¶ Periodontal Disease Prevention and Treatment: An Evidence-Based Clinical Guide
Periodontal disease is a chronic immunoinflammatory condition of the supporting structures of the teeth—including the gingiva, periodontal ligament, and alveolar bone—driven by a dysbiotic subgingival oral biofilm. Resolving periodontal inflammation is a primary clinical priority for healthspan extension: local tissue destruction acts as a persistent source of systemic bacteremia and pro-inflammatory cytokines, accelerating vascular endothelial aging, driving chronic inflammation, impairing metabolic control, and increasing cardiovascular morbidity. Modern periodontal medicine mandates a highly structured, stepwise therapeutic framework to transition patients from localized dysbiosis to long-term clinical stability.
| Classification | Stage I–IV (Severity), Grade A–C (Progression) |
| Primary Therapy | Mechanical debridement (SRP) & biofilm disruption |
| Primary Adjuncts | Chlorhexidine, local antimicrobials, systemic antibiotics |
| Primary Biomarker | Bleeding on probing (BOP) & Probing pocket depth (PPD) |
| Systemic Target | hs-CRP, Glycemic control (HbA1c), Endothelial function |
| Evidence Quality | High (EFP S3 Clinical Guidelines, Consensus) |
¶ TL;DR
- What it is: A chronic inflammatory disease of the supporting periodontal structures, managed via highly structured mechanical plaque control and sequential professional debridement [1].
- Main Benefits: Promotes subgingival biofilm control [1:1], significantly lowers systemic inflammatory markers (hs-CRP), and improves glycemic control in Type 2 Diabetes [2].
- Key Considerations: Efficacy relies on patient compliance with specialized mechanical oral hygiene and clinician adherence to the EFP S3-level stepwise guidelines [1:2] [3].
- Safety & Risks: Highly safe, but debridement requires clinical awareness of patient bleeding profiles. For general clinical parameters, routine adjunctive use of systemic antibiotics is not recommended under clinical guidelines [1:3], while in diabetic populations, adding antimicrobials to mechanical debridement shows no additional glycemic control benefit [4].
- Evidence Base: Supported by high-certainty guidelines, randomized controlled trials, and meta-analyses demonstrating successful clinical endpoints and systemic biomarker reductions [1:4] [5] [2:1].
¶ Quick Answer
Periodontal therapy aims to disrupt the dysbiotic subgingival biofilm, halt tissue destruction, and resolve systemic inflammatory spillover. Successful management requires a strict, sequential clinical escalation: transitioning from patient-mediated plaque control and risk factor modification (Step 1) to professional subgingival scaling and root planing (SRP) (Step 2), followed by surgical intervention for non-resolving deep pockets (Step 3), and lifetime supportive maintenance (Step 4) [1:5]. While biological plausibility and epidemiological studies support an association between periodontitis and systemic conditions like cardiovascular disease (CVD) and cognitive decline, further rigorous clinical studies are needed to confirm the therapeutic potential and establish causal prevention or reversal of these conditions [6] [7]. However, active treatment is clinically proven to lower localized infection, resolve systemic chronic inflammation (hs-CRP), and significantly improve glycemic control (HbA1c) in patients with type 2 diabetes [2:2].
¶ Identify the Type / Candidate Fit
Patient staging, grading, and systemic risk profiling are foundational to tailoring periodontal therapy. Under the EFP/AAP classification framework, staging and grading are designed to link disease classification directly with approaches to prevention, clinical complexity, and treatment [1:6].
¶ Periodontal Staging (Severity and Complexity of Management)
Periodontal staging classifies the disease based on the severity of disease at presentation as well as on the complexity of disease management [8]. This framework is applied to characterize periodontitis, which now groups forms of the disease previously recognized as "chronic" or "aggressive" under a single category [8:1].
¶ Periodontal Grading (Rate of Progression and Risk Assessment)
Periodontal grading provides supplemental information about the biological features of the disease [8:2]:
- Progression Rate: Includes a history-based analysis of the rate of periodontitis progression [8:3].
- Risk Assessment: Assesses the risk for further progression [8:4].
- Treatment Outcomes: Analyzes possible poor outcomes of treatment [8:5].
- Systemic Impact: Evaluates the risk that the disease or its treatment may negatively affect the general health of the patient [8:6].
¶ Systemic Risk Factor Profiling
- Smoking: Active smoking is a significant risk indicator for the development of peri-implant diseases, including both peri-implant mucositis and peri-implantitis [9] [10].
- Vaping / Electronic Cigarettes: Aerosolized nicotine and chemical flavorings induce local oxidative stress and local microvascular changes, mimicking the harmful effects of combustible tobacco on the periodontal tissues.
- Diabetes Mellitus: A profound, bidirectional relationship exists between glycemic control and periodontitis [2:3] [11]. Professional subgingival instrumentation (SRP) is clinically proven to improve glycemic control in people with both periodontitis and diabetes by a clinically significant amount, reducing HbA1c [11:1] and lowering systemic C-reactive protein (CRP) [2:4]. Under the 2017 classification framework, grading provides supplemental information that includes assessing the risk that the periodontal disease or its treatment may negatively affect the general health of the patient [8:7].
- Genetics: Specific genetic susceptibility profiles can hyper-sensitize the host's immunoinflammatory response, leading to aggressive tissue destruction even under low-plaque conditions.
- Age: Epidemiological data demonstrates that mean clinical attachment loss (CAL) increases linearly with age, with gingival recession contributing increasingly to attachment loss with age, particularly after 45 to 49 years, while mean probing depth remains relatively constant across different age groups [12].
¶ Evidence Snapshot
¶ Evidence Summary Table (Human Outcomes)
The clinical utility of preventative and therapeutic interventions for periodontal disease is documented by extensive, high-quality human evidence, synthesized below using the GRADE framework.
| Intervention | Outcome Measured | Effect Size / Direction | Evidence Quality | Consistency | Supporting Evidence | Clinical Notes |
|---|---|---|---|---|---|---|
| Oscillating-Rotating Powered Brushing | Plaque & Gingival Index Reduction | Moderate | High | Matthews et al. [13], Wilder et al. [14] | While short-term studies suggest powered brushes may reduce plaque, long-term clinical trials show manual brushing with correct technique is similarly effective [13:1] [14:1]. | |
| Interdental Brushes (IDBs) | Interproximal Plaque & Inflammation | Moderate | High | EFP S3 Guidelines [1:7], Ng & Lim [15], Cochrane Database [16] | Recommended as first-line interdental cleaning aids [1:8]; especially indicated in patients with widened embrasures [15:1], where they are at least as good if not superior to floss in reducing plaque and gingivitis [15:2]. | |
| Non-Surgical Periodontal Therapy (SRP) | PPD Reduction & CAL Gain | High | High | Sanz et al. [1:9] | Standard of care for pockets with deep pocket depths and inflammation; achieves significant pocket depth reduction and attachment level gain [1:10]. | |
| Guideline-Based Periodontal Therapy (Steps I-III) | Achievement of Endpoints of Therapy (EoT) | High | High | Aimetti et al. [5:1] | Achieves Endpoints of Therapy (EoT—no deep pockets with bleeding on probing) in 93.3% of treated sites [5:2]. | |
| SRP in Type 2 Diabetics | HbA1c & Systemic CRP Reduction | Moderate to High | High | Cochrane Database [11:2], Baeza et al. [2:5] | Yields a mean absolute reduction of 0.43% [11:3] to 0.56% [2:6] in HbA1c, and 1.89 mg/L in CRP [2:7] at 3–4 months. | |
| Supportive Periodontal Therapy (SPT) | Attachment Level Stability & Tooth Retention | High | High | S3 Guidelines [1:11], Fischer et al. [3:1] | Lifetime professional care personalized by risk-profile; essential to prevent disease recurrence [1:12] [3:2]. | |
| Adjunctive Systemic Antibiotics | Clinical Pocket Closure & Attachment Gain | Low to Moderate | High | EFP S3 Guidelines [1:13] | Recommended against for routine Stage I–III cases; mechanical debridement remains the cornerstone of therapy [1:14]. | |
| Adjunctive Chlorhexidine Rinses | Plaque & Gingival Inflammation Control | Moderate | High | Brookes et al. [17] | Short-term adjunctive use reduces plaque and clinical symptoms of gingivitis, though long-term benefit for periodontitis remains uncertain [17:1]. | |
| Locally Delivered Antimicrobials (LDAs) | Professional Utilization & Knowledge | Moderate | Moderate | Ahmed & Alasmari [18] | Survey shows LDAs are viewed as essential but are clinically underutilized, with gaps in provider knowledge regarding current guidelines [18:1]. | |
| Dietary/Caloric Restriction (CR) | Periodontal Indices & Inflammation | Low | Low | Mainas et al. [19] | Emerging pre-clinical and pilot clinical evidence showing reduction in local hyper-inflammation [19:1]. | |
| Supportive Peri-Implant Care (SPC) | Prevention of Peri-Implant Disease | Moderate | High | Herrera et al. [20], Galarraga-Vinueza et al. [9:1] | Custom maintenance commencing from implant planning and loading; maintains healthy peri-implant tissues [20:1] [9:2]. |
- Effect direction: u = up (increase), d = down (decrease), e = equal (no effect), q = unclear. Magnitude: 1 (small), 2 (moderate), e = equal (no effect). Impact: p = positive for health, n = negative for health, x = neutral/unknown.
¶ How it works (Mechanism) & Systemic Aging
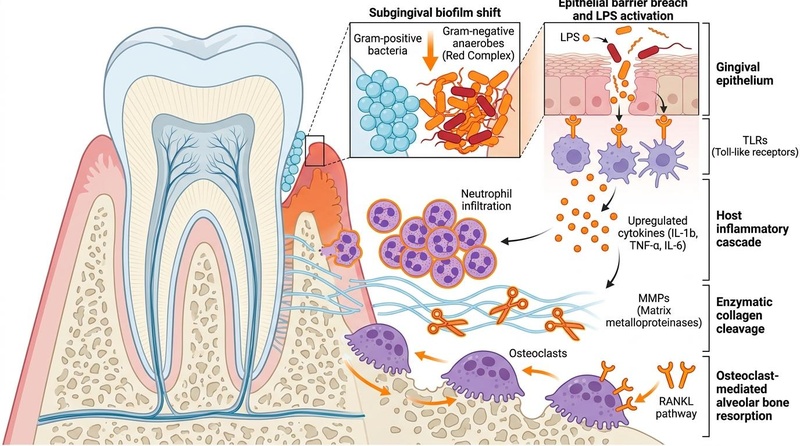
The progression of periodontal disease represents an ecological shift in the subgingival microenvironment, where a symbiotic host-microbe relationship degrades into destructive, host-mediated tissue damage [1:15] [21].
 with an intact gingival margin, shallow sulcus, and healthy alveolar bone compared to the progression of disease (right) showing subgingival calculus, dysbiotic plaque biofilm, active osteoclasts resorbing bone, and upregulation of collagen-degrading Matrix Metalloproteinases (MMPs).")
¶ The Microbiome Shift and Dysbiosis
In periodontal health, the subgingival space is dominated by Gram-positive, facultative anaerobic or aerobic bacteria (primarily Streptococcus and Actinomyces species). When plaque removal is neglected, early colonizers utilize local oxygen and secrete metabolic byproducts, transforming the pocket into a highly anaerobic, nutrient-rich niche. This selects for late-colonizing, obligate anaerobic, Gram-negative species, classically termed the "Red Complex" [21:1]:
- Porphyromonas gingivalis: An obligate anaerobic pathogen associated with chronic periodontitis and systemic inflammatory translocation [7:1]. Scoping reviews suggest that P. gingivalis infection can trigger neuroinflammation, amyloid-β (Aβ) and tau protein aggregation, and gut-brain axis dysregulation [7:2].
- Treponema denticola & Tannerella forsythia: Classified as key disease-associated anaerobic bacterial species that, alongside P. gingivalis, are evaluated in subgingival plaque samples to assess microbiological shifts following periodontal therapy [21:2].
¶ Host-Mediated Immunoinflammatory Cascade and Bone Resorption
Local tissue destruction in periodontitis is not caused directly by bacteria, but by an overactive, dysfunctional host immune response to the dysbiotic biofilm.
- Pattern Recognition: Bacterial lipopolysaccharides (LPS) and other pathogen-associated molecular patterns (PAMPs) bind to Toll-like receptors (TLR2 and TLR4) on gingival epithelial cells, dendritic cells, and macrophages.
- Cytokine Upregulation: Binding activates the nuclear factor-kappa B (NF-B) pathway, prompting the heavy transcription and release of pro-inflammatory cytokines: IL-1, TNF-, and IL-6.
- Neutrophil Hyperactivation: These cytokines recruit polymorphonuclear leukocytes (PMNs/neutrophils) into the periodontal pocket. While essential to contain bacteremic spread, persistent PMN hyperactivation leads to degranulation, releasing reactive oxygen species (ROS) and elastase that cause collateral damage to the healthy connective tissue.
- Enzymatic Collagen Cleavage: Activated local fibroblasts and PMNs upregulate host Matrix Metalloproteinases (MMPs), particularly MMP-8 (collagenase-2) and MMP-9 (gelatinase-B). These enzymes enzymatically cleave the type I collagen fibers forming the periodontal ligament and gingival connective tissue attachment.
- Osteoclast-Mediated Alveolar Bone Resorption: Pro-inflammatory cytokines and lipopolysaccharides upregulate the expression of Receptor Activator of Nuclear Factor kappa-B Ligand (RANKL) on osteoblast-lineage cells and activated T- and B-lymphocytes, while concurrently downregulating Osteoprotegerin (OPG), a decoy receptor that normally binds and neutralizes RANKL. The resulting high RANKL:OPG ratio allows RANKL to bind to its receptor (RANK) on osteoclast precursor cells, stimulating their differentiation and survival into mature, multinucleated osteoclasts. These osteoclasts resorb the alveolar bone housing the tooth roots, eventually leading to tooth mobility and tooth loss.
¶ Connections to Systemic Aging and Inflammaging
Severe periodontitis represents a persistent, low-grade inflammatory wound. This ulcerated pocket epithelium permits the translocation of bacteria, LPS, and local pro-inflammatory mediators into the systemic circulation, driving systemic inflammatory processes [1:16] [2:8].
- Cardiovascular Disease (CVD): Systematic reviews and meta-analyses support an association between periodontal disease, tooth loss, and cardiovascular diseases, with reported odds ratios ranging from 1.22 to 4.42 and risk ratios from 1.14 to 2.88 [6:1].
- Type 2 Diabetes: Direct cytokine leakage impairs hepatic and skeletal muscle insulin receptor signaling, exacerbating insulin resistance. Non-surgical periodontal therapy (SRP) reverses this, lowering HbA1c by a mean of 0.43% [11:4] to 0.56% [2:9] at 3–4 months post-treatment.
- Alzheimer's Disease: Research suggests an association between periodontal pathogens—such as P. gingivalis and F. nucleatum—and Alzheimer's disease or cognitive decline. Baseline periodontal disease has been associated with a significant increase in the rate of cognitive decline over a 6-month period [22].
- Pregnancy and Adverse Outcomes: Epidemiology shows that maternal periodontitis is significantly associated with an increased risk of pre-eclampsia (with reported odds ratios of 3.18) [23], as well as preterm birth and low birth weight [24] [25]. Although periodontal treatment is proven to be safe and effective at improving maternal periodontal health during pregnancy [26] [24:1] [25:1], systematic reviews and consensus guidelines demonstrate that active periodontal therapy (with or without adjunctive systemic antibiotics) does not significantly reduce overall rates of preterm birth or low birth weight [27] [24:2] [25:2].
¶ CRITICAL DISTINCTION: Association vs. Causation
Clinicians must clearly understand that while there is strong biological plausibility and epidemiological evidence linking periodontitis to systemic diseases, systematic reviews show that clinical trials on periodontal treatment have not demonstrated a statistically significant reduction in adverse pregnancy outcomes such as preterm birth [27:1] [26:1], and further high-quality, rigorous research is required to establish whether treating periodontal disease can causally prevent or modify cardiovascular disease [6:2] or Alzheimer's pathology [7:3]. Treating periodontitis is clinically indicated to resolve localized infection, improve local tissues, improve glycemic control (HbA1c) in diabetes [2:10], and reduce systemic chronic inflammation (hs-CRP) [2:11], but claims of direct causal prevention of dementia or myocardial infarction are currently unsupported by interventional trial data.
¶ Clinical and Self-Care Protocols
Management of periodontal disease follows a strict, sequential clinical framework based on the European Federation of Periodontology (EFP) S3-level guidelines [1:17] [3:3]. The EFP represents over 18,000 global professionals and drives evidence-based guidelines and workshops to standardize periodontal care and promote public awareness of oral-systemic links [28]. Furthermore, specialist training programs in periodontology and implant dentistry emphasize the practical application of this classification and CPGs to ensure diagnostic accuracy and optimal treatment delivery [29], although general dentists and dental students can show suboptimal diagnostic accuracy and confidence in applying the 2017 EFP/AAP classification [30].
¶ At-Home Mechanical Biofilm Control
Daily, patient-mediated mechanical biofilm disruption is the foundation of both prevention and treatment [1:18] [3:4].
- Brushing Technique (Modified Bass Technique): Instruct patients to hold the toothbrush head at a 45-degree angle to the long axis of the teeth, directing the bristles slightly into the gingival sulcus (gumline). Apply light, vibrating circular strokes for 10 to 15 seconds per tooth group to physically disrupt subgingival plaque, followed by a sweeping stroke occlussally (away from the gums). Brush for a minimum of 2 minutes twice daily.
- Electric vs. Manual Toothbrushes: While powered toothbrushes show evidence of efficacy for biofilm removal and can increase patient compliance in the short term, evidence for superior long-term clinical or microbiological effects over manual toothbrushes remains limited [13:2] [14:2]. Systematic reviews and trials show that manual toothbrushes, when utilized with proper technique (such as the Modified Bass Technique) and standard fluoride toothpaste, are highly effective for periodontal maintenance [13:3] [14:3].
- Reminating Dentifrices: Recommend toothpastes containing at least 1450 ppm fluoride (such as sodium fluoride or sodium monofluorophosphate) for caries prevention and biofilm control. For patients with exposed root surfaces and dental hypersensitivity, toothpastes formulated with nano-hydroxyapatite (n-HAp) are highly effective at occluding exposed dentinal tubules and promoting cervical enamel remineralization.
- Interdental Hygiene: Daily plaque removal in the interdental region is critical to periodontal health [16:1]. Interdental brushes are especially indicated in periodontal patients where widened embrasures are common, offering ease of use and superior plaque and gingivitis reduction compared to dental floss [15:3]. Traditional dental floss is highly technique-sensitive and may not confer significant benefits over brushing alone when used inactively [15:4].
¶ Lifestyle Modifications and Smoking Cessation
Systemic risk factors must be actively modified to enable tissue healing [1:19] [3:5] [2:12].
- Smoking Cessation: Active smoking is a major risk indicator for peri-implant diseases, including peri-implant mucositis and peri-implantitis [9:3] [10:1]. Promoting smoking cessation is an integral part of risk factor control within comprehensive periodontal clinical management [1:20] [3:6]. Quitting smoking restores host response capacity and supports clinical healing.
- Dietary Interventions: Emphasize a low-glycemic, anti-inflammatory diet. High intake of refined carbohydrates promotes systemic oxidative stress and selects for an acidogenic, dysbiotic oral microflora. Systematic reviews indicate that dietary approaches, specifically caloric restriction (CR), have the potential to reduce local and systemic hyper-inflammatory states and improve periodontal clinical indices [19:2].
¶ Professional Non-Surgical Periodontal Therapy (NSPT)
Professional debridement (Step 2 of the S3 framework) must be performed when subgingival plaque and calculus are present [1:21].
- Indications: Non-surgical periodontal therapy (SRP) is indicated for sites with deep pocket depths and clinical signs of inflammation, such as bleeding on probing [1:22].
- Procedural Steps: Performed under local anesthesia, NSPT consists of thorough subgingival scaling and root planing (SRP) using ultrasonic scalers (for bulk debridement and calculus removal) and hand curettes (such as Gracey curettes for precise root planing and debridement of root concavities).
- Clinical Endpoints of NSPT: Re-evaluate periodontal status at an appropriate post-treatment interval to assess healing [1:23]. The primary clinical endpoints for successful non-surgical periodontal therapy are:
- Pocket Closure: Achieving shallow probing pocket depths with no bleeding on probing (pocket closure), representing a key endpoint of therapy [1:24] [5:3].
- Resolution of Inflammation: Significant reduction in clinical signs of inflammation, such as erythema, suppuration, and bleeding [1:25] [5:4].
- Low Systemic Bleeding: An overall systemic bleeding on probing (BOP) score of of total probed sites.
- Supportive Periodontal Therapy (SPT) Intervals: Long-term clinical maintenance (supportive periodontal care) is mandatory to prevent disease relapse and maintain treatment benefits over time [1:26] [3:7]. Rather than prescribing fixed timelines, clinical guidelines emphasize that recall intervals must be personalized based on the patient's individual risk profile to determine the appropriate frequency of supportive care [1:27] [3:8].
¶ Adjunctive Chemotherapeutic and Antimicrobial Agents
Antimicrobials must only be used as adjuncts to, and never as a replacement for, mechanical biofilm disruption [1:28] [17:2].
- Chlorhexidine (CHX) Mouthrinses: Evidence from clinical reviews supports the short-term adjunctive use of chlorhexidine mouthwash to manage dental plaque and reduce clinical symptoms of gingivitis [17:3]. However, its use must be carefully weighed against side effects (extrinsic teeth staining, potential development of antimicrobial resistance, and rare but severe allergic reactions) [17:4]. Furthermore, evidence supporting chlorhexidine's effectiveness to manage or prevent chronic periodontitis, necrotising periodontal diseases, or peri-implantitis remains less certain [17:5].
- Locally Delivered Antimicrobials (LDAs): Locally delivered antimicrobials (such as chlorhexidine gluconate or tetracycline) are regarded by dental professionals as an important adjunct in periodontal therapy [18:2]. However, cross-sectional survey data indicates that they are frequently underutilized in clinical practice, with half of surveyed dental professionals reporting no history of utilizing LDAs and less than half demonstrating comprehensive knowledge of their pharmacological activities or current clinical practice guidelines [18:3].
- Systemic Antibiotics: Under the EFP S3 clinical practice guidelines, the routine use of adjunctive systemic antibiotics is not recommended for Stage I–III periodontitis, as mechanical debridement (SRP) remains the cornerstone of therapy [1:29]. Furthermore, for patients with both periodontitis and diabetes, a Cochrane systematic review found no consistent evidence that adding systemic or local antimicrobials to SRP provides any additional glycemic control (HbA1c) benefit over SRP alone [4:1].
¶ Surgical Escalation & Specialist Referral
For sites that do not respond to NSPT, surgical intervention (Step 3 of the S3 framework) is indicated [1:30] [5:5].
¶ Referral Thresholds
Re-evaluate the patient at an appropriate post-treatment interval after completion of Step 2 (NSPT) [1:31]. If there are persistent, non-resolving deep pockets with bleeding on probing, the patient must be escalated to Step 3 (Surgical Periodontal Therapy) or referred directly to a specialist [1:32] [5:6].
¶ Surgical Modalities
- Access Flap Surgery: Reflection of a mucoperiosteal flap to allow direct visual access to the root surfaces for thorough debridement of deep, complex pockets and furcation involvements [1:33] [5:7] [21:3].
- Resective Surgery: Apically positioned flaps with or without osseous recontouring to eliminate the pocket wall entirely, facilitating easier long-term cleaning but potentially causing tooth lengthening and root sensitivity [1:34].
- Guided Tissue Regeneration (GTR) & Bone Grafting: Utilizes bone replacement grafts (allografts, xenografts, or synthetic materials) combined with barrier membranes (resorbable or non-resorbable) to prevent epithelial downgrowth, allowing periodontal ligament and bone cells to repopulate the defect and reconstruct the lost periodontal attachment [1:35] [5:8]. Enamel matrix derivatives (EMD / Emdogain) can be applied to the root surface to biologically stimulate cementum, periodontal ligament, and alveolar bone regeneration [1:36]. Guideline-based periodontal therapy (comprising Steps I, II, and III, which includes both NSPT and repeated debridement or surgical therapy) achieves the Endpoints of Therapy (EoT—defined as no deep pockets with bleeding on probing) in up to 93.3% of treated sites in severe Stage III-IV cases [5:9].
- Impact of Periodontal Surgery on the Microbiome: Systematic reviews of periodontal surgery demonstrate that its effect on the subgingival microbiome is highly heterogeneous and does not always result in a consistent decrease of disease-associated bacterial species, highlighting that clinical pocket closure and attachment gain can occur without uniform microbiological clearance [21:4].
¶ Implant Considerations
As dental implants have become widespread, managing the tissues surrounding implants has emerged as a major clinical priority [20:2].
¶ Peri-Implant Mucositis vs. Peri-Implantitis
- Peri-Implant Mucositis: A reversible, plaque-induced inflammatory lesion confined strictly to the soft tissues surrounding a functional dental implant, with no evidence of bone loss [20:3]. It is the biological analogue of gingivitis.
- Peri-Implantitis: A plaque-induced, chronic inflammatory lesion in the tissues surrounding an implant, characterized by bleeding on probing, suppuration, increased probing depths, and progressive, irreversible loss of supporting alveolar bone [20:4]. Managing peri-implantitis is highly complex and carries significant patient morbidity [20:5].
¶ Risk Factors for Peri-Implant Disease
A prior history of periodontitis is a major and established risk factor for developing peri-implant diseases (including both peri-implant mucositis and peri-implantitis) [20:6] [9:4] [10:2]. Other risk indicators identified in systematic reviews include poor oral hygiene (high plaque scores), smoking, alcohol consumption, and diabetes mellitus [9:5] [10:3].
¶ Professional Implant Maintenance and Cleaning
Professional implant maintenance must focus on early prevention and supportive care, commencing from implant planning, surgical placement, and prosthetic loading, including structured periodic clinical assessments of peri-implant tissue health [20:7]. For daily mechanical plaque removal, interdental brushes and oral irrigators are clinically preferred over dental floss [15:5].
¶ Long-Term Supportive Peri-Implant Care
High-quality clinical consensus mandates structured, personalized supportive peri-implant care (SPC) to maintain healthy peri-implant tissues and prevent the development or recurrence of peri-implant diseases [20:8]. Supportive care programs should be tailored to the patient's risk profile, including periodic clinical and radiographic evaluation [20:9].
¶ Tracking Plan
To monitor the success of periodontal interventions, both clinicians and patients should track key quantitative parameters:
- Plaque Control Record (O'Leary Index): The percentage of plaque-free tooth surfaces. The clinical target is plaque-stained surfaces.
- Bleeding on Probing (BOP) Score: The percentage of probed sites that exhibit bleeding within 30 seconds of probing. The clinical target is of total sites.
- Probing Pocket Depth (PPD) and Attachment Level (CAL): Quantitative pocket measurements. The clinical target is pocket closure (all sites mm with no bleeding on probing, or absolute reduction).
- Glycemic Control (HbA1c): For diabetic patients, absolute improvements in metabolic control are monitored post-treatment. Periodontal debridement (SRP) has been shown to reduce HbA1c by a mean of 0.43% [11:5] to 0.56% [2:13] at 3–4 months post-treatment, supporting overall diabetes management.
- Systemic Inflammation (hs-CRP): For general cardiovascular risk tracking, periodontal debridement has been shown to reduce systemic C-reactive protein by a mean of 1.89 mg/L in patients with type-2 diabetes [2:14].
¶ Safety, Red Flags & Urgent Referrals
Periodontal therapy is highly safe, but specific systemic conditions and acute presentations require immediate clinical management.
¶ Absolute and Relative Contraindications
- Do not perform aggressive mechanical subgingival debridement (SRP) in patients with active, uncontrolled bleeding disorders, severe thrombocytopenia, or those on therapeutic-dose anticoagulation without pre-operative medical clearance and hematological stabilization.
- Do not utilize systemic adjunctive antibiotics for mild chronic periodontitis, gingivitis, or as a routine, universal supplement [1:37].
- Immediate replantation of avulsed teeth is contraindicated in patients with advanced periodontal disease, extensive untreated caries, advanced age, immunodeficiency, or lack of cooperation [31].
¶ Urgent Referrals and Red Flags
- Acute Periodontal Abscess: Characterized by localized, rapid-onset, throbbing pain, fluctuant swelling of the gingiva, tooth mobility, and localized bone destruction. Requires immediate clinical drainage, mechanical debridement, and potential antibiotic therapy to prevent systemic spread.
- Necrotizing Ulcerative Gingivitis / Periodontitis (NUG/NUP): Rapidly progressive, destructive inflammatory lesions of the periodontium, characterized by the typical clinical phenotype of interdental papilla necrosis (punched-out papillae), gingival bleeding, and severe pain, associated with host immune response impairments [8:8]. Urgent professional mechanical debridement and appropriate systemic or local supportive therapy are required.
- Spreading Facial Cellulitis: A medical emergency where oral infections breach anatomical fascial planes.
- Key Features: Rapid, painful swelling of the neck, jaw, or submandibular space (Ludwig's Angina), difficulty breathing (dyspnea) or swallowing (dysphagia), high fever, trismus (limited jaw opening). Requires immediate referral to an emergency department or oral-maxillofacial surgeon for airway management, surgical drainage, and high-dose intravenous antibiotic therapy.
¶ FAQs
¶ Can NSPT completely cure periodontitis?
No. Periodontitis is a chronic disease; while active therapy can successfully resolve inflammation and achieve clinical endpoints, the lost bone and attachment are largely irreversible. The disease is managed, not cured, requiring lifetime supportive periodontal care (SPT) to prevent relapse [1:38] [3:9].
¶ Does vaping carry the same periodontal risks as smoking?
Yes. Although vaping avoids combustion, aerosolized nicotine causes microvascular vasoconstriction (masking diagnostic bleeding) and chemical flavorings drive local oxidative stress and dysbiosis, significantly compromising tissue healing and defense.
¶ Why do my gums bleed more after I quit smoking?
This is a normal, positive diagnostic sign. Smoking causes microvascular vasoconstriction, masking underlying inflammation. When you quit smoking, your microcirculation recovers, exposing the actual inflammatory state of your gums, which can then be accurately diagnosed and treated.
¶ Is dental floss really inferior to interdental brushes?
In patients with periodontal disease, yes. Interdental brushes are especially indicated in periodontal patients where widened embrasures are common, offering ease of use and superior plaque and gingivitis reduction compared to dental floss [15:6]. Traditional dental floss is highly technique-sensitive and may not confer significant benefits over brushing alone when used inactively [15:7].
¶ How should dental implants be maintained to prevent disease?
Implant maintenance requires structured periodic clinical assessments of peri-implant tissue health and regular professional supportive care starting from the time of loading [20:10]. For daily home-care, interdental brushes and oral irrigators are clinically preferred over dental floss to optimize plaque removal [15:8].
¶ References
Sanz M, Herrera D, Kebschull M, et al. Treatment of stage I-III periodontitis—The EFP S3 level clinical practice guideline. Journal of Clinical Periodontology. 2020. https://pubmed.ncbi.nlm.nih.gov/32383274/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Baeza M, Morales A, Cisterna C, et al. Effect of periodontal treatment in patients with periodontitis and diabetes: systematic review and meta-analysis. Journal of Applied Oral Science. 2020. https://pubmed.ncbi.nlm.nih.gov/31939522/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Fischer RG, Amaral GCLSD, Huamán-Mendoza AA, et al. Treatment of periodontal diseases: Latin America and the Caribbean Consensus 2024. Brazilian Oral Research. 2024. https://pubmed.ncbi.nlm.nih.gov/39607152/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Simpson TC, Weldon JC, Worthington HV, et al. Treatment of periodontal disease for glycaemic control in people with diabetes mellitus. Cochrane Database of Systematic Reviews. 2015. https://pubmed.ncbi.nlm.nih.gov/26545069/ ↩︎ ↩︎
Aimetti M, Romano F, Costanzo L, et al. Outcomes of Active Periodontal Therapy in a Specialist University Setting Following EFP S3 Treatment Guideline in Stage III-IV Periodontitis Patients. Journal of Clinical Periodontology. 2026. https://pubmed.ncbi.nlm.nih.gov/41554667/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Arbildo-Vega HI, Cruzado-Oliva FH, Coronel-Zubiate FT, et al. Periodontal disease and cardiovascular disease: umbrella review. BMC Oral Health. 2024. https://pubmed.ncbi.nlm.nih.gov/39468505/ ↩︎ ↩︎ ↩︎
Zhang X, Huang X, Chang M, et al. Association between periodontal disease and Alzheimer's disease: a scoping review. Frontiers in Aging Neuroscience. 2025. https://pubmed.ncbi.nlm.nih.gov/41170438/ ↩︎ ↩︎ ↩︎ ↩︎
Papapanou PN, Sanz M, Buduneli N, et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. Journal of Clinical Periodontology. 2018. https://pubmed.ncbi.nlm.nih.gov/29926490/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Galarraga-Vinueza ME, Pagni S, Finkelman M, et al. Prevalence, incidence, systemic, behavioral, and patient-related risk factors and indicators for peri-implant diseases: An AO/AAP systematic review and meta-analysis. Journal of Periodontology. 2025. https://pubmed.ncbi.nlm.nih.gov/40489307/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Renvert S, Quirynen M. Risk indicators for peri-implantitis. A narrative review. Clinical Oral Implants Research. 2015. https://pubmed.ncbi.nlm.nih.gov/26385619/ ↩︎ ↩︎ ↩︎ ↩︎
Simpson TC, Clarkson JE, Worthington HV, et al. Treatment of periodontitis for glycaemic control in people with diabetes mellitus. Cochrane Database of Systematic Reviews. 2022. https://pubmed.ncbi.nlm.nih.gov/35420698/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Billings M, Holtfreter B, Papapanou PN, et al. Age-dependent distribution of periodontitis in two countries: Findings from NHANES 2009 to 2014 and SHIP-TREND 2008 to 2012. Journal of Periodontology. 2018. https://pubmed.ncbi.nlm.nih.gov/29926940/ ↩︎
Matthews DC. Powered toothbrush plus triclosan only as effective as manual brush and fluoride toothpaste for periodontal maintenance patients. Evidence-Based Dentistry. 2008. https://pubmed.ncbi.nlm.nih.gov/18927564/ ↩︎ ↩︎ ↩︎ ↩︎
Wilder RS, Bray KS. Improving periodontal outcomes: merging clinical and behavioral science. Periodontology 2000. 2016. https://pubmed.ncbi.nlm.nih.gov/27045431/ ↩︎ ↩︎ ↩︎ ↩︎
Ng E, Lim LP. An Overview of Different Interdental Cleaning Aids and Their Effectiveness. Dentistry Journal. 2019. https://pubmed.ncbi.nlm.nih.gov/31159354/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Worthington HV, MacDonald L, Poklepovic Pericic T, et al. Home use of interdental cleaning devices, in addition to toothbrushing, for preventing and controlling periodontal diseases and dental caries. Cochrane Database of Systematic Reviews. 2019. https://pubmed.ncbi.nlm.nih.gov/30968949/ ↩︎ ↩︎
Brookes ZLS, Bescos R, Belfield LA, et al. Current uses of chlorhexidine for management of oral disease: a narrative review. Journal of Dentistry. 2020. https://pubmed.ncbi.nlm.nih.gov/33075450/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Ahmed MM, Alasmari DS. A Cross-Sectional Evaluation of Dental Professional's Knowledge of Locally Delivered Antimicrobial Agents and their Application in Periodontal Practice. Journal of Pharmacy & Bioallied Sciences. 2023. https://pubmed.ncbi.nlm.nih.gov/37694064/ ↩︎ ↩︎ ↩︎ ↩︎
Mainas G, Santamaria P, Ide M. Could dietary restrictions affect periodontal disease? A systematic review. Clinical Oral Investigations. 2023. https://pubmed.ncbi.nlm.nih.gov/37199773/ ↩︎ ↩︎ ↩︎
Herrera D, Berglundh T, Schwarz F, et al. Prevention and treatment of peri-implant diseases—The EFP S3 level clinical practice guideline. Journal of Clinical Periodontology. 2023. https://pubmed.ncbi.nlm.nih.gov/37271498/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Krajewski A, Perussolo J, Gkranias N, et al. Influence of periodontal surgery on the subgingival microbiome-A systematic review and meta-analysis. Journal of Periodontal Research. 2023. https://pubmed.ncbi.nlm.nih.gov/36597817/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Borsa L, Dubois M, Sacco G, et al. Analysis the Link between Periodontal Diseases and Alzheimer's Disease: A Systematic Review. International Journal of Environmental Research and Public Health. 2021. https://pubmed.ncbi.nlm.nih.gov/34501899/ ↩︎
Le QA, Akhter R, Coulton KM, et al. Periodontitis and Preeclampsia in Pregnancy: A Systematic Review and Meta-Analysis. Maternal and Child Health Journal. 2022. https://pubmed.ncbi.nlm.nih.gov/36209308/ ↩︎
Sanz M, Kornman K, et al. Periodontitis and adverse pregnancy outcomes: consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. Journal of Clinical Periodontology. 2013. https://pubmed.ncbi.nlm.nih.gov/23627326/ ↩︎ ↩︎ ↩︎
Sanz M, Kornman K, et al. Periodontitis and adverse pregnancy outcomes: consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. Journal of Periodontology. 2013. https://pubmed.ncbi.nlm.nih.gov/23631576/ ↩︎ ↩︎ ↩︎
Favero V, Bacci C, Volpato A, et al. Pregnancy and Dentistry: A Literature Review on Risk Management during Dental Surgical Procedures. Dentistry Journal. 2021. https://pubmed.ncbi.nlm.nih.gov/33921608/ ↩︎ ↩︎
Montoya-Carralero JM, Ávila-Villasmil R, Sánchez-Pérez A, et al. Relationship between periodontal disease and preterm birth. A systematic review and meta-analysis. Medicina Oral, Patología Oral y Cirugía Bucal. 2024. https://pubmed.ncbi.nlm.nih.gov/39396142/ ↩︎ ↩︎
Sanz M, Kamma J, Goldstein M. The impact of the European Federation of Periodontology on European and global periodontology. Periodontology 2000. 2025. https://pubmed.ncbi.nlm.nih.gov/39891466/ ↩︎
Goldstein M, Donos N, Teughels W. Structure, governance and delivery of specialist training programs in periodontology and implant dentistry. Journal of Clinical Periodontology. 2024. https://pubmed.ncbi.nlm.nih.gov/39072845/ ↩︎
Ali K, Charde P, Zahra D, et al. Periodontal precision: diagnostic skills and confidence of dentists in Asian countries in applying the 2017 EFP/AAP periodontal disease classification- a cross-sectional pilot study. BMC Oral Health. 2025. https://pubmed.ncbi.nlm.nih.gov/41350998/ ↩︎
Zerman N. Replantation After Dental Avulsion: A Scoping Review and Proposal of a Flow Chart. European Journal of Paediatric Dentistry. 2024. https://pubmed.ncbi.nlm.nih.gov/39015942/ ↩︎