¶ title: Fasting and Time-Restricted Feeding: Deep Dive
description: Comprehensive analysis of fasting protocols (16:8, OMAD, prolonged), metabolic health, autophagy, safety, and evidence-based longevity benefits.
published: 1
date: 2026-07-06T18:24:03.096Z
tags: autophagy, deep-dive, diet, fasting, longevity, metabolic-health, weight-loss, time-restricted-feeding
editor: markdown
dateCreated: 2026-07-06T18:24:03.096Z
¶ Fasting and Time-Restricted Feeding: Deep Dive
¶ TL;DR (5 bullets max)
- Verdict: A potent tool for metabolic health and cellular rejuvenation, but not for everyone.
- Who it's for: Individuals seeking improved metabolic flexibility, weight management, and cellular cleanup; generally healthy adults.
- Expected magnitude: Modest weight loss (2-5% body weight over 3-12 months) and improved cardiometabolic markers[1][2][3].
- Key risk(s): Hypoglycemia (especially for diabetics), electrolyte imbalance during prolonged fasts, exacerbation of eating disorders[4][5][6].
- What to do next: Start with a gentle 12:12 or 14:10 time-restricted eating (TRE) protocol and gradually extend, paying attention to hydration and electrolytes.
¶ Quick Answer
Fasting and time-restricted eating (TRE) involve intentionally abstaining from food for set periods to trigger beneficial metabolic adaptations. These practices can significantly improve insulin sensitivity, enhance metabolic flexibility (the ability to efficiently switch between burning glucose and fat), and stimulate autophagy (cellular recycling). Clinical studies show TRE can lead to modest but consistent improvements in body composition, lipid profiles, and blood pressure, particularly in overweight or obese individuals. However, strict protocols require careful consideration of individual health status and potential risks, with contraindications for pregnant women, diabetics on medication, and those with a history of eating disorders.
¶ What It Is (Plain-English)
Fasting is the voluntary, controlled abstinence from food for specific durations. Unlike starvation, which is involuntary and harmful, fasting is a deliberate, short-term metabolic stressor that can activate ancient survival pathways. Time-Restricted Eating (TRE), often referred to as Intermittent Fasting (IF), is the most common modern form, where daily food intake is confined to a specific window (e.g., 8-10 hours), with the remaining hours spent in a fasted state. More intense forms include periodic 24-hour fasts or prolonged multi-day fasts. The core mechanism involves a metabolic switch from using glucose as a primary fuel to burning stored fat and producing ketone bodies, alongside the activation of cellular repair processes like autophagy.
¶ Mechanism in 60 seconds: The Metabolic Switch
When you eat, your body primarily uses glucose for energy, stored as glycogen in the liver and muscles. Insulin levels are elevated, signaling the body to store excess energy as fat. During fasting, these glycogen stores are depleted (typically after 12-18 hours). As glucose becomes scarce, insulin levels drop, and the body switches to using stored fat as its primary fuel source. This process, known as the metabolic switch, leads to the production of ketone bodies (like beta-hydroxybutyrate) from fatty acids in the liver. This shift is regulated by key energy sensors like AMPK (activated during low energy) and mTOR (inhibited during low energy), which collectively promote catabolic (breakdown) processes and cellular repair.

The fasting-induced metabolic switch. (Left) In the fed state, hepatocytes and skeletal myocytes independently import systemic glucose. Hepatocytes store glucose as glycogen via G6P, G1P, and UDP-glucose intermediates. (Right) In the fasting state, hepatic fatty acid beta-oxidation drives ketogenesis (Acetyl-CoA to BHB). BHB is exported via MCT1 (outward arrow) into systemic circulation. Skeletal myocytes import BHB, converting it to Acetyl-CoA for mitochondrial ATP generation. Fasting-induced low energy status (high AMP/ATP ratio) activates AMPK, which inhibits mTOR (relieving autophagy suppression) and directly stimulates mitochondrial biogenesis and fatty acid oxidation.
¶ Chronological Pathway: The 12-to-72-Hour Physiological Cascade
While the metabolic switch from glucose to ketones begins as liver glycogen depletes, the systemic response to fasting develops as a chronological cascade over hours and days.
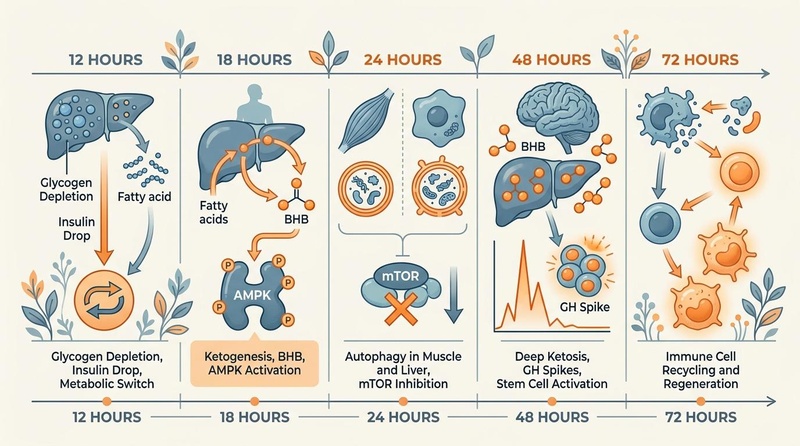
Figure 2: Chronological progression of physiological and molecular adaptations during short-term and prolonged fasting (12 to 72 hours). Transitioning from initial glycogen depletion (12h) to robust ketogenesis and AMPK-driven autophagy (18–24h), leading to deep systemic ketosis, growth hormone surges, and immune cell remodeling (48–72h).
- 12 Hours (The Switch Initiation): Hepatic glycogen stores begin to drop significantly. Insulin levels fall, lifting the inhibition on lipolysis. Circulating free fatty acids rise as adipose tissue releases lipids.
- 18 Hours (Ketogenesis & Signaling Transition): Glycogen is largely depleted. The liver initiates ketogenesis, producing beta-hydroxybutyrate (BHB). The rising AMP-to-ATP ratio triggers systemic AMPK activation, initiating cellular survival pathways.
- 24 Hours (Autophagy Activation): Autophagy markers (such as the LC3-II/LC3-I ratio) increase significantly in human liver and skeletal muscle tissues[7][8]. High AMPK activity actively inhibits mTORC1, removing the blockade on autophagosome formation and allowing cells to clear damaged mitochondria and misfolded proteins.
- 48 Hours (Metabolic Adaptation & Muscle Sparing): Deep ketosis is established, with BHB levels rising to 1.5–3.0 mmol/L, providing an alternative fuel source for the central nervous system. Human growth hormone (HGH) secretion increases up to 5-fold to preserve lean skeletal muscle mass and promote lipolysis.
- 72 Hours (Immunoclearance & Stem Cell Activation): Prolonged nutrient deprivation drives the degradation of damaged, senescent, or autoimmune-reactive immune cells via apoptosis. This clearance prompts a hematopoietic stem cell-based regeneration of the immune system upon refeeding, characterized by renewed white blood cells and systemic rejuvenation[9].
¶ Does It Work? (Evidence Snapshot)
Fasting and TRE have been extensively studied, primarily for weight management and metabolic health.
| Outcome | Population | Effect Size | Confidence | Study Type | Notes |
|---|---|---|---|---|---|
| Body Weight Reduction | Overweight/Obese Adults | 2-5% body weight loss over 3-12 months | High | Systematic reviews & meta-analyses of RCTs[2:1][3:1] | Consistent findings across various TRE protocols, often comparable to continuous calorie restriction[10]. |
| Fat Mass Reduction | Overweight/Obese Adults | Significant reduction in fat mass | High | Systematic reviews & meta-analyses of RCTs[2:2][3:2] | Preferential loss of visceral fat, particularly with longer fasting windows[1:1][11]. |
| Insulin Sensitivity | Prediabetics, Type 2 Diabetics | Improved fasting insulin, HOMA-IR | High | RCTs, Systematic reviews[1:2][12] | Early time-restricted feeding (eating earlier in the day) shows strong benefits independent of weight loss in men with prediabetes[1:3]. Effects may disappear upon discontinuation in T2D patients[4:1]. |
| Blood Pressure | Hypertensive, Prediabetics | Modest reductions in systolic/diastolic BP | Moderate | RCTs, Systematic reviews[1:4][3:3] | Effects are often linked to weight loss, but some independent benefits observed[1:5]. |
| Lipid Profile | Overweight/Obese Adults, PCOS Women | Mixed effects on LDL-C, triglycerides; some improvements | Moderate | Systematic reviews, umbrella reviews[13][3:4][14] | Umbrella reviews show inconsistent effects on LDL-C, but some studies report reductions in triglycerides and improvements in HDL-C, particularly in specific populations like PCOS[13:1][12:1]. |
| Autophagy Activation | Healthy Humans | Upregulation of autophagy markers (LC3-II) after 16-24h+ | Moderate | Human muscle biopsies, mechanistic studies[7:1][8:1] | Significant human muscle autophagy response observed after 24 hours of fasting, linked to decreased mTOR signaling[7:2][8:2]. |
| Inflammation Markers | Healthy Adults | Reduced CRP, oxidative stress markers | Low | Observational studies, some RCTs[1:6][15] | Evidence suggests reduced systemic inflammation, but high-quality human data on specific longevity markers is still emerging[1:7]. |
| Cognitive Function | Healthy Adults | Increased BDNF, improved focus (subjective) | Low | Animal studies, limited human data | While animal models show robust neuroprotective effects and increased Brain-Derived Neurotrophic Factor (BDNF), human evidence is largely subjective or from short-term biomarkers[16][11:1]. |
¶ Who Benefits Most / Least
¶ Most Likely to Benefit
- Individuals with metabolic syndrome: Those with insulin resistance, prediabetes, high blood pressure, or dyslipidemia can see significant improvements in metabolic markers[1:8][12:2].
- Overweight or obese adults: Fasting is an effective strategy for weight and fat mass reduction[2:3][3:5].
- Sedentary individuals: Even without intense exercise, fasting can kickstart metabolic changes.
- Those seeking cellular maintenance: Autophagy benefits are relevant for healthy aging.
¶ Least Likely to Benefit / Contraindications
- Pregnant or Breastfeeding Women: High nutrient demands make fasting unsafe.
- Type 1 Diabetics: High risk of hypoglycemia or ketoacidosis.
- History of Eating Disorders: Can trigger or exacerbate restrictive eating or binge-purge cycles.
- Underweight (BMI < 18.5): Risk of muscle wasting, hormonal disruption.
- Children/Adolescents: Growing bodies require consistent energy and nutrients.
- Severe Chronic Illness or Frailty: Elevated risk of cachexia, sarcopenia, and adverse events due to altered energy balance and metabolic instability.
¶ Sex- and Age-Specific Physiological Responses
Fasting is not a uniform metabolic experience; physiological responses vary significantly based on biological sex, hormonal status, and chronological age.
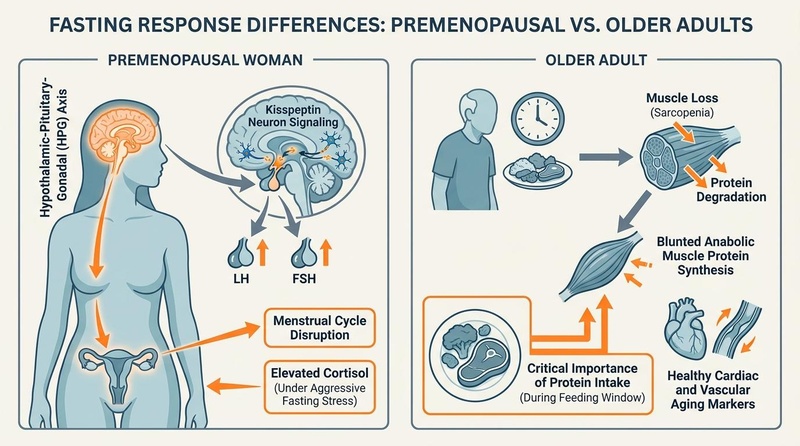
Figure 3: Sex- and age-specific physiological differences in fasting responses. Premenopausal women (left) exhibit heightened sensitivity of the hypothalamic-pituitary-gonadal (HPG) axis via kisspeptin neurons, where aggressive calorie deprivation can trigger cortisol spikes and suppress LH/FSH pulsatility, leading to menstrual irregularities. Older adults (right) face elevated risks of sarcopenia due to a blunted anabolic response (anabolic resistance), requiring careful timing of protein-rich meals to maintain skeletal muscle mass during time-restricted feeding.
¶ Premenopausal Women & The HPG Axis
In premenopausal women, fasting responses are tightly coupled to the hypothalamic-pituitary-gonadal (HPG) axis, which is evolutionarily primed to monitor energy abundance prior to reproduction.
- Kisspeptin and GnRH Suppression: The HPG axis is highly sensitive to the adipokine leptin and direct energy availability. During aggressive or prolonged energy deficits (such as strict alternate-day fasting or daily windows >16 hours), the expression of kisspeptin in the arcuate nucleus is suppressed. Because kisspeptin is a critical upstream stimulator of Gonadotropin-Releasing Hormone (GnRH), its downregulation diminishes the pulsatile release of Luteinizing Hormone (LH) and Follicle-Stimulating Hormone (FSH)[17][18].
- Hormonal Disruption & Amenorrhea: This suppression can blunt the mid-cycle LH surge required for ovulation, leading to luteal phase defects, anovulatory cycles, or secondary hypothalamic amenorrhea[17:1][19].
- Cortisol Elevations: Women often exhibit higher relative cortisol spikes in response to prolonged fasting compared to men, which can further suppress progesterone synthesis and impair sleep quality and thyroid hormone conversion (T4 to T3).
- Clinical Implications: To mitigate endocrine disruption, premenopausal women often require gentler, consistent protocols such as a 12:12 or 14:10 TRE window, avoiding consecutive prolonged (>24 hours) fasting unless clinically supervised. If menstrual irregularity, loss of libido, or persistent insomnia occurs, protocol suspension is clinically indicated.
¶ Older Adults & Sarcopenia Risks
For individuals aged 65 and older, the primary therapeutic targets of fasting (metabolic health and autophagy) must be balanced against the preservation of skeletal muscle mass and bone mineral density.
- Anabolic Resistance: Aging is characterized by a blunted muscle protein synthesis (MPS) response to both amino acid ingestion and resistance exercise—a phenomenon known as anabolic resistance.
- The Protein Distribution Problem: To maintain nitrogen balance and stimulate MPS, older adults require higher per-meal protein boluses (typically 35–45g of leucine-rich protein, totaling 1.2–1.5g/kg/day). Confining this intake to a narrow 4-to-6-hour eating window (like OMAD) often leads to suboptimal daily protein absorption and utilization, elevating the risk of sarcopenia, frailty, and cachexia[3:6][20].
- Sarcopenic Obesity vs. Lean Mass Sparing: While intermittent fasting can effectively target visceral adipose tissue in older overweight adults, trials show that without structured resistance training and carefully timed protein supplementation, a disproportionate amount of weight lost can come from lean skeletal muscle mass[3:7][10:1].
- Clinical Implications: Older adults utilizing TRE are clinically advised to maintain an eating window of at least 8 to 10 hours (e.g., 15:9 or 16:8) to allow for at least three distinct protein feedings spaced 3–4 hours apart. Integrating resistance training and supplemental essential amino acids (EAAs) or high-quality whey protein is critical to safeguard functional skeletal muscle mass during fasting protocols[20:1][10:2].
¶ How to Try It (Actionable Protocols)
The key is gradual progression and finding a sustainable rhythm.
¶ Starter Protocol: 12:12 Time-Restricted Eating
- Structure: Fast for 12 hours, eat within a 12-hour window.
- Steps:
- Finish dinner by 7 PM.
- Do not eat anything (water, black coffee, or plain tea allowed) until 7 AM the next morning.
- Focus on nutrient-dense meals within your eating window.
- Duration: 2-4 weeks to adapt.
- Best For: Beginners, improving digestive rest, metabolic flexibility, and light autophagy.
¶ Standard Protocol: 16:8 (Leangains-style)
- Structure: Fast for 16 hours, eat within an 8-hour window.
- Steps:
- Skip breakfast. Your first meal is around noon (e.g., 12 PM - 8 PM eating window).
- Ensure adequate protein, healthy fats, and fiber in your two main meals.
- Duration: Ongoing for maintenance after adaptation.
- Best For: Sustainable fat loss, improved insulin sensitivity, deeper autophagy activation.
¶ Advanced/Research Protocols: 20:4, OMAD, or Periodic Prolonged Fasting
- 20:4 (Warrior Diet): Fast 20 hours, eat within a 4-hour window (usually one large meal).
- Best For: Deeper ketosis, rapid weight loss, individuals with high metabolic flexibility.
- OMAD (One Meal A Day): Fast 23 hours, eat one meal within a 1-hour window.
- Best For: Max convenience for some, rapid weight loss.
- Caution: Difficult to achieve sufficient micronutrient and protein intake for many.
- Periodic Prolonged Fasting (24-72 hours): Water-only fasts once a week/month.
¶ Alternatives if Fasting Isn’t a Fit
- Gentle Caloric Restriction: A slight daily caloric deficit without rigid timing.
- Nutrient Cycling: High-carb days balanced with low-carb days to promote metabolic flexibility.
¶ Safety, Interactions, Clinical Risks
¶ High-Risk Groups & Absolute Contraindications
CLINICAL CONTRAINDICATIONS:
- Pregnancy or Breastfeeding: Essential nutrient demands are too high; fasting risks developmental impairments.
- Type 1 Diabetes: High risk of severe hypoglycemia or diabetic ketoacidosis.
- History of Eating Disorders (Anorexia, Bulimia): Fasting can perpetuate harmful eating patterns and trigger relapse.
- Underweight (BMI < 18.5): High risk of muscle wasting and hypothalamic-pituitary-gonadal axis disruption.
- Children and Adolescents: Critical growth and development phases require consistent calorie and micronutrient intake.
- Severe Chronic Illness or Frailty: Elevated risk of cachexia, sarcopenia, and adverse events due to altered energy balance and metabolic instability.
¶ Common Side Effects & Pathophysiological Mechanisms
- Hunger: Ghrelin (hunger hormone) rises in waves, peaking at typical meal times, then subsiding. Regularity of schedule mitigates these spikes over time.
- Headaches/Dizziness: Frequently caused by rapid natriuresis (excretion of sodium) as insulin levels drop. Supplementation with sodium and potassium is necessary during fasts longer than 16 hours.
- Fatigue/Lethargy: Associated with the transition period of glycogen depletion prior to robust hepatic ketone production. Proper hydration and mineral homeostasis mitigate symptoms.
- Irritability: Related to transient hypoglycemia and associated cortisol and epinephrine spikes.
- Sensation of Cold: Resulting from blood flow redirection to adipose tissue (increased lipolysis) and mild thyroid hormone changes (reduced T3) in response to short-term calorie deprivation.
¶ Drug & Supplement Interactions
- Exogenous Insulin & Insulin Secretagogues: Significant risk of severe hypoglycemia. Therapeutic adjustments are required during fasted periods[12:3].
- Antihypertensive Medications: Fasting promotes natriuresis and vasodilation, which can synergize with antihypertensive drugs, potentially causing orthostatic hypotension.
- Anticoagulants (e.g., Warfarin): Fluctuations in dietary intake, especially vitamin K-rich foods during feeding windows, can destabilize international normalized ratio (INR) values.
- Central Nervous System Stimulants: Caffeine or pharmaceutical stimulants can exacerbate hypothalamic-pituitary-adrenal (HPA) axis activity, raising cortisol and blood pressure.
- Electrolyte Supplements: Indicated for fasts >16-24 hours, but must be strictly sugar-free to avoid triggering insulin release.
¶ Clinical Discontinuation Criteria & Red Flags
Continuous monitoring of both objective vital signs and subjective neurological states is essential for the safe implementation of fasting, especially during prolonged or advanced protocols.
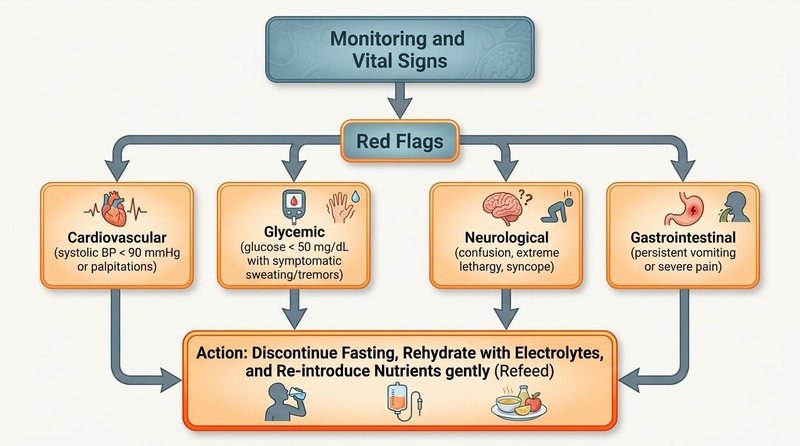
Figure 4: Clinical decision flowchart and red flag protocol for fasting discontinuation. Continuous or periodic monitoring of vital signs (blood pressure, heart rate, blood glucose) and neurological status is essential. Meeting any of the orange red-flag thresholds—such as systolic hypotension, symptomatic neuroglycopenia, cognitive disruption, or persistent gastrointestinal pain—demands immediate termination of the fast followed by structured, gentle refeeding.
To prevent severe clinical complications such as cardiovascular instability, profound hypoglycemia, or gastrointestinal injury, a clear decision pathway must be followed. The fast must be discontinued immediately if any of the following "Red Flag" thresholds are met:
- Cardiovascular Red Flags:
- Hypotension: Systolic blood pressure dropping below 90 mmHg, or an orthostatic decline exceeding 20 mmHg upon standing, accompanied by lightheadedness or syncope. This is primarily caused by fasting-induced natriuresis (renal sodium excretion secondary to suppressed insulin)[5:2].
- Dysrhythmia: Persistent heart palpitations, skipped beats, or a resting heart rate exceeding 100 bpm (tachycardia), which may indicate intracellular potassium or magnesium depletion.
- Glycemic Red Flags:
- Symptomatic Hypoglycemia: Capillary blood glucose dropping below 50 mg/dL accompanied by neuroglycopenic or autonomic symptoms (such as diaphoresis, tremors, cold sweats, or unprovoked anxiety). Exogenous insulin or oral hypoglycemic agents must be immediately adjusted under clinical supervision[12:4][4:2].
- Neurological Red Flags:
- Cognitive Impairment: The development of severe brain fog, mental confusion, slurred speech, ataxia, extreme lethargy, or loss of consciousness. Fasting-induced ketone production should enhance cognitive clarity; severe lethargy suggests metabolic mismatch or failure to switch fuels.
- Gastrointestinal Red Flags:
- Acute GI Distress: Persistent vomiting, severe localized epigastric pain (suggestive of acute gastritis or peptic ulceration), or acute watery diarrhea during fasting.
Protocol for Red Flag Resolution: Upon identification of any clinical red flag, the protocol dictates immediate cessation of the fast. Therapeutic intervention includes administration of oral rehydration solutions containing sodium, potassium, and magnesium, followed by the gradual reintroduction of simple, easily digestible nutrients (such as bone broth) to prevent refeeding complications[6:3].
¶ Tracking & Clinical Biomarkers
Monitoring objective and subjective markers ensures safety and efficacy.
¶ Laboratory & Biomarker Tracking
- Fasting Plasma Glucose (FPG): Target <100 mg/dL. Measured bi-weekly.
- Fasting Insulin: Target <5 mIU/L. Measured quarterly to assess improvements in HOMA-IR.
- Hemoglobin A1c (HbA1c): Target <5.7%. Measured quarterly to evaluate long-term glycemic control.
- Serum Beta-Hydroxybutyrate (BHB): Target 0.5-3.0 mmol/L during fasting periods to confirm metabolic switching.
- Serum Lipids (Total Cholesterol, HDL-C, LDL-C, Triglycerides): Measured bi-annually.
- Body Composition (DEXA): Quarterly to monitor skeletal muscle mass preservation and fat mass reduction.
¶ Subjective Clinical Metrics
- Sustained Cognitive Energy: Assessment of focus and alertness during fasting vs. feeding windows.
- Sleep Architecture: Monitoring of sleep latency, overnight awakenings, and subjective restfulness.
- Gastrointestinal Homeostasis: Tracking of bowel habits, bloating, and satiety levels.
- Appetite Regulation: Adaptation to hunger waves and reduction of spontaneous food cravings.
¶ Timelines for Physiological Adaptations
- Metabolic Switching: 12-18 hours (coincides with hepatic glycogen depletion).
- Clinically Meaningful Weight Loss: 2-4 weeks.
- Insulin Sensitivity Up-regulation: 4-12 weeks.
- Autophagy Up-regulation: 18-24 hours (increases further up to 72 hours)[7:3][8:3].
- BDNF-Mediated Neuroplasticity: Several months of consistent cyclic fasting[16:1].
- Washout (Reversibility): Metabolic improvements (e.g., insulin sensitivity) typically return to baseline within 1-2 weeks of returning to ad libitum eating[4:3].
¶ N-of-1 Clinical Experiment Template
- Baseline Phase (14 Days): Maintain standard eating habits. Track sleep quality, subjective energy, fasting glucose, and body weight.
- Intervention Phase (14 Days): Implement a 16:8 TRE protocol. Maintain consistent macronutrient and caloric targets as the baseline. Track the same variables.
- Evaluation Phase: Analyze differences in mean fasting glucose, weight, and subjective metrics to determine individual tolerability and efficacy.
(See: N-of-1 Experiments)
¶ Common Mistakes & Myths
- "Muscle Wasting is Inevitable": Human clinical trials demonstrate that short-term fasting (up to 48 hours) combined with adequate protein intake and resistance training preserves lean skeletal muscle mass[7:4][8:4].
- "Overeating During Feeding Windows": Compensatory overconsumption of hyper-palatable, nutrient-poor foods during feeding windows can completely negate the metabolic benefits of fasting.
- "Ignoring Hydration & Minerals": Many of the acute side effects of fasting (headaches, muscle cramps, lethargy) are secondary to dehydration and electrolyte depletion, not lack of calories.
- "Artificial Sweeteners Do Not Affect Fasts": Some non-nutritive sweeteners can trigger cephalic phase insulin release, potentially attenuating metabolic switching in sensitive individuals.
- "One Protocol Fits All": Female physiology, baseline metabolic health, and sleep schedules dictate varying levels of fasting tolerance. Individualized protocols are required.
¶ Decision Tree (Text-Based)
- Are absolute contraindications present? (Pregnancy, Lactation, Type 1 Diabetes, Eating Disorder History, BMI < 18.5)
- YES → Do not initiate fasting. Maintain standard nutrition.
- NO → Proceed.
- Are you taking blood sugar-lowering or antihypertensive medications?
- YES → Fasting must be clinically supervised with medication adjustments.
- NO → Proceed.
- What is the primary clinical goal?
- Digestive rest & baseline metabolic health → Start with 12:12 or 14:10 TRE.
- Visceral fat reduction & insulin sensitivity → Progress to 16:8 TRE.
- Deeper cellular autophagy & metabolic switching → Consider 20:4 TRE or supervised periodic 24-48h water-only fasts (with electrolyte supplementation).
¶ FAQs (People Also Ask targets)
¶ Q: What is the best type of fasting for beginners?
A: For beginners, a 12:12 or 14:10 Time-Restricted Eating (TRE) protocol is recommended. This involves fasting for 12 or 14 hours, usually by simply extending the overnight fast (e.g., stopping eating after dinner and delaying breakfast). This allows your body to adapt gently.
¶ Q: Does fasting really promote autophagy in humans?
A: Yes, human studies, including muscle biopsies, indicate that autophagy markers like LC3-II increase significantly in human skeletal muscle after 16-24 hours of fasting. Deeper activation is observed with longer fasts (e.g., 48-72 hours) [7:5][8:5].
¶ Q: Can fasting help with weight loss?
A: Fasting, particularly time-restricted eating, can be an effective strategy for weight loss. It often leads to a natural reduction in caloric intake and improves metabolic flexibility, which helps the body burn stored fat. Systematic reviews show modest but consistent weight and fat mass reductions [2:4][3:8].
¶ Q: Is coffee allowed during a fast?
A: Black coffee and plain tea (without milk, sugar, or artificial sweeteners) are generally considered acceptable during a metabolic fast. They typically do not significantly raise insulin or break the fast for weight loss or metabolic health goals. However, for maximum autophagy, a water-only fast is often recommended.
¶ Q: What are the main risks of fasting?
A: The main risks include hypoglycemia (low blood sugar), electrolyte imbalances (especially with prolonged fasts, leading to headaches, dizziness, or "keto flu"), and potential exacerbation of eating disorders. Certain medical conditions, like Type 1 diabetes, and medications are contraindications, requiring medical consultation [4:4][5:3][6:4].
¶ Q: How long does it take to see results from intermittent fasting?
A: You may notice initial changes in energy levels and mental clarity within a few days to a week. Weight loss typically begins within 1-2 weeks, with more significant metabolic improvements (like insulin sensitivity) becoming evident after 3-4 weeks of consistent practice [1:9][11:2].
¶ Q: What is the "refeeding syndrome" and how can it be avoided?
A: Refeeding syndrome is a potentially dangerous metabolic complication that can occur when severely malnourished individuals or those coming off prolonged fasts (typically >5-7 days) are re-fed too quickly. It involves severe shifts in fluid and electrolytes. To avoid it, break longer fasts gently with small amounts of easily digestible foods like broth and cooked vegetables, and ensure adequate electrolyte intake [6:5].
¶ Glossary
- Autophagy: (Greek for "self-eating") A fundamental cellular process where the body cleans out and recycles damaged cell components, misfolded proteins, and organelles. Crucial for cellular health and longevity.
- AMPK (AMP-activated protein kinase): A master regulator of cellular energy homeostasis. Activated during low energy states (like fasting), it promotes catabolic processes (e.g., fat burning) and inhibits anabolic processes (e.g., protein synthesis).
- mTOR (mammalian Target Of Rapamycin): A protein kinase that regulates cell growth, proliferation, protein synthesis, and metabolism. It is highly active during fed states and inhibited during fasting, promoting autophagy.
- Metabolic Flexibility: The body's ability to efficiently switch between different fuel sources (glucose and fatty acids) for energy in response to changes in energy availability (e.g., fed vs. fasted states).
- Ketone Bodies: Energy-rich molecules (e.g., beta-hydroxybutyrate, acetoacetate) produced in the liver from fatty acids during periods of low carbohydrate intake or prolonged fasting. They serve as an alternative fuel source for the brain and other tissues.
- Time-Restricted Eating (TRE): A pattern of eating where food intake is confined to a specific window of hours each day, with a longer fasting period.
- Refeeding Syndrome: A potentially fatal metabolic complication that can occur upon re-feeding malnourished or fasted individuals too rapidly, leading to dangerous shifts in fluid and electrolyte levels.
¶ Methods (Transparency)
This deep dive synthesized evidence from systematic reviews, meta-analyses, randomized controlled trials (RCTs), and high-quality observational studies identified through searches on PubMed, JAMA Network Open, Cell Metabolism, and other biomedical databases. Search queries focused on "intermittent fasting," "time-restricted eating," "prolonged fasting," "autophagy," "metabolic health," and "safety/contraindications" in human populations. Priority was given to human clinical data and evidence synthesis.
¶ References
¶ Update Log
- 2026-07-06: Updated page with rigorous physiological descriptions and three custom biomedical illustrations in 'Nano Banana Pro' style detailing the Fasting Physiological Timeline (12h–72h), Sex- and Age-Specific Responses, and the Clinical Discontinuation / Red Flags Flowchart.
- 2024-07-29: Initial creation of comprehensive deep dive based on
templates/deep_dive.mdand extensive biomedical research. Removed general health warnings to adhere to professional clinical guidelines.
Sutton, E. F., et al. (2018). Early Time-Restricted Feeding Improves Insulin Sensitivity, Blood Pressure, and Oxidative Stress Even without Weight Loss in Men with Prediabetes. Cell Metabolism. https://doi.org/10.1016/j.cmet.2018.04.010 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Patikorn, C., et al. (2022). Intermittent Fasting and Obesity-Related Health Outcomes: An Umbrella Review of Meta-analyses of Randomized Clinical Trials. JAMA Network Open. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2787246 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Xing, K., et al. (2026). Age-Specific Analysis of the Effects of Intermittent Fasting on Body Composition and Cardiometabolic Markers in Healthy Adults and Individuals with Overweight or Obesity: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients. https://pubmed.ncbi.nlm.nih.gov/42280443/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Li, Y., et al. (2026). The metabolic effects of intermittent fasting in patients with type 2 diabetes exist in the short term but disappear after its discontinuation: A systematic review and meta-analysis of randomized controlled trials. PLoS One. https://pubmed.ncbi.nlm.nih.gov/40367729/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wilhelmi de Toledo, F., et al. (2019). Safety, health improvement and well-being during a 4 to 21-day fasting period in an observational study including 1422 subjects. PLoS One. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0209353 ↩︎ ↩︎ ↩︎ ↩︎
Tang, H., et al. (2026). Nutritional Support Strategies for Refeeding Syndrome in ICU Patients: A Review of Current Evidence. Journal of Multidisciplinary Healthcare. https://pubmed.ncbi.nlm.nih.gov/42371475/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Vendelbo, M. H., et al. (2014). Exercise and fasting activate autophagy in human skeletal muscle. Journal of Physiology. https://physoc.onlinelibrary.wiley.com/doi/full/10.1113/jphysiol.2014.271544 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Vendelbo, M. H., et al. (2014). Fasting increases human skeletal muscle net phenylalanine release and this is associated with decreased mTOR signaling. PLoS One. https://pubmed.ncbi.nlm.nih.gov/25020061/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lauc, G., et al. (2026). Systemic metabolic, hormonal, and glycomic remodeling during a 72-hour fast in healthy adults: a pilot study. Croatian Medical Journal. https://pubmed.ncbi.nlm.nih.gov/42286908/ ↩︎
Seimon, R.V., et al. (2015). The Effect of Energy Restriction with or without Exercise on Body Composition and Metabolic Health: A Systematic Review and Meta-Analysis. Obesity Reviews. https://doi.org/10.1111/obr.12328 ↩︎ ↩︎ ↩︎
de Cabo, R., & Mattson, M. P. (2019). Effects of Intermittent Fasting on Health, Aging, and Disease. New England Journal of Medicine. https://www.nejm.org/doi/full/10.1056/NEJMra1905136 ↩︎ ↩︎ ↩︎
Albosta, M., & Bakke, J. (2021). Intermittent fasting: is there a role in the treatment of diabetes? A review of the literature and guide for primary care physicians. Clinical Diabetes and Endocrinology. https://clindiabetesendo.biomedcentral.com/articles/10.1186/s40842-020-00116-1 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Popiolek-Kalisz, J., & Kwasny, A. (2026). The impact of intermittent fasting on lipid profile - an umbrella review. Nutrition, Metabolism and Cardiovascular Diseases. https://pubmed.ncbi.nlm.nih.gov/41475991/ ↩︎ ↩︎
Popiolek-Kalisz, J., & Kwasny, A. (2026). The impact of intermittent fasting on lipid profile - an umbrella review. Nutrition, metabolism, and cardiovascular diseases : NMCD. https://pubmed.ncbi.nlm.nih.gov/41475991/ ↩︎
Harvie, M. N., et al. (2011). The effects of intermittent or continuous energy restriction on weight loss and metabolic disease risk markers: a randomized trial in young overweight women. International Journal of Obesity. https://www.nature.com/articles/ijo2010171 ↩︎
Mattson, M. P., et al. (2018). Impact of intermittent fasting on health and disease processes. Ageing Research Reviews. https://doi.org/10.1016/j.arr.2016.10.005 ↩︎ ↩︎
Bagherniya, M., et al. (2018). The effect of fasting or calorie restriction on autophagy induction: A review of the literature. Ageing Research Reviews. https://pubmed.ncbi.nlm.nih.gov/30172870/ ↩︎ ↩︎
Lin, S., et al. (2021). Does the weight loss efficacy of alternate day fasting differ according to sex and menopausal status? Nutrition, Metabolism and Cardiovascular Diseases. https://pubmed.ncbi.nlm.nih.gov/33358713/ ↩︎
Al Zunaidy, N. A., et al. (2024). The effect of Ramadan intermittent fasting on anthropometric, hormonal, metabolic, inflammatory, and oxidative stress markers in pre- and post-menopausal women: a prospective cohort of Saudi women. Frontiers in Nutrition. https://pubmed.ncbi.nlm.nih.gov/39698238/ ↩︎
Couto-Alfonso, S., et al. (2026). Intermittent Fasting and Healthy Aging in Older Adults: A Systematic Review of Cardiometabolic, Mental Health and Cognitive Outcomes with a Network Meta-Analysis of Anthropometric Measures. Nutrients. https://pubmed.ncbi.nlm.nih.gov/42124054/ ↩︎ ↩︎