¶ Long COVID
| Indication | Post-Acute Sequelae of SARS-CoV-2 (PASC) |
| Access | Multidisciplinary clinical care & symptom management |
| Diagnostic Criteria | Symptoms persisting beyond 4 to 12 weeks post-infection [^35][^36] |
| Safety Profile | Exercise-dependent (must be tailored to avoid post-exertional malaise [^32]) |
| Key Markers | Inflammatory cytokines, endothelial dysfunction, and coagulopathy markers [^8][^10] |
| Est. Cost | Variable (clinical care, supportive rehabilitation, off-label therapies) |
Long COVID, medically recognized as Post-Acute Sequelae of SARS-CoV-2 Infection (PASC) or Post-COVID-19 Condition (PCC), is a complex, multi-system syndrome that persists or develops following acute SARS-CoV-2 infection [1][2][3]. Lacking a single unifying biomarker, its management relies on phenotypic characterization, systematic differential diagnostics to exclude alternative pathologies, and personalized, symptom-contingent therapeutic and rehabilitative protocols [2:1][4].
¶ At a glance
- What people use it for: Long COVID clinical protocols focus on managing persistent disabling fatigue, post-exertional malaise (PEM), dysautonomia, neurocognitive dysfunction ("brain fog"), sleep disturbances, and chronic pain after an acute SARS-CoV-2 infection [2:2][3:1][4:1].
- Does it work? Combined physical and mental health rehabilitation programs and structured pacing protocols probably improve overall health and quality of life, and physical rehabilitation programs demonstrate short-term improvements in physical function [5][6][7][8]. Other alternative therapies, such as Low-Dose Naltrexone (LDN), show potential in observational studies but currently lack robust, large-scale randomized controlled trial (RCT) validation [9].
- Key risks: Off-label pharmacological therapies and alternative treatments often lack support from large-scale randomized trials to confirm their efficacy and establish long-term safety [9:1], while the underlying pathophysiological mechanisms remain under investigation [4:2].
- Verdict: Management must be highly individualized, non-coercive, and centered on strict energy pacing. While experimental antivirals and immunomodulators are undergoing clinical trials, current clinical care focuses on symptom-targeted support and structured energy management [1:1][2:3][4:3].
¶ 1. Clinical Definition & Diagnostic Timelines
To effectively manage Long COVID, clinicians must navigate three prominent clinical definitions established by major global health organizations. These criteria differ significantly in their diagnostic thresholds, timelines, and clinical implications:
- World Health Organization (WHO): Defines Post-COVID-19 Condition (PCC) as occurring in individuals with a history of probable or confirmed SARS-CoV-2 infection, usually 3 months (12 weeks) from the onset, with symptoms that last for at least 2 months and cannot be explained by an alternative diagnosis [10]. Symptoms may be new onset following initial recovery or persist from the acute illness, and they may fluctuate or relapse over time [10:1].
- Centers for Disease Control and Prevention (CDC): Uses a broader threshold, defining Post-COVID Conditions (PCC) as new, returning, or ongoing health problems persisting 4 or more weeks after the initial acute infection [11][12].
- National Institute for Health and Care Excellence (NICE): Differentiates the post-acute phase into two distinct clinical periods [13]:
- Ongoing Symptomatic COVID-19: Signs and symptoms of COVID-19 from 4 to 12 weeks post-onset.
- Post-COVID-19 Syndrome: Signs and symptoms that develop during or after an infection consistent with COVID-19, continue for more than 12 weeks, and are not explained by an alternative diagnosis.
¶ Comparative Clinical & Diagnostic Implications
The application of these differing diagnostic frameworks carries profound real-world consequences for epidemiology, clinical coding, and patient care:
- Epidemiological Discordance & Prevalence Variation: The CDC's 4-week threshold is highly sensitive, capturing early, transient post-viral fatigue and resolving convalescent symptoms. This yields higher reported prevalence rates in early surveys [11:1]. In contrast, the WHO and NICE 12-week criteria establish a longer duration threshold, defining the post-acute condition by symptoms continuing for more than 12 weeks that cannot be explained by an alternative diagnosis [10:2][13:1]. While global prevalence estimates vary widely from 6% in consensus guidelines [14] to over 30% in systematic meta-analyses of observational cohorts [15], standardizing definition parameters remains crucial for consistent cohort tracking [13:2][15:1].
- Diagnostic Coding & Electronic Health Record (EHR) Utility: Under the ICD-10 clinical coding system, code U09.9 ("Post COVID-19 condition, unspecified") was introduced to track these patients. The introduction of the International Classification of Diseases, Tenth Revision (ICD-10) code U09.9 ('Post COVID-19 condition, unspecified') provides a method of evaluating this condition in electronic health records (EHRs); however, cohort studies have focused on characterizing the utility and accuracy of this code across different healthcare systems by operationalizing standard health agency clinical case definitions [12:1]. However, the specificity of these definitions is a major challenge: clinical trials and observational studies show that up to one-fifth (20%) of test-negative patients who never had SARS-CoV-2 report persistent background symptoms that meet broader Post-COVID-19 Condition criteria, highlighting the lack of specificity in general clinical case definitions [16].
- Clinical Application of Phase Definitions: Rather than a single post-acute entity, the NICE separation of "ongoing symptomatic" (4–12 weeks) and "post-COVID-19 syndrome" (more than 12 weeks) has been challenged by clinical observations [17]. Stratifying patients into distinct post-acute subgroups is proposed to support more targeted diagnostic workups, personalized symptom management, and accurate epidemiological tracking [17:1].
- Disability Considerations: Long COVID can significantly impair daily and occupational functioning. Consensus guidance emphasizes that management should focus on symptom-based supportive care, energy conservation strategies, and addressing comorbidities [14:1]. Overly intense activity must be avoided to prevent triggering symptom exacerbations [14:2].
- Research Cohort Homogeneity: Comparing clinical trials that enroll participants at the 4-week mark with those enrolling at 12 weeks introduces massive confounding. Stratifying patients into "SARS-CoV-2-induced diseases" (e.g., organ damage) versus true "post-acute COVID condition" (characterized by post-exertional malaise and dysautonomia) is mandatory for achieving reproducible clinical trial outcomes [17:2].
¶ 2. Phenotypic Characterization
Long COVID is a heterogeneous syndrome. Clinicians should categorize patients into distinct, often overlapping, physiological phenotypes to guide targeted therapy.
¶ Post-Exertional Malaise (PEM)
Post-exertional malaise (PEM), also referred to as post-exertional symptom exacerbation (PESE), is the cardinal symptom of Long COVID and post-COVID syndrome [14:3]. It is characterized by an exacerbation of systemic symptoms following physical, cognitive, or emotional exertion [14:4]. Managing activities across physical, cognitive, and emotional domains to avoid triggering these episodes is a core focus of clinical care [14:5].
¶ Dysautonomia & Autonomic Dysregulation
Autonomic nervous system dysfunction and autonomic dysregulation are well-documented pathophysiological features in patients with Long COVID, manifesting as general dysautonomia [18][3:2]. In a subset of patients, particularly adolescents and young adults, this autonomic impairment manifests as Postural Orthostatic Tachycardia Syndrome (POTS), causing severe orthostatic intolerance, tachycardia, and dizziness upon standing [19]. These autonomic complications are central drivers of the persistent, multi-system symptom burden and functional impairment observed in clinical cohorts [18:1][3:3][14:6].
¶ Respiratory & Ventilatory Dysfunction
This phenotype presents primarily with persistent exertional dyspnea, which is a highly prevalent post-acute symptom that can endure for many months following the initial infection [20], as well as cough [11:2]. Rather than a direct link to localized pulmonary tissue, these symptoms occur in the context of general systemic endotheliopathy, microvascular injury, and overlapping inflammatory pathways that characterize post-acute COVID sequelae [21]. Clinical evidence indicates that while pulmonary rehabilitation significantly improves physical capacity, fatigue, and quality of life, meta-analytic evidence shows it does not lead to a statistically significant improvement in persistent dyspnea [5:1].
¶ Neurocognitive Impairment ("Brain Fog")
Patients frequently experience neurocognitive deficits, commonly described as 'brain fog,' which include impairments in concentration, memory, and cognitive function [4:4]. Research into interventions for mental health, cognition, and psychological well-being in Long COVID is highly heterogeneous, with studies evaluating psychosocial, pharmaceutical, natural supplement, neurocognitive, physical, and integrated rehabilitation approaches finding that the evidence base remains inconclusive to date [22].
¶ Sleep Disturbances
Sleep disturbances and sleep disorders represent a common manifestation of Long COVID, presenting alongside other persistent multi-system symptoms [3:4].
¶ Pain-Related Manifestations
Pain-related symptoms, such as chest pain, are frequently reported among the multi-system manifestations of Long COVID [4:5], while pain and myalgias (muscle pain) are recognized as common symptoms in consensus guidelines [14:7].
¶ Thromboembolic & Vascular Pathology
This phenotype is characterized by endothelial injury, dysfunction, and associated inflammatory pathways and coagulopathies [21:1][23]. It is associated with pro-coagulant effects, endothelial injury, and potential thrombotic risks that may require clinical management such as thromboprophylaxis [21:2][23:1].
¶ 3. Differential Diagnostics & Red Flags
Because Long COVID lacks a definitive diagnostic assay, systematic exclusion of other organic, treatable post-viral complications and overlapping pathologies is mandatory.
¶ Cardiovascular Workup
Clinicians must exclude myocarditis, pericarditis, coronary artery disease, heart failure, and pulmonary hypertension.
- Initial Tests: 12-lead electrocardiogram (ECG), high-sensitivity cardiac troponin, N-terminal pro-brain natriuretic peptide (NT-proBNP), and transthoracic echocardiogram.
- Advanced Imaging: Cardiac MRI (if myocarditis is suspected) or ambulatory 24-hour to 7-day Holter monitoring (to differentiate autonomic symptoms from primary cardiac arrhythmias).
¶ Pulmonary Workup
Exclude Interstitial Lung Disease (ILD), pulmonary embolism, and reactive airway disease.
- Initial Tests: Spirometry, lung volume plethysmography, and diffusing capacity of the lungs for carbon monoxide (DLCO).
- Advanced Imaging: Computed tomography pulmonary angiography (CTPA) or ventilation-perfusion (V/Q) scan if thromboembolic disease is suspected.
¶ Endocrine and Metabolic Screen
Exclude thyroiditis, adrenal insufficiency, new-onset diabetes mellitus, and profound nutritional deficiencies.
- Required Labs: Thyroid-stimulating hormone (TSH), free thyroxine (FT4), morning cortisol, adrenocorticotropic hormone (ACTH), hemoglobin A1c (HbA1c), vitamin B12, folate, and 25-hydroxyvitamin D.
¶ Autoimmune and Rheumatological Screening
Exclude systemic lupus erythematosus (SLE), rheumatoid arthritis, Sjögren’s syndrome, and systemic vasculitis.
- Required Labs: Antinuclear antibodies (ANA), rheumatoid factor (RF), anti-cyclic citrullinated peptide (anti-CCP), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and extractable nuclear antigen (ENA) panel.
¶ Clinical Red Flags
The presence of any of the following "Red Flag" symptoms warrants immediate emergency evaluation or direct specialist referral:
- Suicidal ideation or acute psychological crisis (immediate psychiatric or specialist escalation)
- Acute or progressive chest pain (ischemia, myocarditis, or pericarditis)
- Resting oxygen desaturation () or a drop of on minimal exertion (pulmonary embolism, interstitial lung disease)
- Syncope or pre-syncope upon standing (severe orthostatic hypotension, cardiac arrhythmia)
- Focal neurological deficits (stroke, transient ischemic attack, or myelopathy)
- Unexplained rapid weight loss, high fever, or drenching night sweats (malignancy, chronic infection, or systemic vasculitis)
¶ 4. Post-Exertional Malaise (PEM) Screening & Energy Management
Identifying PEM is the single most critical step in Long COVID clinical management. Rigid exercise is poorly tolerated and can exacerbate symptoms in patients with post-exertional malaise, requiring an individualized pacing-first approach [14:8].
¶ Screening for Post-Exertional Symptom Exacerbation (PESE/PEM)
Screening for post-exertional malaise or post-exertional symptom exacerbation (PESE) is critical for identifying patients at risk of clinical regression from physical activity [14:9]. Clinical protocols utilize structured history-taking and validated questionnaires to identify the presence and frequency of exertional triggers across physical, cognitive, and emotional domains [14:10].
To screen for PEM/PESE, clinical protocols utilize structured history-taking and validated questionnaires to identify the presence and frequency of exertional triggers across physical, cognitive, and emotional domains [14:11][17:3]. The DePaul Symptom Questionnaire Post-Exertional Malaise (DSQ-PEM) is a standardized tool widely recommended to characterize post-exertional malaise in patients with infection-associated chronic conditions [24]. To safely manage activity, clinicians must carefully differentiate and identify the presence of post-exertional malaise (PEM), as physical activity recommendations must be tailored to the patient's current tolerance to avoid triggering PEM/PESE [14:12][17:4].
¶ Clinical Presentation of Delayed Symptom Flares
The clinical hallmark of PEM/PESE is the exacerbation of multi-system symptoms and a profound reduction in baseline function following physical, cognitive, or emotional exertion [14:13][24:1]. A crucial, high-stakes diagnostic feature is the delayed onset or flare of symptoms: unlike standard physiological fatigue or deconditioning which resolves with rest and occurs immediately after exertion, PEM/PESE typically manifests with a distinct latency [14:14][25]. Symptom flares can trigger significant setbacks and deteriorated function following overexertion, highlighting the clinical necessity of activity monitoring and stabilization [25:1].
This post-exertional symptom exacerbation represents a state where metabolic and physical activities exceed the patient's biological energy envelope, leading to substantial setbacks and cellular-level damage that matches the clinical severity and thresholds observed in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) [25:2]. Clinicians must systematically screen for these delayed flares to differentiate PEM/PESE from deconditioning, and educate patients to stay strictly within their functional limits, as physical activity recommendations must be carefully tailored to the patient's current activity tolerance to avoid triggering PEM/PESE [14:15].
¶ The Biology of PEM
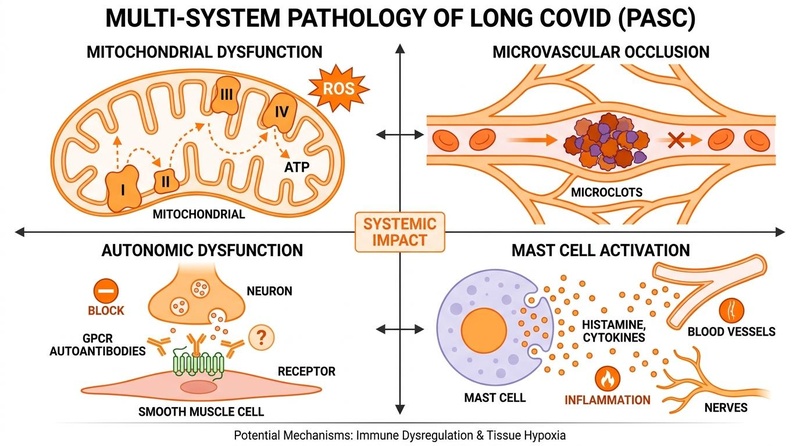
The symptom exacerbation characteristic of post-exertional symptom exacerbation is rooted in cellular metabolic alterations, mitochondrial dysfunction, and microvascular impairment [18:2][2:4][21:3][23:2]:
- Mitochondrial Dysfunction & Bioenergetics: Viral infections, particularly SARS-CoV-2, disrupt mitochondrial bioenergetics [18:3]. This disruption involves altered mitochondrial membrane integrity, increased mitochondrial reactive oxygen species (mtROS), and impaired mitophagy, leading to metabolic imbalance and sustained immune activation [18:4].
- Microvascular & Endothelial Injury: Persistent endothelial injury and dysfunction are key pathobiological processes in Long COVID [21:4][23:3]. Endothelial cell damage and dysfunction are linked to systemic inflammatory pathways and coagulopathies, which represent key mechanisms in SARS-CoV-2 associated endotheliopathies [21:5][23:4].
- Persistent Inflammation: Ongoing immune dysregulation, persistent inflammation, and viral reservoir persistence are hypothesized to drive systemic symptoms [1:2][2:5][4:6].
¶ Pacing Protocols & Energy Management
Clinical management relies entirely on energy pacing to prevent exceeding the patient's individual functional thresholds.
[ THE PACING FRAMEWORK ]
+------------------------------+
| THE ENERGY ENVELOPE |
| |
| [Current Bio-Capacity] |
| ====================== | <-- Keep all activities below this line
| |
| - Supine stretching |
| - Structured rest periods |
| - Cognitive intervaling |
| |
+------------------------------+
*Forced physical push -> CRASH (Mitochondrial Injury)*
- Symptom pacing: Rather than following rigid, time-gated schedules, patients are guided to stay within their functional limits, managing activities across physical, cognitive, and emotional domains to avoid triggering PESE episodes [14:16].
- Structured Pacing Protocols: Clinical studies support the use of structured energy pacing protocols—such as a 5-phase pacing protocol—which can reduce post-exertional symptom exacerbations across physical, cognitive, and emotional triggers, thereby improving overall health and quality of life [7:1].
- Cognitive and Emotional Pacing: Managing non-physical triggers is equally vital. Pacing protocols must target cognitive and emotional exertions alongside physical activities to help reduce post-exertional symptoms [7:2].
¶ 5. Symptom-Contingent Rehabilitation
Traditional rehabilitation paradigms must be radically adapted for patients experiencing post-exertional malaise to prevent clinical deterioration and systemic harm.
¶ Individualized, Patient-Guided Activity Management vs. Rigid Progressive Training
A critical clinical consensus in post-viral rehabilitation is the shift toward patient-guided pacing and energy management instead of rigid, progressive physical conditioning for patients experiencing post-exertional malaise (PEM/PESE) [14:17][25:3]:
- The Risk of Overly Intense Physical Activity: While exercise-based rehabilitation is helpful for general cohorts, forcing patients with a positive PEM/PESE phenotype to engage in overly intense physical activity is clinically counterproductive. Rather than reversing fatigue, exceeding the patient's individual activity tolerance can trigger severe post-exertional symptom exacerbation [14:18]. Because of this potential for setbacks and deteriorated function following overexertion, activity levels must be managed based on individual biological limits [25:4].
- Adaptive Energy Pacing: In contrast, energy pacing is a dynamic, patient-guided self-management framework where daily activity is carefully aligned with the individual's current functional limits [14:19][25:5]. Rather than pursuing rigid, calendar-based physical milestones, activity level adjustments are dynamically adapted based on real-time symptom stability and daily biological tolerance to prevent triggering post-exertional symptom exacerbations [7:3][25:6].
¶ Clinical Recommendations Regarding Rigid Physical Training
In patients presenting with a confirmed PEM/PESE phenotype, rigid progressive aerobic training programs (such as progressive physical training schedules) are not recommended due to risk of harm:
- Pathophysiological Mechanisms: SARS-CoV-2 infection is associated with altered mitochondrial membrane integrity, increased production of mitochondrial reactive oxygen species (mtROS), and impaired mitophagy (the clearance of damaged mitochondria), leading to a state of sustained metabolic imbalance and chronic systemic inflammation [18:5]. While these mitochondrial defects are a direct consequence of viral infection and spike-protein exposure rather than being directly demonstrated to be caused by physical activity [18:6], clinical guidelines caution that physical exertion must be tailored to avoid triggering post-exertional symptom exacerbation (PESE/PEM) in patients with these underlying cellular alterations [14:20].
- Risk of Setbacks: Rather than reversing fatigue or deconditioning, rigid physical pushing creates a significant potential for setbacks and deteriorated physical function [25:7].
- Consensus Guidelines Recommendations: Recognizing these substantial risks, multidisciplinary consensus statements emphasize that physical activity recommendations must be carefully tailored to the patient's current activity tolerance, as overly intense activity can trigger PEM/PESE [14:21].
¶ Mitochondrial and Cellular Disruption in PESE
In patients with a confirmed PEM/PESE phenotype, physical overexertion can exacerbate underlying mitochondrial and metabolic imbalances:
- Mitochondrial Disruption: SARS-CoV-2 infection is associated with altered mitochondrial membrane integrity, increased production of mitochondrial reactive oxygen species (mtROS), and impaired mitophagy, leading to a state of sustained metabolic imbalance and immune activation [18:7].
- Mitophagy and mtROS Exacerbation: SARS-CoV-2 infection disrupts mitochondrial bioenergetics by altering membrane integrity, increasing mtROS production, and impairing mitophagy (the clearance of damaged mitochondria), which contributes to chronic systemic inflammation and the multi-system symptoms of Long COVID [18:8].
- Activity Stabilization Priority: Clinical management must prioritize activity stabilization and strict pacing—ensuring the patient remains within their biological energy envelope—before any physical progress or increase in active time is contemplated [14:22][25:8].
¶ A Pacing-First, Symptom-Contingent Rehabilitation Framework
Rather than employing a linear or rigid progression, clinical rehabilitation must follow a pacing-first, symptom-contingent framework focused on energy conservation and activity stabilization [14:23][25:9]:
- Symptom Stabilization: Activity level adjustments are guided by the patient's demonstrated symptom stability and tolerance, rather than pre-scheduled calendar increases, helping prevent post-exertional symptom exacerbation [7:4][25:10].
- Immediate Regression Rules: Standard clinical experience dictates that if any post-exertional crash or symptom exacerbation occurs, the program must be immediately halted or rolled back to the previous stable baseline. Progression does not resume until stability is re-established.
- Structured Activity Pacing: Rather than following rigid physical training, physical activity recommendations must be carefully tailored to the patient's current activity tolerance to avoid triggering PEM/PESE [14:24].
- Supine and Parasympathetic-Sparing Modalities: Exercises can initially be restricted to supine or reclined positions (such as supine stretching, recumbent cycling, or floor-based yoga) to minimize orthostatic stress and avoid exacerbating dysautonomia or POTS. This helps spare the sympathetic nervous system and prioritize parasympathetic recovery.
- Cognitive and Emotional Intervaling: Cognitive exertion can be managed using structured rest intervals (such as scheduled breaks during cognitive tasks) to prevent cognitive-induced PEM crashes.
¶ Physical & Pulmonary Rehabilitation in General Cohorts
For patients who do not exhibit PEM/PESE (as confirmed by clinical screening), systematic reviews and meta-analyses show that pulmonary and cardiorespiratory rehabilitation programs can be implemented [5:2][6:1]. Specifically, pulmonary rehabilitation programs have been shown to significantly improve six-minute walk distance, maximal inspiratory pressure, fatigue, and overall quality of life [5:3], while cardiorespiratory rehabilitation program outcomes support significant improvements in submaximal exercise performance [6:2]. Subgroup analyses indicate that telerehabilitation offers a clinically equivalent alternative to in-person rehabilitation across these major outcomes [5:4]. Additionally, systematic review and meta-analytic evidence indicates that a program duration of 4 to 8 weeks combining both breathing exercises and multicomponent training is highly effective for managing these long-term syndromes [26].
¶ 6. Symptom-Targeted Care, RTW, & Prevention
Pharmacotherapy in Long COVID is directed at managing specific phenotypic manifestations, supporting safe clinical recovery, and preventing further physiological deterioration.
¶ Autonomic Symptoms (POTS & Dysautonomia)
General dysautonomia and Postural Orthostatic Tachycardia Syndrome (POTS) are highly disabling manifestations of Long COVID [18:9][3:5][19:1]. While there are no established, FDA-approved disease-specific pharmacological treatments for Long COVID autonomic symptoms, clinical management focuses on symptom-based supportive care and non-pharmacological pacing strategies [14:25]:
- Symptom-Based Support: To date, there are limited data to guide medication management specifically in the context of Long COVID. Clinical guidelines suggest focusing on supportive, symptom-targeted care, while non-pharmacological pacing and energy conservation strategies remain the cornerstone of managing autonomic and orthostatic symptoms [14:26].
- Comorbidities and Symptom Burden: Patient comorbidities can significantly influence the burden of Post-COVID-19 Condition. Specifically, in vaccinated patients with advanced chronic kidney disease (CKD stages G4-G5), those on dialysis, and kidney transplant recipients, Post-COVID-19 Condition occurs at high prevalence (ranging from 21% to 29%) and is associated with a high self-reported symptom burden [27].
- Multidisciplinary Rehabilitation: Activity recommendations should be tailored to the patient's current activity tolerance, focusing on energy conservation and symptom-based supportive care to manage orthostatic and autonomic symptoms [14:27].
¶ Low-Dose Naltrexone (LDN)
Low-Dose Naltrexone (LDN) is widely utilized off-label for the management of persistent symptoms such as chronic fatigue and neurocognitive deficits in Long COVID [9:2]:
- Evidence Status: Early findings from observational studies and case series suggest that LDN shows potential as an alternative supportive therapy [9:3].
- Clinical Limitations: LDN currently lacks robust, large-scale randomized controlled trials (RCTs) to confirm its efficacy and establish standardized dosing, titration protocols, or long-term safety profiles in patients with Post-COVID-19 Condition [9:4].
¶ Vaccination & Primary Prevention
Active immunization against SARS-CoV-2 is associated with lower post-acute symptom risks in specific clinical cohorts:
- Antibody Level Correlation: In prospective studies of vulnerable cohorts (such as advanced chronic kidney disease, dialysis, and kidney transplant patients), the odds of developing Post-COVID-19 Condition (PCC) are significantly lower per 10-fold increase in anti-spike antibody levels achieved after vaccination (aOR 0.82 [95% CI: 0.70-0.96], p = 0.01) [27:1].
- Impact of Vaccination Status: Cohort profiles of patients presenting with Long COVID often include individuals who received prior vaccines, with a significant proportion having received three or more doses before infection [28].
- Symptom Modulation in Established Long COVID: In a nationwide survey of U.S. adults, approximately 28.7% of respondents with a history of positive SARS-CoV-2 testing reported believing that receiving a COVID-19 vaccine made their pre-existing long-term symptoms better [11:3].
¶ Influence of Viral Variants and Infection Severity
The risk and severity of Post-COVID-19 Condition are heavily influenced by the specific viral variant of the acute infection [29]:
- Wuhan vs. Omicron Cohorts: Prospective matched cohort studies indicate that early ancestral variants (such as the Wuhan variant) carry a significantly higher propensity for inducing a broad spectrum of persistent physical, fatigue, and emotional-behavioral symptoms compared to later variants [29:1].
- Omicron Variant Outcomes: In pediatric and young adult cohorts, acute infection with the Omicron variant results in fewer post-infection effects, with long-term symptom incidence rates that do not differ significantly from common non-SARS-CoV-2 seasonal respiratory or intestinal illnesses [29:2].
¶ Return-to-Work (RTW) Strategies
Returning to occupational duties represents a major clinical milestone, requiring a structured, non-coercive approach to avoid PEM triggering:
- Graduated Schedules: Clinicians often recommend a graduated return-to-work program, typically commencing at 10% to 25% of baseline hours (e.g., 4 to 8 hours per week), with weekly or biweekly step-ups only after the patient demonstrates complete symptom stability. These highly specific percentages are general clinical parameters tailored to individual tolerance.
- Cognitive Pacing in the Workplace: Cognitive exertion must be paced identically to physical activity. Practical workplace accommodations in common clinical usage include implementing frequent scheduled micro-breaks, breaking complex tasks into short focused blocks, avoiding multitasking, and utilizing physical notebooks or dictation software to reduce short-term memory burdens.
- Physical Accommodations: The return-to-work process can be highly challenging because symptoms fluctuate and affect both physical and cognitive functional areas, prompting general disability considerations [14:28]. To support patient recovery, clinicians can work with employers to identify suitable workplace modifications such as ergonomic setups, flexible work hours, remote-work permissions to eliminate commuting fatigue, and allowing supine positioning during breaks.
¶ Clinical Differentiation from Vaccine Adverse Events
Because certain post-vaccine adverse events can present with overlapping symptoms (such as fatigue, dyspnea, or cognitive dysfunction), clinicians must perform a systematic clinical assessment [30]. Differentiating between these conditions relies on careful analysis of the timing of symptom onset relative to vaccination or SARS-CoV-2 infection, detailed symptom characterization, and the use of targeted diagnostic tools [30:1]. Accurate differentiation is critical for appropriate clinical management and patient care [30:2].
¶ 7. Experimental Interventions & Alternative Approaches
Numerous therapeutics are currently being investigated off-label or in active clinical trials. Clinicians must analyze these options with high clinical objectivity, distinguishing between theoretical biological plausibility and proven randomized clinical trial (RCT) efficacy.
¶ Antivirals & Replication Inhibitors
Sustained retention of SARS-CoV-2 viral antigen or genetic material in tissue reservoirs is a leading hypothesized mechanism driving Post-Acute Sequelae of SARS-CoV-2 (PASC) [1:3].
- Oral RdRp Inhibitors: To target viral replication and potentially prevent or reduce PASC, next-generation oral derivatives of the RNA-dependent RNA polymerase (RdRp) inhibitor GS-441524 (such as VV116, ATV006, and GS-621763) are being developed and evaluated for clinical utility [31].
- Clinical Trial Requirement: Both primary pathobiological studies and clinical experts emphasize that potential antiviral therapies and repurposed medications must undergo formal testing within structured clinical trial settings, discouraging off-label experimentation in unsupervised environments [1:4][2:6].
¶ Endothelial Protection & Thromboprophylaxis
Given the clinical findings of endothelial injury, vascular inflammation, and microvascular dysfunction in post-acute sequelae [21:6][23:5], some protocols utilize standard thromboprophylaxis with low-molecular-weight heparin (LMWH) or direct oral anticoagulants (DOACs) in carefully selected patients with documented coagulopathy to mitigate pro-coagulant effects and manage thromboembolic risks [21:7]. Pleiotropic endothelial-protective agents like defibrotide are also under active investigation for their potential direct vasculoprotective and fibrinolytic properties [23:6].
¶ Therapeutic Apheresis & Immunoglobulins
Extracorporeal therapies and immunomodulators are being explored as alternative supportive interventions in post-acute care [9:5]:
- Emerging Status: Emerging therapies, including intravenous immunoglobulin (IVIg) and therapeutic apheresis, are under investigation as potential supportive interventions for Long COVID [9:6].
- Clinical Trial Limitations: These interventions currently lack robust, large-scale randomized controlled trials to confirm their efficacy, optimize patient selection, or establish safety, emphasizing the need for rigorous research before clinical implementation [9:7].
¶ Immunomodulators & Anti-Inflammatories
Systemic autoimmunity, autoantibodies, and chronic inflammatory cascades represent major proposed mechanisms underlying Long COVID [1:5][2:7][4:7].
- IVIG and Corticosteroids: Immunomodulating therapies such as intravenous immunoglobulin (IVIg) and anti-inflammatory drugs like corticosteroids (e.g., dexamethasone) are under investigation as supportive interventions [9:8]. While observational data and small clinical series show some potential for these agents in managing severe post-viral complications and inflammatory flares, they lack support from robust, large-scale trials [9:9].
¶ Metformin
Repurposed pharmacological agents are being evaluated for their ability to target underlying mechanisms like viral persistence, inflammation, and cellular dysfunction [9:10].
- Clinical Evidence: Among non-antiviral pharmacological treatments, Metformin has the strongest clinical evidence supporting its use in Long COVID management, notably from large phase 3 randomized clinical trials [9:11]. Metformin is being evaluated for its potential anti-inflammatory and metabolic properties [9:12].
¶ Oxaloacetate (OAA)
Oxaloacetate (OAA) is being evaluated in clinical trials for its potential to support cellular energy metabolism and improve post-viral fatigue:
- Efficacy Findings: In a double-blind, randomized, controlled trial (the REGAIN trial), oral oxaloacetate (OAA) administered at 2,000 mg/day was well tolerated and demonstrated significantly greater improvements in fatigue and total symptom burden at day 21, with significant gains in cognitive performance [32].
¶ Olfactory Training, PEA, and Luteolin
Post-viral sensory deficits represent a prominent phenotypic cluster that can be addressed with sensory and nutritional interventions:
- Clinical Evidence: A randomized clinical trial evaluated the combination of olfactory rehabilitation paired with oral supplementation of Palmitoylethanolamide (PEA) and Luteolin, demonstrating a significantly greater improvement in olfactory dysfunction compared to olfactory rehabilitation alone [33].
¶ Alternative Interventions Lacking Compelling Evidence
A living systematic review evaluated the efficacy of multiple alternative pharmacological and non-pharmacological therapies for the management of Post-COVID-19 Condition [8:1]:
- Interventions Checked: The review analyzed several commonly proposed interventions, including vortioxetine, leronlimab, combined probiotics-prebiotics, coenzyme Q10, amygdala and insula retraining, combined L-arginine and vitamin C, inspiratory muscle training, transcranial direct current stimulation, hyperbaric oxygen, and educational mobile applications [8:2].
- Lack of Compelling Evidence: The meta-analysis found no compelling evidence to support the clinical effectiveness of these specific interventions, concluding that they should not be adopted into standard practice without further rigorous randomized trials [8:3].
¶ 8. Clinical Safety, Toxicology, & Monitoring Protocols
To ensure clinical safety when evaluating or administering experimental or off-label interventions for Long COVID, clinicians must adhere to strict toxicological boundaries, screening guidelines, and predefined stopping rules.
¶ Pregnancy & Lactation Safety
- Lack of Safety Data: The safety profiles of many off-label or experimental therapeutics discussed—including low-dose naltrexone (LDN), defibrotide, next-generation oral RdRp inhibitors, and repurposed agents—have not been established in pregnant or lactating populations.
- Clinical Action: These interventions require extreme caution and a comprehensive risk-benefit analysis in pregnant and lactating patients due to the potential for unrecognized fetal or infant toxicity.
¶ Medication Interactions & Toxicities
- CYP450 Metabolism: Oral antivirals and other repurposed small molecules can be substrates, inhibitors, or inducers of hepatic cytochrome P450 enzymes. This creates a risk for clinically significant drug-drug interactions when co-administered with common cardiovascular, neuropsychiatric, or metabolic medications, requiring clinicians to conduct a comprehensive medication review prior to initiation.
- Anticoagulants: Concomitant use of anticoagulants (such as low-molecular-weight heparin or direct oral anticoagulants) co-administered with other antiplatelets, non-steroidal anti-inflammatory drugs (NSAIDs), or systemic corticosteroids elevates the risk of gastrointestinal, systemic, and life-threatening hemorrhage, requiring careful monitoring.
¶ Structured Clinical Limits & Stopping Rules
Clear clinical thresholds must be established to determine when to discontinue experimental therapies:
- Experimental Therapy Monitoring: Alternative or trial therapies like Low-Dose Naltrexone (LDN) show potential based on observational studies but lack robust, large-scale trial support to confirm efficacy or guide standardized clinical use [9:13]. In clinical practice, if there is no documented, measurable improvement in a patient's fatigue or pain scores within an appropriate clinical observation period, clinicians typically discontinue the trial.
¶ 9. Evidence summary table (human outcomes)
The following matrix summarizes the clinical efficacy, consistency, and evidence quality of primary therapeutic and rehabilitative interventions for Long COVID.
| Intervention / Target | Effect* | Consistency** | Evidence quality | Trials*** | Notes (clinical population, duration, and protocols) |
|---|---|---|---|---|---|
| Energy Pacing (PEM & Fatigue) | High | Moderate | Cohort Studies | Structured pacing protocols reduce post-exertional symptoms and improve overall health-related quality of life [7:5][25:11]. | |
| Metformin (Long COVID Management) | High | High | Phase 3 RCTs | Non-antiviral drug with the strongest clinical evidence from large phase 3 trials [9:14]. | |
| Low-Dose Naltrexone (Symptom Support) | Moderate | Low | Observational Studies | Alternative therapy that shows potential based on observational studies, but lacks robust, large-scale RCT validation [9:15]. | |
| Oxaloacetate (OAA) | High | Moderate | RCTs | 2,000 mg/day OAA; trial demonstrates significantly earlier fatigue relief and cognitive gains [32:1]. | |
| Autonomic Dysfunction Screening | Moderate | Low | Clinical Practice | General dysautonomia is a recognized manifestation that often goes unnoticed by standard clinical diagnostic tests [18:10][3:6]. | |
| Pulmonary / Cardiorespiratory Rehabilitation | High | Moderate | Systematic Reviews & RCTs | Supervised, combined physical and ventilatory training over 4–8 weeks; significantly improves submaximal walking capacity, physical function, and fatigue [5:5][6:3][26:1]. | |
| RdRp Inhibitors (GS-441524 Derivatives) | Moderate | Low | Clinical Trials | Next-generation oral inhibitors of RdRp under active development to reduce post-acute sequelae [31:1]. | |
| Standard Thromboprophylaxis (Coagulopathy) | Moderate | Low | Clinical Practice | LMWH or DOACs may be considered in appropriate clinical settings to mitigate pro-coagulant effects [21:8]. | |
| Olfactory Rehabilitation + PEA & Luteolin | High | Moderate | RCTs | Supplementation combined with olfactory training significantly improves post-COVID olfactory dysfunction [33:1]. | |
| Overly Intense Exercise (in PEM) | High | Moderate | Clinical Consensus | Contraindicated for PEM/PESE; overly intense activity can trigger PEM/PESE [14:29]. | |
| Vaccination (Primary Prevention) | High | High | Cohort Studies | Vaccination is associated with reduced risk; odds of PCC are lower per 10-fold increase in anti-spike IgG post-vaccination [27:2]. |
- *Effect: Compact renderer encoding:
<effect e="[dir][mag][impact]"></effect>wheredir=u|d|e|q(up/down/equal/unclear),mag=0|1|2|3(0-3 magnitude),impact=p|n|x(positive/negative/neutral). Examples:d2p= moderate decrease, positive;u2n= moderate increase, negative;q0x= unclear/unknown. - **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- ***Trials: Level of evidence informing this outcome (Meta-Analyses, RCTs, Cohort Studies, or Observational)
¶ 10. References
Bonilla H, Peluso MJ, Rodgers K. Therapeutic trials for long COVID-19: A call to action from the interventions taskforce of the RECOVER initiative. Frontiers in Immunology. 2023. https://pubmed.ncbi.nlm.nih.gov/36969241/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Peluso MJ, Deeks SG. Mechanisms of long COVID and the path toward therapeutics. Cell. 2024. https://pubmed.ncbi.nlm.nih.gov/39326415/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Makhluf H, Madany H, Kim K. Long COVID: Long-Term Impact of SARS-CoV2. Diagnostics (Basel). 2024. https://pubmed.ncbi.nlm.nih.gov/38611624/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chatterjee D, Maparu K. Long COVID syndrome: exploring therapies for managing and overcoming persistent symptoms. Inflammopharmacology. 2025. https://pubmed.ncbi.nlm.nih.gov/40622467/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Yue Y, Han X, Chen Q. The effect of pulmonary rehabilitation for post-acute sequelae of SARS-CoV-2 infection in patients: a systematic review and meta-analysis. Frontiers in Rehabilitation Sciences. 2025. https://pubmed.ncbi.nlm.nih.gov/41244103/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Ghram A, Latiri I, Methnani J. Effects of cardiorespiratory rehabilitation program on submaximal exercise in patients with long-COVID-19 conditions: a systematic review of randomized controlled trials and recommendations for future studies. Expert Review of Respiratory Medicine. 2023. https://pubmed.ncbi.nlm.nih.gov/38063359/ ↩︎ ↩︎ ↩︎ ↩︎
Parker M, Sawant HB, Flannery T. Effect of using a structured pacing protocol on post-exertional symptom exacerbation and health status in a longitudinal cohort with the post-COVID-19 syndrome. Journal of Medical Virology. 2023. https://pubmed.ncbi.nlm.nih.gov/36461167/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zeraatkar D, Ling M, Kirsh S. Interventions for the management of long covid (post-covid condition): living systematic review. BMJ. 2024. https://pubmed.ncbi.nlm.nih.gov/39603702/ ↩︎ ↩︎ ↩︎ ↩︎
Livieratos A, Gogos C, Akinosoglou K. Beyond Antivirals: Alternative Therapies for Long COVID. Viruses. 2024. https://pubmed.ncbi.nlm.nih.gov/39599909/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Soriano JB, Murthy S, Marshall JC. A clinical case definition of post-COVID-19 condition by a Delphi consensus. The Lancet Infectious Diseases. 2022. https://pubmed.ncbi.nlm.nih.gov/34951953/ ↩︎ ↩︎ ↩︎
Wanga V, Chevinsky JR, Dimitrov LV. Long-Term Symptoms Among Adults Tested for SARS-CoV-2 - United States, January 2020-April 2021. MMWR Morbidity and Mortality Weekly Report. 2021. https://pubmed.ncbi.nlm.nih.gov/34499626/ ↩︎ ↩︎ ↩︎ ↩︎
Maripuri M, Dey A, Honerlaw J. Characterization of Post-COVID-19 Definitions and Clinical Coding Practices: Longitudinal Study. Online Journal of Public Health Informatics. 2024. https://pubmed.ncbi.nlm.nih.gov/38700929/ ↩︎ ↩︎
National Institute for Health and Care Excellence (NICE). COVID-19 rapid guideline: managing the long-term effects of COVID-19. NICE Guideline, No. 188. 2024. https://pubmed.ncbi.nlm.nih.gov/33555768/ ↩︎ ↩︎ ↩︎
Cheng AL, Herman E, Abramoff B. Multidisciplinary collaborative guidance on the assessment and treatment of patients with Long COVID: A compendium statement. PM & R. 2025. https://pubmed.ncbi.nlm.nih.gov/40261198/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kassymbek S, Abduldayeva A, Safonov N. Global prevalence of post-COVID-19 condition (Long COVID): a systematic review and meta-analysis of observational studies. Frontiers in Public Health. 2026. https://pubmed.ncbi.nlm.nih.gov/42428921/ ↩︎ ↩︎
Archambault PM, Rosychuk RJ, Audet M. Post-COVID-19 condition symptoms among emergency department patients tested for SARS-CoV-2 infection. Nature Communications. 2024. https://pubmed.ncbi.nlm.nih.gov/39349926/ ↩︎
Hoffmann K, Stingl M, O'Mahony L. A Practical Approach to Tailor the Term Long COVID for Diagnostics, Therapy and Epidemiological Research for Improved Long COVID Patient Care. Infectious Diseases and Therapy. 2024. https://pubmed.ncbi.nlm.nih.gov/39127990/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lee E, Ozigbo AA, Varon J. Mitochondrial Reactive Oxygen Species: A Unifying Mechanism in Long COVID and Spike Protein-Associated Injury: A Narrative Review. Biomolecules. 2025. https://pubmed.ncbi.nlm.nih.gov/41008646/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Toepfner N, Brinkmann F, Augustin S. Long COVID in pediatrics-epidemiology, diagnosis, and management. European Journal of Pediatrics. 2024. https://pubmed.ncbi.nlm.nih.gov/38279014/ ↩︎ ↩︎
Kelly JD, Curteis T, Rawal A. SARS-CoV-2 post-acute sequelae in previously hospitalised patients: systematic literature review and meta-analysis. European Respiratory Review. 2023. https://pubmed.ncbi.nlm.nih.gov/37437914/ ↩︎
Mo CC, Richardson E, Calabretta E. Endothelial injury and dysfunction with emerging immunotherapies in multiple myeloma, the impact of COVID-19, and endothelial protection with a focus on the evolving role of defibrotide. Blood Reviews. 2024. https://pubmed.ncbi.nlm.nih.gov/38852017/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Hawke LD, Nguyen ATP, Wang W. Systematic review of interventions for mental health, cognition and psychological well-being in long COVID. BMJ Mental Health. 2024. https://pubmed.ncbi.nlm.nih.gov/39384321/ ↩︎
Richardson E, Mo CC, Calabretta E. Defibrotide for Protecting Against and Managing Endothelial Injury in Hematologic Malignancies and COVID-19. Biomolecules. 2025. https://pubmed.ncbi.nlm.nih.gov/40723876/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
An Y, Guo Z, Fan J. Prevalence and measurement of post-exertional malaise in post-acute COVID-19 syndrome: A systematic review and meta-analysis. General Hospital Psychiatry. 2024. https://pubmed.ncbi.nlm.nih.gov/39490027/ ↩︎ ↩︎
Twomey R, DeMars J, Franklin K. Chronic Fatigue and Postexertional Malaise in People Living With Long COVID: An Observational Study. Physical Therapy. 2022. https://pubmed.ncbi.nlm.nih.gov/35079817/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Li S, Dai B, Hou Y. Effect of pulmonary rehabilitation for patients with long COVID-19: a systematic review and meta-analysis of randomized controlled trials. Therapeutic Advances in Respiratory Disease. 2025. https://pubmed.ncbi.nlm.nih.gov/40083165/ ↩︎ ↩︎
Bouwmans P, Malahe SRK, Messchendorp AL. Post COVID-19 condition imposes significant burden in patients with advanced chronic kidney disease: A nested case-control study. International Journal of Infectious Diseases. 2024. https://pubmed.ncbi.nlm.nih.gov/38428480/ ↩︎ ↩︎ ↩︎
Carpio-Orantes LD, Trelles-Hernández D, García-Méndez S. Clinical-epidemiological characterization of patients with long COVID in Mexico. Gaceta Medica de Mexico. 2024. https://pubmed.ncbi.nlm.nih.gov/39116863/ ↩︎
Pazukhina E, Rumyantsev M, Baimukhambetova D. Event rates and incidence of post-COVID-19 condition in hospitalised SARS-CoV-2 positive children and young people and controls across different pandemic waves: exposure-stratified prospective cohort study in Moscow (StopCOVID). BMC Medicine. 2024. https://pubmed.ncbi.nlm.nih.gov/38302974/ ↩︎ ↩︎ ↩︎
Domingo JL. Differentiating COVID-19 vaccine-related adverse events from long COVID: A comprehensive review of clinical manifestations, pathophysiology, and diagnostic approaches. Vaccine. 2025. https://pubmed.ncbi.nlm.nih.gov/41076807/ ↩︎ ↩︎ ↩︎
Wang Z, Yang L, Song XQ. Oral GS-441524 derivatives: Next-generation inhibitors of SARS-CoV-2 RNA-dependent RNA polymerase. Frontiers in Immunology. 2022. https://pubmed.ncbi.nlm.nih.gov/36561747/ ↩︎ ↩︎
Vernon SD, Rond C, Bell J. REGAIN: a randomized controlled clinical trial of oxaloacetate for improving the symptoms of long COVID. Frontiers in Neuroscience. 2025. https://pubmed.ncbi.nlm.nih.gov/40757370/ ↩︎ ↩︎
Veronese N, Bonica R, Cotugno S. Interventions for Improving Long COVID-19 Symptomatology: A Systematic Review. Viruses. 2022. https://pubmed.ncbi.nlm.nih.gov/36146672/ ↩︎ ↩︎