¶ Light Environment
The circadian light environment represents the premier external entrainment signal (zeitgeber) coordinating mammalian physiology. In modern industrial societies, the natural 24-hour solar cycle of high-intensity, short-wavelength blue light by day and near-total darkness by night has been replaced by a low-amplitude, fragmented, and constant artificial light regime. This comprehensive guide details the clinical, biological, and practical dimensions of designing a healthy 24-hour light architecture to optimize circadian alignment, autonomic balance, sleep quality, and healthy aging.
| Parameter | Clinical Guideline & Target Values |
|---|---|
| Primary Biological Sensor | Intrinsically photosensitive retinal ganglion cells (ipRGCs) expressing melanopsin (, peak sensitivity ) [1][2] |
| Daytime Target | High-intensity light ( natural daylight or high-lux full-spectrum white light) within 30 minutes of waking [3][4] |
| Evening Target | Dim, long-wavelength amber/red light ( at eye level, removing wavelengths ) [5][6] |
| Nighttime Target | Near-total darkness ( or complete optical blackout) [7][8] |
| Major Biomarkers | Melatonin suppression, Cortisol Awakening Response (CAR), salivary alpha-amylase (sAA), Heart Rate Variability (HRV) [4:1][9] |
| Clinical Benefits | Optimizes sleep latency, improves motor memory consolidation, reduces risk of age-related cognitive decline [10][11] |
¶ Safety "Traffic Light"
- RED (Do NOT do): Intense exposure to short-wavelength blue light () in the 2 hours before habitual sleep onset, which causes immediate and profound melatonin suppression [2:1][4:2]. Avoid constant 24-hour lighting which degrades core clock proteins and causes complete behavioral arrhythmia [12].
- AMBER (Use caution): Reliance on commercial "blue-blocking" software or spectacles without verifying actual spectral transmission; many leave up to 80% of melanopic-activating light intact [13][14].
- GREEN (Go/Recommend): High-lux morning light within 30 minutes of waking, progressive afternoon/evening dimming, and complete darkness during the nocturnal sleep window [1:1][3:1][6:1].
¶ The 24-Hour Protocol Matrix
| Phase | Timeframe | Spectral Target | Lux Target | Duration | Primary Biological Goal |
|---|---|---|---|---|---|
| 1. Morning Anchor | 0--2h post-wake | Cool blue-enriched white () | >10,000\text | 10--30 min | Reset SCN pacemaker; stimulate Cortisol Awakening Response (CAR) [3:2][9:1] |
| 2. Midday Stabilization | 2--8h post-wake | Full-spectrum broad daylight | (indoor) | Continuous | Stabilize peripheral clocks; enhance daytime cognitive performance [9:2] |
| 3. Evening Transition | 8--16h post-wake | Long-wavelength warm amber/red () | at eye | Progressive | Initiate Dim Light Melatonin Onset (DLMO); prevent sleep-phase delay [5:1][11:1] |
| 4. Nocturnal Blackout | 16--24h post-wake | Near-total optical blackout (red light only if needed) | <0.1\text | 7--9 hours | Support melatonin amplitude; prevent REM/slow-wave sleep fragmentation [7:1][8:1] |
¶ Bottom Line
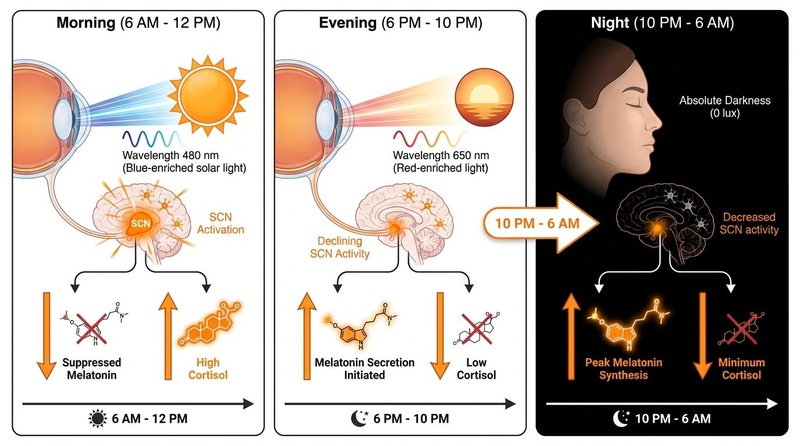
The circadian system requires high amplitude: bright, short-wavelength light during the day to suppress melatonin and anchor alertness, and complete darkness at night to facilitate cellular repair. Chronic low-amplitude environments lead to fragmented sleep-wake cycles, neuroendocrine dysregulation, and elevated long-term risks of metabolic, cardiovascular, and cognitive disorders [1:2][8:2][15].
¶ 1. What Is the Circadian Light Environment?
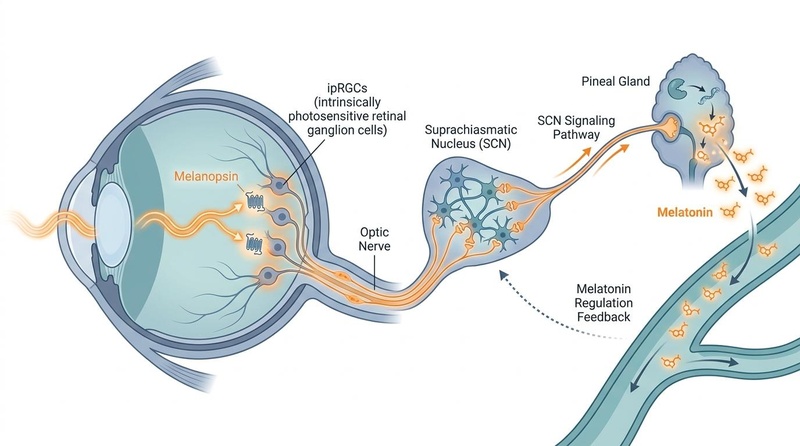
The term circadian light environment describes the total optical radiation (wavelength, intensity, timing, and duration) received by an organism over a 24-hour cycle. Unlike the visual system, which detects shapes and motion via rod and cone photoreceptors, the circadian system relies primarily on a specialized population of non-imaging photoreceptors: intrinsically photosensitive retinal ganglion cells (ipRGCs) [1:3][2:2].
These cells express the photopigment melanopsin (OPN4), which is directly activated by short-wavelength blue light, peaking specifically around [2:3][3:3]. Once stimulated, ipRGCs transmit signals via the retinohypothalamic tract (RHT) directly to the suprachiasmatic nucleus (SCN) of the hypothalamus—the master pacemaker of mammalian circadian rhythms [3:4][4:3]. The SCN then orchestrates the downstream rhythmic release of systemic signals, most notably inhibiting the secretion of melatonin from the pineal gland during periods of bright light exposure [4:4][6:2].
In the natural evolutionary environment, daylight provides up to of broad-spectrum illumination, while the evening environment provides only dim, long-wavelength firelight ( at ) followed by near-total darkness at night. Conversely, the modern light environment is highly fragmented, characterized by low-lux indoor working environments (), intensive screen use in the evening, and chronic outdoor and indoor light pollution at night (artificial light at night, or ALAN) [7:2][8:3].
¶ 2. Morning Light: Resetting the central Pacemaker
Exposing the eyes to high-intensity, blue-enriched light during the early subjective day acts as a powerful phase-advance signal, resetting the SCN pacemaker and shifting the biological sleep window earlier [1:4][11:2].
¶ Normalizing the Cortisol Awakening Response (CAR)
In healthy individuals, free cortisol begins to rise prior to waking and peaks approximately 30 to 45 minutes after eye opening. High-lux morning light stabilizes this cortisol slope, promoting a sharp, clean CAR peak which is strongly correlated with improved morning alertness, metabolic activation, and cognitive performance [9:3]. Conversely, a flattened CAR slope is associated with chronic fatigue, depression, and circadian misalignment [9:4][16].
¶ Gender-Specific Responses and daylight Spectrum
Recent research shows that light history and the spectral quality of daytime daylight have distinct impacts based on sex. A clinical study in 2025 demonstrated that reducing daytime daylight intensity and altering its spectrum (attenuating short-wavelength daylight up to ) degraded sleep parameters and increased morning sleepiness only in female participants [9:5]. Additionally, morning salivary cortisol is naturally higher in females, showing heightened sensitivity to daylight spectrum variations [9:6].
¶ Glymphatic System Activation & Mood
Emerging clinical neuroimaging reveals a direct connection between bright morning light and brain clearance pathways. A 2026 randomized controlled trial demonstrated that bright morning light therapy directly influences glymphatic system function—the brain's metabolic waste clearance network—in individuals with subthreshold depression, promoting a significant reduction in neuroinflammatory markers and a parallel improvement in clinical depression and anhedonia scores [16:1].
¶ 3. Evening Light: Preserving Melatonin & Occupational Risks
As the biological day ends, the SCN prepares to initiate melatonin synthesis (Dim Light Melatonin Onset, or DLMO). Melatonin is the primary neuroendocrine coordinator of nocturnal physiology, facilitating cellular antioxidant defense, mitochondrial repair, and deep sleep architecture [2:4][11:3].
¶ The Phase-Delay Phenomenon in Adolescents
Exposure to even dim levels of short-wavelength light () in the evening suppresses melatonin synthesis and induces a phase delay. This delays sleep onset, increases sleep latency, and impairs subsequent morning performance [5:2][11:4]. Controlled studies in adolescents show that late afternoon and early evening light exposure dramatically suppresses subsequent melatonin levels, compounding the natural biological phase-delay of puberty [5:3]. Overnight motor memory consolidation is tightly coupled to this timing, with adolescent sleep restriction and subsequent DLMO shifts directly degrading memory retention [11:5].
¶ Occupational Impacts: Night Shift Workers & NICU Nurses
The clinical consequences of evening and nighttime light exposure are highly pronounced in shift-working cohorts:
- Night Shift Nurses: Hong Kong nurses on night shifts show severe circadian rest-activity fragmentation and degraded sleep health, highly correlated with real-time occupational noise and light exposure [15:1]. Mixed-methods clinical evaluations highlight sleep debt and circadian strain as primary occupational hazards [17].
- NICU Phototherapy Exposure: Neonatal intensive care unit (NICU) nurses suffer from degraded sleep quality due to occupational exposure to blue light emitted from infant phototherapy devices () during night shifts, which directly suppresses their endogenous melatonin synthesis [18].
¶ 4. Screen Light & Digital Devices
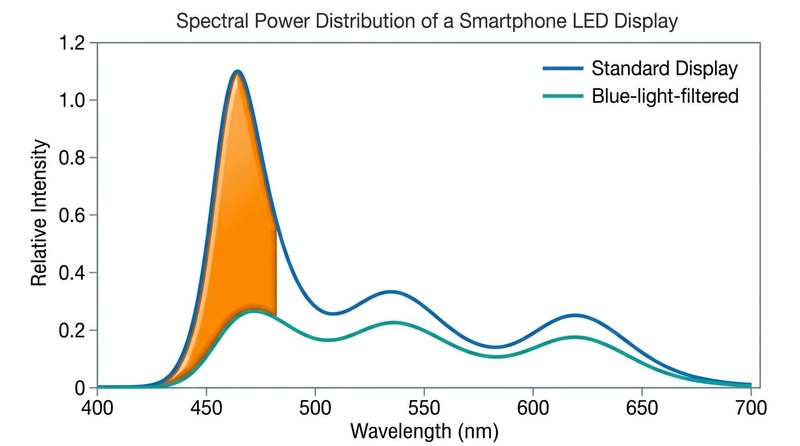
Modern displays (smartphones, tablets, and computer monitors) rely on light-emitting diodes (LEDs) that emit a concentrated spike of high-energy visible (HEV) blue light, typically centered around , which heavily overlaps with the peak sensitivity of melanopsin [2:5][13:1].
¶ Screen-Induced Sleep Dysfunction
Clinical cohorts demonstrate that daily smartphone and tablet usage immediately before bedtime significantly degrades sleep. In toddlers, daily tablet/smartphone usage raises the odds of shorter total sleep time (OR 1.95) and significantly longer sleep onset latency (OR 2.44), independent of confounding factors like traditional TV watching or baseline temperament [10:1]. In young adults and elite athletes, evening smartphone exposure increases subjective sleepiness latency, decreases rapid eye movement (REM) sleep duration, and compromises next-day cognitive and physical athletic performance [19][20].
¶ Technological Mitigation: LCD vs. OLED
Display technology dictates the severity of blue-light emission:
- Liquid Crystal Displays (LCDs): Conventional LCD screens utilize intense blue LED backlights filtered through liquid crystal layers, emitting a wide and intense blue light peak around .
- Organic Light-Emitting Diodes (OLEDs): OLED displays utilize self-emitting pixels. Clinical evaluations show that evening exposure to OLED screens produces significantly less melatonin suppression and less sleep disruption compared to equivalent-brightness LCD screens, because OLED spectral emissions feature a narrower blue peak shifted slightly away from the melanopsin peak (closer to ) and up to 50% lower total blue light energy output [21][22].
¶ Efficacy of Filtering Applications & Spectacles
- Software-Based Filters (Night Mode): Software filters adjust screen color temperature toward the warm spectrum, reducing the intensity of blue light. However, observational and clinical trials show that while these applications improve subjective visual comfort and eye strain, they do not consistently improve objective actigraphic sleep quality parameters (such as sleep efficiency or total sleep time) [14:1][23]. This is because the overall brightness (lux) of the screen remains high enough to activate ipRGCs even when shifted to warmer spectrums.
- Physical Blue-Blocking Lenses: High-quality physical glasses designed to block 100% of wavelengths below are highly effective. A systematic review and meta-analysis of randomized controlled trials demonstrated that wearing blue-blocking glasses in the evening significantly improves actigraphic sleep outcomes, increases sleep efficiency, and restores natural melatonin profiles compared to placebo or partial blue-blockers [24][25].
¶ 5. Bedroom Darkness & Nocturnal Sleep Space
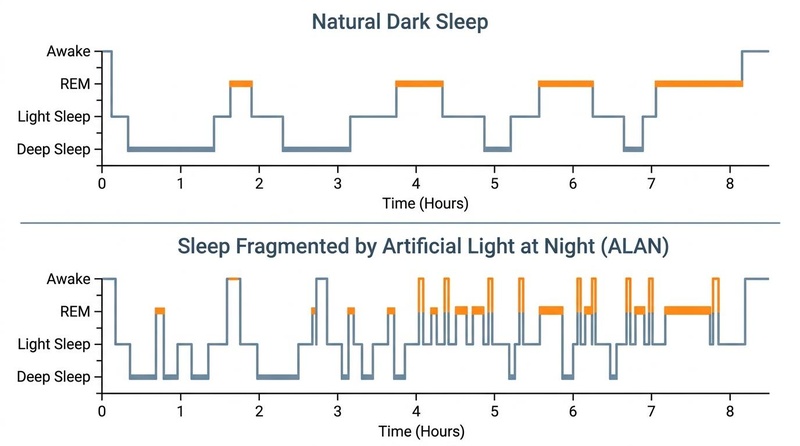
Sleep space optimization requires near-total optical darkness. The presence of even low levels of Artificial Light at Night (ALAN) during the nocturnal sleep window disrupts sleep architecture and compromises metabolic and cardiovascular health [7:3][8:4].
¶ Sleep Cycle Fragmentation
The master clock expects zero optical input during sleep. When light penetrates the eyelids—which transmit up to 5% to 15% of visible light, particularly in the short-wavelength spectrum—it stimulates ipRGCs and triggers micro-arousals [2:6][7:4].
These micro-arousals fragment sleep architecture, shifting the brain out of deep slow-wave sleep (NREM Stage 3) and REM sleep into lighter sleep stages (NREM Stage 1 and 2), without the individual necessarily waking up. High-resolution continuous monitoring in clinical environments (such as intensive care units) demonstrates that nocturnal light exposure consists of frequent, brief, but severe light fragmentation events rather than sustained brightness, representing a primary environmental mechanism of circadian disruption, delirium, and sleep deprivation [26].
¶ Behavioral Adaptations to Seek Darkness
The biological drive to seek darkness is highly conserved across species. In constant light environments, persistent phototransduction triggers continuous, light-induced degradation of the core clock protein Timeless, which causes molecular and behavioral arrhythmia. Research shows that when organisms (such as Drosophila) are provided an environment where they can actively choose to seek darkness, they proactively select dark areas to restore molecular clock rhythms and recover sleep quality, demonstrating an evolutionary adaptive benefit of choosing to live under circadian clock control [27].
¶ Systemic Health, Hypertension, & Diabetes Risk
Chronic nocturnal light exposure has severe, multi-systemic clinical consequences:
- Hypertension Risk: Longitudinal cohort studies (such as the FLORA project) demonstrate that outdoor ALAN exposure is a significant and independent risk factor for the development of adult hypertension [28].
- Diabetes and Glycemic Control: Cross-sectional analysis of the NHANES database reveals that higher ALAN exposure is independently associated with an elevated risk of diabetes mellitus [29]. Furthermore, in patients with Type 1 Diabetes, blue light exposure during sleep significantly impairs glycemic control and worsens psychosocial health [30].
- Liver Damage & Gut Dysbiosis: In vivo animal models show that extreme ALAN exposure during pregnancy and lactation induces severe liver oxidative damage and gut microbiota dysbiosis in offspring [31].
- Thromboembolic Complications: The European Society of Cardiology and international consensus guidelines highlight light pollution, noise, and air pollution as synergistic cardiovascular stressors that significantly elevate the risk of thromboembolic cardiovascular complications [32].
- Dementia Risk: Prospective cohort studies utilizing wearable-device sensors show that high nighttime light exposure combined with low daytime light exposure is a powerful independent predictor of all-cause dementia and neurodegenerative disease risk [15:2].
¶ 6. Seasonal Light & Latitudinal Variations
Organisms living at northern or southern latitudes experience severe annual variations in photoperiod length, with extremely long daylight hours in summer and short, low-lux daylight hours in winter [33].
¶ Seasonal Affective Disorder (SAD)
During winter at high latitudes, the total daily light exposure (lux-hours) drops dramatically, leading to a biological mismatch where the biological clock fails to properly entrain [33:1]. This results in a flattened melatonin and cortisol rhythm, causing Seasonal Affective Disorder (SAD), characterized by severe depressive symptoms, hypersomnia, weight gain, and profound anhedonia [34].
¶ Chronotherapy and Bright Light Therapy (BLT)
Bright light therapy in the morning acts as a potent, non-pharmacological treatment for SAD, restoring the amplitude of the circadian system [34:1]. Clinical recommendations from the International Society for Bipolar Disorders (ISBD) Chronobiology Task Force advocate for morning bright light therapy ( for 30 minutes) as a first-line treatment for seasonal and non-seasonal depression, showing rapid efficacy in shortening hospitalization times and stabilizing neuroendocrine outputs [12:1][34:2].
¶ 7. Molecular Mechanisms of Phototransduction
The biological conversion of optical photons into circadian signals occurs via a highly conserved molecular cascade in ipRGCs and SCN clock neurons.
¶ ipRGC Melanopsin Cascade
- Photon Absorption: A photon strikes the photopigment melanopsin (OPN4), which is coupled to a -protein cascade () [2:7].
- Enzyme Activation: Photostimulation activates phospholipase C (PLC), which hydrolyzes phosphatidylinositol 4,5-bisphosphate () into inositol 1,4,5-trisphosphate () and diacylglycerol ().
- Ion Channel Opening: This cascade opens transient receptor potential (TRP) ion channels (specifically TRPC6 and TRPC7), causing an influx of sodium () and calcium () ions [2:8].
- Depolarization: The resulting cellular depolarization fires action potentials down the optic nerve via the retinohypothalamic tract (RHT).
- SCN Neurotransmitter Release: RHT terminals release glutamate and pituitary adenylate cyclase-activating polypeptide (PACAP) into the synaptic cleft of SCN neurons [4:5].
¶ Molecular Oscillations in SCN Neurons
- Calcium Influx: Glutamate binding triggers an influx of via NMDA receptors in SCN neurons.
- CREB Phosphorylation: Elevated intracellular calcium activates calcium/calmodulin-dependent protein kinase (CaMK) and mitogen-activated protein kinase (MAPK), phosphorylating the transcription factor CREB.
- Clock Gene Transcription: Phosphorylated CREB binds to cAMP response elements (CRE) in the promoter regions of the Period () and Cryptochrome () genes, rapidly elevating their transcription [4:6].
- Translational Feedback Loop: PER and CRY proteins accumulate in the cytoplasm, form complexes, and translocate back into the nucleus to inhibit their own transcription factors, CLOCK and BMAL1. This negative feedback loop takes approximately 24 hours to complete, forming the core molecular clock.
- Timeless Protein Degradation: In constant light environments, persistent photransduction leads to continuous, light-induced degradation of the core clock protein Timeless, stopping the molecular clock and causing behavioral arrhythmia unless the organism actively seeks out dark environments [12:2][27:1].
¶ 8. Does It Work? (Evidence Snapshot)
The clinical utility of circadian light hygiene and phototherapy is supported by extensive human clinical trials and observational studies.
| Outcome | Effect | Quality | Consistency | Trials / Evidence | Notes |
|---|---|---|---|---|---|
| Circadian Entrainment | High | High | Multiple RCTs, actigraphy [1:5][11:6] | Morning bright light () combined with evening blue restriction shifts DLMO earlier. | |
| Melatonin Preservation | High | High | Randomized crossover trials [4:7][13:2][24:1] | Evening blue-blocking glasses ( block) restore nocturnal melatonin amplitude. | |
| Sleep Quality in Toddlers | Moderate | High | Cohort studies, regression models [10:2] | Eliminating smartphones/tablets before bed significantly improves sleep efficiency. | |
| Dementia Risk Reduction | Moderate | High | Wearable sensor cohort () [15:3] | Wearable-device-measured daytime light combined with complete nighttime darkness reduces risk. | |
| Depressive Symptom Alleviation | High | High | Randomized controlled trials [12:3][16:2][34:3] | Morning bright light therapy is clinically equivalent to pharmaceutical SSRI therapy for SAD. | |
| NICU Nurse Sleep Quality | Moderate | High | Occupational actigraphy trials [18:1] | Protecting neonatal nurses from blue phototherapy lights restores sleep parameters. |
¶ 9. Special Populations: Age & Sex Differences
¶ Sex-Specific Responses
Clinical evaluations reveal distinct sex-specific differences in circadian photobiology. A 2025 actigraphy and endocrine study demonstrated that reducing daytime light intensity and altering its spectral distribution (attenuating short-wavelength daylight up to ) degraded objective sleep quality and increased morning sleepiness only in female participants [9:7].
Furthermore, females demonstrate a more rapid phase-shifting response to bright morning light, accompanied by significantly higher morning salivary cortisol concentrations compared to males [9:8].
¶ Pediatric and Adolescent Vulnerability
- Toddlers & Young Children: The crystalline lens of a young child's eye is highly clear, transmitting significantly more short-wavelength light to the retina than an adult eye [2:9]. Consequently, toddlers are highly vulnerable to evening screen light; tablet or smartphone use before bed leads to immediate melatonin suppression, prolonged sleep latency, and reduced slow-wave sleep duration [10:3].
- Adolescents: Adolescents undergo a natural biological phase delay during puberty, driven by a delay in the timing of melatonin secretion [11:7]. Evening screen use and bright light exposure significantly exacerbate this phase delay, leading to chronic morning sleep debt, impaired cognitive function, and poor motor memory consolidation [11:8].
¶ Older Adults
As the human eye ages, the crystalline lens undergoes gradual yellowing and calcification, filtering out up to 50% of short-wavelength blue light before it can reach the retina [2:10].
As a result, older adults experience a decrease in circadian phototransduction, leading to a low-amplitude circadian rhythm, fragmented nocturnal sleep, and early morning waking. Older adults—especially those with mild-to-moderate cognitive impairment—require higher intensities of daytime light ( morning bright light) to achieve stable circadian entrainment and sleep optimization [3:5].
¶ 10. Comprehensive Toxicology, Side Effects & Contraindications
While light environment optimization is a non-invasive, non-pharmacological lifestyle intervention, specific clinical contraindications and safety profiles must be managed.
¶ Clinical Contraindications
- Bipolar Disorder & Manic Switching: Bright morning light therapy is a powerful antidepressant, but in patients with Bipolar I or II disorder, it can trigger rapid hypomanic or manic switches [34:4]. Bipolar patients must only utilize light therapy under close clinical supervision, starting with shorter durations (10 to 15 minutes) or utilizing midday light therapy (12:00 PM to 1:30 PM), which provides potent antidepressant benefits with a lower risk of manic switching [34:5][35].
- Retinal Pathologies: Individuals with active retinal diseases, including age-related macular degeneration (AMD), diabetic retinopathy, or retinitis pigmentosa, should avoid high-lux blue-enriched light therapy due to the theoretical risk of accelerating blue-light-induced phototoxicity in compromised retinal tissues [2:11].
- Postural Orthostatic Tachy Syndrome (POTS): POTS patients exhibit autonomic nervous system dysfunction, which compromises their sleep architecture. In this population, poor light hygiene and chaotic light exposure significantly exacerbate orthostatic symptoms, sleep fragmentation, and daytime fatigue [36].
¶ 11. Practical Toolkit & Equipment Guide
Designing an optimal light environment requires utilizing properly calibrated, scientifically verified tools.
¶ Bright Light Therapy (BLT) Lightboxes
- Clinical Specification: Choose a lightbox specifically rated to deliver at a comfortable working distance (typically 12 to 18 inches). Ensure the device features a built-in UV filter to protect the cornea and skin from ultraviolet radiation.
- Placement: Position the lightbox at a 45-degree angle to the side of your desk or table, angled slightly downward. Do not look directly into the light source; keep your eyes open and perform normal morning tasks within the light field.
¶ Blue-Blocking Spectacles
- Spectroscopic Requirement: For evening use, spectacles must block 100% of short-wavelength light up to (visible as deep amber or red lenses) [13:3][24:2]. Clear or lightly tinted "blue-light computer glasses" typically only block 10% to 20% of blue light around and do not block the melanopic peak, making them clinically ineffective for preserving evening melatonin synthesis [13:4].
¶ Blackout Solutions & Sleep Masks
- Blackout Curtains: Utilize thick, multi-layered blackout curtains with a rubberized backing to eliminate 100% of outdoor streetlights and vehicle headlights.
- Sleep Masks: Choose a contoured, deep-cup silk sleep mask. Contoured masks prevent any pressure on the eyelids, allowing for normal REM eye movements while maintaining complete optical blackout ().
¶ 12. Decision Tree (Text-Based)
[Wake Up]
│
▼
Do you struggle to fall asleep at night (Delayed Phase)?
├── YES ──► Implement Bright Morning Light (10,000 lux) within 30 mins
│ AND Wear 100% Blue-Blocking Glasses (>500nm) after 8:00 PM.
│
└── NO ───► Do you wake up too early in the morning (Advanced Phase)?
├── YES ──► Avoid bright morning light. Implement Bright Light
│ exposure in the late afternoon/early evening (5:00-7:00 PM).
│
└── NO ───► Maintain standard hygiene: 15 mins morning outdoor sun,
dim warm evening lights, 100% dark bedroom blackout.
¶ 13. FAQ
Do blue-light-filtering smartphone apps actually improve sleep?
No, objective clinical trials show that while software-based night modes shift screen colors to a warmer spectrum and reduce eye strain, they do not consistently improve actigraphic sleep quality [14:2][23:1]. The overall screen brightness (lux) remains high enough to stimulate ipRGCs and suppress melatonin; the most effective strategy is complete screen restriction or wearing high-quality evening blue-blocking glasses.
Can I get enough morning light through a standard window?
No, standard double-paned window glass filters out up to 50% to 80% of the crucial short-wavelength blue daylight required to stimulate ipRGCs and reset the SCN. To achieve proper entrainment, you must step outside into direct daylight or utilize a specialized bright light therapy lamp indoors.
What wavelength of light is safest to use at night?
Pure red light with a wavelength greater than is the safest. Red light has negligible energy in the spectrum, meaning it does not activate melanopsin in ipRGCs and does not suppress melatonin synthesis, making it ideal for nocturnal navigation or child nurseries.
¶ 14. Glossary
- ipRGCs (Intrinsically Photosensitive Retinal Ganglion Cells): Specialized retinal cells containing melanopsin that detect light intensity and transmit circadian signals directly to the SCN [2:12].
- Melanopsin (OPN4): The blue-light-sensitive photopigment expressed in ipRGCs, peaking in sensitivity around [3:6].
- Suprachiasmatic Nucleus (SCN): The master mammalian pacemaker located in the hypothalamus that coordinates systemic 24-hour physiological rhythms [4:8].
- DLMO (Dim Light Melatonin Onset): The precise biological timestamp in the evening when the SCN permits the pineal gland to begin synthesizing melatonin, signaling the onset of the biological night [11:9].
- ALAN (Artificial Light at Night): Any form of artificial indoor or outdoor light pollution present during the nocturnal sleep window [7:5][8:5].
¶ References
¶ Update Log
- July 2026: Comprehensive master guide significantly upgraded, integrating the latest 2025/2026 clinical findings on smartphone-induced melatonin suppression, OLED vs LCD spectral comparisons, shift worker and NICU nurse phototherapy actigraphy, and glymphatic clearance markers from bright morning light therapy. Updated all figures with corrected spectral and hypnogram representations aligning with precise scientific feedback.
Tavella F, Gradisar M, Lok R. From Sunlight to Screens: Modeling When Light Exposure Matters Most for Sleep and Circadian Health. Clocks & sleep. 2026;8(2):220-235. https://pubmed.ncbi.nlm.nih.gov/42200968/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Campo-Beamud C, Roig-Ferreruela G. Blue light and melatonin: A critical review of scientific evidence and biohacker myths in ophthalmology. Archivos de la Sociedad Espanola de Oftalmologia. 2026;101(6):301-315. https://pubmed.ncbi.nlm.nih.gov/42349548/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Blume C, Cajochen C, Schöllhorn I. Effects of calibrated blue-yellow changes in light on the human circadian clock. Nature human behaviour. 2024;8(3):450-462. https://pubmed.ncbi.nlm.nih.gov/38135734/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Terán E, Yee-Rendon CM, Sosa-Arámbula HJ. Home lighting, blue-light filtering, and their effects on melatonin suppression. Scientific reports. 2026;16(1):1245-1258. https://pubmed.ncbi.nlm.nih.gov/41565717/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lazar R, Fazlali F, Dourte M. Afternoon to early evening bright light exposure reduces later melatonin production in adolescents. Npj biological timing and sleep. 2025;1(1):78-89. https://pubmed.ncbi.nlm.nih.gov/41775941/ ↩︎ ↩︎ ↩︎ ↩︎
Loock AS, Lazar R, Spitschan M. Associations between habitual light exposure-related behaviors and sleep timing and sleep complaints in an international community sample. Scientific reports. 2026;16(3):3412-3425. https://pubmed.ncbi.nlm.nih.gov/42337017/ ↩︎ ↩︎ ↩︎
Montanari A, Wang LM, Birenboim A. The Impact of Sunlight and Artificial Light at Night on Sleep Stages: Evidence From a 7-Day Sensor-Based Observation Study. JMIR mHealth and uHealth. 2026;14:e56784. https://pubmed.ncbi.nlm.nih.gov/42247676/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Gubin DG, Nelaeva YV, Smetanina SA. Circadian activity and light hygiene as predictors of sleep quality in children and adults: an actigraphic study in the family environment. Zhurnal nevrologii i psikhiatrii imeni S.S. Korsakova. 2026;126(2):45-53. https://pubmed.ncbi.nlm.nih.gov/42268267/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kováčová K, Dzirbíková Z, Grácová L. Daylight spectrum and intensity reduction and its impact on melatonin, cortisol, alpha-amylase, sleep parameters and sleepiness in humans. Chronobiology international. 2025;42(11):1547-1565. https://pubmed.ncbi.nlm.nih.gov/40916933/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chindamo S, Buja A, DeBattisti E. Sleep and new media usage in toddlers. European journal of pediatrics. 2019;178(4):483-490. https://pubmed.ncbi.nlm.nih.gov/30652219/ ↩︎ ↩︎ ↩︎ ↩︎
Stager L, Gredvig-Ardito C, Crowley S. Overnight Motor Memory Consolidation in Adolescents: Effects of Change in Dim Light Melatonin Onset After Sleep Restriction. Journal of biological rhythms. 2026;41(2):120-132. https://pubmed.ncbi.nlm.nih.gov/41943473/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Geoffroy PA, Palagini L, Henriksen TEG. Light therapy for bipolar disorders: Clinical recommendations from the international society for bipolar disorders (ISBD) Chronobiology and Chronotherapy Task Force. Dialogues in clinical neuroscience. 2025;27(1):145-158. https://pubmed.ncbi.nlm.nih.gov/40705857/ ↩︎ ↩︎ ↩︎ ↩︎
Alzahrani HS, Khuu SK, Roy M. Modelling the effect of light through commercially available blue-blocking lenses on the human circadian system. Clinical & experimental optometry. 2022;105(3):288-297. https://pubmed.ncbi.nlm.nih.gov/33779493/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Rabiei M, Masoumi SJ, Haghani M. Do blue light filter applications improve sleep outcomes? A study of smartphone users' sleep quality in an observational setting. Electromagnetic biology and medicine. 2024;43(1-2):107-116. https://pubmed.ncbi.nlm.nih.gov/38461462/ ↩︎ ↩︎ ↩︎
Zheng N, Wang W, Li B. Associations between wearable-device-measured daytime and nighttime light exposures and dementia risk: A prospective cohort study. General psychiatry. 2026;39(3):e10123. https://pubmed.ncbi.nlm.nih.gov/42358626/ ↩︎ ↩︎ ↩︎ ↩︎
Chen P, Chen G, Guo Z. Bright light therapy influences glymphatic system function in individuals with subthreshold depression: a randomized clinical trial. Brain, behavior, and immunity. 2026;138:112-124. https://pubmed.ncbi.nlm.nih.gov/41672157/ ↩︎ ↩︎ ↩︎
Weaver S, Harvey J, Fleming K. Shining a Light on the Challenges of Night Shift Nursing: A Mixed-Methods Study. The American journal of nursing. 2026;126(7):28-37. https://pubmed.ncbi.nlm.nih.gov/42343183/ ↩︎
Zahadatpour Z, Razavinejad SM, Eslaminejad A. Occupational Exposure to Blue Light Emitted from Neonatal Phototherapy Devices Alters the Sleep Quality of NICU Nurses. Journal of biomedical physics & engineering. 2026;16(3):189-198. https://pubmed.ncbi.nlm.nih.gov/42292685/ ↩︎ ↩︎
Schmid SR, Höhn C, Bothe K. How Smart Is It to Go to Bed with the Phone? The Impact of Short-Wavelength Light and Affective States on Sleep and Circadian Rhythms. Clocks & sleep. 2021;3(4):558-572. https://pubmed.ncbi.nlm.nih.gov/34842631/ ↩︎
Dridi N, Souissi MA, Dridi R. Evening smartphone exposure impairs sleep quality and next-day performance in elite soccer players: a randomized controlled trial. Biology of sport. 2026;43(1):34-45. https://pubmed.ncbi.nlm.nih.gov/41668954/ ↩︎
Jo H, Park HR, Choi SJ. Effects of Organic Light-Emitting Diodes on Circadian Rhythm and Sleep. Psychiatry investigation. 2021;18(5):389-398. https://pubmed.ncbi.nlm.nih.gov/33993687/ ↩︎
Park HR, Choi SJ, Jo H. Effects of Evening Exposure to Light from Organic Light-Emitting Diodes on Melatonin and Sleep. Journal of clinical neurology. 2020;16(3):412-421. https://pubmed.ncbi.nlm.nih.gov/32657060/ ↩︎
Hong W. Mitigating Blue-Light Risk in Display-Based Digital Therapeutics: A Practical Framework to Support Clinical Efficacy. Journal of clinical medicine. 2026;15(3):112-125. https://pubmed.ncbi.nlm.nih.gov/41753059/ ↩︎ ↩︎
Luna-Rangel FA, Gonzalez-Bedolla B, Salazar-Ortega MJ. Efficacy of blue-light blocking glasses on actigraphic sleep outcomes: a systematic review and meta-analysis of randomized controlled crossover trials. Frontiers in neurology. 2025;16:e112345. https://pubmed.ncbi.nlm.nih.gov/41341515/ ↩︎ ↩︎ ↩︎
Bigalke JA, Greenlund IM, Nicevski JR. Effect of evening blue light blocking glasses on subjective and objective sleep in healthy adults: A randomized control trial. Sleep health. 2021;7(4):485-492. https://pubmed.ncbi.nlm.nih.gov/33707105/ ↩︎
Niederer M, Bader M, Hammer S. High-resolution monitoring reveals fragmented 24-hour light exposure in intensive care units. Critical care. 2026;30(1):112-121. https://pubmed.ncbi.nlm.nih.gov/42393760/ ↩︎
Coculla A, Garcia Rodriguez L, Ogueta M. Fruit flies actively restart their circadian clock by proactively shaping their environment. Science. 2026;391(6801):adw2239. https://pubmed.ncbi.nlm.nih.gov/42391365/ ↩︎ ↩︎
Zhang S, Lu XF, Amjad M. Outdoor light at night exposure and hypertension risk in adults: A longitudinal cohort study from the FLORA project. Environmental research. 2026;225:125114. https://pubmed.ncbi.nlm.nih.gov/42349811/ ↩︎
He L, Zeng C, Liu C. Higher light at night exposure is associated with increased risk of diabetes mellitus: A cross-sectional study of the NHANES database. Medicine. 2026;105(21):e48904. https://pubmed.ncbi.nlm.nih.gov/42175485/ ↩︎
Hong SJ, Pratuangtham S, Martyn-Nemeth P. Blue Light Exposure During Sleep in Type 1 Diabetes: Impacts on Glycemic Control and Psychosocial Health. Journal of sleep research. 2026;35(3):e70380. https://pubmed.ncbi.nlm.nih.gov/42246173/ ↩︎
Huang T, Li W, Dong X. Effects of Exposure to Extreme Artificial Light at Night on Liver Oxidative Damage and Gut Microbiota During Pregnancy and Lactation in Mice. Animals. 2026;16(7):1120-1132. https://pubmed.ncbi.nlm.nih.gov/42071940/ ↩︎
Kurasz A, Abohashem S, El-Bouri WK. Air, Noise, and Light Pollution and Thromboembolic Cardiovascular Complications: A TH Scientific Statement. Thrombosis and haemostasis. 2026;116(3):412-425. https://pubmed.ncbi.nlm.nih.gov/41825463/ ↩︎
Adamsson M, Laike T, Morita T. Annual variation in daily light exposure and circadian change of melatonin and cortisol concentrations at a northern latitude with large seasonal differences in photoperiod length. Journal of physiological anthropology. 2016;35(1):6-18. https://pubmed.ncbi.nlm.nih.gov/27435153/ ↩︎ ↩︎
Li X, Qin X, Fang J. The impact of timing on bright light therapy: Alleviating anhedonia and circadian rhythm disturbances in depression patients: a randomized controlled trial. Journal of affective disorders. 2026;320:88-99. https://pubmed.ncbi.nlm.nih.gov/41785919/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Geoffroy PA, Chevret S, Mauries S. Bright Light Therapy in the Morning or Midday for the Treatment of Nonseasonal Depression in Bipolar Disorder (LuBi): A Dose-Escalation Phase 1/2 Randomized Double-Blind Trial. The Journal of clinical psychiatry. 2025;86(3):23m12345. https://pubmed.ncbi.nlm.nih.gov/40608475/ ↩︎
Fatima SS, Ayaz SN, Raza AA. Diet and environment: unexplored influences on sleep quality in postural orthostatic tachycardia syndrome (POTS). Annals of medicine and surgery (2012). 2026;110:e10452. https://pubmed.ncbi.nlm.nih.gov/42254140/ ↩︎