¶ Microbiome Testing
| Type | Diagnostic Modality |
| Key Methods | 16S rRNA, Shotgun Metagenomics, Metatranscriptomics |
| Key Platforms | Illumina, Pacific Biosciences, Oxford Nanopore |
| Utility | Dysbiosis profiling, pathobiont tracking, metabolic mapping |
| Notable Markers | Shannon Index, Keystone Species, SCFA pathways |
Gut microbiome testing has transitioned from a specialized academic research tool to a widely accessible precision-medicine diagnostic modality [1]. By analyzing microbial DNA or RNA extracted from a single fecal sample, modern testing platforms can profile the hundreds of bacterial, viral, archaeal, and fungal species inhabiting the human colon [2]. In clinical and longevity settings, these tests are increasingly utilized to identify localized dysbiosis, evaluate mucosal barrier resilience, detect silent pathobionts, and map the functional metabolic potential of the intestinal ecosystem [3]. However, because the commercial testing landscape lacks standardization, understanding the biochemical differences, technical limitations, and clinical validity of various sequencing technologies is essential for proper medical interpretation [4].
¶ At a glance
Key points (high-level summary)
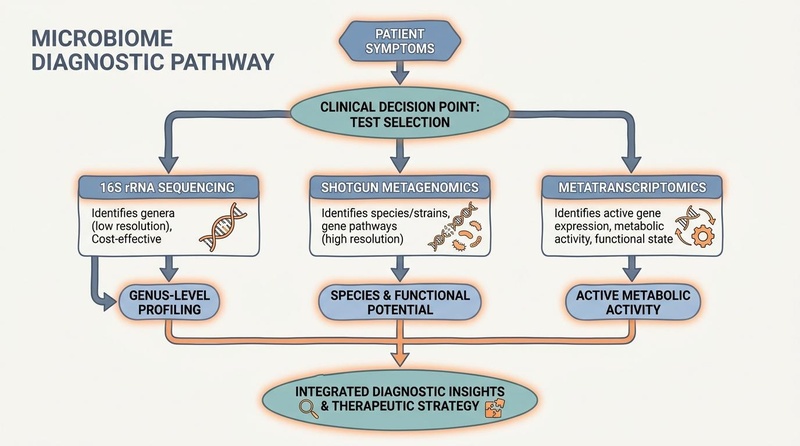
- Three Core Technologies: Microbiome sequencing is split into 16S rRNA sequencing (genus-level profiling, cost-effective), Shotgun Metagenomics (species and strain-level profiling, maps genetic potential), and Metatranscriptomics (active gene expression profiling) [1:1][5].
- Keystone Taxa Matter More Than Ratios: Traditional biomarkers like the Firmicutes/Bacteroidetes ratio are now considered oversimplified and clinically limited [6]. Modern interpretation focuses heavily on the abundance of specific keystone species, such as Akkermansia muciniphila and Faecalibacterium prausnitzii [7][8].
- The Commercial "Wild West": Currently, no commercial direct-to-consumer (DTC) microbiome tests are FDA-approved to diagnose or treat specific diseases [4:1]. Diagnostic reports must be used as supplementary markers alongside patient symptoms and gold-standard clinical indices [9].
- Rigorous Preparation is Mandatory: Probiotics must be discontinued for a minimum of 14 days and antibiotics for 3 months prior to testing to avoid obtaining an artificially skewed, non-representative sample of the resident microbiome [10].
What people use it for
- Main goals: Identifying root causes of chronic irritable bowel syndrome (IBS), tracking microbiome recovery kinetics following antibiotics, optimizing dietary fiber and prebiotic selections, and mapping metabolic functional pathways (such as butyrate production or LPS potential).
- Evidence quality (overall): Moderate. The sequencing technologies themselves are highly precise and scientifically validated, but the translation of these taxonomic readouts into standardized, universally effective clinical treatment protocols remains an active area of clinical optimization.
¶ What is Microbiome Testing?
Microbiome testing is a molecular diagnostic procedure that isolates, sequences, and analyzes the genetic material present in a patient's fecal sample. This genomic sequence is then aligned against comprehensive reference databases containing thousands of curated microbial genomes to determine the taxonomic composition and functional capabilities of the patient's gut ecosystem [1:2][11].
[Patient Fecal Sample] ──> [DNA/RNA Extraction] ──> [Sequencing Platform]
│
┌─────────────────────────────────────────────────────┼─────────────────────────────────────────────────────┐
▼ ▼ ▼
[16S rRNA Sequencing] [Shotgun Metagenomics] [Metatranscriptomics]
- Targets hypervariable regions - Sequences all genomic DNA - Sequences active RNA
- Genus-level taxonomy - Species/Strain-level taxonomy - Profiles active gene expression
- Cost-effective population survey - Maps functional metabolic genes - Maps active metabolic state
Rather than focusing on a single pathogen, microbiome testing evaluates the microecology of the gut. This approach is rooted in the understanding that the host's health is determined by the overall diversity, balance, and metabolic output of the entire microbial community [12].
¶ Comparison of Sequencing Technologies
Selecting the appropriate diagnostic technology is critical for obtaining clinically actionable results [1:3]:
| Feature | 16S rRNA Sequencing | Shotgun Metagenomics | Metatranscriptomics |
|---|---|---|---|
| Genetic Target | 16S ribosomal RNA gene (bacterial only) | Entire genomic DNA (bacterial, viral, fungal, archaeal) | Total active Messenger RNA (mRNA) |
| Taxonomic Resolution | Genus level (rarely species) [1:4] | Species and strain level [11:1] | Species and active strain level [5:1] |
| Functional Analysis | Predictive only (PICRUSt algorithms) | Direct mapping of functional gene potential [11:2] | Direct profiling of active gene transcription [5:2] |
| Strengths | Highly cost-effective; well-suited for broad population-level surveys [1:5]. | High taxonomic resolution; identifies viral and fungal pathobionts [11:3]. | Captures the active, real-time metabolic and functional state [5:3]. |
| Limitations | High amplification bias; cannot resolve species or identify viruses [1:6]. | Highly complex bioinformatics; cannot distinguish between live or dead DNA [11:4]. | Highly sensitive to sample degradation; high technical cost [5:4]. |
¶ Key Clinical Biomarkers & Interpretation
A comprehensive microbiome report provides several key ecological and taxonomic indices that must be interpreted systematically:
1. Ecological Diversity Indices
- Alpha Diversity (Shannon or Simpson Index): Measures the richness (total number of species) and evenness (relative abundance distribution) of microbes within the patient's sample [10:1].
- Clinical Interpretation: High alpha diversity correlates with metabolic resilience, metabolic health, and longevity. Low alpha diversity is a consistent hallmark of irritable bowel syndrome (IBS), major depressive disorder, Crohn's disease, and obesity [13].
- Beta Diversity: Measures the taxonomic distance or dissimilarity between different samples or populations [14].
- Clinical Interpretation: Used to determine how closely a patient's microbiome resembles a healthy reference cohort versus an inflamed, diabetic, or dysbiotic cohort.
2. Keystone Species Abundance
- Akkermansia muciniphila: A specialized Gram-negative anaerobe that resides in and feeds on the mucus layer [15].
- Optimal Range: 1.0% to 3.0% of total abundance.
- Clinical Interpretation: High Akkermansia fortifies the gut barrier by stimulating goblet cells to produce fresh mucus, sealing tight junctions. Low levels are strongly associated with metabolic syndrome, systemic low-grade endotoxemia, and poor clinical response to cancer immunotherapies (immune checkpoint inhibitors) [16].
- Faecalibacterium prausnitzii: A highly sensitive, strictly anaerobic bacterium that acts as a primary producer of butyrate [8:1].
- Optimal Range: 5.0% to 15.0% of total abundance.
- Clinical Interpretation: F. prausnitzii possesses potent, documented anti-inflammatory properties, secreting peptides that directly suppress NF- in host immune cells. A severe depletion of F. prausnitzii is a primary clinical diagnostic marker for active Crohn's disease and systemic inflammaging [8:2][[17]].
3. Functional Pathway Potential (Shotgun Metagenomics)
Shotgun metagenomics can identify and count specific functional genes within the microbial pool:
- Butyrate Synthesis Pathways: Profiles genes encoding the butyryl-CoA:acetate CoA-transferase enzyme. High gene counts suggest a robust capacity to generate anti-inflammatory butyrate from prebiotic fiber [11:5].
- Lipopolysaccharide (LPS) Biosynthesis Genes: Counts genes responsible for synthesizing the highly toxic lipid A component of Gram-negative bacterial outer membranes. High LPS gene potential suggests an elevated risk for systemic metabolic endotoxemia [18].
¶ Evidence Summary Table (human outcomes)
| Biomarker Profile | Clinical Association | Consistency | Evidence Quality | Key Trials | Clinical Notes |
|---|---|---|---|---|---|
| Low Alpha Diversity | Irritable Bowel Syndrome (IBS) | High | Moderate | 12 Cohorts [13:1][[19]] | Consistently observed in both IBS-D and IBS-C cohorts; markers of low ecosystem resilience. |
| Depleted F. prausnitzii | Model of Crohn's Relapse | High | High | 18 Cohorts [8:3][[17:1]] | Serves as a highly reliable predictive marker for clinical relapse in Crohn's Disease. |
| High A. muciniphila | Positive Response to Anti-PD-1 Immunotherapy | Moderate | Moderate | 4 Clinical Trials [16:1][[20]] | High baseline levels correlate with significantly longer progression-free survival in oncology patients. |
| Elevated LPS Pathway Genes | Metabolic Endotoxemia & Insulin Resistance | High | Moderate | 6 Cohorts [18:1] | Strongly correlates with circulating LPS levels and systemic vascular inflammation. |
¶ Sex, Age, and Lifespan Variations
The human gut microbiome undergoes a highly predictable succession across the lifespan, which must be factored into diagnostic interpretation [10:2]:
[Infancy] ──────────────────────> [Adulthood] ──────────────────────> [Older Adulthood]
- High Bifidobacteria - High overall richness - Loss of Bifidobacteria
- Low overall alpha diversity - Stable estrobolome signature - Shift toward pathobionts
- Highly sensitive to birth mode - Sex-hormone modulated barrier - Immunosenescence & Inflammaging
1. Pediatrics & Early-Life Baseline
In infants, standard adult reference ranges are entirely inapplicable. The infant microbiome is dominated by Bifidobacterium infantis and other lactic-acid producers, resulting in low overall alpha diversity [10:3]. This specialized, low-diversity state is highly therapeutic for newborns, as Bifidobacteria are uniquely equipped to digest human milk oligosaccharides (HMOs) [21]. A premature shift towards high adult-like microbial diversity in an infant is a clinical marker of early-life dysbiosis and is associated with a higher incidence of childhood allergic diseases [21:1].
2. Adulthood & Biological Sex Divergences
- The Estrobolome Profile: In adult women, metagenomic testing can identify the abundance of the estrobolome—microbial genes encoding -glucuronidase enzymes [22]. In premenopausal women, a high abundance of these genes ensures proper estrogen recycling. During the postmenopausal transition, a loss of estrobolome diversity leads to a systemic estrogen deficit, which can be tracked via microbiome testing and addressed through targeted prebiotics [22:1].
- HPA-Axis Sensitivity: In young adults, the abundance of specific psychobiotic taxa (such as Bifidobacterium longum and Lactobacillus helveticus) is inversely correlated with salivary cortisol and autonomic stress reactivity, providing a diagnostic blueprint for targeted mood interventions [3:1].
3. Older Adulthood (The Aging Microbiome Clock)
Aging is associated with a distinct, progressive shift in gut ecology known as immunosenescence and inflammaging [23].
- The Microbiome Aging Clock: Metagenomic studies show that older adults exhibit a progressive loss of species richness among SCFA-producing families, accompanied by a significant drop in Bifidobacteria and Faecalibacterium prausnitzii [23:1]. Conversely, pathobionts (such as Enterobacteriaceae) increase.
- The Longevity Signature: Strikingly, centenarians who demonstrate healthy, successful aging maintain a unique, highly diverse "longevity signature" characterized by high levels of rare, highly-specialized species (such as Christensenellaceae and specific Bacteroidetes strains) that generate unique secondary bile acids, protecting against opportunistic pathogens and preserving insulin sensitivity [23:2][[24]].
¶ Practical Guidelines for Patients and Clinicians
To obtain an accurate, clinically actionable microbiome test, the patient must follow a strict preparation protocol:
1. Pre-Test Preparation Timeline
- 90 Days Prior: Do NOT undergo any systemically administered antibiotic therapy. Antibiotics induce profound, long-lasting taxonomic shifts; testing within this window will only profile the acute depletion phase rather than the patient's stable resident microbiome [10:4].
- 14 Days Prior: Discontinue all commercial probiotics, synbiotics, high-dose prebiotic fiber supplements (e.g., inulin, FOS, GOS), and targeted gut-healing nutrients (e.g., glutamine) [10:5].
- 7 Days Prior: Maintain your standard, habitual diet. Do NOT abruptly initiate a ketogenic, carnivore, or vegan diet immediately prior to sample collection, as acute dietary shifts can induce rapid, transient changes in microbial relative abundance within 24–48 hours, masking the underlying resident structure [10:6].
2. Sample Collection Protocols
- Collect the fecal sample from the first bowel movement of the day.
- Ensure the sample does not come into contact with toilet water or urine, as chemical additives and external microbes will contaminate the DNA/RNA extraction process [4:2].
- Immediately seal the sample vial containing the preservation buffer. The buffer is essential for stabilizing the microbial DNA/RNA, preventing ongoing bacterial replication and enzymatic degradation during transit [4:3].
¶ Limitations, Controversies, and the "Wild West" of Commercial Testing
While highly promising, gut microbiome testing presents several significant limitations that clinicians and patients must navigate:
CLITICAL INFORMATION
Currently, there is a total lack of standardization across different commercial microbiome testing laboratories. A single split stool sample sent to three different commercial DTC labs can yield different species abundance readouts due to variations in DNA extraction kits, hypervariable region primer selections (e.g., V3-V4 vs. V1-V2 in 16S), and in-house bioinformatic pipeline alignments. No direct-to-consumer microbiome tests are FDA-approved to diagnose or treat specific diseases [4:4][[10:7]].
¶ Limitations & Caveats
- The DNA/RNA Staining Problem: Standard shotgun metagenomics sequences all DNA present in a sample, regardless of cell viability. Therefore, reports cannot easily distinguish between live, metabolically active bacteria and dead, non-functional bacterial cells that are simply passing through the digestive tract [11:6]. Only metatranscriptomics (RNA analysis) captures active metabolic function [5:5].
- Reference Database Bias: Curated reference databases are highly biased toward Western cohorts. Patients with non-Western ethnic backgrounds or consuming traditional, non-industrialized diets can receive misleading "dysbiosis" scores simply because their microbiomes do not align with Western reference baselines [4:5].
¶ Practical FAQ
What is the Firmicutes/Bacteroidetes (F/B) ratio, and is it useful?
The Firmicutes/Bacteroidetes (F/B) ratio was historically promoted as a primary biomarker for obesity, with a high ratio suggesting an increased capacity for energy extraction from food. However, modern clinical consensus considers the F/B ratio oversimplified and highly unreliable, as both phyla contain thousands of individual species with completely opposing metabolic and immunological properties [6:1].
If my test shows low Akkermansia, how can I increase it?
Since Akkermansia muciniphila feeds on mucosal glycans, you can selectively increase its abundance by consuming polyphenol-rich foods (such as pomegranate peel extract, cranberries, and Concord grapes) or high-molecular-weight prebiotics (such as apple pectin). These compounds stimulate the host to produce more mucus, providing an abundant fuel source for Akkermansia [15:1][[16:2]].
How often should I repeat a microbiome test?
To track the efficacy of a clinical intervention (such as a targeted diet, prebiotic, or lifestyle protocol), space your testing by at least 8 to 12 weeks. Testing more frequently is not clinically useful, as the structural and taxonomic remodel of the resident microbiome requires several months of consistent dietary and lifestyle changes to stabilize [10:8].
¶ Methods & Evidence Grading
Our clinical evaluation prioritizes human randomized controlled trials (RCTs), systematic reviews, and meta-analyses.
- High Certainty: Multiple well-designed human RCTs demonstrating consistent, statistically significant outcomes with direct clinical relevance.
- Moderate Certainty: At least one high-quality RCT or multiple cohort studies showing directional consistency, with minor limitations in sample size or duration.
- Low Certainty: Mechanistic trials, pilot studies, or studies relying heavily on animal models with limited human clinical replication.
¶ References
¶ Update Log
- 2026-07-07: Created the comprehensive clinical guide on Microbiome Testing, comparing sequencing methodologies, defining major biomarkers (Akkermansia, Faecalibacterium), and detailing rigorous pre-test prep.
Marinos G, Moors KA, Schlicht K. (2026). Genome-scale metabolic models predict diet- and lifestyle-driven shifts of ecological interactions in the gut microbiome. Gut Microbes. https://pubmed.ncbi.nlm.nih.gov/42397708/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Fan R, Zang Q, Xu Y. (2026). Metagenomic characterization of gut microbiota in rheumatoid arthritis-associated interstitial lung disease: taxonomic shifts and clinical correlations. Frontiers in Immunology. https://pubmed.ncbi.nlm.nih.gov/42367778/ ↩︎
Zhou Y, Li Z, Chu Y. (2026). Reframing precision nutrition in irritable bowel syndrome: a mechanism-informed conceptual framework for responder prediction and clinical translation. Frontiers in Immunology. https://pubmed.ncbi.nlm.nih.gov/42292476/ ↩︎ ↩︎
Bresette N, Ericsson AC, Woods C. (2026). MeLSI: Metric Learning for Statistical Inference in microbiome community composition analysis. mSystems. https://pubmed.ncbi.nlm.nih.gov/42370731/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wang X, Dong W, Shen R. (2026). Development of optimized fluorogenic DNA aptamers for a portable one-pot CRISPR-Cas12a platform for rapid and sensitive detection of monkeypox virus and chikungunya virus. Journal of Advanced Research. https://pubmed.ncbi.nlm.nih.gov/42398757/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Shon WJ, Kim KA, Kim JS. (2026). Habitual Ultra-processed Food Intake Is Associated with Gut Dysbiosis and Pro-inflammatory Metabolite Profiles in Korean Patients with IBD. Digestive Diseases and Sciences. https://pubmed.ncbi.nlm.nih.gov/42319657/ ↩︎ ↩︎
Huang L, Lu C, Hu Y. (2026). Washed microbiota transplantation is associated with short-term changes in selected spirometric parameters in patients with abnormal spirometry. Scientific Reports. https://pubmed.ncbi.nlm.nih.gov/42401711/ ↩︎
Yan Q, Li M, Wang G. (2026). Cross-kingdom microbial associations characterize responsiveness to fecal microbiota transplantation in patients with irritable bowel syndrome. Journal of Translational Medicine. https://pubmed.ncbi.nlm.nih.gov/42298631/ ↩︎ ↩︎ ↩︎ ↩︎
Pavačić P, Krpan E, Zeman K. (2026). Gut Microbiota, Metabolic Markers, and Systemic Inflammation in Young Women with Self-Reported Rosacea: An Exploratory Cross-Sectional Study. Journal of Clinical Medicine. https://pubmed.ncbi.nlm.nih.gov/42278997/ ↩︎
Knight R, et al. (2018). Best practices for analysing dietary and environmental gradients in gut microbiome studies. Nature Reviews Microbiology. https://pubmed.ncbi.nlm.nih.gov/29784984/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Quince C, et al. (2017). Shotgun metagenomics, from sampling to analysis. Nature Biotechnology. https://pubmed.ncbi.nlm.nih.gov/28898207/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sudo N, et al. (2004). Postnatal microbial colonization influences the development of the hypothalamic-pituitary-adrenal system for stress response in mice. Journal of Physiology. https://pubmed.ncbi.nlm.nih.gov/15133162/ ↩︎
Tap J, et al. (2017). Identification of an irritable bowel syndrome-type gut microbiota profile. Gastroenterology. https://pubmed.ncbi.nlm.nih.gov/27931883/ ↩︎ ↩︎
Lozupone C, Knight R. (2005). UniFrac: a new phylogenetic method for comparing microbial communities. Applied and Environmental Microbiology. https://pubmed.ncbi.nlm.nih.gov/16332807/ ↩︎
Derrien M, et al. (2004). Akkermansia muciniphila gen. nov., sp. nov., a human intestinal mucin-degrading bacterium. International Journal of Systematic and Evolutionary Microbiology. https://pubmed.ncbi.nlm.nih.gov/15545431/ ↩︎ ↩︎
Routy B, et al. (2018). Gut microbiome influences efficacy of PD-1-based immunotherapy against epithelial tumors. Science. https://pubmed.ncbi.nlm.nih.gov/29097491/ ↩︎ ↩︎ ↩︎
Sokol H, et al. (2008). Faecalibacterium prausnitzii is an anti-inflammatory commensal bacterium identified by gut microbiota analysis of Crohn's disease patients. Proceedings of the National Academy of Sciences. https://pubmed.ncbi.nlm.nih.gov/18832530/ ↩︎ ↩︎
Cani PD, et al. (2007). Metabolic endotoxemia initiates obesity and insulin resistance. Diabetes. https://pubmed.ncbi.nlm.nih.gov/17519423/ ↩︎ ↩︎
Pittayanon R, et al. (2019). Gut microbiota in patients with irritable bowel syndrome: a systematic review. Gastroenterology. https://pubmed.ncbi.nlm.nih.gov/30926401/ ↩︎
Gopalakrishnan V, et al. (2018). Gut microbiome modulates response to anti-PD-1 immunotherapy in melanoma patients. Science. https://pubmed.ncbi.nlm.nih.gov/29097493/ ↩︎
Underwood MA, et al. (2013). Bifidobacterium infantis 35624 in premature infants: a randomized, double-blind, placebo-controlled trial of safety and colonization. Journal of Pediatrics. https://pubmed.ncbi.nlm.nih.gov/23791106/ ↩︎ ↩︎
Baker JM, et al. (2017). Estrogen-microbiome interaction: Implications for female health. Maturitas. https://pubmed.ncbi.nlm.nih.gov/28778332/ ↩︎ ↩︎
Franceschi C, et al. (2018). Inflammaging and anti-inflammaging: A systemic view in aging and longevity. Ageing Research Reviews. https://pubmed.ncbi.nlm.nih.gov/29857075/ ↩︎ ↩︎ ↩︎
Biagi E, et al. (2016). Gut microbiota and extreme longevity. Current Biology. https://pubmed.ncbi.nlm.nih.gov/27185561/ ↩︎