¶ Polycystic Ovary Syndrome
| Indication | Anovulatory infertility, metabolic dysfunction, hyperandrogenism |
| Access | Clinical diagnosis and multidisciplinary management |
| Diagnostic Criteria | Rotterdam Consensus (2 of 3 features) or PMOS standards |
| Safety Profile | Low-to-moderate risk, personalized pharmacotherapy |
| Key Markers | Total/Free Testosterone, LH/FSH, fasting insulin, DHEAS, AMH |
| Est. Cost | Variable; depends on pharmacological and lifestyle interventions |
Polycystic Ovary Syndrome (PCOS) is a heterogeneous endocrine disorder affecting women of reproductive age worldwide [1], and is recognized as the most common endocrine disorder in this population [2]. To better reflect its multi-systemic physiological nature and avoid the historical misconception that pathological ovarian cysts are a mandatory feature, global expert consensus has initiated a transition toward renaming the condition to Polyendocrine Metabolic Ovarian Syndrome (PMOS) [3].
¶ At a glance
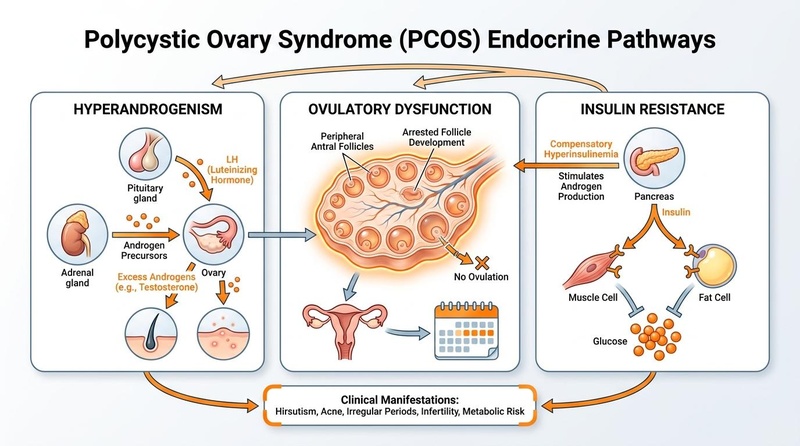
- Systemic Endocrine Pathology: Polycystic Ovary Syndrome is not a localized ovarian disease, but rather a complex, heterogeneous endocrine disorder characterized by excessive androgen activity, abnormal insulin activity, and ovarian dysfunction [1:1][4]. While its exact cause remains unknown, its clinical hallmarks are hyperandrogenism and insulin resistance [1:2][5].
- High Global Prevalence: The Cochrane Database of Systematic Reviews (Lim et al., 2019) estimates that PCOS affects approximately 8% to 13% of women of reproductive age globally [6]. Global prevalence estimates vary across different cohorts and ethnicities; a systematic review and meta-analysis of unselected populations by Bozdag et al. (2016) reported a prevalence of 6% (95% CI: 5%–8%) under NIH criteria and 9% (95% CI: 7%–12%) under Rotterdam criteria, while the overall pooled prevalence across all included populations was 10% (95% CI: 8%–13%) under Rotterdam criteria [2:1], while a comprehensive global meta-analysis by Salari et al. (2024) estimated a global prevalence of 9.2% (95% CI: 6.8%–12.5%) [7].
- Multi-Organ Risks: Left unmanaged, the condition significantly elevates the risk of developing type 2 diabetes (T2D), metabolic syndrome, endometrial neoplasia, and severe psychosocial comorbidities [8][9][10][11].
- Efficacy-Led Management: Clinical management must focus on phenotypic staging and patient-specific goals—prioritizing lifestyle modifications as a supportive metabolic foundation, combined oral contraceptive pills (COCPs) for cycle control and hyperandrogenism, and targeted therapies for ovulation induction or insulin sensitization [8:1][12].
¶ Diagnostic Frameworks & Clinical Assessment
The diagnosis of PCOS has historically been a subject of evolving clinical consensus. Because of its phenotypic heterogeneity, three major diagnostic standards are recognized internationally. Accurate diagnosis requires the fulfillment of specific criteria and the mandatory exclusion of mimicking disorders.
¶ Comparison of Diagnostic Standards
- Rotterdam Consensus (2003): Requires at least 2 of 3 features [13][14]:
- Ovulatory Dysfunction (Oligo- or Anovulation)
- Hyperandrogenism (Clinical and/or Biochemical)
- Polycystic Ovarian Morphology (PCOM) on ultrasound or high serum AMH
- NIH Criteria (1990): Requires both [13:1][2:2]:
- Ovulatory Dysfunction
- Hyperandrogenism (Clinical and/or Biochemical)
- AE-PCOS Criteria (2006): Requires both [15][2:3]:
- Hyperandrogenism (Clinical and/or Biochemical)
- Ovarian Dysfunction (Ovulatory Dysfunction and/or PCOM)
¶ 1. The Rotterdam Consensus (2003)
The Rotterdam criteria are the most widely used and accepted diagnostic framework internationally [8:2][14:1]. Under this framework, a diagnosis of PCOS is established if at least two of the following three features are present:
- Oligo- or Anovulation: Typically presenting as amenorrhea (absence of menstruation) or oligomenorrhea (menstrual cycles of irregular frequency) [4:1].
- Hyperandrogenism: Either clinical signs (such as severe acne or hirsutism) or biochemical markers (elevated free testosterone or free androgen index) [13:2][1:3].
- Polycystic Ovarian Morphology (PCOM): Characterized on ultrasound by an elevated follicle count and/or enlarged ovarian volume [14:2][16]. The 2023 international guidelines incorporate the use of serum Anti-Müllerian Hormone (AMH) as an alternative diagnostic marker for polycystic ovarian morphology (PCOM) in adult populations, reflecting its robust diagnostic performance for adult PCOS with a high pooled sensitivity of 0.79 and specificity of 0.87 in the meta-analysis of 82 studies by van der Ham et al. (2024) [17].
¶ 2. The National Institutes of Health (NIH) Criteria (1990)
Based on the original 1990 NIH-sponsored conference criteria, a diagnosis of PCOS required the presence of both chronic anovulation (ovulatory dysfunction) and clinical or biochemical hyperandrogenism, which excludes phenotypes without androgen excess or those with normal ovulatory function [13:3][2:4][5:1].
¶ 3. The Androgen Excess & PCOS (AE-PCOS) Society Criteria (2006)
The AE-PCOS Society criteria (2006) position androgen excess as the fundamental hallmark of the syndrome [15:1]. To establish a diagnosis under this framework, the patient must exhibit hyperandrogenism (clinical and/or biochemical) in combination with at least one feature of ovarian dysfunction (either oligo-anovulation or polycystic ovarian morphology on ultrasound) [15:2].
¶ Adolescent Diagnostic Caveats
Diagnosing PCOS in adolescents requires extreme caution to avoid over-diagnosis. Normal pubertal transition often mimics several features of the syndrome, including transient insulin resistance, irregular anovulatory menstrual cycles, and multicystic ovarian appearance on ultrasound.
- Post-Menarche Delay: A formal diagnosis of PCOS is often challenging and should be made with caution in the immediate years post-menarche, as normal pubertal changes can mimic several features of the syndrome [18].
- Inapplicability of Ultrasound: Pelvic ultrasound is not recommended and should not be used for diagnostic purposes in adolescent patients, as normal pubertal development can mimic several phenotypic features of the syndrome [19][18:1].
- Strict Criteria for Adolescents: To prevent over-diagnosis, diagnostic standards in adolescents require the simultaneous presence of both persistent ovulatory dysfunction and clinical or biochemical hyperandrogenism, as established in the 2023 international guidelines [8:3][19:1][18:2].
¶ Differential Diagnosis & Mimic Exclusions (Crucial Clinical Checklist)
Because the diagnostic frameworks are syndromic, PCOS/PMOS is fundamentally a diagnosis of exclusion. A clinician must systematically evaluate and exclude look-alike endocrine disorders before assigning the diagnosis. Standard protocols require a comprehensive differential workup to exclude these mimics.
| Disorder to Exclude | Primary Clinical Clues | Diagnostic Test & Exclusion Threshold | Clinical Guidelines & Evidence Alignment |
|---|---|---|---|
| Thyroid Dysfunction | Weight changes, thermal intolerance, fatigue, menstrual irregularity | Fasting Serum Thyroid-Stimulating Hormone (TSH). Exclusion Threshold: TSH must be within standard clinical reference ranges. Abnormal TSH levels require clinical investigation of hypothyroidism or hyperthyroidism to rule out thyroid-induced ovulatory dysfunction [1:4][4:2][20]. |
Systematically evaluate thyroid status to rule out alternative causes of ovulatory and menstrual cycle dysfunction, particularly in patients with suspected secondary endocrine disruptions [1:5][4:3][20:1]. |
| Hyperprolactinemia | Galactorrhea, visual changes, headache, oligomenorrhea or amenorrhea | Fasting morning serum prolactin. Exclusion Threshold: Prolactin levels must be within standard reference limits. Elevated prolactin levels require investigation of secondary hyperprolactinemia or drug-induced prolactin excess [1:6][4:4][20:2]. |
Evaluate for prolactin excess or drug-induced hyperprolactinemia to rule out alternative causes of menstrual irregularity and chronic anovulation [1:7][4:5][20:3]. |
| Non-Classic Congenital Adrenal Hyperplasia (NCCAH) | Early adrenarche, hirsutism, acne, short stature, oligomenorrhea | Fasting morning follicular-phase 17-hydroxyprogesterone (17-OHP). Exclusion Threshold: 17-OHP must be within standard reference limits. Elevated values require dynamic ACTH stimulation testing to differentiate from PCOS [14:3][15:3][21]. |
Exclude congenital adrenal disorders or genetic causes of androgen excess, as guidelines require the systematic exclusion of alternate adrenal pathologies in hyperandrogenic presentations [14:4][15:4][21:1]. |
| Cushing's Syndrome | Central obesity, purple striae, proximal muscle weakness, buffalo hump, hypertension | 1 mg overnight dexamethasone suppression test (DST), 24-hour urinary free cortisol (UFC), or late-night salivary cortisol. Exclusion Thresholds: Normal cortisol suppression or cortisol levels within standard reference ranges rule out Cushing's syndrome [14:5][1:8]. |
Clinically evaluate for cortisol excess in patients presenting with overlapping metabolic and physical features of Cushing's syndrome to rule out alternative endocrine disorders [14:6][1:9][5:2]. |
| Androgen-Secreting Neoplasms | Virilization (voice deepening, clitoromegaly), rapid-onset, severe, progressive hirsutism | Fasting serum total testosterone and dehydroepiandrosterone sulfate (DHEAS). Exclusion Thresholds: Testosterone and DHEAS levels within typical ranges for benign androgen excess. Rapidly progressive hyperandrogenism or highly elevated markers require pelvic/adrenal imaging [14:7][21:2]. |
Exclude underlying adrenal or ovarian neoplasms, especially in cases presenting with severe hyperandrogenism or rapid-onset virilizing features [14:8][21:3]. |
¶ Systemic & Multi-Organ Implications
PCOS/PMOS is a systemic condition with profound metabolic, tissue-level, and psychological implications that span the patient’s lifespan.
: HPO Axis & Insulin Resistance")
┌───────────────────────────┐
│ PCOS Pathology │
└─────────────┬─────────────┘
│
┌───────────────────────────────┼──────────────────────────────┐
▼ ▼ ▼
┌──────────────────┐ ┌──────────────────┐ ┌──────────────────┐
│ Metabolic │ │ Endometrial │ │ Fertility │
│ Insulin Resist. │ │ Anovulation │ │ Anovulation │
│ T2D & MetS │ │ Unopposed Est. │ │ Subfertility │
│ Cardiovasc. Risk │ │ Hyperpl./Cancer │ │ Gestational DM │
└──────────────────┘ └──────────────────┘ └──────────────────┘
¶ 1. Metabolic Dysregulation & Cardiovascular Risk
The pathophysiology of PCOS is deeply intertwined with insulin resistance. Insulin resistance is a key feature of PCOS that is highly prevalent in overweight and obese individuals, significantly increasing the risk of metabolic syndrome [10:1].
- Type 2 Diabetes Risk: Women with PCOS face a significantly increased risk of developing type 2 diabetes compared to age-matched controls, as established in the 2023 international guidelines [8:4].
- Metabolic Syndrome: There is a highly increased prevalence of metabolic syndrome, with an overall odds ratio of 3.35 (95% CI: 2.44–4.59) reported in the meta-analysis of unselected populations by Lim et al. (2019), particularly in overweight and obese individuals [10:2]. This metabolic risk is pathophysiologically linked to underlying insulin resistance, chronic hyperinsulinemia, and cardiovascular risk markers [10:3][1:10].
- Cardiovascular & Metabolic Risk: Chronic hyperinsulinemia, insulin resistance, and dyslipidemia significantly elevate the long-term risk of cardiovascular disease, hypertension, and metabolic syndrome in women with PCOS [10:4][11:1].
¶ 2. Endometrial Integrity & Neoplastic Risk
Chronic anovulation disrupts regular endometrial shedding. In patients with PCOS:
- Malignancy Risk: Chronic anovulation is associated with a significantly increased risk of developing endometrial cancer, representing a key long-term neoplastic risk in reproductive-aged women with this syndrome [11:2].
¶ 3. Fertility and Obstetrical Complications
PCOS is the leading cause of anovulatory infertility, representing the majority of reproductive dysfunction cases [1:11].
- Oocyte Competence & Folliculogenesis: The excessive secretion or activity of androgens, combined with altered gonadotropin dynamics and inadequate follicle-stimulating hormone, leads to chronic anovulation and follicle-related infertility in women with PCOS [1:12][5:3].
- Obstetrical Risks: When conception is achieved, women with PCOS experience significantly higher odds of pregnancy-related complications. Meta-analytic evidence from 104 studies by Bahri Khomami et al. (2024) indicates significantly increased odds of gestational diabetes mellitus (GDM), preeclampsia, gestational hypertension, miscarriage, and cesarean section [22].
¶ 4. Dermatologic Manifestations & Cutaneous Markers
Hyperandrogenemia directly impacts pilosebaceous units, leading to classic dermatologic hallmarks:
- Hirsutism: Excessive growth of terminal body hair (hirsutism) on the face, chest, stomach, or thighs is a primary clinical sign of androgen excess [1:13][21:4][23]. Hirsutism is commonly assessed in clinical settings using the modified Ferriman-Gallwey (mFG) scoring system [24][21:5].
- Acne Vulgaris & Hirsutism: Severe acne and hirsutism are common clinical signs of androgen excess and hyperandrogenism [1:14][21:6].
- Acanthosis Nigricans: Hyperpigmented, velvety plaques localized in intertriginous areas (e.g., axillae, neck, groin). This is a direct cutaneous marker of underlying insulin resistance.
¶ 5. Sleep Architecture & Mental Health
The neuropsychiatric burden of PCOS is extensive and frequently underestimated in clinical practice.
- Obstructive Sleep Apnea (OSA): Clinical practice guidelines recommend evaluating risk factors for obstructive sleep apnea (OSA) in patients with PCOS, as it is a recognized clinical risk factor that can complicate metabolic and cardiovascular health [14:9].
- Psychiatric Comorbidities: A systematic review and meta-analysis of 172,040 patients by Brutocao et al. (2018) demonstrated that women with PCOS exhibit significantly increased odds of clinical depression (OR 2.79; 95% CI: 2.23–3.50) and anxiety (OR 2.75; 95% CI: 2.10–3.60) compared to controls [9:1]. This psychological burden is associated with reduced overall quality of life [25], and is often exacerbated by common patient concerns such as infertility, weight management struggles, and delayed diagnosis [26].
¶ Evidence Summary Table (Human Outcomes)
The following table evaluates major clinical, lifestyle, and supplemental interventions for Polycystic Ovary Syndrome based on high-authority human clinical trials and meta-analyses.
| Outcome | Effect | Quality | Consistency | Trials | Notes |
|---|---|---|---|---|---|
| Improvement in Body Composition and BMI (Lifestyle Modifications) | High | High | >25 RCTs | Structured aerobic or resistance exercise reduces body mass index (BMI) (SMD -0.35 in a meta-analysis of 10 RCTs [27]), and improves metabolic parameters [6:1]. | |
| Suppression of Ovarian Androgen Synthesis and Cycle Regulation (COCPs) | High | High | >30 RCTs | First-line non-fertility therapy; typically contains an estrogen and progestin combination. Regulates cycles and biochemically reduces FAI and increases SHBG as shown by Melin et al. (2024) [12:1]. | |
| Glycemic Control and Fasting Insulin Reduction (Metformin) | High | High | >40 RCTs | Metformin at typical therapeutic doses significantly improves metabolic parameters; a meta-analysis of 36 RCTs shows that metformin does not significantly reduce clinical hirsutism compared to COCPs, although metformin lowers fasting insulin levels by 27.12 pmol/L compared with COCP therapy [12:2]. | |
| Alleviation of Hirsutism and Androgenic Alopecia (Spironolactone) | Moderate | High | >15 RCTs | Standard therapeutic doses of anti-androgens (e.g., spironolactone, flutamide, or finasteride) can be considered to treat hirsutism when COCPs are contraindicated, poorly tolerated, or show sub-optimal response after 6 months, as recommended in the 2023 International PCOS Guideline [8:5][28]. | |
| Ovulation Induction and Live Birth Rate (Letrozole) | High | High | Multi-center RCTs | Standard follicular-phase dosing; letrozole is associated with significantly higher live-birth and ovulation rates compared to clomiphene in a letrozole vs. clomiphene trial of 750 women by Legro et al. (2014) [29]. | |
| Ovulation Induction and Live Birth Rate (Clomiphene Citrate) | High | High | Multi-center RCTs | Standard follicular-phase dosing; historically first-line, but associated with lower cumulative live-birth and ovulation rates compared to letrozole under the Legro et al. (2014) trial [29:1]. | |
| Cycle Regularity and Insulin Sensitivity (Myo / D-chiro Inositol) | Moderate | Moderate | >20 RCTs | Inositol treatment is associated with a higher risk of having a regular cycle (RR 1.79) compared to placebo in the meta-analysis of 26 RCTs [30]; however, the 2023 International Guideline update concluded that current evidence remains limited and inconclusive [31]. | |
| Glycemic Control and Insulin Sensitivity Reduction (Vitamin D) | Moderate | Moderate | >10 RCTs | Standard supplemental doses improve glycemic parameters, insulin sensitivity, and HOMA-IR in deficient patients [32]; a meta-analysis of 13 RCTs reported that vitamin D supplementation led to a notable reduction in fasting blood glucose (MD -2.91 mg/dL) and insulin levels (MD -1.98 µIU/mL) [33]; evidence supports total cholesterol (TC) reduction [34]. | |
| Insulin Resistance and Hormonal Balance Improvement (Probiotics & Synbiotics) | Moderate | High | >10 RCTs | Systematic reviews show that probiotic/synbiotic supplementation significantly reduces HOMA-IR, fasting blood glucose, fasting insulin, and total testosterone, while increasing SHBG [35][36]. | |
| Endocrine Profile Regulation and Menstrual Health (Resveratrol & N-Acetylcysteine) | Moderate | Moderate | >25 RCTs | Resveratrol significantly reduces testosterone, LH, and DHEAS [37], while NAC increases progesterone levels, endometrial thickness, and luteinizing hormone (LH) levels as shown in a 2025 meta-analysis [38]. |
¶ Pregnancy Safety, Preconception Transitions, and Health Inequities
Managing PCOS requires proactive care coordination when transitioning from symptom control to pregnancy planning. It also demands a deep understanding of systemic barriers and clinical inequities that affect care delivery.
¶ Preconception Medication Transitions
Several primary therapies used to manage PCOS symptoms are contraindicated during pregnancy and must be safely managed prior to conception:
- Anti-Androgens (Spironolactone, Flutamide, Finasteride): Anti-androgens require concomitant contraception under standard clinical protocols, and their clinical use for hirsutism is reserved for cases where COCPs are contraindicated, poorly tolerated, or show sub-optimal response after 6 months as recommended by the 2023 International Guideline [8:6][28:1].
- Metformin Transition: Metformin is historically discontinued at the time of a positive pregnancy test. While clinical usage and discontinuation protocols may vary, any decisions regarding pharmacological management during pregnancy must be highly individualized based on the patient's metabolic baseline and under strict clinical supervision.
- Aromatase Inhibitors (Letrozole): Letrozole is a nonsteroidal aromatase inhibitor used for preconception ovulation induction. It is associated with significantly higher live-birth and ovulation rates compared to clomiphene in infertile women with PCOS under the Legro et al. (2014) trial [29:2]. Standard daily letrozole dosing is applied across treatment cycles to achieve ovulation induction [29:3].
¶ Gestational Monitoring & Obstetrical Risks
Because PCOS independently increases the risk of maternal and fetal complications, patients require specialized monitoring protocols:
- Preconception and Early Pregnancy Screening: Due to a high baseline risk of gestational diabetes and adverse pregnancy complications, international guidelines emphasize capturing PCOS status preconception or early in pregnancy to facilitate preventative care and appropriate glycemic monitoring [8:7][22:1].
- Hypertensive Monitoring: Patients with PCOS have increased odds of preeclampsia and gestational hypertension, necessitating appropriate clinical monitoring under standard obstetrical protocols [22:2].
¶ Inequities, Diagnostic Delays, and Culturally Competent Care
The clinical journey for PCOS patients is often hindered by systemic barriers and medical bias:
- Ethnic Variations in Presentation: PCOS prevalence estimates vary across different cohorts and ethnicities, reflecting differences in study design, diagnostic criteria, and geographic populations as shown by Bozdag et al. (2016) [2:5].
- Severe Diagnostic Delays: A significant proportion of women experience multi-year delays (with 33.6% reporting > 2 years in the study of 1,385 women by Gibson-Helm et al., 2017) and consult multiple healthcare providers before receiving a definitive diagnosis [26:1]. This delay prolongs untreated metabolic dysfunction and induces profound psychological distress [9:2][26:2].
- Weight-Neutral & Supportive Lifestyle Interventions: Lifestyle interventions (incorporating diet, exercise, and behavioral therapies) are recommended as initial treatment strategies to reduce body weight and improve metabolic and endocrine parameters such as the free androgen index [8:8][6:2]. Given the high psychological burden associated with the condition, clinical guidelines emphasize taking appropriate measures to deliver safe and supportive care while considering factors like weight stigma, as explicitly highlighted in the 2023 international guideline [8:9] and professional exercise position statements [25:1].
¶ Actionable Clinical Protocols
This protocol provides clinicians and patients with a clear, staged pathway for the systematic evaluation, staging, and therapeutic management of PCOS/PMOS.
¶ Step 1: Mimic Exclusion & Diagnosis Verification
Ensure the patient meets Rotterdam criteria (at least 2 of 3 features) or PMOS criteria, and run the mimic exclusion panel before commencing therapy.
┌──────────────────────────────────────────────┐
│ Suspected PCOS Patient Presentation │
└──────────────────────┬───────────────────────┘
│
▼
┌──────────────────────────────────────────────┐
│ Systemic Mimic Screening │
│ • Clinically exclude thyroid disorders │
│ • Exclude hyperprolactinemic disorders │
│ • Exclude non-classic CAH (NCCAH) │
│ • Rule out severe androgen excess/neoplasms │
└──────────────────────┬───────────────────────┘
│
┌─────────────────┴─────────────────┐
▼ ▼
[Any Mimic Confirmed] [All Mimics Excluded]
│ │
▼ ▼
Treat Specific Primary Proceed to Diagnostic Phenotype
Endocrine Pathology Staging (Rotterdam/PMOS)
- Verify Rotterdam Criteria: Ensure at least 2 of 3 features are met in adults, or adolescent-specific hyperandrogenic and menstrual cycle criteria are satisfied [14:10][19:2][18:3].
- Clinical and Laboratory Exclusion Strategy:
- Thyroid Status: Thyroid dysfunction (such as hypothyroidism or hyperthyroidism) must be clinically evaluated and ruled out as an alternative cause of menstrual irregularity and ovulatory disruption [1:15][4:6][20:4].
- Prolactin Assessment: Rule out alternative causes of menstrual dysfunction and anovulation, including hyperprolactinemic conditions or drug-induced prolactin elevations [1:16][4:7][20:5].
- Adrenal and Genetic Pathology: Systematically evaluate and exclude alternate causes of androgen excess, such as congenital adrenal hyperplasia (CAH) or related genetic disorders, in patients presenting with signs of hyperandrogenism [14:11][15:5][21:7].
- Androgen-Secreting Neoplasms: Investigate severe or rapid-onset clinical and biochemical androgen excess to rule out underlying adrenal or ovarian tumors, in accordance with clinical practice guidelines for the assessment of severe hyperandrogenism [14:12][21:8].
¶ Step 2: Phenotypic Staging & Goal Identification
Categorize the patient into one of the four established Rotterdam phenotypes to guide targeted therapy:
- Phenotype A (Classic): Hyperandrogenism + Ovulatory Dysfunction + PCOM
- Phenotype B (Hyperandrogenic-Anovulatory): Hyperandrogenism + Ovulatory Dysfunction
- Phenotype C (Ovulatory): Hyperandrogenism + PCOM
- Phenotype D (Non-Hyperandrogenic): Ovulatory Dysfunction + PCOM
Determine the primary clinical goal:
- Cosmetic / Dermatologic (Acne, Hirsutism, Alopecia)
- Metabolic (Insulin Resistance, Weight, Dyslipidemia)
- Reproductive (Ovulation Induction, Pregnancy Planning)
¶ Step 3: Actionable Therapeutic Pathways
¶ Pathway 1: Metabolic Foundation (Mandatory for all Phenotypes)
- Exercise Protocol: The 2023 International PCOS Guideline and Exercise and Sports Science Australia (ESSA, 2024) recommend implementing weekly physical activity of 150 to 300 minutes of moderate-intensity or 75 to 150 minutes of vigorous-intensity aerobic exercise, combined with muscle-strengthening activities on 2 non-consecutive days per week, to reduce body mass index and improve body composition [27:1][25:2], with broader metabolic benefits [8:10]. Focus on functional improvements (VO2 max and strength) rather than weight endpoints.
- Nutritional Strategy: Prioritize nutritional interventions and dietary modifications (such as low-carbohydrate, DASH, or low-glycemic diets) to improve metabolic and endocrine outcomes [35:1].
- Supplemental Adjuncts:
- Myo / D-chiro inositol: Can be considered as an alternative or adjunctive option with modest metabolic benefits and significantly fewer gastrointestinal adverse events compared with metformin, although the overall evidence supporting its use remains limited and inconclusive [31:1][30:1].
- Vitamin D: Supplementation of vitamin D improves metabolic parameters, fasting blood glucose, insulin, and lipid levels, particularly in deficient patients with obesity or insulin resistance [33:1][32:1][34:1].
- Probiotics & Synbiotics: Supplementation with probiotics and synbiotics has been shown to modulate the gut microbiota and significantly improve insulin resistance, lipid profiles, and androgen balance, with synbiotics demonstrating more pronounced benefits compared to probiotics alone [35:2][36:1].
- Resveratrol & N-Acetylcysteine (NAC): Resveratrol significantly reduces testosterone, LH, and DHEAS levels compared to placebo [37:1], while NAC has been shown to significantly increase progesterone levels and endometrial thickness in women with PCOS [38:1].
¶ Pathway 2: Cycle Regulation & Hyperandrogenism
- First-Line Pharmacotherapy: Combined oral contraceptive pills (COCPs) containing an estrogen and progestin combination are the first-line pharmacotherapy to regulate the menstrual cycle, reduce circulating androgens, and manage hirsutism or acne [14:13][12:3].
- Anti-Androgen Optimization: Consider adding oral anti-androgens (such as spironolactone, flutamide, or finasteride) under clinical supervision to target clinical hirsutism if goals are not met after 6 months of COCP therapy, ensuring concomitant use of effective contraception as suggested by the 2023 International Guideline [8:11][28:2].
¶ Pathway 3: Ovulation Induction & Fertility
- First-Line Pharmacotherapy: Letrozole is the preferred first-line agent for ovulation induction, as it is associated with significantly higher cumulative ovulation and live-birth rates compared to clomiphene in the Legro et al. (2014) trial [29:4].
- Second-Line Pharmacotherapy: Clomiphene Citrate can be considered as a secondary option for ovulation induction [29:5], or gonadotropin therapy.
- Metabolic Adjunct: Metformin is beneficial for managing metabolic and glycemic abnormalities in PCOS, but it has limited or no benefit as a monotherapy for treating hirsutism, acne, or infertility [14:14][12:4].
¶ FAQ Section
¶ Is an ultrasound required for the diagnosis of PCOS?
No. Under the Rotterdam criteria, because a diagnosis is established by the presence of any two of the three cardinal features (androgen excess, ovulatory dysfunction, or polycystic ovaries), a pelvic ultrasound is not strictly required if a patient already exhibits both clinical or biochemical hyperandrogenism and chronic anovulation [14:15]. Furthermore, the 2023 international guidelines incorporate serum Anti-Müllerian Hormone (AMH) as an alternative diagnostic marker for detecting polycystic ovarian morphology in adults, supported by meta-analytic diagnostic performance of 0.79 sensitivity and 0.87 specificity for adult PCOS diagnosis across 82 studies by van der Ham et al. (2024), although no universal cutoff is established [17:1]. Pelvic ultrasound is not recommended for diagnosing PCOS in adolescents, as normal pubertal development can mimic several phenotypic features of the syndrome, making both persistent ovulatory dysfunction and hyperandrogenism the only reliable diagnostic requirements in this population [19:3][18:4].
¶ Can inositol supplements fully replace metformin?
Inositol (specifically Myo-inositol) acts as an alternative or adjunctive option that offers modest metabolic benefits and significantly fewer gastrointestinal adverse events compared with metformin, although the overall evidence supporting its use remains limited and inconclusive [31:2]. Meta-analytic evidence suggests that metformin may improve waist-to-hip ratio and hirsutism compared to inositol, but there is likely no difference for major reproductive outcomes, and myo-inositol causes fewer gastrointestinal side effects (which are typically mild and self-limited) [31:3]. While some trials support inositol's potential for cycle regulation (showing an RR of 1.79 for cycle normalization compared to placebo in Greff et al. (2023) [30:2]), clinical guidelines maintain that metformin is the primary insulin-sensitizing pharmacotherapy for metabolic and glycemic abnormalities in PCOS [8:12][12:5]. Therefore, inositol should be considered an alternative or adjunctive option with modest metabolic benefits rather than a full therapeutic replacement [31:4][30:3].
¶ What is the role of lifestyle and dietary modifications in PCOS management?
Lifestyle modifications (including diet, exercise, and behavioral therapy) are recommended as first-line treatment strategies to improve metabolic parameters and reduce body mass index [8:13][27:2]. While weight management is a key component, clinicians are encouraged to deliver these interventions in a supportive manner that reduces psychological distress and considers weight stigma, as explicitly highlighted in the 2023 international guideline [8:14].
¶ References
Norman RJ, Dewailly D, Legro RS. Polycystic ovary syndrome. Lancet. 2007;370(9588):685-697. https://pubmed.ncbi.nlm.nih.gov/17720020/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bozdag G, Mumusoglu S, Zengin D, et al. The prevalence and phenotypic features of polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod. 2016;31(12):2841-2855. https://pubmed.ncbi.nlm.nih.gov/27664216/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Teede HJ, Khomami MB, Morman R, et al. Polyendocrine metabolic ovarian syndrome, the new name for polycystic ovary syndrome: a multistep global consensus process. Lancet. 2026;407(10542):2110-2115. https://pubmed.ncbi.nlm.nih.gov/42119588/ ↩︎
King J. Polycystic ovary syndrome. J Midwifery Womens Health. 2006;51(6):415-422. https://pubmed.ncbi.nlm.nih.gov/17081931/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Guzick DS. Polycystic ovary syndrome. Obstet Gynecol. 2004;103(1):181-193. https://pubmed.ncbi.nlm.nih.gov/14704263/ ↩︎ ↩︎ ↩︎ ↩︎
Lim SS, Hutchison SK, Van Ryswyk E, et al. Lifestyle changes in women with polycystic ovary syndrome. Cochrane Database Syst Rev. 2019;3(3):CD007506. https://pubmed.ncbi.nlm.nih.gov/30921477/ ↩︎ ↩︎ ↩︎
Salari N, Nankali A, Ghanbari A, et al. Global prevalence of polycystic ovary syndrome in women worldwide: a comprehensive systematic review and meta-analysis. Arch Gynecol Obstet. 2024;310(3):1211-1225. https://pubmed.ncbi.nlm.nih.gov/38922413/ ↩︎
Teede HJ, Tay CT, Laven JJEL, et al. Recommendations from the 2023 international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Eur J Endocrinol. 2023;189(2):G43-G64. https://pubmed.ncbi.nlm.nih.gov/37580861/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Brutocao C, Zaiem F, Alsawas M, et al. Psychiatric disorders in women with polycystic ovary syndrome: a systematic review and meta-analysis. Endocrine. 2018;62(2):318-325. https://pubmed.ncbi.nlm.nih.gov/30066285/ ↩︎ ↩︎ ↩︎
Lim SS, Kakoly NS, Tan JWJ, et al. Metabolic syndrome in polycystic ovary syndrome: a systematic review, meta-analysis and meta-regression. Obes Rev. 2019;20(2):339-352. https://pubmed.ncbi.nlm.nih.gov/30339316/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chen ZJ, Shi Y. Polycystic ovary syndrome. Front Med China. 2010;4(3):246-250. https://pubmed.ncbi.nlm.nih.gov/21191832/ ↩︎ ↩︎ ↩︎
Melin J, Forslund M, Alesi S, et al. Metformin and Combined Oral Contraceptive Pills in the Management of Polycystic Ovary Syndrome: A Systematic Review and Meta-analysis. J Clin Endocrinol Metab. 2024;109(2):e826-e841. https://pubmed.ncbi.nlm.nih.gov/37554096/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lizneva D, Suturina L, Walker W, et al. Criteria, prevalence, and phenotypes of polycystic ovary syndrome. Fertil Steril. 2016;106(1):6-15. https://pubmed.ncbi.nlm.nih.gov/27233760/ ↩︎ ↩︎ ↩︎ ↩︎
Legro RS, Arslanian SA, Ehrmann DA, et al. Diagnosis and treatment of polycystic ovary syndrome: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2013;98(12):4565-4592. https://pubmed.ncbi.nlm.nih.gov/24151290/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Azziz R, Carmina E, Dewailly D, et al. The Androgen Excess and PCOS Society criteria for the polycystic ovary syndrome: the complete task force report. Fertil Steril. 2009;91(2):456-488. https://pubmed.ncbi.nlm.nih.gov/18950759/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Legro RS, Brzyski RG, Diamond MP, et al. The Pregnancy in Polycystic Ovary Syndrome II study: baseline characteristics and effects of obesity from a multicenter randomized clinical trial. Fertil Steril. 2014;101(1):230-239. https://pubmed.ncbi.nlm.nih.gov/24156957/ ↩︎
van der Ham K, Laven JSE, Tay CT. Anti-müllerian hormone as a diagnostic biomarker for polycystic ovary syndrome and polycystic ovarian morphology: a systematic review and meta-analysis. Fertil Steril. 2024;122(4):686-696. https://pubmed.ncbi.nlm.nih.gov/38944177/ ↩︎ ↩︎
Rothenberg SS, Beverley R, Barnard E. Polycystic ovary syndrome in adolescents. Best Pract Res Clin Obstet Gynaecol. 2018;48:103-114. https://pubmed.ncbi.nlm.nih.gov/28919160/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Saleh FL, Starkman H, Furness A. Polycystic Ovary Syndrome in Adolescents. Obstet Gynecol Clin North Am. 2024;51(4):789-801. https://pubmed.ncbi.nlm.nih.gov/39510738/ ↩︎ ↩︎ ↩︎ ↩︎
Talib HJ, Alderman EM. Gynecologic and reproductive health concerns of adolescents using selected psychotropic medications. J Pediatr Adolesc Gynecol. 2013;26(1):3-9. https://pubmed.ncbi.nlm.nih.gov/22929762/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Elhassan YS, Hawley JM, Cussen L, et al. Society for Endocrinology Clinical Practice Guideline for the Evaluation of Androgen Excess in Women. Clin Endocrinol. 2025;103:1-12. https://pubmed.ncbi.nlm.nih.gov/40364581/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bahri Khomami M, Shorakae S, Hashemi S, et al. Systematic review and meta-analysis of pregnancy outcomes in women with polycystic ovary syndrome. Nat Commun. 2024;15(1):5642. https://pubmed.ncbi.nlm.nih.gov/38965226/ ↩︎ ↩︎ ↩︎
Huddleston HG, Dokras A. Diagnosis and Treatment of Polycystic Ovary Syndrome. JAMA. 2022;327(3):273-274. https://pubmed.ncbi.nlm.nih.gov/35040896/ ↩︎
Kelly FA, de Oliveira Macena Lôbo A, Cardoso JHCO, et al. Comparison of metformin with inositol versus metformin alone in women with polycystic ovary syndrome: a systematic review and meta-analysis of randomized controlled trials. Endocrine. 2025. https://pubmed.ncbi.nlm.nih.gov/39331347/ ↩︎
Sabag A, Patten RK, Moreno-Asso A, et al. Exercise in the management of polycystic ovary syndrome: A position statement from Exercise and Sports Science Australia. J Sci Med Sport. 2024. https://pubmed.ncbi.nlm.nih.gov/38960811/ ↩︎ ↩︎ ↩︎
Gibson-Helm M, Teede H, Dunaif A, Dokras A. Delayed Diagnosis and a Lack of Information Associated With Dissatisfaction in Women With Polycystic Ovary Syndrome. J Clin Endocrinol Metab. 2017;102(2):604-612. https://pubmed.ncbi.nlm.nih.gov/27906550/ ↩︎ ↩︎ ↩︎
Dos Santos IK, Ashe MC, Cobucci RN, et al. The effect of exercise as an intervention for women with polycystic ovary syndrome: A systematic review and meta-analysis. Medicine. 2020;99(16):e19644. https://pubmed.ncbi.nlm.nih.gov/32311937/ ↩︎ ↩︎ ↩︎
Alesi S, Ghelani D, Melin J, et al. Efficacy and safety of anti-androgens in the management of polycystic ovary syndrome: a systematic review and meta-analysis of randomised controlled trials. J Clin Endocrinol Metab. 2023;108(11):e1335-e1346. https://pubmed.ncbi.nlm.nih.gov/37583655/ ↩︎ ↩︎ ↩︎
Legro RS, Brzyski RG, Diamond MP, et al. Letrozole versus clomiphene for infertility in the polycystic ovary syndrome. N Engl J Med. 2014;371(2):119-129. https://pubmed.ncbi.nlm.nih.gov/25006718/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Greff D, Juhász AE, Váncsa S, et al. Inositol is an effective and safe treatment in polycystic ovary syndrome: a systematic review and meta-analysis of randomized controlled trials. Reprod Biol Endocrinol. 2023;21(1):10. https://pubmed.ncbi.nlm.nih.gov/36703143/ ↩︎ ↩︎ ↩︎ ↩︎
Fitz V, Graca S, Mahalingaiah S, et al. Inositol for Polycystic Ovary Syndrome: A Systematic Review and Meta-analysis to Inform the 2023 Update of the International Evidence-based PCOS Guidelines. J Clin Endocrinol Metab. 2024;109(5):1343-1354. https://pubmed.ncbi.nlm.nih.gov/38163998/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wen X, Wang L, Li F. Effects of vitamin D supplementation on metabolic parameters in women with polycystic ovary syndrome: a randomized controlled trial. J Ovarian Res. 2024. https://pubmed.ncbi.nlm.nih.gov/39014475/ ↩︎ ↩︎
Yu M, Chen S, Liu X. The impact of vitamin D supplementation on glycemic control and lipid metabolism in polycystic ovary syndrome: a systematic review of randomized controlled trials. BMC Endocr Disord. 2025;25:1. https://pubmed.ncbi.nlm.nih.gov/40259331/ ↩︎ ↩︎
Hu X, Wang W, Su X, et al. Comparison of nutritional supplements in improving glycolipid metabolism and endocrine function in polycystic ovary syndrome: a systematic review and network meta-analysis. PeerJ. 2023. https://pubmed.ncbi.nlm.nih.gov/38025704/ ↩︎ ↩︎
Moslehi N, Zeraattalab-Motlagh S, Rahimi Sakak F, et al. Effects of nutrition on metabolic and endocrine outcomes in women with polycystic ovary syndrome: an umbrella review of meta-analyses of randomized controlled trials. Nutr Rev. 2023;81(9):1152-1178. https://pubmed.ncbi.nlm.nih.gov/36099162/ ↩︎ ↩︎ ↩︎
Martinez Guevara D, Vidal Cañas S, Palacios I, et al. Effectiveness of Probiotics, Prebiotics, and Synbiotics in Managing Insulin Resistance and Hormonal Imbalance in Women with Polycystic Ovary Syndrome (PCOS): A Systematic Review of Randomized Clinical Trials. Nutrients. 2024;16(22):3812. https://pubmed.ncbi.nlm.nih.gov/39599701/ ↩︎ ↩︎
Ali Fadlalmola H, Elhusein AM, Al-Sayaghi KM, et al. Efficacy of resveratrol in women with polycystic ovary syndrome: a systematic review and meta-analysis of randomized clinical trials. Pan Afr Med J. 2023;45:110. https://pubmed.ncbi.nlm.nih.gov/37333786/ ↩︎ ↩︎
Viña I, Viña JR, Carranza M, et al. Efficacy of N-Acetylcysteine in Polycystic Ovary Syndrome: Systematic Review and Meta-Analysis. Nutrients. 2025;17(2):242. https://pubmed.ncbi.nlm.nih.gov/39861414/ ↩︎ ↩︎