¶ title: Post-Inflammatory Hyperpigmentation and Melasma: A Mechanism-Aware Aesthetic Longevity Guide
description: A comprehensive guide to understanding and treating post-inflammatory hyperpigmentation (PIH) and melasma, focusing on mechanisms, evidence-based interventions, and clinical strategies for aesthetic longevity.
published: 1
date: 2026-07-06T18:24:13.170Z
tags: aesthetics, chemical-peels, dermatology, hyperpigmentation, interventions, lasers, longevity, melasma, pih, skin-health, topical-treatments
editor: markdown
dateCreated: 2026-07-06T18:24:13.170Z
¶ Post-Inflammatory Hyperpigmentation and Melasma: A Mechanism-Aware Aesthetic Longevity Guide
¶ TL;DR
- Effective Photoprotection is Paramount: Consistent use of broad-spectrum sunscreen with iron oxides is the foundational treatment, blocking both UV and HEV light.
- Targeted Tyrosinase Inhibitors are First-Line: Ingredients like hydroquinone, cysteamine, and azelaic acid directly reduce melanin production.
- Melasma Requires Multimodal Approach: Combines topical agents, oral therapies (e.g., tranexamic acid), and sometimes lasers or peels for optimal results.
- Avoid Aggressive Exfoliation: Physical scrubbing or harsh peels can worsen post-inflammatory hyperpigmentation (PIH), especially in darker skin types.
- Patience and Consistency are Key: Improvement timelines range from 2-3 months for PIH to 3-6 months for melasma, with ongoing maintenance crucial to prevent recurrence.
¶ Quick Answer
The core therapeutic strategy for post-inflammatory hyperpigmentation (PIH) and melasma involves diligent broad-spectrum photoprotection, especially with sunscreens containing iron oxides, combined with the consistent application of targeted topical tyrosinase inhibitors such as hydroquinone, cysteamine, or azelaic acid. For melasma, this regimen is often augmented by oral tranexamic acid and, in some cases, gentle clinical procedures like superficial chemical peels or low-fluence lasers, all carefully managed to prevent rebound hyperpigmentation.
¶ Type-Identification Table
| Condition | Characteristics | Wood's Lamp Examination |
|---|---|---|
| Post-Inflammatory Hyperpigmentation (PIH) | Flat, brown, gray, or black spots occurring at sites of previous inflammation (e.g., acne, eczema, trauma). | No enhancement or slight enhancement. |
| Epidermal Melasma | Light-brown, well-defined symmetric patches on the face. | Pigmentation is enhanced, appearing darker and more prominent. |
| Dermal Melasma | Gray-blue, ill-defined patches that are deeper in the skin. | No significant enhancement. |
| Mixed Melasma | A combination of epidermal and dermal features. | Partially enhanced, with some areas appearing darker. |
¶ Evidence Snapshot Table (human outcomes)
| Intervention | Typical Outcome | Certainty Grade | Notes |
|---|---|---|---|
| Hydroquinone (2-4%) | Significant reduction in hyperpigmentation. | High | Gold standard tyrosinase inhibitor [1], [2]. Must be cycled. |
| Cysteamine (5%) | Effective for stubborn pigmentary disorders. | High/Moderate | Non-cytotoxic tyrosinase inhibitor with good safety [3], [4], [5]. |
| Azelaic Acid (15-20%) | Excellent for acne-induced PIH. | Moderate | Reduces melanin production and inflammation [6], [7]. |
| Tranexamic Acid (Oral) | Strong systemic reduction in melasma. | High | Significant pigment clearance with good patient satisfaction [8], [9], [10]. |
| Tranexamic Acid (Topical 2-5%) | Gentle adjuvant for PIH and melasma. | Moderate | Effective at clearing acne-induced PIH and melasma [10:1], [7:1]. |
| Retinoids (Tretinoin) | Accelerates keratinocyte turnover, aids pigment shedding. | High | Effective for PIH, especially in combination therapies [6:1]. |
| Chemical Peels (Glycolic/Salicylic/TCA) | Accelerates epidermal shedding, enhances topical penetration. | Moderate | Adjuvant to topical treatments; careful selection needed for darker skin [11], [12]. |
| Picosecond Nd:YAG Laser (1064 nm) | High-tier pigment destruction. | Moderate/High | Highly effective and safe for melasma treatment [13], [14]. |
| Picosecond Alexandrite Laser (755 nm) | Fast pigment clearance. | Moderate | Higher risk of rebound PIH compared to topical agents [15]. |
¶ Causes Tied to Biology & Anatomy
Hyperpigmentation disorders like PIH and melasma stem from complex biological interactions within the skin:
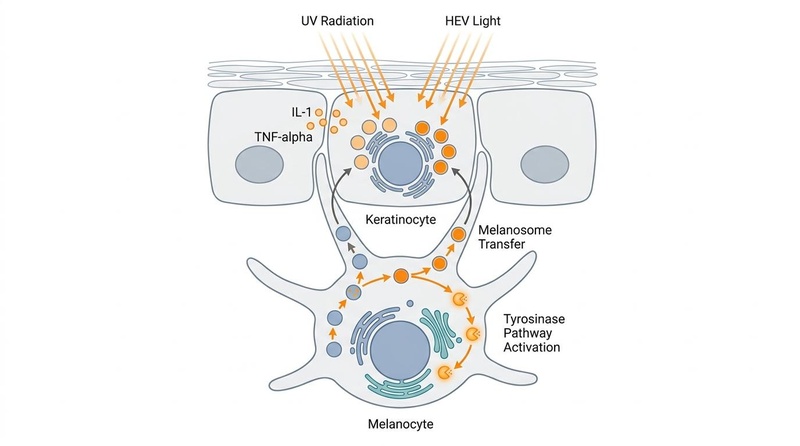
- Melanocyte Hyperactivity and Melanogenesis Pathways: At the core, these conditions involve the overproduction of melanin by melanocytes. Key enzymatic steps, particularly those involving tyrosinase, convert tyrosine into dopaquinone, which then proceeds through a cascade of reactions to form melanin. Melanosomes, the melanin-containing organelles, are then transferred from melanocytes to surrounding keratinocytes, leading to visible pigmentation.
- Inflammatory Cytokines Stimulating Melanogenesis (The PIH Mechanism): In PIH, inflammatory processes trigger the release of various cytokines, including IL-1, TNF-alpha, and endothelin-1, along with activation of the arachidonic acid cascade. These inflammatory mediators directly stimulate melanocytes, leading to increased melanin synthesis and transfer, thus explaining why PIH occurs at sites of previous injury or inflammation.
- Plasminogen Pathway Activation and Localized Microvascular Upregulation in Melasma: Melasma involves distinct pathways beyond simple melanocyte hyperactivity. Activation of the plasminogen pathway leads to increased melanin production, and localized microvascular upregulation contributes to the reddish-brown appearance often seen in melasma. This vascular component highlights why melasma can be particularly challenging to treat.
- The Role of UV and High-Energy Visible (HEV/Blue) Light in Stimulating Melanocytes: Both ultraviolet (UV) radiation and high-energy visible (HEV) light, also known as blue light, are potent stimulators of melanogenesis. They trigger pathways in keratinocytes that, in turn, signal melanocytes to produce more melanin, exacerbating both PIH and melasma and underscoring the critical role of photoprotection.
¶ Starter Protocol
This foundational protocol prioritizes gentle, consistent intervention and broad-spectrum photoprotection.
- Broad-Spectrum Physical (Mineral) Sunscreen: Apply a generous amount daily, every morning, and reapply every 2-3 hours when outdoors. Opt for formulas containing zinc oxide and titanium dioxide for physical blockage, along with iron oxides to effectively block high-energy visible (HEV/blue) light, which is crucial for melasma and PIH management.
- First-Line Topical Tyrosinase Inhibitors:
- Azelaic Acid (15-20%): Apply once or twice daily. Excellent for reducing inflammation and inhibiting tyrosinase, making it ideal for acne-induced PIH [6:2], [7:2].
- Niacinamide (5-10%): Apply once or twice daily. Helps reduce melanosome transfer to keratinocytes and improves skin barrier function.
- Vitamin C (L-Ascorbic Acid 10-20%): Apply mornings. Acts as an antioxidant, reduces melanin production, and brightens skin tone.
¶ Stronger Add-On Path
For more persistent or resistant hyperpigmentation, consider these additional topical therapies, often integrated with the starter protocol.
- Topical Cysteamine 5%: Apply daily as a short-contact therapy (e.g., leave on for 15-30 minutes, then rinse). This highly effective non-hydroquinone alternative is a potent tyrosinase inhibitor and dopaquinone scavenger, with a favorable safety profile and no risk of exogenous ochronosis [3:1], [4:1], [5:1].
- Hydroquinone (2-4%): Used under strict clinical guidance with a 3-month cycle / 3-month holiday rule to prevent exogenous ochronosis (permanent blue-black pigmentation) [2:1]. This is considered the gold standard tyrosinase inhibitor for its rapid and effective depigmenting action.
- Topical Retinoids (e.g., Tretinoin): Apply at night. Accelerates keratinocyte turnover, promoting faster shedding of pigmented skin cells. This enhances the efficacy of other topical agents [6:3]. Start with lower concentrations (e.g., 0.025%) and gradually increase as tolerated to minimize irritation.
¶ Clinical/Procedure Path
These advanced interventions are typically performed by dermatologists and can provide more rapid or significant improvement for recalcitrant cases, often in combination with topical and oral therapies.
- Low-Fluence Q-switched 1064 nm Nd:YAG or Picosecond Lasers: These lasers target melanin with minimal thermal damage, effectively breaking down pigment. They are particularly effective for melasma and PIH, especially when combined with oral tranexamic acid for quicker clearance and reduced rebound risk [13:1], [14:1], [16].
- Superficial Chemical Peels:
- Glycolic Acid: An alpha-hydroxy acid (AHA) that promotes exfoliation.
- Salicylic/Mandelic Acid Combination: Beta-hydroxy acid (BHA) and AHA combination suitable for acne-prone skin and darker skin types.
- Trichloroacetic Acid (TCA): A stronger chemical peel that can be used at various concentrations (e.g., 15-25%) for more significant epidermal shedding. Superficial peels accelerate epidermal shedding and enhance the penetration of topical agents, but careful patient selection is critical to prevent rebound hyperpigmentation [11:1], [12:1].
- Oral Tranexamic Acid (250 mg BID for 3-6 months): This systemic treatment is highly effective for melasma by inhibiting the plasminogen pathway, which contributes to melanin production and vascular changes. Mandatory thromboembolic risk screening is required before initiation due to its potential to increase clotting risk [9:1], [10:2].
¶ What Fails
Understanding ineffective or counterproductive practices is as important as knowing effective treatments.
- Physical Scrubbing or Mechanical Exfoliation: Aggressive scrubbing, harsh brushes, or abrasive exfoliants can trigger inflammation, which in turn worsens PIH, especially in individuals with Fitzpatrick IV-VI skin types.
- Over-use of High-Strength Peeling Acids without Photoprotection: Applying strong chemical peels or high concentrations of alpha/beta hydroxy acids without rigorous, consistent photoprotection leaves the skin highly vulnerable to UV and HEV light, almost guaranteeing rebound hyperpigmentation.
- Long-Term Steroid-Containing Fading Creams: While steroids can initially reduce inflammation, prolonged use of potent topical corticosteroids can lead to skin thinning (atrophy), telangiectasias (spider veins), and steroid-induced acne, ultimately exacerbating hyperpigmentation or causing new dermatological issues.
- Inconsistent Photoprotection: Even brief, unprotected sun exposure can undo months of diligent treatment, resetting the melanogenesis cycle and causing rapid recurrence of PIH and melasma. Sunscreen application must be a daily, consistent habit, even on cloudy days or indoors near windows.
¶ Tracking Plan
Consistent tracking helps assess progress and adjust treatment strategies.
- Timelines for Improvement:
- PIH: Expect initial improvements within 2-3 months of consistent treatment.
- Melasma: Progress is slower, typically requiring 3-6 months to see significant reduction.
- Self-Photography: Take standardized photographs under consistent lighting (e.g., same location, time of day, angle) weekly or bi-weekly. This provides an objective visual record of changes.
- Wood's Lamp Evaluation: A dermatologist can use a Wood's lamp to differentiate between epidermal, dermal, and mixed melasma. This helps track changes in pigment depth and guides treatment adjustments, as epidermal pigment responds more readily to topical treatments.
¶ Safety & Red Flags
Awareness of potential adverse effects and when to seek clinical advice is crucial.
- Exogenous Ochronosis: This is a permanent, irreversible blue-black pigmentation that can result from prolonged and improper use of hydroquinone, especially in darker skin types. It underscores the importance of strict cycling and clinical supervision.
- Rebound Hyperpigmentation: Aggressive laser treatments or strong chemical peels, particularly in Fitzpatrick IV-VI skin, can induce significant inflammation that leads to a worsening or recurrence of hyperpigmentation, often more severe than the initial condition.
- Mottled Hypopigmentation: Permanent loss of pigment, resulting in lighter spots or patches, can occur with overly aggressive treatments, especially certain lasers, if not carefully controlled.
¶ FAQs
What is the difference between PIH and melasma?
PIH (Post-Inflammatory Hyperpigmentation) occurs after skin inflammation or injury, appearing as dark spots where the lesion was. Melasma is a chronic condition characterized by symmetrical brown or gray-brown patches on the face, often triggered by hormonal changes, sun exposure, and genetics.
Can melasma be cured completely?
Melasma is a chronic condition that can be managed effectively but rarely cured completely. Treatment focuses on significant reduction and long-term maintenance to prevent recurrence.
What is the most effective ingredient for hyperpigmentation?
Do I need to wear sunscreen indoors for hyperpigmentation?
Yes, it is recommended, especially if you are near windows. UV and HEV (blue light) can penetrate windows and contribute to hyperpigmentation. Sunscreens with iron oxides are particularly beneficial for blocking HEV light.
How long does it take to see results from hyperpigmentation treatments?
For PIH, initial improvements can be seen within 2-3 months. Melasma typically requires 3-6 months of consistent treatment, and ongoing maintenance is essential to prevent recurrence.
Are natural remedies effective for hyperpigmentation?
While some natural ingredients like Vitamin C, licorice extract, and kojic acid have depigmenting properties, they are generally less potent than prescription-strength options like hydroquinone or cysteamine. They can be good adjunctive therapies or for mild cases.
What treatments should I avoid if I have dark skin and hyperpigmentation?
Individuals with darker skin (Fitzpatrick IV-VI) should exercise extreme caution with aggressive lasers and strong chemical peels, as these can easily cause rebound hyperpigmentation. Physical scrubbing and prolonged use of high-strength steroid creams should also be avoided.
¶ References
Mar, K., Khalid, B., & Maazi, M. (2024). Treatment of Post-Inflammatory Hyperpigmentation in Skin of Colour: A Systematic Review. Journal of Cutaneous Medicine and Surgery. https://pubmed.ncbi.nlm.nih.gov/39075672/ ↩︎ ↩︎
Bhattar, P. A., & Zafaryab, M. (2024). Different therapeutic approaches in melasma: advances and limitations. Frontiers in Pharmacology. https://www.frontiersin.org/journals/pharmacology/articles/10.3389/fphar.2024.1337282/full ↩︎ ↩︎ ↩︎
Desai, S., et al. (2021). Topical Stabilized Cysteamine as a New Treatment for Hyperpigmentation Disorders: Melasma, Post-Inflammatory Hyperpigmentation, and Lentigines. Journal of Drugs in Dermatology (JDD). https://pubmed.ncbi.nlm.nih.gov/34898155/ ↩︎ ↩︎ ↩︎
Desai, S., et al. (2023). Assessing the Effectiveness of Stabilized Cysteamine 5% Cream Compared to Hydroquinone 4%/Ascorbic Acid 3% Combination Cream in Treating Acne-induced Post-inflammatory Hyperpigmentation: A Randomized, Controlled Study. Journal of Clinical and Aesthetic Dermatology (JCAD). https://jcadonline.com/effectiveness-cysteamine-cream-hydroquinone-ascorbic-acid/ ↩︎ ↩︎
Karrabi, M., et al. (2021). Clinical evaluation of efficacy, safety and tolerability of cysteamine 5% cream in comparison with modified Kligman’s formula in subjects with epidermal melasma: A randomized, double-blind clinical trial study. Skin Research and Technology. https://esmed.org/MRA/mra/article/view/6992 ↩︎ ↩︎
Grimes, P. E. (2010). Postinflammatory Hyperpigmentation: A Review of the Epidemiology, Clinical Features, and Treatment Options in Skin of Color. Journal of Clinical and Aesthetic Dermatology (JCAD). https://pmc.ncbi.nlm.nih.gov/articles/PMC2921758/ ↩︎ ↩︎ ↩︎ ↩︎
Sobhan, S. M., et al. (2022). A comparative study of 20% azelaic acid cream versus 5% tranexamic acid solution for the treatment of postinflammatory hyperpigmentation in patients with acne vulgaris: a single-blinded randomized clinical trial. Journal of Cosmetic Dermatology. https://onlinelibrary.wiley.com/doi/10.1111/jocd.15561 ↩︎ ↩︎ ↩︎
AlJabr, N. N., et al. (2026). Tranexamic Acid for Hyperpigmentation Disorders: A Literature Review on Efficacy and Safety in Melasma and PIH. Journal of Cosmetic Dermatology. https://pmc.ncbi.nlm.nih.gov/articles/PMC12848551/ ↩︎
Sarkar, R., et al. (2023). Oral Tranexamic Acid for the Treatment of Melasma: Evidence and Experience-Based Consensus Statement from Indian Experts. Indian Journal of Dermatology. https://pubmed.ncbi.nlm.nih.gov/42109558/ ↩︎ ↩︎
Janney, C., et al. (2024). Randomized Clinical Trial on the Efficacy of Oral Tranexamic Acid Versus Topical Tranexamic Acid in Treatment of Melasma. Journal of Clinical and Diagnostic Research. https://pubmed.ncbi.nlm.nih.gov/42228070/ ↩︎ ↩︎ ↩︎
Sarkar, R., et al. (2016). Comparative Evaluation of Efficacy and Tolerability of Glycolic Acid, Salicylic Mandelic Acid, and Phytic Acid Combination Peels in Melasma. Dermatologic Surgery. https://pubmed.ncbi.nlm.nih.gov/12472345/ ↩︎ ↩︎
Spirovska, M., et al. (2025). Evaluation of the Degree of Melasma Reduction After Application of a Chemical Skin Stimulation Product in Combination with a Lightening Serum. Cosmetics. https://www.mdpi.com/2079-9284/12/6/276 ↩︎ ↩︎
Choudhary, K., et al. (2023). Efficacy and safety of picosecond laser for the treatment of melasma: a systematic review and meta-analysis. Archives of Dermatological Research. https://pubmed.ncbi.nlm.nih.gov/36897459/ ↩︎ ↩︎
Zhu, N., et al. (2023). Comparison of the efficacy and safety of picosecond Nd:YAG laser (1,064 nm), picosecond alexandrite laser (755 nm) and 2% hydroquinone cream in the treatment of melasma: A randomized, controlled, assessor-blinded trial. Frontiers in Medicine. https://pubmed.ncbi.nlm.nih.gov/42064496/ ↩︎ ↩︎
Chua, S., et al. (2025). Assessing the Safety and Efficacy of Picosecond Alexandrite Lasers in the Management of Melasma: A Systematic Review and Meta‐Analysis of Randomised Control Trials. Australasian Journal of Dermatology. https://onlinelibrary.wiley.com/doi/10.1111/ajd.70051?af=R ↩︎
Feng, X., et al. (2025). Low‐Fluence Q‐Switch 1064 Nm Laser Combined With Oral Tranexamic Acid: A Quicker Treatment for Laser‐Induced Postinflammatory Hyperpigmentation. Journal of Cosmetic Dermatology. https://onlinelibrary.wiley.com/doi/full/10.1111/jocd.70018 ↩︎