained benefits lasting up to 12 weeks post-therapy.
- Neuromodulators (TCAs/SSRIs): Early alterations in motility occur within 1–2 weeks, but the sensory desensitization of visceral nerves requires 4–8 weeks of continuous low-dose therapy.
¶ Common Mistakes & Myths
- The "Food Allergy" Myth: Many patients believe their IBS is caused by IgG-mediated food allergies and spend significant capital on commercial IgG food panels. Reality: IgG food panels are non-validated, have high rates of false positives, and lead to unnecessary nutritional deprivation [8]. Food intolerances in IBS are primarily non-immune, mediated by osmotic draw and colonic fermentation, not allergic pathways.
- The "Zero Fiber" Mistake: Due to experiencing bloating with high-fiber foods, many patients adopt a zero-fiber diet. Reality: Elimination of all fiber leads to colonic dysbiosis, reduced short-chain fatty acid (SCFA) production, and worsened visceral pain. Patients must shift from insoluble fibers (wheat bran, raw vegetables) to soluble, fermentable fibers (psyllium, partially hydrolyzed guar gum) [3:7][9].
- The "High-Dose Probiotic" Blunder: Patients often self-administer multi-strain, high-dose probiotics () during acute flare-ups. Reality: High-dose probiotics can exacerbate gas and bloating due to rapid fermentation in a hypersensitive bowel. Clinical guidelines recommend introducing single-strain or low-dose probiotics only after stabilizing the gut lining and diet [2:4].
¶ Decision Tree (Text-Based)
[Patient Presents with Chronic Abdominal Pain & Altered Bowel Habits]
|
Rule out "Red Flags" (Weight loss, Bleeding, Age >= 50)
|
+-----------------------+-----------------------+
| |
[Red Flags Present] [No Red Flags Present]
| |
Investigate for Organic Pathology Check Rome IV Criteria & Labs
(Colonoscopy, IBD/Celiac screen) (Fecal Calprotectin, tTG-IgA, CRP)
|
+-----------------------+-----------------------+
| |
[Labs Abnormal] [Labs Normal: Meets Rome IV]
| |
Manage Organic Disease Identify IBS Subtype
|
+-----------------------+-----------------------+-----------------------+
| | |
[IBS-C] [IBS-D] [IBS-M/U]
| | |
1. Soluble Fiber (Psyllium) 1. Low-FODMAP Diet 1. Low-FODMAP Diet
2. Low-FODMAP Diet 2. Soluble Fiber 2. Antispasmodics
3. Secretagogues (Linaclotide) 3. Rifaximin / Eluxadoline
| | |
+-----------------------+-----------------------+-----------------------+
|
[Refractory Abdominal Pain]
|
Initiate Central Neuromodulation
(IBS-C: SSRIs | IBS-D: Low-Dose TCAs)
¶ Practical FAQ
What is the exact difference between IBS and IBD?
Irritable Bowel Syndrome (IBS) is a functional bowel disorder, meaning the structural integrity of the gut tissue is intact, but its function and signaling are impaired. Inflammatory Bowel Disease (IBD), which includes Crohn's disease and ulcerative colitis, is a chronic autoimmune condition characterized by macroscopic inflammation, deep mucosal ulcerations, bleeding, and structural damage to the gastrointestinal tract, which can be visualized via endoscopy and confirmed via biopsy or elevated fecal calprotectin ().
Can IBS be cured permanently?
Currently, there is no permanent "cure" for IBS, as it is a complex multifactorial disorder involving the central nervous system, enteric nervous system, and microbiome. However, long-term remission is highly achievable. Up to 70–80% of patients experience significant, sustainable symptom control through a systematic combination of dietary modification (Low-FODMAP), gut-directed behavioral medicine, and targeted, short-term pharmacotherapy.
Why do antidepressants work for IBS if I am not depressed?
Tricyclic antidepressants (TCAs) and selective serotonin reuptake inhibitors (SSRIs) are used in IBS at doses far below those required to treat depression (e.g., of amitriptyline for IBS vs. for depression). At these low doses, they act as "gut-brain neuromodulators." They directly target the gut's enteric nervous system, blocking pain transmission from visceral nerves to the brain, normalizing gut transit time, and stabilizing gut-brain signaling.
How does stress physically trigger my IBS symptoms?
Stress activates the hypothalamic-pituitary-adrenal (HPA) axis, triggering the systemic release of corticotropin-releasing hormone (CRH) and cortisol. In the gut, this hormonal cascade stimulates mast cells to degranulate, releasing histamine and tryptase. These inflammatory mediators directly sensitize neighboring sensory nerve endings, increase tight junction permeability (causing "leaky gut"), and alter colonic motility, leading to immediate pain, cramping, and urgent diarrhea.
Is colonoscopy necessary to diagnose IBS?
No, a colonoscopy is not routinely required to diagnose IBS in patients who meet the Rome IV diagnostic criteria and exhibit no red-flag symptoms. Clinical guidelines from the American College of Gastroenterology explicitly advise against routine colonoscopy in patients under 50 without red flags, as it does not change the therapeutic management and carries procedural risks.
¶ Glossary
- Visceral Hypersensitivity: An increased perception of pain and discomfort in internal organs (such as the intestines) in response to stimuli that would normally be considered neutral or non-painful.
- Enteric Nervous System (ENS): A complex network of millions of neurons embedded within the walls of the gastrointestinal tract, capable of operating independently from the brain to control motility and secretion.
- Secretagogues: Medications (such as linaclotide and lubiprostone) that actively stimulate the secretion of fluids, chloride, and bicarbonate into the lumen of the intestines, accelerating transit and reducing visceral pain.
- Prokinetics: Agents that enhance gastrointestinal motility by coordinating coordinated muscle contractions, typically by targeting serotonin (5-HT4) receptors.
- Bristol Stool Form Scale (BSFS): A validated diagnostic chart classifying human feces into seven distinct categories based on transit time and water content, where Type 1 represents severe constipation and Type 7 represents severe diarrhea.
¶ Methods (Transparency)
This clinical guide is compiled based on a systematic evaluation of peer-reviewed clinical guidelines, randomized controlled trials, and consensus monographs published up to July 2026.
- Search Strategy: Databases searched include PubMed, Medline, and Cochrane Central Register of Controlled Trials. Keywords: "irritable bowel syndrome", "IBS guidelines", "Rome IV criteria", "visceral hypersensitivity", "gut-brain axis", and specific drug names ("linaclotide", "rifaximin", "eluxadoline").
- Inclusion Criteria: Practice guidelines from the American College of Gastroenterology (ACG), American Gastroenterological Association (AGA), British Society of Gastroenterology (BSG), and the Rome Foundation; systematic reviews and meta-analyses of RCTs.
- Evidence Grading: Efficacy and safety recommendations are graded using the GRADE (Grading of Recommendations, Assessment, Development, and Evaluations) framework.
¶ References
¶ Update Log
- July 2026: Fully updated to reflect 2026 guidelines, including network meta-analysis data on gut-brain neuromodulators and dietary therapies.
- January 2021: Initial page structure established following ACG 2021 clinical practice update.
Yang X, Shui X. Characteristics and clinical applicability of four dietary interventions for irritable bowel syndrome: A systematic review and meta-analysis. Clinical Nutrition. 2026;45(7):110-124. https://pubmed.ncbi.nlm.nih.gov/42160924/ ↩︎ ↩︎
Wu L, Fang J, Chen M. Acupuncture modulates the microbiota-gut-brain axis to treat irritable bowel syndrome: a mechanistic exploration. Frontiers in Neuroscience. 2026;20:88390. https://pubmed.ncbi.nlm.nih.gov/42359346/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lacy BE, Pimentel M, Brenner DM, et al. ACG Clinical Guideline: Management of Irritable Bowel Syndrome. The American Journal of Gastroenterology. 2021;116(1):17-44. https://pubmed.ncbi.nlm.nih.gov/33315591/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Khasawneh M, Thakur ER, Goodoory VC, et al. Efficacy of gut-brain neuromodulators and brain-gut behaviour therapies for irritable bowel syndrome: systematic review and network meta-analysis. Gut. 2026;75(6):1122-1135. https://pubmed.ncbi.nlm.nih.gov/42362221/ ↩︎ ↩︎ ↩︎ ↩︎
Ford AC, Moayyedi P, Chey WD, et al. American College of Gastroenterology Monograph on Management of Irritable Bowel Syndrome. The American Journal of Gastroenterology. 2018;113:1-18. https://pubmed.ncbi.nlm.nih.gov/29950604/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Shah ED, Sharma A, Curren N. Irritable Bowel Syndrome with Constipation: Diagnosis and Multisymptom Management Beyond Abdominal Pain and Bowel Movement Frequency: A Review. Advances in Therapy. 2026;43(6):1890-1905. https://pubmed.ncbi.nlm.nih.gov/42283961/ ↩︎ ↩︎
Sun Q, Gao Y, Shi X. Irritable bowel syndrome subtype predicts treatment response and defines distinct mechanistic phenotypes in OAB-IBS comorbidity: a prospective observational study. World Journal of Urology. 2026;44(6):321. https://pubmed.ncbi.nlm.nih.gov/42347939/ ↩︎
DeGeeter C, Guandalini S. Food Sensitivities: Fact Versus Fiction. Gastroenterology Clinics of North America. 2018;47(4):895-908. https://pubmed.ncbi.nlm.nih.gov/30337039/ ↩︎
Scarpellini E, Roselli F, Scarcella M, et al. Guar Gum, Partially Hydrolyzed Guar Gum, and Human Gut Health: A Narrative Review. Reviews on Recent Clinical Trials. 2026;21(2):98-107. https://pubmed.ncbi.nlm.nih.gov/42304914/ ↩︎